Embed Size (px)
Citation preview
FEATURE ARTICLE
Improving Self-Care Management in Low-IncomeLatinos With Type 2 Diabetes Using Peer-Led U.S.Conversation Maps: A Quality Improvement Projectin a Free ClinicCarla R. Fallas,1,2 Katherine Pereira,3,4 Blanca Iris Padilla,4,5 Irene Felsman,4 Sharon Allen,6,7 and Curtis Preik1
A culturally sensitive Healthy Interactions Conversa-tions Maps program was implemented for teachingdiabetes self-management education (DSME) to Latinoswith type 2 diabetes using peer-led educators in acommunity health center. Patients were invited toparticipate in a group care setting to improve access toproviders and DSME. Goals were to improve diabetesdistress, self-efficacy, and glycemic control as mea-sured by A1C. Significant improvements were found formean diabetes self-efficacy scores from before (2.536
0.59) to after (2.916 0.50) DSME (P,0.001). Mean A1Cdecreased significantly from before (9.51 6 1.72%) toafter (8.796 1.68%) DSME (P5 0.043) at the end of the6-month intervention. Thus, this program was found tobe a useful tool for providing DSME in community healthclinics serving low-income Latinos.
As the fastest growing racial/ethnic minority, Latinos aredisproportionately affected by diabetes, and their riskof developing diabetes is 66% higher than that of Cau-casians (1). Moreover, Latinos are twice as likely asCaucasians to die of diabetes-related complications (1).Less than half of Latinos with type 2 diabetes are ableto achieve the recommended A1C goal of ,7.0% (2).
Social Cognitive Theory (SCT) proposes that individualswith high self-efficacy are more likely to change theirbehavior, make healthy choices, be more positive in self-attribution, and have a better sense of control (3). TheAmerican Diabetes Association’s (ADA’s) Standards ofMedical Care in Diabetes (4) recommend that primary careproviders offer patient-centered group or individualizeddiabetes self-management education (DSME) to patients
to assist them in achieving the key goals of improveddiabetes self-management, clinical outcomes, healthstatus, and quality of life.
The ADA also recommends routine monitoring for dia-betes distress (DD) using validated measures to addressareas of self-care that are most relevant to patients andaffect their clinical management (4). Patients often ex-perience a considerable degree of emotional involvementin diabetes care, which can cause anxiety and depression(5). Depression is two times more prevalent in patientswith type 2 diabetes than in those without diabetes;however, there is a distinction between depressivepsychiatric disorders and diabetes-related distress (5).
DD and DSME: Literature Review
DD is defined as patients’ personal concerns about theirdisease management, providers, family support, emo-tional burden, and access to health care (6). High levelsof DD have been associated with worse clinical andpsychosocial outcomes (5). A recent systematic reviewand meta-analysis of 55 studies reported a 36% overallprevalence of DD in people with type 2 diabetes (7).However, female sex and comorbid depressive symptomscould act as potential confounders, limiting the ability toeffectively measure DD (7).
DD is more closely associated with diabetes self-management and diabetes-related behavioral and bio-medical outcomes than depression (7). Specifically, highlevels of DD are related to worsening glycemic control (7).A meta-analysis of randomized controlled trials noted thatinteractive self-management interventions help reduce
1Camino Community Center, Charlotte, NC; 2Lenoir-Rhyne University, Hickory, NC; 3Endocrinology Division, Duke University Medical Center,Durham, NC; 4Duke University School of Nursing, Durham, NC; 5Lincoln Community Health Center, Durham, NC; 6Nursing Administration, AtriumHealth, Carolinas Healthcare System NorthEast, Concord, NC; 7School of Nursing, University of North Carolina, Charlotte, Charlotte, NC
https://doi.org/10.2337/cd19-0052
©2020 by the American Diabetes Association. Readers may use this article as long as the work is properly cited, the use is educational and notfor profit, and the work is not altered. More information is available at https://www.diabetesjournals.org/content/license.
VOLUME 38, NUMBER 3, SUMMER 2020 213
A1C (by a mean of 20.43%), improve diabetesknowledge, enhance self-efficacy, and reduce DD (8).The behavioral interactive self-management techniquesimplemented in trials included providing feedbackto patients on performance, problem-solving, andaction-planning.
A systematic review of 13 randomized controlled trialsconcluded that DSME in conjunction with primary careeffectively improved glycemic control in Latino adultswith type 2 diabetes (9), with greater reductions if amultimodal, multiprovider, culturally sensitive DSMEprogramwas used (9,10). In this review, multiple types ofeducators (e.g., medical care providers, certified diabeteseducators [CDEs], and peer educators) administered theDSME sessions; however, peer educators alone appearedto be effective (9).
