Embed Size (px)
DESCRIPTION
Chapter 32 Role of The Clinical Microbiology Laboratory in Hospital Epidemiology and Infection Control Hui Wang. IN HOSPITAL EPIDEMIOLOGY AND INFECTION CONTROL. Nosocomial infection : acquired in a hospital or healthcare facility - PowerPoint PPT Presentation
Citation preview

Chapter 32 Role of The Clinical
Microbiology Laboratory in Hospital Epidemiology and
Infection Control
Hui Wang

IN HOSPITAL EPIDEMIOLOGY AND INFECTION CONTROL
Nosocomial infection : acquired in a hospital or healthcare facility an onset of symptom more than 48 hours
after admission (shorter hospital stays)
(eg. surgical wound infections ) may not be recognized until after discharge
(postdischarge surveillance )

EPIDEMIOLOGY CHARACTERISTICS OF NOSOCOMIAL INFECTIONS(1)
Main Infection Sites (5% to 10% of inpatients) UTI: urinary tract 35% to 40% SSI: surgical wound infections 20% LRI: lower respiratory tract 15% BSI: bloodstream infections 5% to 10%
Devices related: various catheters, tubes, etc.Device days —risk adjustment of nosocomial infection
rates (ICU)

EPIDEMIOLOGY CHARACTERISTICS OF NOSOCOMIAL INFECTIONS(2)
Predominant Pathogens

EPIDEMIOLOGY CHARACTERISTICS OF NOSOCOMIAL INFECTIONS(3)
Predominant Pathogens
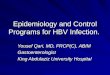
NNIS :ICU
Jan 1986-Apr 1997 Infection Site Pathogen Percentag
e
Bloodstream CoNS 33.5
S. aureus 13.4
Enterococcus spp.
12.8
C. albicans 5.8
Enterobacter spp. 5.2
Pneumonia P. aeruginosa 17.4
S. aureus 17.4
Enterobacter spp. 11.4
K. pneumoniae 6.7
H. influenzae 4.9

Infection Site Pathogen Percentage
Surgical Site Enterococcus spp.
15.3
CoNS 12.6
S. aureus 11.2
P. aeruginosa 10.3
Enterobacter spp. 9.5
Urinary Tract
E. coli 19.2
C. albicans 14.4
Enterococcus spp.
14.1
P. aeruginosa 11.2
K. pneumoniae 5.8
Predominant Pathogens
NNIS :ICU
Jan 1986-Apr 1997
EPIDEMIOLOGY CHARACTERISTICS OF NOSOCOMIAL INFECTIONS(4)

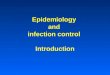
EPIDEMIOLOGY CHARACTERISTICS OF NOSOCOMIAL INFECTIONS(5)
NNIS, ICU, HA-Candidemia, 1989-1999

The Hospital Infection Control Program surveillance of nosocomial infections continuing education of medical staff control of infectious diseases outbreaks protection of employees from infection advice on new products and procedures timely feedback of infection rates suggestions for improvement and reemphasis of
existing infection control practices
EPIDEMIOLOGY CHARACTERISTICS OF NOSOCOMIAL INFECTIONS(6)

The Hospital Infection Control Program Device days — risk adjustment of nosocomial
infection rates (ICU)• CAUTI: urinary catheter-associated urinary tract
infection• CLAB: central line-associated bloodstream infection• VAP: ventilator-associated pneumonia
EPIDEMIOLOGY CHARACTERISTICS OF NOSOCOMIAL INFECTIONS(7)

The Hospital Infection Control Program Surveillance -- essential • Limited resources focused in the highest risk areas
(ICUs, hematology-oncology, burn units, organ transplant wards)
• various screens :
microbiology reports, nursing care plans, antibiotic orders, and discharge diagnoses
EPIDEMIOLOGY CHARACTERISTICS OF NOSOCOMIAL INFECTIONS(8)

The Hospital Infection Control Program Review of microbiology reports ward-based, laboratory-based linking data from• pharmacy (antimicrobial use) • laboratory • Radiology• billing (diagnostic codesnursing notes (temperature
charts, care plans)
EPIDEMIOLOGY CHARACTERISTICS OF NOSOCOMIAL INFECTIONS(9)

