Embed Size (px)
Citation preview
94
Introduction
The Diabetes Control and Complications Trial1,2 andUnited Kingdom Prospective Diabetes Study3,4
have forced diabetes educators and care providers
to reconsider the kind and quality of educationservices offered. Patient education designed toimprove knowledge, skills, and attitudes is appro-priate at times but is clearly insufficient to promote
The Journal of Continuing Education in the Health Professions, Volume 22, pp. 94–102. Printed in the U.S.A. Copyright © 2002 The Alliancefor Continuing Medical Education, the Society for Academic Continuing Medical Education, and the Council on CME, Association forHospital Medical Education. All rights reserved.
Original Article
Improving the Skills of Health Professionals in EngagingPatients in Diabetes-Related Problem Solving
Elaine Boswell King, MSN, RN, CS, CDE, David G. Schlundt, PhD, James W. Pichert, PhD, Charles K. Kinzer, PhD, and Barbara A. Backer, MD
Abstract
Introduction: Despite instruction, many patients do not employ diabetes-related self-man-agement skills recommended by health professionals. One problem suggested by research isthat many health professionals do not often use teaching and counseling skills widely con-sidered to be effective. Among these are specific skills that help health professionals conductadherence-related assessments, brainstorm workable solutions to obstacles, collaborate duringlong-term follow-up, and provide effective direct instruction.
Methods: “Effective Patient Teaching and Problem Solving” was developed and taught in ablock of 24 hours over 3 days to groups of health professionals. Course content emphasized13 operationally defined skills in four major categories: (A) assessment, (B) brainstorming,(C) collaboration, and (D) direct instruction skills. To evaluate participants’ (n = 33) use ofthe various skills, a standardized patient teaching exercise was videotaped at both the begin-ning and end of the course.
Results: Total mean scores increased significantly (t = 7.7, p < .001) from 1.8 to 2.5 on a scalethat ranged from 1 to 5. Skills improved in all four major categories (p < .003). The length ofteaching sessions did not change, lasting 13.2 minutes before the course and 13.6 minutesafter the intervention.
Discussion: Health professionals play a crucial role in patient education but rarely receivetraining in effective teaching and counseling techniques. The “Effective Patient Teaching andProblem Solving” course improved several kinds of important skills. As standards of diabetescare for improved glycemic control become more widespread, and as health providers attemptnot just to teach but also to help patients overcome considerable obstacles to consistent dia-betes self-management, a premium will be placed on the ability of health professionals tocounsel efficiently and effectively.
Key Words: Education, medical, continuing, diabetes, evaluation, patient counseling, patienteducation, problem solving, teaching skills
Ms. King and Drs. Schlundt and Pichert: VanderbiltUniversity Diabetes Research and Training Center,Nashville, Tennessee; Dr. Kinzer: Vanderbilt University,Nashville, Tennessee; Dr. Backer: Department of InternalMedicine, Rush-Presbyterian-St. Luke’s Medical Center,Chicago, Illinois.
Reprint requests: Elaine Boswell King, MSN, RN, CS,CDE, Vanderbilt Diabetes Research and Training Center,315 Medical Arts Building, 1211 21st Avenue South,Nashville, TN 37212.

the lifestyle and behavior changes that are the sinequa non of modern diabetes management.5,6 Unfor-tunately, many health professionals fail to use basicteaching techniques such as clarifying objectivesand evaluating patient learning to help patientslearn their therapeutic regimens.7 In addition, healthprofessionals do not routinely engage patients andfamilies in brainstorming and problem solvingthat can help patients cope with obstacles to self-management that hinder achievement of their ther-apeutic goals.8,9 These instructional lapses mayoccur because the specific skills that educatorsneed for fostering ongoing behavior change haveneither been well defined nor routinely empha-sized either in undergraduate health professionstraining or continuing education programs.10–13
This article discusses a continuum of teachingskills that educators can use to help patients achievetheir goals and to present an evaluation of a con-tinuing education workshop designed to train edu-cators to use those skills.
