Embed Size (px)
Citation preview

2/8/2016
1
Improving Survival after In-hospital Cardiac Arrest:
Life after Death
Saket Girotra MD, SMAssistant Professor of Medicine
University of Iowa Carver College of Medicine
Disclosures
• Co-chair, Adult Research Task ForceGet With The Guidelines-Resuscitation American Heart Association
Learning Objectives
• Describe epidemiology of in-hospital cardiac arrest
• Describe processes of care associated with improved survival
• Outline potential strategies for improving survival and neurologic outcomes
2/8/2016
2
History of CPR
1500-1700
Modern History
• Peter Safar
– Head tilt, chin lift
– Mouth-to-mouth respiration
– ‘ABC’ of resuscitation
• William Kouvenhoven
– closed cardiac massage
• Bernard Lown
– Modern defibrillators

2/8/2016
3
Recommended Guidelines for Reviewing, Reporting, and Conducting Research on In-Hospital Resuscitation:
The In-Hospital ‘Utstein Style’
Richard O. Cummins, Douglas Chamberlain, Mary Fran Hazinski, Vinay Nadkarni, Walter Kloeck, Efraim Kramer, Lance Becker,
Colin Robertson, Rudi Koster, Arno Zaritsky, Leo Bossaert, Joseph P. Ornato, Victor Callanan, Mervyn Allen, Petter Steen,
Brian Connolly, Arthur Sanders, Ahamed Idris, and Stuart Cobbe
CirculationVolume 95(8):2213-2239
April 15, 1997
Copyright © American Heart Association, Inc. All rights reserved.
Conceptual Model
Cardiac Arrest“Surviving a code”
or ROSCNeurologically Intact Survival
Acute Resuscitation Phase
• Patient Factors(age, sex, co-morbidities)
• Cardiac arrest characteristics(rhythm, witnessed)
• Resuscitation response(response time, quality of CPR, timely defibrillation)
Post Resuscitation Phase
• Availability of treatment (hypothermia, cardiac cath)
• Supportive critical care(intensive care nurses, structured treatment protocols)
• Resources & Personnel (specialists, physicians)
• Variability in advanced care directives
National Registry of Cardiopulmonary Resuscitation (NRCPR)
• Established in 2000
• Based on the Utstein template for cardiac arrest
• Multi-center registry of IHCA
• Multi-pronged strategy for identifying IHCA
• Rich clinical data abstracted by trained personnel
• Focus – quality improvement
• Now “Get With The Guidelines-Resuscitation”

2/8/2016
4
Epidemiology of in-hospital CA
• 200,000 patients in U.S. every year
• 20% are black
• 25% of IHCA is due to VF/VT
• Burden of co-morbidities is higher
• Survival 17%Peberdy et al Resuscitation 2003Merchant et al Crit Care Med 2011
Delayed Defibrillation for VF/VT
2/8/2016
5
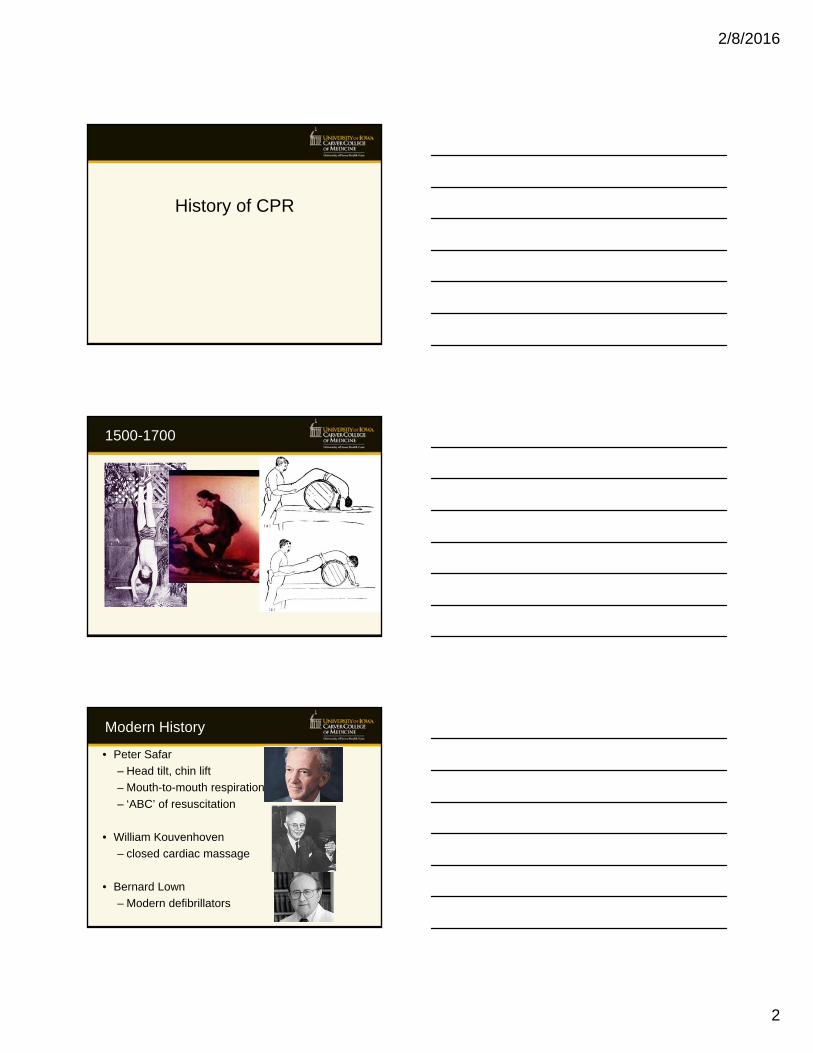
Survival to discharge RR
Unadjusted 0.73 (0.67-0.79)
Adjusted for age and sex 0.70 (0.64-0.76)
plus clinical characteristics 0.81 (0.75-0.86)
plus hospital characteristics 0.82 (0.76-0.89)
plus time to defibrillation 0.90 (0.83-0.96)
• N=84,625 patients between 2000-2009 at 374 hospitals
• Examined whether survival outcomes have improved over time using a GEE model