The Hospital Infection Control Program sensitivity and specificity • frequency of culturing • quality of the specimens
Optimal surveillance a combination of all the above data charts deserve further review
EPIDEMIOLOGY CHARACTERISTICS OF NOSOCOMIAL INFECTIONS(10)

MICROBIOLOGY TESTING IN NOSOCOMIAL INFECTION(1)
Specimens Collection
nosocomial pathogens
colonizing organisms
colonizing organisms

Specimens Collection inappropriate specimens • wrong transport media • leaking containers • undue delay from collection to transport
accurate, least misleading microbiological data • monitoring of specimen quality • enforcement of strict criteria for acceptance
MICROBIOLOGY TESTING IN NOSOCOMIAL INFECTION (2)

MICROBIOLOGY TESTING IN NOSOCOMIAL INFECTION (3)
Accurate Identification of Nosocomial Pathogens capability to identify microorganisms to species level • Conventional identification methods• automated commercial systems • unusual nosocomial pathogens: send to a reference
laboratory

MICROBIOLOGY TESTING IN NOSOCOMIAL INFECTION (4)
Accurate Identification of Nosocomial Pathogens

MICROBIOLOGY TESTING IN NOSOCOMIAL INFECTION(5)
Antimicrobial Susceptibility Testing macro- and microbroth dilution method

MICROBIOLOGY TESTING IN NOSOCOMIAL INFECTION (6)
Antimicrobial Susceptibility Testing agar dilution method

MICROBIOLOGY TESTING IN NOSOCOMIAL INFECTION(7)
Antimicrobial Susceptibility Testing disk diffusion method

MICROBIOLOGY TESTING IN NOSOCOMIAL INFECTION(8)
Antimicrobial Susceptibility Testing Etest

MICROBIOLOGY TESTING IN NOSOCOMIAL INFECTION(9)
Antimicrobial Susceptibility Testing automated commercial systems
short (3- to 5-hour) incubation periods
significant AST errors
( ESBL-producing Enterobacteriaceae, MRS, VRE, VRSA, false resistance )
• Supplement with additional methods• keep up with current literature regarding the
ability of automated systems

Resistance Patterns Testing extended-spectrum β-lactamases (ESBL) stably derepressed Bush-Jacoby-Medeiros group 1
cephalosporinases among Enterobacteriaceae glycopeptide resistance among enterococci and
staphylococci penicillin resistance among S. pneumoniae and
viridans-group streptococci
MICROBIOLOGY TESTING IN NOSOCOMIAL INFECTION (10)

Reporting of Laboratory Data direct communication between laboratory and
infection control personnel a weekly “work rounds”: • discuss areas of mutual concern • supplementary studies (molecular typing,
environmental cultures, etc.) an early phone call
MICROBIOLOGY TESTING IN NOSOCOMIAL INFECTION (11)

Reporting of Laboratory Data an early phone call• positive blood or normally sterile site cultures • smears or cultures positive for acid-fast bacilli (AFB) • isolation of Salmonella or Shigella • isolation of MRSA, VRE, etc.• detection of new or unusual pathogens (e.g., Legionella spp., vancomycin-resistant Gram-
positive organisms)
MICROBIOLOGY TESTING IN NOSOCOMIAL INFECTION(12)

Reporting of Laboratory Data a computer database facilitating retrieval and analysis • specimen type date of collection• patient identification hospital number• hospital service ward location• organisms identified specialized testing • antimicrobial susceptibility test results
establishing a baseline for nosocomial infection rates
MICROBIOLOGY TESTING IN NOSOCOMIAL INFECTION(13)

Reporting of Laboratory Data Summary antibiogram • frequency of isolation of nosocomial pathogens
by anatomical site
by hospital service • empiric antimicrobial therapy
MICROBIOLOGY TESTING IN NOSOCOMIAL INFECTION (14)