Course Description
“Effective Patient Teaching and Problem Solving”(EPT-PS) is a 24-hour continuing education coursedeveloped at the Diabetes Research and TrainingCenter (DRTC) at Vanderbilt University School ofMedicine. It is the successor to “EPT,” which,from 1983 to 1996, was offered to undergraduatemedical, nursing, and dietetic students14,15 and topracticing health professionals.16–18 Evaluationsof the original EPT program demonstrated that par-ticipants’ didactic teaching skills changed,14,19
changes translated to the practice environment,20
changes persisted for at least several months,21 andEPT could be effectively disseminated at otherinstitutions.22–24
Despite these successes, evaluations alsoshowed that EPT did not result in meaningfulimprovement in participants’use of teaching tech-niques thought to help patients make lifestylechanges.17,21–23 Specifically, course participantswere no more likely after taking EPT to engagepatients and families in negotiating treatment
plans, formulate behavioral plans by obtainingpatient preferences and input, or foster account-ability for professional and patient assessment ofpatient performance of the treatment plan’s vari-ous elements. We concluded that EPT needed toprovide greater time to and emphasis and practiceon teaching skills that foster behavior changes. Inaddition, examination of EPT course content andthe considerable literature on problem solving25–27
led us to conclude that the specific skills educa-tors need to apply those strategies had not been suf-ficiently well defined.28–30
This recognition forced us to reconsider therange of specific skills that health educators needfor teaching patients with chronic diseases like dia-betes. We now conceive of patient education as acontinuum, from direct, didactic instruction onone end to patient-initiated problem solving on theother (Fig. 1). On the left side of the continuum,instructional power is concentrated in the handsof the health professional, as when a new diagnosisrequires that survival skills be taught. Under suchcircumstances, a spirit of paternalistic concernfor the patient provides educational impetus fordirect instruction. At this end of the continuum,direct instruction is the educational vehicle ofchoice because assessment has revealed that thepatient lacks knowledge, the problem is straight-forward, there is one best solution, the patientlacks the cognitive capacity to problem solve, or,despite the educator’s best attempts, the patientchooses not to engage in problem solving.
On the right side of the teaching continuum,instructional power is almost entirely in the handsof the patient who chooses to take independent self-care actions but uses health professionals as con-sultants. A spirit of support for the patient provideseducational impetus for ongoing problem solving.At this end of the continuum, problem solving isthe educational vehicle of choice because assess-ment has revealed that the patient has decided tomake changes, desires a plan for better health,and wants to be involved in decision making forwhich one best answer or strategy exists for han-dling the problem. Most important, the patient
95
King et al.

has to make complex self-care decisions in situ-ations for which health professional guidance isnot readily available.
Most persons with diabetes need both directinstruction and engagement in problem solvingwith their health professionals.31–34 For that tohappen, diabetes educators must have skills tomove fluidly back and forth along the continuum,ever mindful of their patients’ needs and con-cerns. The middle of the continuum is thereforecharacterized by active exchange of ideas, explic-itly negotiated goals and objectives, and sharedpower and influence that serve patients’ interestsand foster patient self-management and long-termbehavior change.
With the concept of the teaching continuumin mind, we asked what specific skills educatorsneed to meet patients’ needs. We reached twoconclusions: direct instruction skills useful foraccomplishing goals suggested by the left half ofthe continuum had been well defined and could betaught,14–24,35,36 but specific, operationally definedskills for engaging patients in problem solvinghad not. Defining those skills was accomplishedvia a systematic process of literature review, solic-itation of advice from experts who had publishedresearch articles about problem solving in dia-betes, and statistical analysis of professional judg-ments about the skills (The process will bedescribed in detail elsewhere.)
96
Improving Problem-Solving Skills
Figure 1 Patient education: a continuum from direct instruction to independent problem solving. HCP = health
care professional.
HCP Takes Initiative
Information Transmission
Do Direct InstructionIf assessment reveals:
• Patient lacks knowledge andcontent is better taught using directinstruction
• Problem is well defined, simple,straightforward
• Only one best answer or strategyto address patient problem
• Patient not capable of engaging inproblem solving
• Patient chooses not to be involved• This is a “one-shot deal”• There are severe time limitations
(not to be overused!)
Collaboration
Enhanced Autonomy
Do Direct InstructionAND Problem Solving
To help most patients changebehaviors and achieve theirtherapeutic goals, there will be timesfor teaching AND problem solving;the educator will move fluidly backand forth along the continuum.