2/8/2016
6
Risk-Adjusted Survival to Discharge
10.7%
14.8%
Adj RR per-10 year = 1.42 (1.23-1.64)
13.717.1 18.2 17.8 18.9 20.0 20.5 21.2
23.3 22.3
0
10
20
30
40
50
60
70
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
Su
rviv
al t
o D
isc
ha
rge
, %
P for trend < 0.001
OVERALL
Adj RR per-10 year = 1.42 (1.23-1.64)
Girotra et al NEJM 2012
Risk-AdjustedSurvival to Discharge -By Rhythm
10.7%
14.8%
Adj RR per-10 year = 1.42 (1.23-1.64)
28.6
41.5
6.8
13.3
0
10
20
30
40
50
60
70
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
Su
rviv
al t
o D
isc
ha
rge
, %
P for trend < 0.001 for all
Adj RR per-10 year = 1.71 (1.39-2.10)
Adj RR per-10 year = 1.25 (1.08-1.44)
ASYSTOLE & PEA
VF & VT
Girotra et al NEJM 2012
Neurological Disability
10.7%
14.8%
Adj RR per-10 year = 1.42 (1.23-1.64)32.928.1
0
10
20
30
40
50
60
70
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
Ne
uro
log
ica
l D
isa
bil
ity,
% (
CP
C >
1)
Adj RR per 10-year = 0.82 (0.74, 0.99)
OVERALL
P for trend 0.02
Girotra et al NEJM 2012

2/8/2016
7
Racial differences in survival trends
Overall Stratified by rhythm type
0
0.05
0.1
0.15
0.2
0.25
Su
rviv
al t
o d
isch
arg
e
White Black p<.0001
0
0.05
0.1
0.15
0.2
0.25
0.3
0.35
0.4
0.45
0.5
Su
rviv
al t
o d
isch
arg
e
VF and VT VF and VT
Asystole and PEA Asystole and PEA
p = 0.0037
p = 0.0739
Long-term survival
Chan et al NEJM 2013
Has improvement in survival been uniform, or
have some hospitals improved more than others