Organism Storage isolates from normally sterile sites important antibiotic-resistant organisms from any site
(MRSA, VRE, ESBL-producing Enterobacteriaceae) epidemiologically important pathogens (e.g., M.
Tuberculosis)
3 to 5 years
MICROBIOLOGY TESTING IN NOSOCOMIAL INFECTION (15)

OUTBREAK RECOGNITION AND INVESTIGATION (1)
infection control committee • detects an outbreak of nosocomial infection• define the extent of the outbreak • learn the mode of transmission • institute appropriate control measures
clinical microbiology laboratory: support

Communication
infection control practitioners
& Laboratory personnel• outbreak types in the past• laboratory resources required in the future• extra costs
OUTBREAK RECOGNITION AND INVESTIGATION (2)

Problem 1: the number of cases necessary to constitute an outbreak
• organism• patient population• institution
Problem 2: pseudo-outbreak • misdiagnosis • misinterpretation of epidemiologic data
OUTBREAK RECOGNITION AND INVESTIGATION (3)

Quality control problems • contamination of strain preparation reagents • false antimicrobial susceptibility test results • culture specimen contamination
Resolvent• Care attention to quality control • sterile technique • construction controls
OUTBREAK RECOGNITION AND INVESTIGATION (4)

MOLECULAR TYPING IN THE OUTBREAKING SETTING (1)
hospital epidemiology • clinical setting • species identification an epidemiologic link • Antibiogram
phenotypic typing methods • AST• biochemical profiles • bacteriophage susceptibility patterns • multilocus enzyme electrophoresis profiles

epidemiologic objectives • etermination of the source and extent • the mode of transmission • efficacy of preventative measures • monitoring of infection in high risk areas
genotypic typing methods
MOLECULAR TYPING IN THE OUTBREAKING SETTING(2)

MOLECULAR TYPING IN THE OUTBREAKING SETTING(3)
genotypic typing methods Plasmid fingerprinting

MOLECULAR TYPING IN THE OUTBREAKING SETTING(4)
genotypic typing methods Restriction endonuclease analysis of chromosomal
DNA with conventional electrophoresis

MOLECULAR TYPING IN THE OUTBREAKING SETTING (5)
genotypic typing methods
Restriction-fragment length polymorphism (RFLP) analysis with nucleic acid probes

MOLECULAR TYPING IN THE OUTBREAKING SETTING(6)
genotypic typing methods Pulsed-field gel electrophoresis

MOLECULAR TYPING IN THE OUTBREAKING SETTING(7)
genotypic typing methods Polymerase chain reaction (e.g., RAPD, rep-PCR,
CFLP, AFLP)

CULTRUES OF HOSPITAL PERSONNEL AND ENVIRONMENT (1)
Only when involvement in transmission of a nosocomail pathogen.
• Blood products• Parenteral fluids and intravenous devices • Environmental surfaces • Tubes and containers • Disinfectants and Antiseptics
• Respiratory therapy equipment• Air • Water and ice • Hands of personnel • Anterior nares of personnel

hand of healthcare workers • an important vehicle for transmission • confirming the mechanism of cross-infection • Culture method: broth-bag technique
anterior nares • usual reservoir for S. aureus (including MRSA)
colonization
CULTRUES OF HOSPITAL PERSONNEL AND ENVIRONMENT (2)

Result interpretation finding the outbreak strain
does not establish the direction of transmission or definitively implicate the health care worker as the source or reservoir for the outbreak
Indiscriminate culturing confusing results ill will toward the infection control program
CULTRUES OF HOSPITAL PERSONNEL AND ENVIRONMENT(3)

routine monitoring • sterilization • infant formula • other hospital-prepared products • blood components prepared in an “open” system • hemodialysis fluid • disinfected equipment
Others should not be performed.
CULTRUES OF HOSPITAL PERSONNEL AND ENVIRONMENT (4)

CONCLUSION
Clinical microbiology laboratory --an essential component
Ongoing cooperation and collaboration between the laboratory and the infection–control personnel
Appropriate application of the newer methods for detection, identification, and typing of nosocomial pathogens