Embed Size (px)
Citation preview

Improving the quality of endodontic record keeping through clinical auditE. King,*1 L. Shekaran2 and A. Muthukrishnan3
involved in the patient’s care. Good quality clinical records are imperative for intra- and inter-clinician communication and indispen-sable when it comes to dento-legal evidence.
Considering record keeping is such a fun-damental part of practice, there are relatively few reports in the literature concerning the standard of record keeping. In the United Kingdom, only five studies have analysed the quality of record keeping among dental prac-titioners.3–7 In all five studies the common findings included missing information and discrepancies in record keeping between practitioners. Cole and Michael6 audited clinical record keeping standards among Worcestershire dentists and as a result of the poor quality and wide variation in record keeping, the authors recommended further postgraduate education to improve standards. Pessian et al.,5 who conducted a record-keeping audit of undergraduate student notes, reported that although note keeping improved following education, missing data continued to remain a
Introduction
Clinical record keeping is an essential part of everyday clinical practice. It is clearly stated in GDC guidelines that it is the responsibil-ity of every clinician to maintain up-to-date, complete, clear, accurate and legible records.1 This is reinforced in FGDP guidelines, which states records must be legible, accurate, comprehensive and contemporaneous.2 The principal rationale for record keeping is to create a detailed account of patient manage-ment that can be reflected upon by anyone
Introduction Record keeping is an essential part of day-to-day practice and plays an important role in treatment, audit
and dento-legal procedures. Creating effective endodontic records is challenging due to the scope of information required
for comprehensive notes. Two audits were performed to assess the standards of endodontic record keeping by dentists
in a restorative dentistry department and students on an endodontic MSc course. Methods Fifty sets of departmental
records and 10 sets of student records were retrospectively evaluated against the European Society of Endodontology 2006
guidelines. Results of the first cycle of both audits were presented to departmental staff and MSc students, alongside an
educational session. Additionally, departmental guidelines, consent leaflets and endodontic record keeping forms were
developed. Both audits were repeated using the same number of records, thus completing both audit cycles. Results The
most commonly absent records included consent, anaesthetic details, rubber dam method, working length reference point,
irrigation details and obturation technique. Almost all areas of record keeping improved following the second audit cycle,
with some areas reaching 100% compliance when record keeping forms were used. Statistically significant improvements
were seen in 24 of the 29 areas in the departmental audit and 14 of the 29 areas in the MSc audit (P = 0.05). Conclusions Significant improvements in endodontic record keeping can be achieved through the provision of education, departmental
guidelines, consent leaflets and endodontic record keeping forms.
problem suggesting that education alone is not enough to improve record keeping. McAndrew et al.7 conducted an audit comparing under-graduate dental student hand-written and computer records and determined that computer records encouraged clinicians to record the correct data in comparison to paper records. It is possible that the templates used by the computer software acted as a prompt for clinicians to record the correct information. It is clear from these studies that the quality of record keeping remains a problem throughout the dental profession and further improve-ments are required.
Record keeping for endodontic treatment can be complex due to the extent of informa-tion that needs to be documented. Endodontic treatment encompasses a range of procedures intended to treat pulpal and peri-apical diseases. A vast range of materials, measure-ments, file systems and techniques are used during endodontic treatment, which all have to be recorded accurately in order to produce
1Speciality Registrar in Restorative Dentistry; 3Associate Specialist in Restorative Dentistry, Specialist in Special Care Dentistry and Oral Surgery; Morriston Hospital, Heol Maes Eglwys, Morriston, Swansea, SA6 6NL; 2Statistician, Univer-sity of Warwick, Gibbet Hill Rd, Coventry, CV4 7AL *Correspondence to: Elizabeth King Email: [email protected]
Refereed Paper. Accepted 3 January 2017 DOI: 10.1038/sj.bdj.2017.223©British Dental Journal 2017; 222: 373-380
Suggests how guidelines can be implemented in everyday practice through clinical governance, audit and quality improvement projects.
Provides an example of how the clinical audit project can significantly improve record keeping and clinical practice.
Provides an example of endodontic record keeping forms and patient information leaflets developed to encourage effective endodontic record keeping and consent process.
In briefIn brief
BRITISH DENTAL JOURNAL | VOLUME 222 NO. 5 | MARCH 10 2017 373
RESEARCH
© 2017
British
Dental
Association.
All
rights
reserved.
comprehensive notes. Endodontic treatment is seldom completed in one appointment. Therefore, it is important to be able to easily review previous records to recommence treatment without repeating or omitting treatment stages. Furthermore, when monitor-ing long-term endodontic outcomes, compre-hensive records are invaluable to refer back to in order to determine the possible causes of complications or failure. It is not uncommon for patients undergoing endodontic treatment to be seen by other practitioners should they return with pain or require treatment to be
completed by a different clinician. In these circumstances, good quality clinical records are required for a new clinician to establish what stage of treatment a patient is at. Finally, endodontic treatment is associated with several complications, for example instrument separation and perforation, thus thorough documentation of any complications that may arise during treatment is essential for dento-legal purposes.
