Embed Size (px)
Citation preview

Improving the Accuracy of American Indian Data through Linkage to Tribal
Rolls
NAPHSIS2008

Need for Accurate American Indian Health Data
Public Health Priority IssueKnown Health DisparitiesStrong Tribal Interest in DataRecognized Lack of Reliable Data

Federally Recognized TribesMichigan
Keweenaw Bay ChippewaLac Vieux Desert Band of ChippewaSaginaw ChippewaThe Sault Tribe of ChippewaLittle Traverse Bay Band of OdawaPokegon Band of PotawatomiGun Lake PottawattomiLittle River band of OttawaGrand Traverse Band of Ottawa and ChippewaHannahville PotawatomiHuron PotawatomiBay Mills Chippewa

Concern for Accuracy of American Indian Data
History of UnderreportingExtremely Low Disease RatesSpecial Interest PopulationTribal Health Planners lack Reliable Data8th largest American Indian Population73,295 Michigan American Indians in 2004

Summary of Previous of AI/AN Linkages
Study Incidence (# cases) before match
Incidence (# cases) after match
Change
Washington(1992-93)
153.5 267.5 74%
Minnesota(1988-93)
245.2 390.25 59%
California(1988-92)
89.6 211.0 135.5%
Puget Sound(1974-89)
(137) (233) 70%



Swan, J and Edwards BK. Cancer Rates among American Indians and Alaska Natives: Is there a National Perspective? Cancer. 2003;98(6):1262-1272.
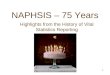
472.3
239.6
62.6
33.154.2
34.7
170.1
53.6
135
58
0
50
100
150
200
250
300
350
400
450
500
All Cancers Lung/Bronchus Rectum/Colon Prostate (men) Breast (women)
Incidence (per 100,000 people)
Cancer Incidence in AIAN and Total U.S. Populations (SEER 1992-2000)
Total U.S. Population AIAN Population
Cancer Incidence in American Indians appears to be MUCH LOWER than Total U.S. Population

Age-Adjus ted Incidence R ate of Malignant C ancer B efore Quality Improvement L inkages (IHS and Tribal)
0
100
200
300
400
500
600
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004Age-
Ajus
ted
Can
cer I
ncid
ence
Rat
e pe
r 100
,000
per
son-
year
s
S tate A I/AN (As R eported) S tate - A ll R aces National S E E R - A ll R aces

CDC and IHS Initiative
Link IHS registry to health dataTarget cancer and death registriesPromote use of improved dataKey contacts are David Espey, CDC/IHS
[email protected] Melissa Jim, CDC/IHS

Assessing and improving the quality ofcancer surveillance data for American Indians
• Link records from state cancer registries/death records with IHS patient registration database
• Identify AI/AN cancer cases/deaths misclassified as non-Native
• Use “improved” data to report cancer burden of American Indians

ApprovalsIHS National IRBCDC National Center for Chronic Disease Prevention and Health PromotionState IRB approvals (i.e. Department of Health & Senior Services, Office of Public Health)
A data quality improvement activity in support of routine public health surveillance
– public health practice not research

Data Management
MOA or state Data Use AgreementData sent to ABQ or travel to stateLinkage done using LinkPlusSend back Match File 3 Contains both IHS & state information
that was used to determine if the match was a link
Create de-identified analysis files

Linkages between IHS and state cancer registries
NV
WA
ORID
MT ND
SDMN
WIMIWY
CA
UTCO
AZ NM
AK
HI
TX
NE
KS
OK
LA
ALMS
MO
IL IN
KY
TN
GA
FL
SC
NC
VAWV
PA
NY
ME
NJCT
MD
OH DE
RI
MAVT
NH
AR
IANV

Registry linkages
Linkage status captured in “IHS Link” variable in NAACCR layout
Surveillance monograph in journal Cancer
Annual Report to the Nation with special section on cancer in AI/AN