2/8/2016
8
Hospital variation in IHCA survival
0
10
20
30
40
50
60
0.12 to<0.14
0.14 to<0.16
0.16 to<0.18
0.18 to<0.20
0.20 to<0.22
0.22 to<0.24
0.24 to<0.26
0.26 to<0.28
0.28 to<0.30
0.30 to<0.32
0.32 to<0.34
0.34 to0.40
Ho
spit
als,
n
Risk-Standardized Hospital Survival Rate for Cardiac Arrest
Chan et al JACC 2013
Adjusted Hospital Trends
OVERALL1st Quartile (Bottom)
2nd Quartile 3rd Quartile4th Quartile
(Top)
Mean change 1.07 1.01 1.05 1.05 1.13
Range 0.97-1.18 0.97-1.03 1.03-1.07 1.04-1.07 1.11-1.18
Odds ratios
Num
ber of hospitals
1.00 1.05 1.10 1.15
05
1015
0
5
10
15
20
25
1 6 11 16 21 26 31
Nu
mb
er o
f H
osp
ital
s
Rate of Survival to Discharge
2000-2003
2007-2010
Hospital Rates of Survival to Discharge
2/8/2016
9
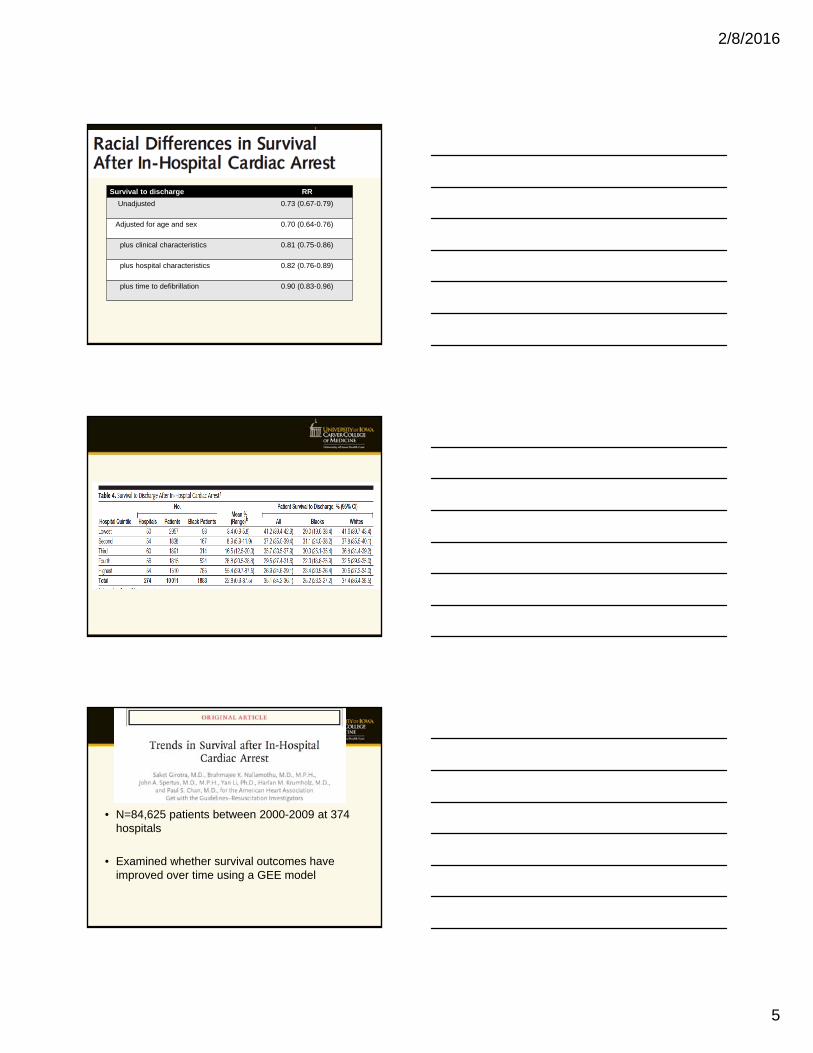
Association of Hospital Characteristics with Survival Improvement
Hospital Characteristic P for interaction
Census Region 0.81
Location (Urban or rural) 0.57
Ownership status 0.55
Bed size 0.73
Teaching 0.03
Post-resuscitation phase of IHCA
Post-resuscitation phase
• Accounts for nearly 40% of in-hospital cardiac arrest deaths
• Limited evidence regarding effectiveness of different strategies for improving post-resuscitation survival in IHCA
• Extrapolated from studies of OHCA
– Therapeutic hypothermia
– Early coronary angiography