Inevitably, the quality of endodontic treatment varies between practitioners. However, in 2006, the European Society of
Endontology (ESE) released the consensus report ‘Quality Guidelines for Endodontic Treatment’, which intended to represent current good practice and therefore standard-ise the quality of endodontic treatment within the profession.8 These guidelines, which are outlined in Box 1, contain a summary of what information should be recorded to maintain good endodontic practice.
At present no studies have investigated the quality of record keeping in endodontics. This article presents two audits concerning the quality of endodontic record keeping in a specialist department to compare current practice against the ESE guidelines.8 The aim of both audits was to identify areas of poor record keeping and implement the necessary changes to improve endodontic record keeping in the restorative department and on the MSc course.
Methodology
First audit cycleTwo retrospective audits were conducted at Morriston Hospital, Swansea. One audit was conducted in the NHS Restorative Dentistry department (audit 1) and the other on the postgraduate Endodontic Master of Science (MSc) course (audit 2). A single dentist ran both audit cycles. The proposed standard for both audits was as follows: all clinical records should conform to the endodontic record keeping standards as reported by the ESE 2006 Quality Guidelines for Endodontic Treatment with 100% compliance.
For audit 1, fifty records of patients treated between January 2012 and January 2013 in the Restorative Dentistry Department were audited. Patients who had undergone treatment in this time period were identified using the computerised national patient administration system (Mryddin). A range of clinicians’ notes were selected to be audited which included one consultant, one specialist, two staff grades, one speciality registrar (StR) and one senior house officer (SHO). To select the patient records for audit, the first ten patients who were seen from January 2012 to January 2013 were selected ret-rospectively from the consultant’s, specialist’s, StR’s and SHO’s treatment list stored on the patient administration system. For the two staff grades, the first five patients that were seen for endodontic treatment between January 2012 to January 2013 were selected for record keeping.
For audit 2, ten records of patients treated between September 2012 and August 2013 on the MSc course were audited. The patient
Fig. 1 Choosing wisely patient information leaflet developed to encourage the discussion of consent
374 BRITISH DENTAL JOURNAL | VOLUME 222 NO. 5 | MARCH 10 2017
RESEARCH
© 2017
British
Dental
Association.
All
rights
reserved. ©
2017
British
Dental
Association.
All
rights
reserved.
records were selected using archived lists of patients who had previously been treated on the course. The records of the first ten patients on the archived lists provided were selected for audit. All clinicians providing treatment were general dental practitioners.
Audit data for both audits was collected by one dentist retrospectively assessing paper clinical records. Audit data was documented as: recorded correctly (Y), not recorded (N) and not applicable to the patient’s treatment (NA). Local anaesthetic administration, rubber dam application and irrigation are procedures that are repeated at each treatment appoint-ment. Therefore, multiple entries of data were recorded for these criteria. All other criteria were recorded as a single entry of data. The