Patients and HCPs actively exchangeideas, explicitly negotiate goals andobjectives, and share power andinfluence to serve the patient’sinterests and foster patientself-management and behaviorchange.
Patient Takes Initiative, Choices
Greater Independence
Do Problem SolvingIf assessment reveals:
• Patient has decided to makechange(s)
• Patient wants a plan for betterhealth
• Patient wants to be involved indecision making
• Patient is ready to implementchanges and wants help decidinghow
• Patient wants or already hasspecific plans but is encounteringobstacles
• Problem-solving approach is betterfor achieving goals
• There is more than one “best”answer or strategy to solveproblems
• Patient has to make complexdecisions in situations for whichhelp is not available

Table 1 presents four major skill categories and13 specific skill sets that emerged. Operational def-initions of each skill have been developed. Assess-ment skills are important across the entire con-tinuum and revolve around information gathering,gaining patients’ confidence, and defining andexploring patients’ goals and obstacles. An edu-cator’s brainstorming skills help patients identifystrategies for changing behaviors, overcome bar-riers, and handle lapses. The collaboration skillsfoster mutual evaluation, feedback, and account-ability throughout a long-term patient-professionalrelationship. Finally, direct instruction skills helppatients learn and recall diabetes-related contenttaught via direct instruction.
The EPT-PS course method involves facultymodeling and demonstration, participant practice,and group feedback. Videotaped mock teachingsessions of 3 to 10 minutes duration are conductedusing the principles of microteaching.37 Participantsin EPT-PS are encouraged to target a few teach-
ing skills in each practice teaching session. Video-tapes are replayed the same day, and other par-ticipants are encouraged to join faculty in providingcompassionate peer review in which actual per-formances are compared with definitions of eachskill. With another course participant role-playinga surrogate patient, each participant performs onepractice teaching session for each of the fourmajor skills categories and a final, more lengthypractice session to “put it all together.” Thesepractice teaching and critique sessions consumeabout half of the course time.
Of interest were evaluations of educators’problem-based teaching skills, use of problem-based teaching skills, and amount of time spent inproblem-solving activities. The following researchquestions were defined:
• Question 1: Do total teaching skills scoresimprove from before to after EPT-PS?
• Question 2: Do skills scores improve in each ofthe four major categories?
• Question 3: Does the length of teaching sessionschange from before to after the course?
The authors’ Institutional Review Boardapproved the project.
Subjects and Design
Thirty-three health professionals (30 nurses anddietitians, 2 physicians, and 1 pharmacist) partic-ipated in the evaluation of EPT-PS. These personsattended EPT-PS programs in Nashville, Ten-nessee, or Toronto, Ontario. To evaluate partici-pants’use of various skills, informed consent wasobtained for videotaping a standardized patientteaching exercise at both the beginning and endof the course.
The standardized patient case involved “JaneSmith,” a 21-year-old female college student withsystemic lupus erythematosis, who has been expe-riencing frequent symptom flare-ups related toregimen nonadherence. Lupus was chosen toreduce knowledge disparities among diabetes edu-
97
King et al.
Table 1 Four Major Skill Categories and 13 Specific Skill Sets
A. Assessment1. Information gathering/patient facilitation2. Formulating hypotheses and identifying
patient barriers to regimen adherence3. Negotiating realistic behavioral goals
B. Brainstorming4. Getting ideas on the table5. Narrowing the list6. Identifying strategies for gaining, maintain-
ing commitment to behavior change7. Preventing relapse
C. Collaboration8. Evaluation9. Feedback
10. Follow-upD. Direct Instruction
11. Openings12. Highlighting main messages, gaining active
learner involvement13. Closure/homework

cator course participants. Lupus was also chosenas the disease state because, like diabetes, its con-trol involves daily attention to a variety of self-management behaviors. These circumstances helpparticipants concentrate on issues of behaviorchange during the course rather than content.
University students with interests in behavioralmedicine and health psychology were recruitedand trained to play the role of Jane. They were givena substantial medical and social history to memo-rize, which included such issues as medicationnonadherence, stressful life circumstances relatedto academic and social pressures, less than ideal eat-ing patterns, smoking, and occasional binge drink-ing. These factors are known to aggravate lupus.