2/8/2016
10
Hospital variation in post-resuscitation survival
Girotra et al Unpublished data
0
20
40
60
80
100
120
140
160
20% 25% 30% 35% 40% 45% 50% 55% 60%
Nu
mb
er
of
Ho
sp
ita
ls
Risk Standardized Survival to Discharge Rate
Hospital variation in IHCA survival
0
10
20
30
40
50
60
0.12 to<0.14
0.14 to<0.16
0.16 to<0.18
0.18 to<0.20
0.20 to<0.22
0.22 to<0.24
0.24 to<0.26
0.26 to<0.28
0.28 to<0.30
0.30 to<0.32
0.32 to<0.34
0.34 to0.40
Ho
spit
als,
n
Risk-Standardized Hospital Survival Rate for Cardiac Arrest
Lessons from STEMI Care
• Identified top-performers for STEMI care– Hospitals that had consistently shorter D2B
times
• Mixed-methods study– Site visits at top performing hospitals
– Key strategies at top performing hospitals
– Surveyed hospitals to narrow down
Bradley et al JACC 2006Bradley et al Circ 2006

2/8/2016
11
Bradley et al NEJM 2006
Trends in D2B time in recent years
Krumholz et al Circ 2011
Survey of hospital practices
• Therapeutic hypothermia
• Early coronary angiography
• Intensive care
• Nurse-patient ratio
• Structured treatment protocols
• Quality improvement activities

2/8/2016
12
Summary
• In-hospital cardiac arrest is common, and associated with poor survival
• Processes of care such as time to defibrillation can be important metrics to monitor resuscitation quality
• Survival after IHCA has improved in recent years, although the underlying factors remain unclear
Summary
• Marked variation in survival across hospitals persists
• Identifying best-practices related to resuscitation care at hospitals could be an innovative strategy to improve IHCA survival
Acknowledgements
• National Institutes of Health
– K08 Career Development Award
• American Heart Association
• Mentors
– Paul Chan
– Peter Cram
– Gary Rosenthal
• Mentees
– Ankur Vyas
– Lee Joseph
– Rohan Khera

2/8/2016
13
Thank you
Questions?
ADDITIONAL SLIDES
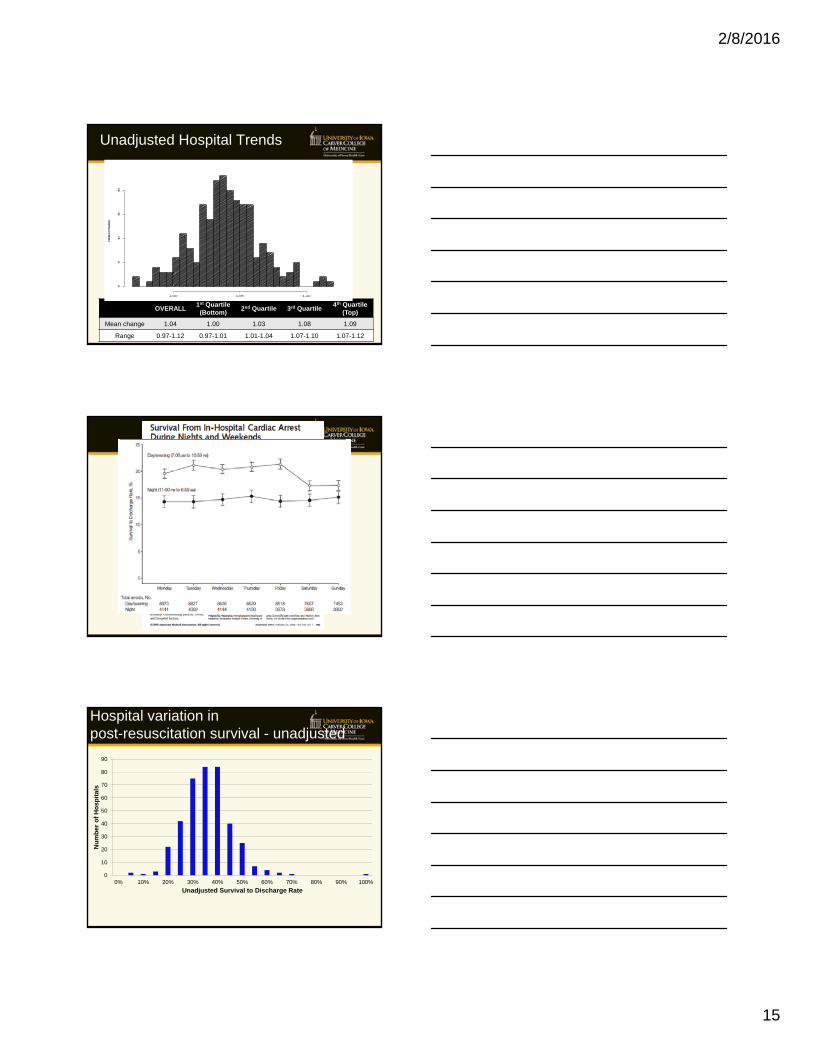
Hospital variation in post-resuscitation survival - unadjusted
0
10
20
30
40
50
60
70
80
90
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Nu
mb
er
of
Ho
sp
ita
ls
Unadjusted Survival to Discharge Rate
Girotra et al Unpublished data