audit data was input onto and analysed using an Excel spread sheet. To determine compli-ance to standards NA scores were excluded from calculations and Y and N scores were used to calculate percentages.
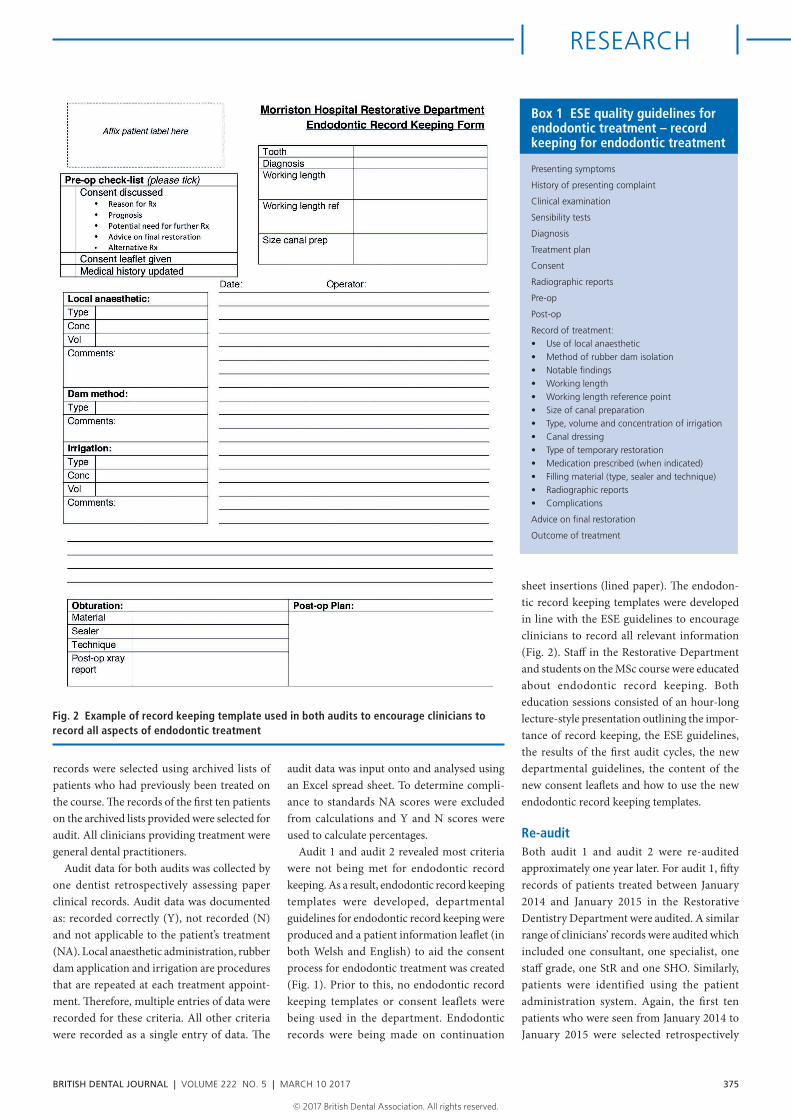
Audit 1 and audit 2 revealed most criteria were not being met for endodontic record keeping. As a result, endodontic record keeping templates were developed, departmental guidelines for endodontic record keeping were produced and a patient information leaflet (in both Welsh and English) to aid the consent process for endodontic treatment was created (Fig. 1). Prior to this, no endodontic record keeping templates or consent leaflets were being used in the department. Endodontic records were being made on continuation
sheet insertions (lined paper). The endodon-tic record keeping templates were developed in line with the ESE guidelines to encourage clinicians to record all relevant information (Fig. 2). Staff in the Restorative Department and students on the MSc course were educated about endodontic record keeping. Both education sessions consisted of an hour-long lecture-style presentation outlining the impor-tance of record keeping, the ESE guidelines, the results of the first audit cycles, the new departmental guidelines, the content of the new consent leaflets and how to use the new endodontic record keeping templates.
Re-auditBoth audit 1 and audit 2 were re-audited approximately one year later. For audit 1, fifty records of patients treated between January 2014 and January 2015 in the Restorative Dentistry Department were audited. A similar range of clinicians’ records were audited which included one consultant, one specialist, one staff grade, one StR and one SHO. Similarly, patients were identified using the patient administration system. Again, the first ten patients who were seen from January 2014 to January 2015 were selected retrospectively
Fig. 2 Example of record keeping template used in both audits to encourage clinicians to record all aspects of endodontic treatment
Presenting symptoms
History of presenting complaint
Clinical examination
Sensibility tests
Diagnosis
Treatment plan
Consent
Radiographic reports
Pre-op
Post-op
Record of treatment:• Use of local anaesthetic• Method of rubber dam isolation• Notable findings• Working length• Working length reference point• Size of canal preparation• Type, volume and concentration of irrigation• Canal dressing• Type of temporary restoration• Medication prescribed (when indicated)• Filling material (type, sealer and technique)• Radiographic reports• Complications
Advice on final restoration
Outcome of treatment
Box 1 ESE quality guidelines for endodontic treatment – record keeping for endodontic treatment
BRITISH DENTAL JOURNAL | VOLUME 222 NO. 5 | MARCH 10 2017 375
RESEARCH
© 2017
British
Dental
Association.
All
rights
reserved. ©
2017
British
Dental
Association.
All
rights
reserved.
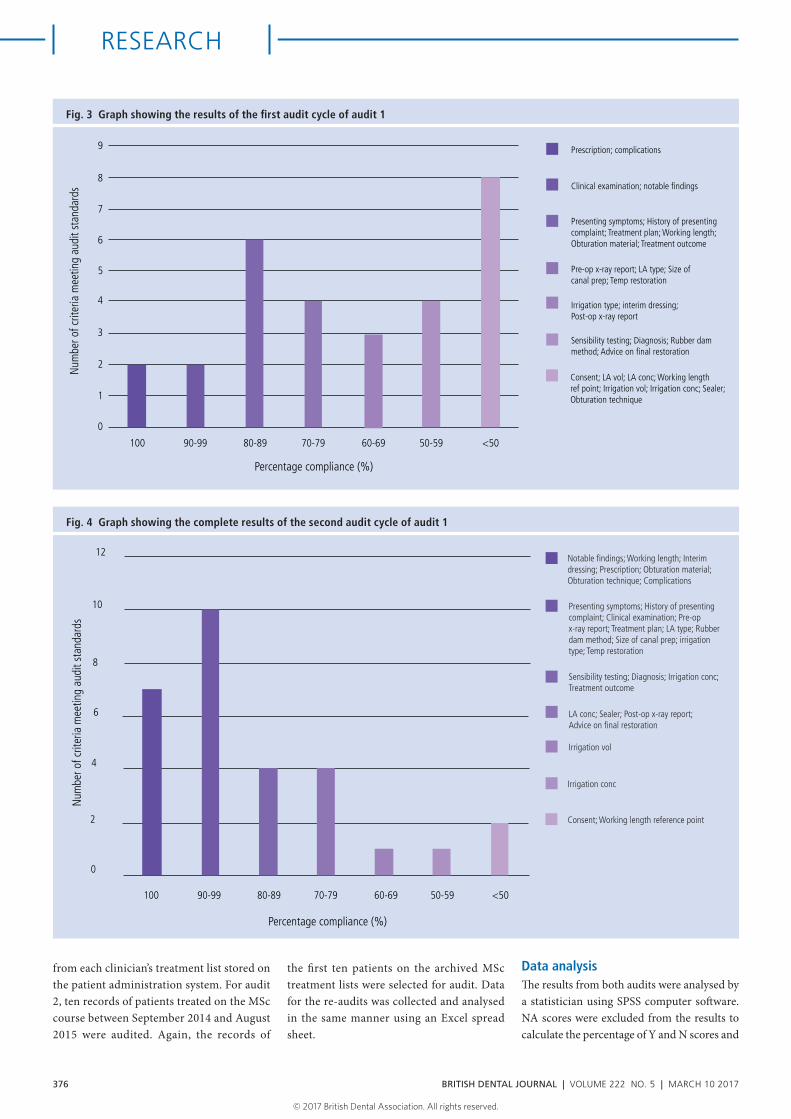
Fig. 3 Graph showing the results of the first audit cycle of audit 1
from each clinician’s treatment list stored on the patient administration system. For audit 2, ten records of patients treated on the MSc course between September 2014 and August 2015 were audited. Again, the records of
the first ten patients on the archived MSc treatment lists were selected for audit. Data for the re-audits was collected and analysed in the same manner using an Excel spread sheet.