Participants in the EPT-PS course wereinstructed to help Jane identify changes she canmake that will give her relief from lupus symptomsand help prevent the recurrence of flare-ups. Noother instructions were provided, so participantswere left to approach the task as they might per-form it in a clinical situation. Participants weregiven approximately 15 minutes for counselingJane. Sessions were videotaped.
Scoring
Videotaped interviews were rated in random orderby three trained raters, who demonstrated an inter-rater reliability of 0.87. Raters were blinded as towhether interviews were taped at the beginning orend of the course. After watching each videotape,raters gave each of the 13 skills a score from 1(low) to 5 (high). For example, one skill involvesidentifying specific barriers that reduce the patient’slevel of adherence to the therapeutic plan. Thehealth professional receives a score of 1 if he orshe starts teaching after discovering the patient’sfirst problem without assessing whether other bar-riers might also contribute to the problem. At theother end of the scale, the participant scores a 5if he or she assesses overall adherence, checks forthe presence of several barriers, and summarizeshis or her comprehension of the situation for thepatient.
Using more teaching and counseling strategiesyields higher scores for each of the skills. How-ever, each skill would not be observed in every ses-sion because each session is individualized. Inother words, high ratings on every skill were notexpected. Course developers consider a score of3 on each skill to reflect a basic level of use of eachskill.
Results