Subgroup analysis from this review suggested thatculturally tailored DSME interventions involving bothtrained diabetes educators and peer educators mayprovide the greatest benefit (9). Peer-led diabetes self-management, a potential low-cost, flexible modality, hasbeen found to successfully maintain key improvements inA1C in rural communities (11,12). Providing bicultural/bilingual educational materials and involving teammembers from the community can enhance the culturalsensitivity of DSME programs (13).
Tomeet the increasing demand for delivery of health careservices to a large number of patients with chronic disease,many health care professionals (HCPs) have adopted agroup care model. Group care strategies involving in-teractions with HCPs (either in person or via telephone)have been found to have large effect sizes than otherstrategies (9,14). A systematic review and meta-analysisof 26 studies demonstrated that groupmedical visits had apositive effect on clinical and patient-reported outcomesandyieldeda significant reduction inmeanA1C(20.46%,95% CI20.80 to20.31) (15). It is important to note thatthe most successful DSME interventions in Hispanicpatients with diabetes were culturally tailored, whetheradministered in person to individuals or groups or inmultimodal sessions (9).
This pilot project used a culturally sensitive, evidence-basedU.S. ConversationMaps program(16). TheHealthyInteractions Conversation Maps (available in English andSpanish) were developed in collaboration with the ADAfor use in the United States and with the InternationalDiabetes Federation for use elsewhere in the world (16).Conversation Maps are designed to be used in a smallgroup environment, encourage peer involvement, anddeliver patient-centered education. A 2017meta-analysis
(17) examinedglycemicoutcomesusing theConversationMap tools to deliver DSME and included 851 participantsin nine studies from five countries. All cohorts showedsignificant reductions in A1C (overall mean reduction20.84%) (17). Another meta-analysis by Yang and Fang(18), with data from 3,360 patients in 22 trials, notedsignificant reductions in fasting blood glucose, 2-hourpostprandial blood glucose, and A1C levels comparedwith individuals in control groups.
Study Objectives
The first aim of this quality improvement (QI) project wasto determine whether implementing a culturally sensitiveHealthy Interactions Conversations Maps DSME programwith peer educators for Latinos with type 2 diabetes in acommunity health clinic could improve self-efficacy asmeasured by the Lifestyle Self-Efficacy Scale for Latinoswith Diabetes (LSESLD) (19). The LSESLD was used toassess participants for improvement in perceived controland confidence over 6 months. The second aim of theproject was to determine whether implementation of thisprogram over 6 months could reduce DD as measuredby the 17-item Diabetes Distress Scale (DDS-17) (20).A final aim was to improve A1C by 0.5–1.0% within6 months for patients with an A1C .7% at baseline.
Design and Methods
This QI project had a two-sample, paired, pre-/post-testintervention design. Outcome variables included self-efficacy, DD, depression, and A1C. Descriptive dataincluded participants’ sex, age, country of origin, BMI,insulin use, duration of diabetes, history of hypertensionand hyperlipidemia, and number of DSME sessionsattended. The LSESLD was used to assess self-efficacyrelated to diabetes self-management (19). The DDS-17was used to measure changes in DD (21). Both scales wereused with the permission of their developers. The PatientHealth Questionnaire (PHQ-9) was used to screen forsymptoms of depression and is in the public domain (22).
The project was formally evaluated using a QI checklistand determined to not be human subject research byan internal review process at Duke University Schoolof Nursing.
Setting and Patient Population
The project was implemented at Camino CommunityCenter, a free health community clinic in theCharlotte, NC, metropolitan area. The free clinicserves ~3,000 patients who are mostly Latino and
214 CLINICAL.DIABETESJOURNALS.ORG
FEATURE ARTICLE Peer-Led DSME in Low-Income Latinos

all uninsured and earning less than 200% of the federalpoverty level. The community center provides severalservices, including a medical and mental health clinic,a food pantry, and a fitness center. Its mission is “toequip people to live healthy, hopeful, and productivelives” (23).
Each group session included 8–10 patients. Each par-ticipant was asked to physically attend four unique groupsessions within the 6-month period. Optional make-upsessions were offered for each Conversation Map dis-cussion session at the end of the 6-month period. Patientswere eligible to participate if they were low-income(,200% of the poverty level), $18 years of age, andhad uncontrolled type 2 diabetes as indicated by anA1C .7%. Exclusion criteria included the presenceof end-stage renal disease, diagnosed pregnancy, orimpaired vision or blindness.
The clinic staff includes one physician, one nursepractitioner, a CDE, a diabetes health coach, an adultpsychologist, and two peer educators, all of whom arebilingual. Sending routine motivational text messagesto patients between appointments, with the objectiveof maintaining patient engagement, is a standard of carein the clinic.