Data analysisThe results from both audits were analysed by a statistician using SPSS computer software. NA scores were excluded from the results to calculate the percentage of Y and N scores and
Num
ber o
f crit
eria
mee
ting
audi
t sta
ndar
ds
9
8
7
6
5
4
3
2
1
0
100 90-99 80-89 70-79 60-69 50-59 <50
Percentage compliance (%)
Prescription; complications
Clinical examination; notable findings
Presenting symptoms; History of presentingcomplaint; Treatment plan; Working length;Obturation material; Treatment outcome
Pre-op x-ray report; LA type; Size ofcanal prep; Temp restoration
Irrigation type; interim dressing;Post-op x-ray report
Sensibility testing; Diagnosis; Rubber dammethod; Advice on final restoration
Consent; LA vol; LA conc; Working lengthref point; Irrigation vol; Irrigation conc; Sealer;Obturation technique
Fig. 4 Graph showing the complete results of the second audit cycle of audit 1
12
10
8
6
4
2
0
100 90-99 80-89 70-79 60-69 50-59 <50
Percentage compliance (%)
Num
ber o
f crit
eria
mee
ting
audi
t sta
ndar
ds
Notable findings; Working length; Interimdressing; Prescription; Obturation material;Obturation technique; Complications
Presenting symptoms; History of presentingcomplaint; Clinical examination; Pre-opx-ray report; Treatment plan; LA type; Rubberdam method; Size of canal prep; irrigationtype; Temp restoration
Sensibility testing; Diagnosis; Irrigation conc;Treatment outcome
LA conc; Sealer; Post-op x-ray report;Advice on final restoration
Irrigation vol
Irrigation conc
Consent; Working length reference point
376 BRITISH DENTAL JOURNAL | VOLUME 222 NO. 5 | MARCH 10 2017
RESEARCH
© 2017
British
Dental
Association.
All
rights
reserved. ©
2017
British
Dental
Association.
All
rights
reserved.
therefore compliance to the audit standards. To assess whether there were any statistically sig-nificant differences between data sets, aPvalue was set a P = 0.05.