Evaluation of the EPT-PS program has includedassessments of student satisfaction and of gains inteaching skills. Participants’ ratings on a satis-faction questionnaire administered at the end of thecourse for CEU purposes have been uniformlyenthusiastic.
The results are based on a final n = 31. Oneparticipant dropped out of the course after thefirst day and one participant arrived at the courseafter the precourse videotaping.
In analyzing the data, three questions wereasked. First, did total overall skill scores improvefrom before to after the EPT course (Fig. 2)? Meanscores before and after the course were comparedusing paired t tests. Possible scores range from 1to 5. Mean scores increased from 1.8 before thecourse to 2.5 after the course (t = 7.7, p < .001).Second, do skills scores improve in each of the four
98
Improving Problem-Solving Skills
Figure 2 Total teaching skills scores before and
after “Effective Patient Teaching and Problem
Solving” (EPT-PS). Possible scores range from
1 to 5; t = 7.7, p < .001.
Tota
l Tea
chin
gS
kills
Sco
res
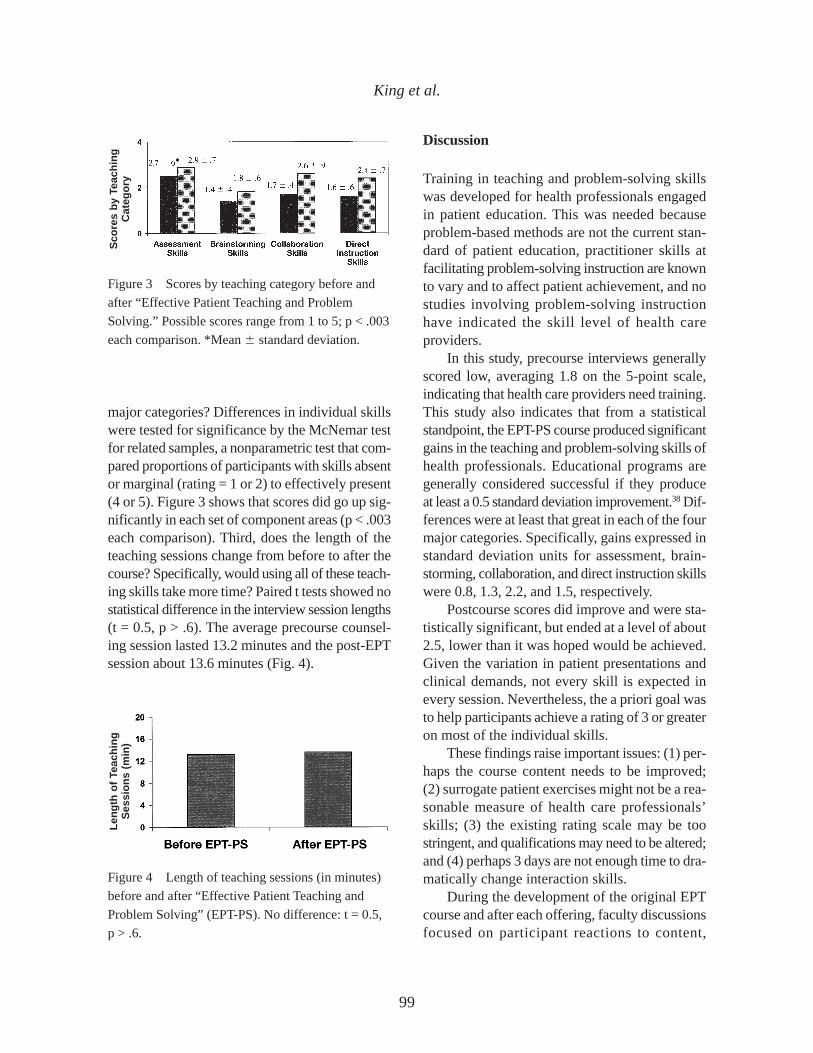
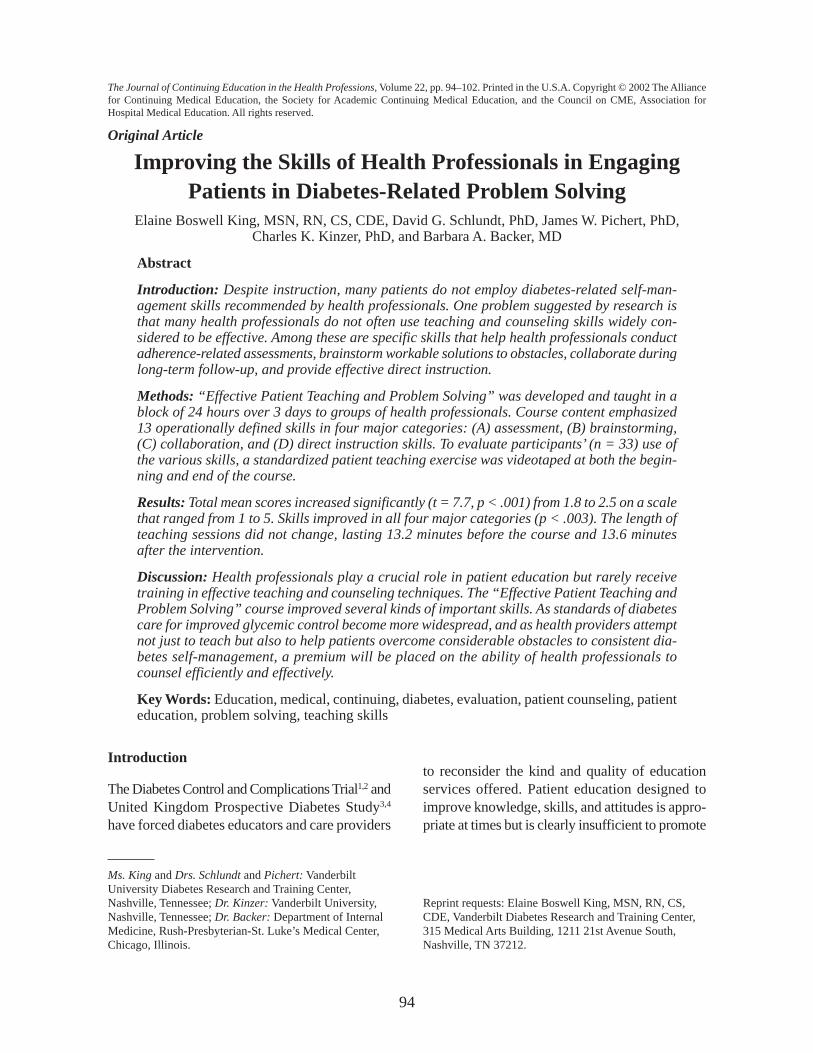
major categories? Differences in individual skillswere tested for significance by the McNemar testfor related samples, a nonparametric test that com-pared proportions of participants with skills absentor marginal (rating = 1 or 2) to effectively present(4 or 5). Figure 3 shows that scores did go up sig-nificantly in each set of component areas (p < .003each comparison). Third, does the length of theteaching sessions change from before to after thecourse? Specifically, would using all of these teach-ing skills take more time? Paired t tests showed nostatistical difference in the interview session lengths(t = 0.5, p > .6). The average precourse counsel-ing session lasted 13.2 minutes and the post-EPTsession about 13.6 minutes (Fig. 4).