Record Linkage between NPCR Program registries and IHS administrative records
0
1000
2000
3000
4000
5000
6000
7000
8000
pre-link added by linkage
0
50
100
150
200
WV
VT
NH
KY
DE IN TN
MA LA RI
PA
SC AL
VA
GA
ME
OH
MD IL AR
Graph with smaller scale for lower 20 NPCR Program registries

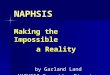
CHSDA Non-CHSDA

Michigan NPCR-IHS Linkage Results, 1995-2002
CHSDA Before: 250 individuals After: 612 individuals Difference: 362 individuals that were previously
coded as race other than Al/AN in registry
Non-CHSDA Before: 248 After: 350 Difference: 102 individuals that were previously
coded as race other than AI/AN in registry

Linkages between IHS and state death records
Similar problems of misclassificationMuch larger databasesLess standardization than cancer registries

NV
WA
ORID
MT ND
SDMN
WIMIWY
CA
UTCO
AZNM
AK
HI
TX
NE
KS
OK
LA
ALMS
MO
IL IN
KY
TN
GA
FL
SC
NC
VAWV
PA
NY
ME
NJCT
MD
OH DE
RIMA
VT
NH
AR
IANV
IHS/state death records data linkage
Linkage completedData rec’d – linkage in progressInterest expressed – data not rec’dNot participating

Michigan Division of Vital Records and Health Statistics-IHS Linkage Results,
1990-2002
Before: 5,585 individualsAfter: 5,924 individualsDifference: 339 individuals that were previously coded as race other than AI/AN on death certificate

Linkage of death records from State VS with
administrative records from the IHS(1990-2003)
0
5000
10000
15000
20000
25000
30000
ID UT ND OR MN MT MI NC WA NM CA AZ OK
Pre-link Post-link

Collecting ancestry in 1989 noticeablyimproved the reporting of American Indian

Live Births and Deaths Reported as Native American by Year
139 137 132
335 352324
478 484525
844805
766
0
100
200
300
400
500
600
700
800
900
1986 1987 1988 1989 1990 1991
Year
Nu
mb
er
Deaths
Live Births
62 percent increase
Certificate revised in 1989
150 percent increase

Multiple Responses now Collected
Up to 5 choices for race Collected on Deaths since 2004
450 Native American 1st choice 840 “any mention” in 2005 data
Collected on Births since 2006

Considering Both Parents for Newborns
Increases Cases Significantly
During 2005, 736 Native American Mothers 734 Native American Fathers
1,239 either parent Native American

Additional Change in “Process”
Collecting Principle Tribe

American Indian
Additional Change in “Process”

Little Traverse Bay Ottawa
Beginning to Collect Principle Tribe

Issues
What proportion in Michigan are IHS?IHS recipients more or less likely to be reported as American Indian?Census population issues compound problem?Who should be considered American Indian?

Solution Appears to be Tribal Links
Applies tribal definition of membershipEnables analysis of Tribe as a cohortEmpowers tribal health plannersResolves numerator/denominator concerns

Proposal for Link to Tribal RollsInterested Tribe would Provide Tribal RollLink Tribal Roll to Dataset of Interest: Births Deaths Cancer Registry
Release Results on Tribe to Participating Tribe DCH would provide a de-identified file for analysis
Augment state level data Special reports on American Indian Health
Validate accuracy of case reportsEvaluate principle tribe reporting

Proposed Approach
Develop a Protocol and Data Use AgreementEstablish as a Research Project Assure protection of the data
Develop Approach that Assures Confidentiality Options include:
Provide tribal roll to DCH for Link Identifiable data used only for linkage then destroyed
Jointly conduct link on a portable devise Role loaded/linked/destroyed
DCH to retain which specific cases linkedTribe to receive an agreed de-identified data set

Issues
Need interest of tribal health plannersNeed approval of tribal leadersNeed to assure confidentialityNeed to maximize privacy of tribal roll

Approach
Contact Michigan Intertribal Council Build on history of collaboration
Model after IHS approach Develop tribal interest Organize meeting through Intertribal
Council
Develop clear written agreement Obtain IRB review