Results
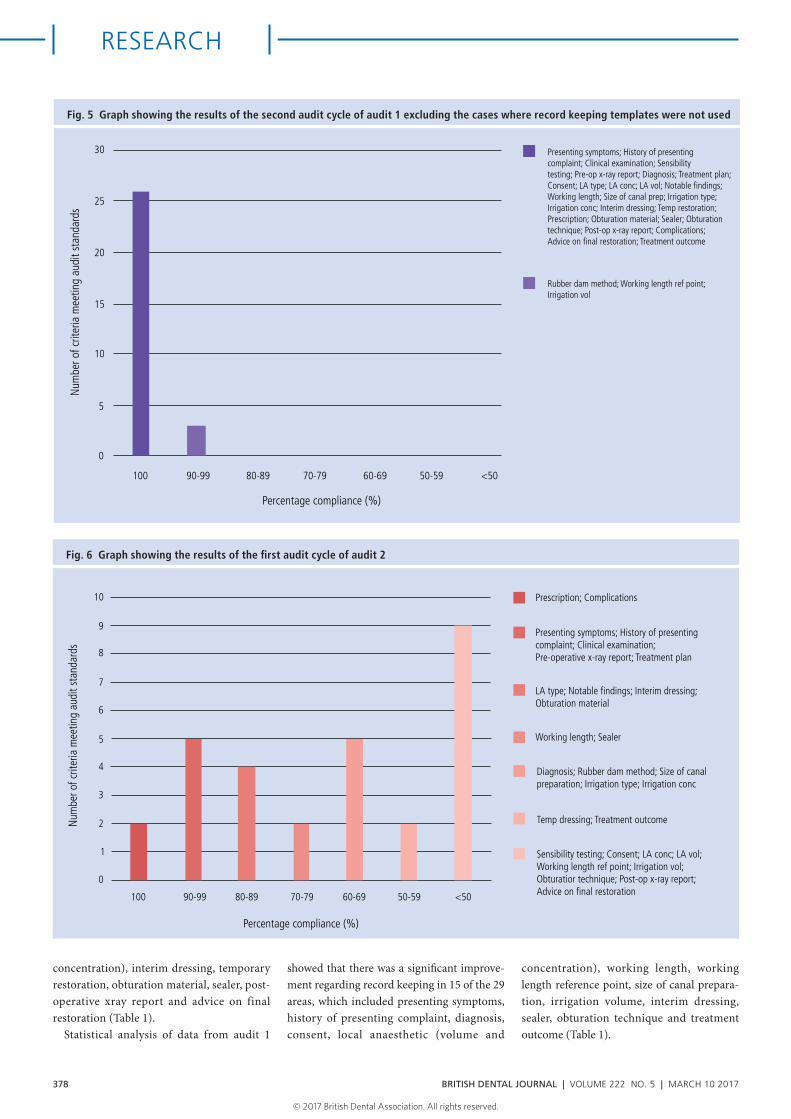
First audit cycleResults from the first audit cycles for audit 1 and audit 2 are presented in Figure 3 and Figure 6. In both audits almost all the criteria failed to meet the standards with the exception of ‘prescription’ and ‘complications’. In audit 1 the areas of particular concern (<50% com-pliance with standards) included consent, local anaesthetic (volume and concentration), working length ref point, irrigation (volume and concentration), sealer and obturation technique. In audit 2 the areas of least com-pliance (<50% compliance with standards) included sensibility testing, consent, local anaesthetic (volume and concentration), working length reference point, irrigation volume, obturation technique, post-operative xray report and advice on final restoration. The clinicians in the Restorative Dentistry Department performed marginally better than the MSc students with regards to record keeping.
Re-auditResults from the re-audit cycle for audit 1 are presented in Figure 4 and Figure 5 and the results from the re-audit cycle for audit 2 are presented in Figure 7.
For audit 1, when looking at the whole data set (Fig. 4) a substantial improvement in record keeping was seen in all areas, with 100% compliance achieved in seven criteria and >90% compliance achieved in 17 criteria. However, the criteria ‘consent’ and ‘working length reference point’ were still below 50% compliance levels. The new endodontic record keeping templates had only been used in 17 of the 50 case notes selected. By excluding the cases where the record keeping templates had not been used, analysis of the 17 data sets where the endo-dontic record keeping templates had been used (Fig. 5) showed even greater improve-ments with 26 of the criteria reaching 100% compliance and all criteria reaching >90% compliance. Interestingly, compliance when using the new record keeping templates was better with certain grades of staff, with StRs and staff grades demonstrating the most compliance. Furthermore, the grades of
staff demonstrating most improvement in record keeping included StR, staff grades and specialists.
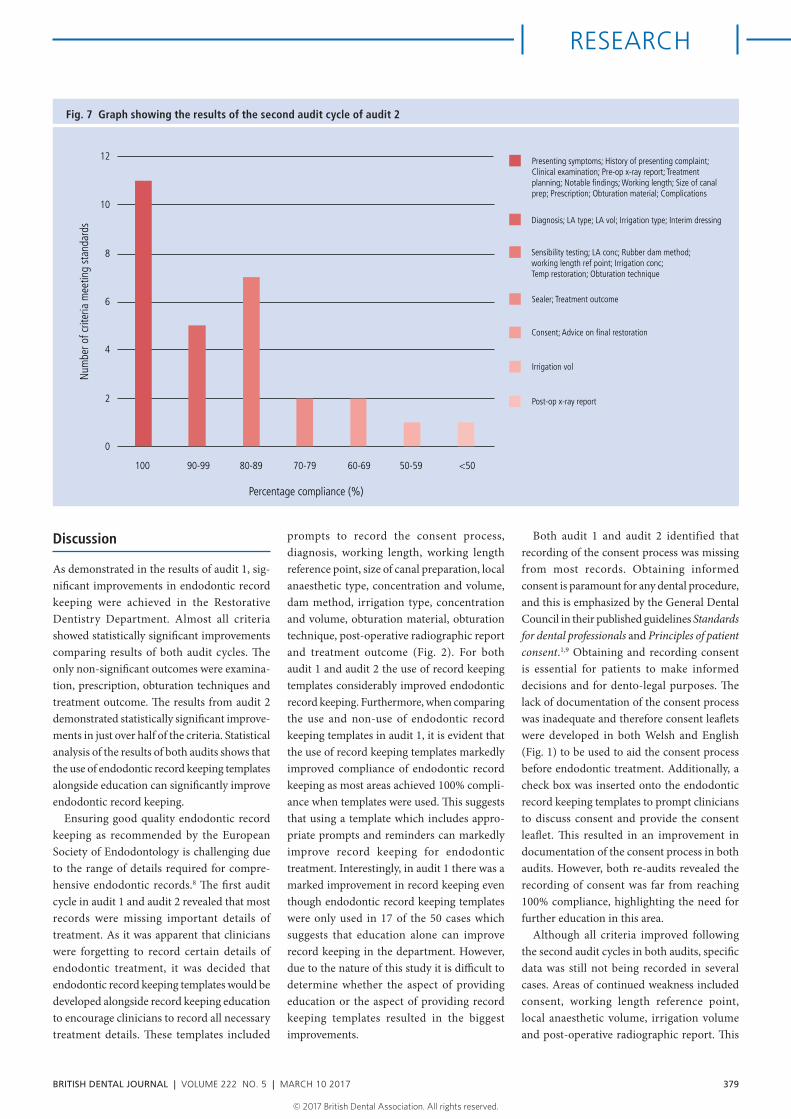
The results from the re-audit of audit 2 also show substantial improvements in all areas except ‘post-operative radiographic report’. ‘Consent’ and ‘irrigation volume’ and ‘advice on final restoration’ showed con-siderable improvements, however, they still only achieved 50–60% compliance with the standards. In all case notes the new endodontic record keeping templates had been used.