Discussion
Training in teaching and problem-solving skillswas developed for health professionals engagedin patient education. This was needed becauseproblem-based methods are not the current stan-dard of patient education, practitioner skills atfacilitating problem-solving instruction are knownto vary and to affect patient achievement, and nostudies involving problem-solving instructionhave indicated the skill level of health careproviders.
In this study, precourse interviews generallyscored low, averaging 1.8 on the 5-point scale,indicating that health care providers need training.This study also indicates that from a statisticalstandpoint, the EPT-PS course produced significantgains in the teaching and problem-solving skills ofhealth professionals. Educational programs aregenerally considered successful if they produceat least a 0.5 standard deviation improvement.38 Dif-ferences were at least that great in each of the fourmajor categories. Specifically, gains expressed instandard deviation units for assessment, brain-storming, collaboration, and direct instruction skillswere 0.8, 1.3, 2.2, and 1.5, respectively.
Postcourse scores did improve and were sta-tistically significant, but ended at a level of about2.5, lower than it was hoped would be achieved.Given the variation in patient presentations andclinical demands, not every skill is expected inevery session. Nevertheless, the a priori goal wasto help participants achieve a rating of 3 or greateron most of the individual skills.
These findings raise important issues: (1) per-haps the course content needs to be improved;(2) surrogate patient exercises might not be a rea-sonable measure of health care professionals’skills; (3) the existing rating scale may be toostringent, and qualifications may need to be altered;and (4) perhaps 3 days are not enough time to dra-matically change interaction skills.
During the development of the original EPTcourse and after each offering, faculty discussionsfocused on participant reactions to content,
99
King et al.
Figure 3 Scores by teaching category before and
after “Effective Patient Teaching and Problem
Solving.” Possible scores range from 1 to 5; p < .003
each comparison. *Mean � standard deviation.
Figure 4 Length of teaching sessions (in minutes)
before and after “Effective Patient Teaching and
Problem Solving” (EPT-PS). No difference: t = 0.5,
p > .6.
Len
gth
of
Teac
hin
gS
essi
on
s (m
in)
Sco
res
by
Teac
hin
gC
ateg
ory

adequacy of time allotted to each topic, and qual-ity of our own presentations, such as how well theyexemplified effective teaching. Each critique sug-gested course modifications, all of which wereincorporated and tested in subsequent presenta-tions. Most likely, revisions and refinements of thiscurrent EPT-PS course would also enhance theimpact on health professionals’use of teaching andproblem-solving skills. Empiric observations alsoled us to suspect that 3 days are not enough timeto dramatically change interaction skills and habitsthat have developed over years of health carepractice.
Finally, the question arose as to whether usingadditional teaching skills would take more time—a realistic concern when patients may be waitingin a waiting room. After all, if using the skillsrequires substantially more time, that would be amajor barrier to their use in the increasingly busyworld of clinical practice. With the increase inskills used without an increase in time spent, weconclude that these skills do not necessarily bur-den health care providers.
Limitations and Possible Future Studies
This study’s limitations include its pretest/post-test design, in which participants served as theirown controls. Second, although not observed inour previous research using similar methods,17,22
videotaping may have affected participants’ coun-seling behaviors. Next, this was a short-term,classroom-based, standardized-patient study thatprecluded knowing effects on actual patients inclinical settings. Finally, we do not know what lev-els of skills are needed to achieve desired patientoutcomes. Nevertheless, we have made substan-tial progress in determining what skills are impor-tant and in learning how to teach them to healthprofessionals.
Possible future studies include study replica-tion, including a control group, determining ifresults of training last, and identifying ways toimprove training. Potential research also includesmeasuring the skill levels of practicing profes-
sionals, evaluating whether some skills are moreimportant than others, and assessing whetherimproved problem-solving skills have an impacton patient behavior and health care outcomes.
Conclusion
Health care providers play a crucial role in patienteducation but rarely receive training in effectiveteaching techniques. This study found that healthcare providers who take the course “EffectivePatient Teaching and Problem Solving” showedimprovements in the four main counseling skillscategories. The data also raise important ques-tions about whether the gains are satisfactory orsufficient.