2/8/2016
14
Trends in Survival
Acute Resuscitation Survival
42.7
54.1
10
20
30
40
50
60
70
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
Su
rviv
al,
%
P for trend < 0.001
OVERALL
Post-resuscitation survival
32.0
42.9
10
20
30
40
50
60
70
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
Po
st-R
esu
scit
atio
n S
urv
iva
l, %
P for trend < 0.05
OVERALL
Girotra et al NEJM 2012
Hospital Variation in Survival Trends
• N=93,342 IHCA patients at 231 hospitals
• Two-level hierarchical multivariable regression model (random intercept & random slope model)
• Magnitude of survival improvement at each hospital was quantified using odds ratio – Odds ratio = 1 (No improvement)
– Odds ratio > 1 (improvement in survival)
– Odds ratio < 1 (worsening of survival)
Girotra et al JAHA 2014
Hospital Characteristics
CHARACTERISTICS N=231
Census Region
North Mid-Atlantic 33 (14.3)
South Atlantic 59 (25.5)
North Central 52 (22.5)
South Central 41 (17.7)
Mountain/Pacific 46 (19.9)
Urban Location 207 (89.9)
Non-profit ownership 162 (70.1)
Bed size < 250 82 (35.5)
Major Teaching 55 (23.8)
2/8/2016
15
Unadjusted Hospital Trends
OVERALL1st Quartile (Bottom)
2nd Quartile 3rd Quartile4th Quartile
(Top)
Mean change 1.04 1.00 1.03 1.08 1.09
Range 0.97-1.12 0.97-1.01 1.01-1.04 1.07-1.10 1.07-1.12
Odd ti f
Num
ber of hos
pita
ls
1.00 1.05 1.10
05
1015
20
Hospital variation in post-resuscitation survival - unadjusted
0
10
20
30
40
50
60
70
80
90
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Nu
mb
er
of
Ho
sp
ita
ls
Unadjusted Survival to Discharge Rate

2/8/2016
16
Bradley et al NEJM 2006
Trends in D2B time in recent years
Krumholz et al Circ 2011
Epidemiology
• Cardiac arrest is the 3rd leading cause of death in the industrialized world
• In Canada, – 30,000-45,000 patients suffer an out-of-hospital cardiac
arrest
– Xxx patients suffer an in-hospital cardiac arrest
• In the United States,
– OHCA: 350,000 per-year
– IHCA 210,000 per-yearChan et al Circulation 2014 Go et al Circulation 2015Merchant et al Resuscitation 2011 Girotra NEJM 2012

2/8/2016
17
Conceptual Model
Cardiac Arrest“Surviving a code”
or ROSCNeurologically Intact Survival
Acute Resuscitation Phase
• Patient Factors(age, sex, co-morbidities)
• Cardiac arrest characteristics(rhythm, witnessed)
• Resuscitation response(response time, quality of CPR, timely defibrillation)
Post Resuscitation Phase
• Availability of treatment (hypothermia, cardiac cath)
• Supportive critical care(intensive care nurses, structured treatment protocols)
• Resources & Personnel (specialists, physicians)
• https://www.youtube.com/watch?v=ILxjxfB4zNk
Post-resuscitation phase
• Approximately 30-50% of cardiac arrest deaths occur during post-resuscitation phase
• Most of these deaths are due to deleterious consequences of no-flow state
• Emerging evidence that care during the post-resuscitation phase may impact patient outcomes

2/8/2016
18
IMPLICATIONS
• Assuming a stable incidence 200,000 cardiac arrests / year
2000 2009Net
Gain
Survival to discharge 27,400 44,600 17,200
No significant neurological disability
18,385 32,067 13,682