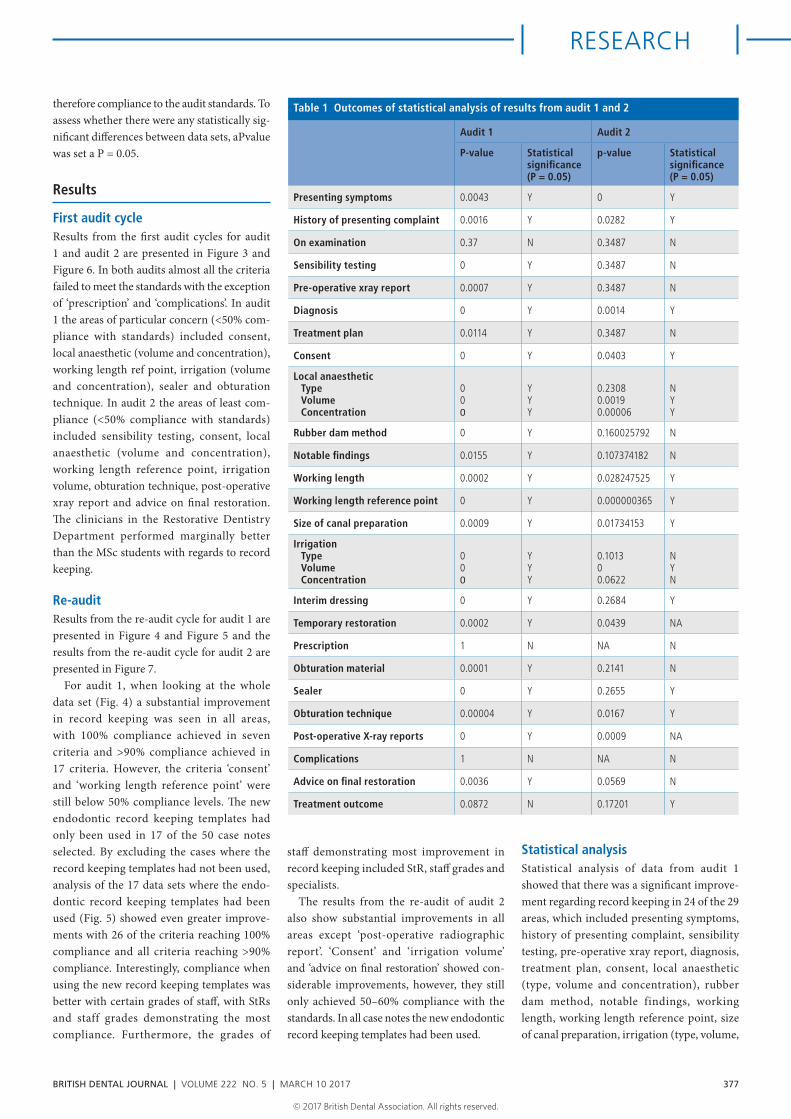
Statistical analysisStatistical analysis of data from audit 1 showed that there was a significant improve-ment regarding record keeping in 24 of the 29 areas, which included presenting symptoms, history of presenting complaint, sensibility testing, pre-operative xray report, diagnosis, treatment plan, consent, local anaesthetic (type, volume and concentration), rubber dam method, notable findings, working length, working length reference point, size of canal preparation, irrigation (type, volume,
Table 1 Outcomes of statistical analysis of results from audit 1 and 2
Audit 1 Audit 2
P-value Statistical significance (P = 0.05)
p-value Statistical significance (P = 0.05)
Presenting symptoms 0.0043 Y 0 Y
History of presenting complaint 0.0016 Y 0.0282 Y
On examination 0.37 N 0.3487 N
Sensibility testing 0 Y 0.3487 N
Pre-operative xray report 0.0007 Y 0.3487 N
Diagnosis 0 Y 0.0014 Y
Treatment plan 0.0114 Y 0.3487 N
Consent 0 Y 0.0403 Y
Local anaestheticTypeVolumeConcentration
000
YYY
0.23080.00190.00006
NYY
Rubber dam method 0 Y 0.160025792 N
Notable findings 0.0155 Y 0.107374182 N
Working length 0.0002 Y 0.028247525 Y
Working length reference point 0 Y 0.000000365 Y
Size of canal preparation 0.0009 Y 0.01734153 Y
IrrigationTypeVolumeConcentration
000
YYY
0.101300.0622
NYN
Interim dressing 0 Y 0.2684 Y
Temporary restoration 0.0002 Y 0.0439 NA
Prescription 1 N NA N
Obturation material 0.0001 Y 0.2141 N
Sealer 0 Y 0.2655 Y
Obturation technique 0.00004 Y 0.0167 Y
Post-operative X-ray reports 0 Y 0.0009 NA
Complications 1 N NA N
Advice on final restoration 0.0036 Y 0.0569 N
Treatment outcome 0.0872 N 0.17201 Y
BRITISH DENTAL JOURNAL | VOLUME 222 NO. 5 | MARCH 10 2017 377
RESEARCH
© 2017
British
Dental
Association.