Outcomes
De-identified file of linked cases to tribe File is owned by tribe for use in analysis of
cancer incidence and related issues Any results to be released only with
approval of the tribe
Id number field for linked cases to state State can use to improve registry data on
American Indian

Questions using Tribe-specific data:
What types of cancers are most/least common in tribe members?
How do tribal rates of cancer by type compare to other populations?
What stage is cancer in tribal members at diagnosis?
How long do tribal members with cancer live after being diagnosed?
What is the geographic distribution of cancer (rural vs. urban, county-level characteristics)

In Attendance
The Linkage was conducted on 7/20/2007 at the tribal Administration BuildingTribal Staff Present: Database Manager Tribal Registrar Tribal Attorney Environmental Manager
State Staff: MI Cancer Registrar
Study Staff: Study PI from University of Michigan

De-Identified DatasetDrop first, middle, last name, SSN, DOBKeep cancer characteristics (eg. primary site, stage, year of diagnosis, age at diagnosis)Keep some demographics (sex, race and ethnicity as reported, survival time)Keep county-level characteristics (eg. urban/rural, % American Indian, % minorities)
Tribe and State receive a copy of this de-identified dataset.
Access to the state data set must be restricted under the terms of the data use agreement

Other Limitations
Periods of open and closed enrollment–changes in the tribe’s population over time are difficult to interpretEnrollment bias many people who identify as tribal members
may not be in the database are sicker people more likely to enroll than
healthy people?
Detection bias Cancer registry only picks up cancers in
Michigan; if a tribal member was never treated for cancer in MI, they wouldn’t be recorded; tribal roster, on the other hand, is worldwide

Reported as AI/AN to the State Cancer Registry
Linked to IHS patient files
Linked to the TribeEnrollment Roster
366 cases316 individuals
282 cases256 individuals
190 cases168 individuals
178 cases147 individuals
20 cases17 individuals
361 cases309 individuals
99 cases89 individuals

Reported as American Indian to the State Death Registry Linked to Indian Health
Services patient files (IHS)
Linked to TribalMembership roster
56 deaths
154 deaths
200 deaths
128 cases
*IHS began linking with the MI registry in 1995, so this diagram is for 1995 – 2004.
4,975 deaths

Age-Adjus ted Incidence R ate of Malignant C ancer B efore Quality Improvement L inkages (IHS and Tribal)
0
100
200
300
400
500
600
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004Age-
Ajus
ted
Can
cer I
ncid
ence
Rat
e pe
r 100
,000
per
son-
year
s
S tate A I/AN (As R eported) S tate - A ll R aces National S E E R - A ll R aces

Age-Adjus ted Incidence R ate of Malignant C ancer B efore and After HIS Quality Improvement L inkages
0
100
200
300
400
500
600
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004Age-
Ajus
ted
Can
cer I
ncid
ence
Rat
e pe
r 100
,000
per
son-
year
s
S tate A I/AN (As R eported) S tate A I/AN (After IHS L inkage) S tate - A ll R aces National S E E R - A ll R aces

Age-Adjus ted Incidence R ate of Malignant C ancer B efore and After Quality Improvement L inkages (IHS and Tribal)
0
100
200
300
400
500
600
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004Age-
Ajus
ted
Can
cer I
ncid
ence
Rat
e pe
r 100
,000
per
son-
year
s
S tate A I/AN (As R eported) S tate A I/AN (After IHS L inkage) S tate A I/AN (After Tribe L ink)
S tate - A ll R aces National S E E R - A ll R aces

Directions
Develop interest in other tribesAssist with tribal cancer control planPromote the linkage of births and deathsWork toward a periodic linkage routine Establish baseline and monitor trends

Acknowledgements
Intertribal Council of Michigan Rick Haverkate, Health Director Noel Pingatore Elizabeth Kushman
Dan Tadgerson Tribal Environmental Manager
David Espey, CDC/IHSMelissa Jim, CDC/IHSJennifer Johnson, UM Doctoral Candidate