As standards of diabetes care for improvedglycemic control become more widespread, andas health professionals attempt not just to teach butalso to help patients overcome considerable obsta-cles to consistent diabetes self-management, apremium will be placed on the ability of health pro-fessionals to counsel efficiently and effectively. TheVanderbilt DRTC has initiated a program of
100
Improving Problem-Solving Skills
Lessons for Practice
• Health professionals who take thecourse “Effective Patient Teaching andProblem Solving” show improvementsin four counseling skills categories:assessment, brainstorming, collabora-tion, and direct instruction skills.
• Health professionals can increase theiruse of teaching and problem-solvingskills without increasing the length oftime spent in patient education sessions.
• More research is needed to addresssatisfactory gains in diabetes-relatedproblem solving.
101
King et al.
research and development to learn more aboutthese issues.
Acknowledgment
This research was supported by National Institutesof Health Grant No. P60 DK 20593.
References
1. Diabetes Control and Complications Trial(DCCT) Research Group. The effect of inten-sive treatment of diabetes on the developmentand progression of long-term complications ininsulin-dependent diabetes mellitus. N Engl JMed 1993; 329:977–986.
2. American Diabetes Association. Implicationsof the Diabetes Control and ComplicationsTrial. Diabetes Care 2002; 25(Suppl 1):S25–S27.
3. U.K. Prospective Diabetes Study Group.Intensive blood-glucose control with sulpho-nylureas or insulin compared with convention-al treatment and risk of complications inpatients with type 2 diabetes. Lancet 1998;352:837–853.
4. American Diabetes Association. Implicationsof the United Kingdom Prospective DiabetesStudy. Diabetes Care 2002; 25(Suppl 1):28–32.
5. Clement S. Diabetes self-management.Diabetes Care 1995; 18:1204–1214.
6. Hunt LM, Pugh J, Valenzuela M. Howpatients adapt diabetes self-care recommenda-tions in everyday life. J Fam Pract 1998;46:205–206.
7. Harris G, Diment A, Sulway M, Wilkinson M.Glucagon administration—underevaluated andundertaught. Pract Diab Int 2001;18(1):22–25.
8. Lorenz RA, Bubb J, Davis D, Jacobson A,Jannasch K, Kramer J, Lipps J, Schlundt D.Changing behavior: practical lessons from theDiabetes Control and Complications Trial.Diabetes Care 1996; 19:648–652.
9. Schlundt DG, Quesenberry L, Pichert JW,Lorenz RA, Boswell EJ. Evaluation of a train-
ing program for improving adherence promo-tion skills. Pat Educ Couns 1994; 24:165–173.
10. Whittemore R. Strategies to facilitate lifestylechange associated with diabetes mellitus. JNurs Scholarship 2000; 32:225–232.
11. Young-Hyman D. Provider impact in diabeteseducation: what we know, what we would liketo know, paradigms for asking. Diabetes Educ1999; 25(Suppl 1):S34–S42.
12. Larme AC, Pugh JA. Attitudes of primary careproviders toward diabetes: barriers to guide-line implementation. Diabetes Care 1998;21:1391–1396.
13. Kruijver IPM, Kerkstra A, Francke AL,Bensing JM, van de Wiel HBM. Evaluation ofcommunication training programs in nursingcare: a review of the literature. Pat EducCouns 2000; 39:129–145.
14. Lorenz RA, Pichert JW, Boswell EJ, JamisonRN, Schlundt DG. Training health professionstudents to be effective patient teachers. MedTeacher 1987; 9:403–408.
15. Schlundt DG, Quesenberry L, Pichert JW,Wolf J, Ray S, Lorenz RA, Boswell EJ.Evaluation of a training program for improv-ing adherence-promotion skills of dieteticinterns. J Am Diet Assoc 1994; 94:1421–1425.
16. Boswell EJ, Pichert JW, Lorenz RA, SchlundtDG. Training health care professionals toenhance their patient teaching skills. J NursStaff Dev 1990; 6:233–239.
17. Stetson BA, Pichert JW, Roach RR, LorenzRA, Boswell EJ, Schlundt DG. Registereddietitians’ teaching and adherence promotionskills during routine patient education. PatEduc Couns 1992; 19:273–280.