All
rights
reserved. ©
2017
British
Dental
Association.
All
rights
reserved.
concentration), interim dressing, temporary restoration, obturation material, sealer, post-operative xray report and advice on final restoration (Table 1).
Statistical analysis of data from audit 1
showed that there was a significant improve-ment regarding record keeping in 15 of the 29 areas, which included presenting symptoms, history of presenting complaint, diagnosis, consent, local anaesthetic (volume and
concentration), working length, working length reference point, size of canal prepara-tion, irrigation volume, interim dressing, sealer, obturation technique and treatment outcome (Table 1).
Fig. 5 Graph showing the results of the second audit cycle of audit 1 excluding the cases where record keeping templates were not used
30
25
20
15
10
5
0
100 90-99 80-89 70-79 60-69 50-59 <50
Percentage compliance (%)
Num
ber o
f crit
eria
mee
ting
audi
t sta
ndar
ds
Presenting symptoms; History of presentingcomplaint; Clinical examination; Sensibilitytesting; Pre-op x-ray report; Diagnosis; Treatment plan;Consent; LA type; LA conc; LA vol; Notable findings;Working length; Size of canal prep; Irrigation type;Irrigation conc; Interim dressing; Temp restoration;Prescription; Obturation material; Sealer; Obturationtechnique; Post-op x-ray report; Complications; Advice on final restoration; Treatment outcome
Rubber dam method; Working length ref point; Irrigation vol
10
9
8
7
6
5
4
3
2
1
0
100 90-99 80-89 70-79 60-69 50-59 <50
Prescription; Complications
Presenting symptoms; History of presentingcomplaint; Clinical examination;Pre-operative x-ray report; Treatment plan
Num
ber o
f crit
eria
mee
ting
audi
t sta
ndar
ds
LA type; Notable findings; Interim dressing;Obturation material
Working length; Sealer
Diagnosis; Rubber dam method; Size of canalpreparation; Irrigation type; Irrigation conc
Temp dressing; Treatment outcome
Sensibility testing; Consent; LA conc; LA vol; Working length ref point; Irrigation vol;Obturatior technique; Post-op x-ray report;Advice on final restoration
Percentage compliance (%)
Fig. 6 Graph showing the results of the first audit cycle of audit 2
378 BRITISH DENTAL JOURNAL | VOLUME 222 NO. 5 | MARCH 10 2017
RESEARCH
© 2017
British
Dental
Association.
All
rights
reserved. ©
2017
British
Dental
Association.
All
rights
reserved.
Discussion
As demonstrated in the results of audit 1, sig-nificant improvements in endodontic record keeping were achieved in the Restorative Dentistry Department. Almost all criteria showed statistically significant improvements comparing results of both audit cycles. The only non-significant outcomes were examina-tion, prescription, obturation techniques and treatment outcome. The results from audit 2 demonstrated statistically significant improve-ments in just over half of the criteria. Statistical analysis of the results of both audits shows that the use of endodontic record keeping templates alongside education can significantly improve endodontic record keeping.