18. Boswell EJ, Lorenz RA, Pichert JW, SchlundtDG, Penha MLI. Evaluation of a home studycontinuing education program on patientteaching skills. J Contin Educ Health Prof1994; 14:155–165.
19. Boswell EJ, Pichert JW, Lorenz RA, SchlundtDG. Training health care professionals toenhance their patient teaching skills. J NursStaff Dev 1990; 6:233–239.
20. Lorenz RA, Pichert JW, Boswell EJ, SchlundtDG. Teaching skills training for health profes-
102
Improving Problem-Solving Skills
sionals: effects on immediate recall by surro-gate patients. Teach Learn Med 1989;1:26–30.
21. Roach RR, Pichert JW, Stetson BA, LorenzRA, Boswell EJ, Schlundt DG. Improvingdietitians’ teaching skills. J Am Diet Assoc1992; 92:1466–1473.
22. Pichert JW, Stetson BA, Lorenz RA, BoswellEJ, Schlundt DG, Oldham JA. Continuingeducation on teaching skills for health profes-sionals. Eval Health Prof 1993; 16:400–416.
23. Pichert JW, Roach RR, Lorenz RA, BoswellEJ, Schlundt DG. Translating the “EffectivePatient Teaching” course to a second universi-ty setting. J Nutr Educ 1994; 26:149–152.
24. Boswell EJ, Pichert JW, Lorenz RA, et al.Evaluation of a patient teaching skills coursedisseminated through staff developers. PatEduc Couns 1996;27:247–256.
25. Benjamin EM, Schneider MS, Hinchey KT.Implementing practice guidelines for diabetescare using problem-based learning. DiabetesCare 1999; 22:1672–1678.
26. Frauenknecht M, Black DR. Social problem-solving inventory for adolescents (SPSI-A):development and preliminary psychometricevaluation. J Pers Assess 1995; 64:522–539.
27. Norman GR, Schmidt HG. The psychologicalbasis of problem-based learning: a review ofthe literature. Acad Med 1992; 67:557–565.
28. Brown SA. Interventions to promote diabetesself-management: state of the science.Diabetes Educ 1999; 25(Suppl 1):52–61.
29. D’Zurilla TJ, Maydeu-Olivares A. Conceptualand methodological issues in social problem-
solving assessment. Behav Ther 1995;26:409–432.
30. Glasgow RE, Osteen VL. Evaluating diabeteseducation: are we measuring the most impor-tant outcomes? Diabetes Care 1992;15:1423–1432.
31. Quill TE, Brody H. Physician recommenda-tions and patient autonomy: finding a balancebetween physician power and patient choice.Ann Intern Med 1996; 125:763–769.
32. Kyle M. Collaboration. In: Snyder M, MirrMP, eds. Advanced practice nursing. NewYork: Springer, 1995:169–191.
33. Kaplan SH, Greenfield S, Ware JE Jr.Assessing the effects of physician-patientinteractions on the outcomes of chronic dis-ease. Med Care 1989; 27(Suppl 3):110–127.
34. Schon DA. Educating the reflective practition-er: toward a new design for teaching andlearning in the professions. San Francisco:Jossey, 1987.
35. Mensing C, Boucher J, Cypress M, et al.National standards for diabetes self-manage-ment education. Diabetes Care 2002;25(Suppl 1):S140–S147.
36. American Association of Diabetes Educators.The 1999 scope of practice for diabetes educa-tors and the standards of practice for diabeteseducators. Diabetes Educ 2000; 26:519–525.
37. Allen D, Ryan K. Microteaching. Reading,MA: Addison-Wesley, 1969.
38. Borg WR, Gall MD. Educational research anddevelopment. In: Borg WR, Gall MD, eds.Educational research. 3rd Ed. New York:Longman, 1979:623–644.





















![[Challenge:Future] Engaging Youths in Active Problem Solving & Skills Acquisition](https://img.pdfslide.us/doc/110x75/5566221dd8b42a7d608b5497/challengefuture-engaging-youths-in-active-problem-solving-skills-acquisition.jpg)