Ensuring good quality endodontic record keeping as recommended by the European Society of Endodontology is challenging due to the range of details required for compre-hensive endodontic records.8 The first audit cycle in audit 1 and audit 2 revealed that most records were missing important details of treatment. As it was apparent that clinicians were forgetting to record certain details of endodontic treatment, it was decided that endodontic record keeping templates would be developed alongside record keeping education to encourage clinicians to record all necessary treatment details. These templates included
prompts to record the consent process, diagnosis, working length, working length reference point, size of canal preparation, local anaesthetic type, concentration and volume, dam method, irrigation type, concentration and volume, obturation material, obturation technique, post-operative radiographic report and treatment outcome (Fig. 2). For both audit 1 and audit 2 the use of record keeping templates considerably improved endodontic record keeping. Furthermore, when comparing the use and non-use of endodontic record keeping templates in audit 1, it is evident that the use of record keeping templates markedly improved compliance of endodontic record keeping as most areas achieved 100% compli-ance when templates were used. This suggests that using a template which includes appro-priate prompts and reminders can markedly improve record keeping for endodontic treatment. Interestingly, in audit 1 there was a marked improvement in record keeping even though endodontic record keeping templates were only used in 17 of the 50 cases which suggests that education alone can improve record keeping in the department. However, due to the nature of this study it is difficult to determine whether the aspect of providing education or the aspect of providing record keeping templates resulted in the biggest improvements.
Both audit 1 and audit 2 identified that recording of the consent process was missing from most records. Obtaining informed consent is paramount for any dental procedure, and this is emphasized by the General Dental Council in their published guidelines Standards for dental professionals and Principles of patient consent.1,9 Obtaining and recording consent is essential for patients to make informed decisions and for dento-legal purposes. The lack of documentation of the consent process was inadequate and therefore consent leaflets were developed in both Welsh and English (Fig. 1) to be used to aid the consent process before endodontic treatment. Additionally, a check box was inserted onto the endodontic record keeping templates to prompt clinicians to discuss consent and provide the consent leaflet. This resulted in an improvement in documentation of the consent process in both audits. However, both re-audits revealed the recording of consent was far from reaching 100% compliance, highlighting the need for further education in this area.
Although all criteria improved following the second audit cycles in both audits, specific data was still not being recorded in several cases. Areas of continued weakness included consent, working length reference point, local anaesthetic volume, irrigation volume and post-operative radiographic report. This
12
10
8
6
4
2
0
100 90-99 80-89 70-79 60-69 50-59 <50
Num
ber o
f crit
eria
mee
ting
stan
dard
s
Percentage compliance (%)
Presenting symptoms; History of presenting complaint;Clinical examination; Pre-op x-ray report; Treatmentplanning; Notable findings; Working length; Size of canalprep; Prescription; Obturation material; Complications
Diagnosis; LA type; LA vol; Irrigation type; Interim dressing
Sensibility testing; LA conc; Rubber dam method;working length ref point; Irrigation conc; Temp restoration; Obturation technique
Sealer; Treatment outcome
Consent; Advice on final restoration
Irrigation vol
Post-op x-ray report
Fig. 7 Graph showing the results of the second audit cycle of audit 2
BRITISH DENTAL JOURNAL | VOLUME 222 NO. 5 | MARCH 10 2017 379
RESEARCH
© 2017
British
Dental
Association.
All
rights
reserved. ©
2017
British
Dental
Association.
All
rights
reserved.

demonstrates that even with the provision of record keeping education and record keeping templates, the variation of record keeping between clinicians remains a problem. It is therefore important to continue regular education and auditing to ensure record keeping standards are met and maintained.
These audits highlight the importance of good endodontic record keeping and how it can be improved using departmental guide-lines, education, consent leaflets and endodon-tic record keeping templates.
Conclusions
In relation to both audits, the following rec-ommendations have been made with the aim
to help clinicians improve their endodontic record keeping:• Endodontic record keeping templates are
recommended to encourage comprehensive endodontic record keeping
• Consent leaflets are effective for encour-aging the discussion and recording of the consent process
• Record keeping education can successfully improve endodontic record keeping
• Regular education and audit is required to ensure standards of record keeping are met and maintained.
1. General Dental Council. Standards for Dental Profes-sionals. London: GDC, 2005.
2. Faculty of General Dental Practitioners. Clinical Exam-ination and Record-Keeping: Good Practice Guidelines. 2nd ed. London: FGDP, 2009.
3. Platt M, Yewe-Dyer M. How accurate is your charting? Dent Update 1995; 22: 374.
4. Morgan RG. Quality evaluation of clinical records of a group of general dental practitioners entering a quality assurance programme. Br Dent J 2001 27; 191: 436–441.
5. Pessian F, Beckett H A. Record keeping by undergrad-uate dental students: a clinical audit. Br Dent J 2004; 197: 703–705.
6. Cole A, McMichael A. Audit of dental practice record-keeping: a PCT-coordinated clinical audit by Worcestershire dentists. Prim Dent Care 2009; 16: 85–93.
7. McAndrew R, Ban J, Playle R. A comparison of computerand hand-generated clinical dental notes with statutory regulations in record keeping. Eur J Dent Educ 2012; 16: e117–e121.
8. European Society of Endodontology. Quality guidelines for endodontic treatment: consensus report of the European Society of Endodontology. Int Endod J 2006; 39: 921–930.
9. General Dental Council. Principles of Patient Consent. London: GDC, 2005.
380 BRITISH DENTAL JOURNAL | VOLUME 222 NO. 5 | MARCH 10 2017
RESEARCH
© 2017
British
Dental
Association.
All
rights
reserved.