Gaining access to bilingual providers has been achronic challenge for patients at the clinic; thereis an average wait time of more than 2 months forappointments for new diabetes patients. HCP visitshave also been lengthy because of the time spentattempting to educate patients about diabetesself-management. One goal of this project was toimprove access to HCPs by adopting a group caremodel and thereby reduce wait times for newpatients and improve attendance at DSMEsessions.
Data Collection
The project was championed by the full-time family nursepractitioner at the clinic and lasted for 8 months. The peereducators were patients with diabetes who had suc-cessfully completed DSME, had high literacy, and couldnavigate the U.S. Conversation Maps easily. Peer edu-cators signed a confidentiality and participation agree-ment form before participating and received facilitatortraining in the use of the Healthy Interactions U.S.Conversation Maps (16). Both the CDE and the diabeteshealth coach also completed facilitator training andagreed to participate in the DSME sessions. Facilita-tor training occurred in two 1.5-hour sessions inSeptember 2018.
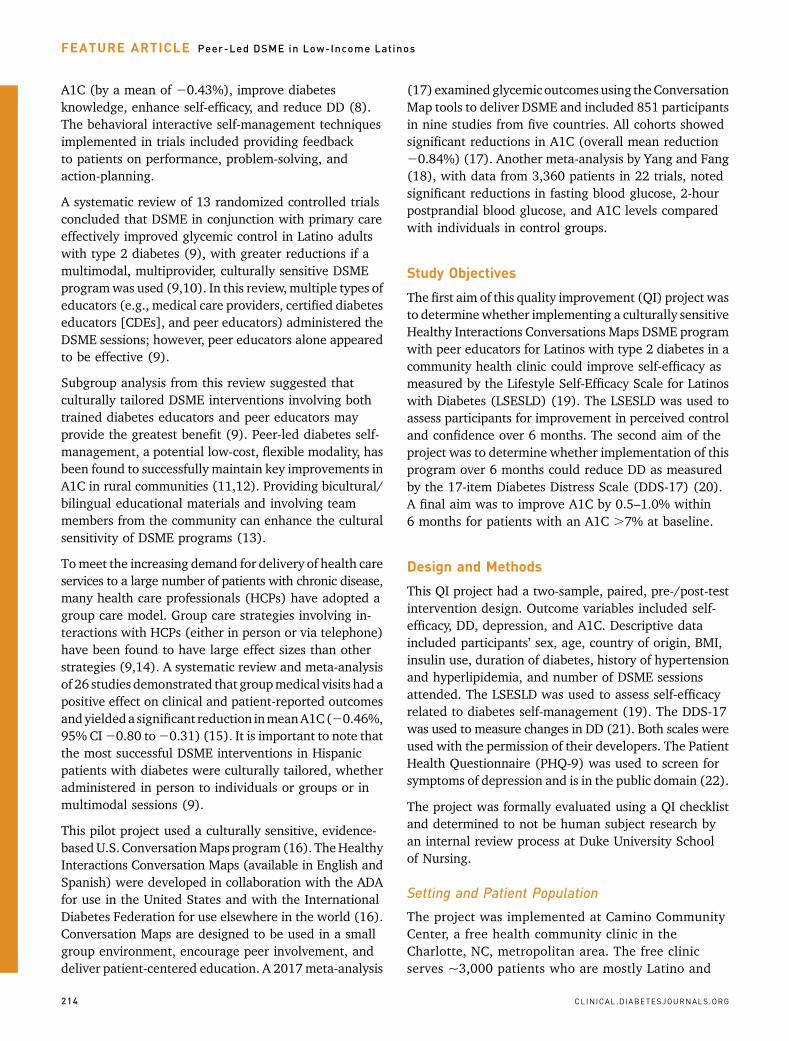
The medical care providers invited patients to participatein group care during regularly scheduled appointmentsin themonths before the program’s implementation, afterreviewing patients’medical records for inclusion criteria.The clinic adapted its scheduling system in anticipation ofscheduling 8–10 patients for each diabetes group session,preferably on the same day of their HCP office visit, tofacilitate implementing the group care model. The groupsessions were held three times monthly during the8-month implementation period. Group sessions weresuspended for December holidays because of anticipatedlow attendance. Each group was limited to 8–10participants (Figure 1).
Participants began inSeptember 2018by completing theirpre-implementation questionnaires (PHQ-9,DDS-17, andLSESLD) in either a hard copy format or an electronic,Health Insurance Portability and Accountability Act–compliant JotForm format via a digital tablet (19,20,22).The LSESLD demonstrates good internal consistency,reasonable construct validity, and sensitivity tointervention-related changes over time (19). It has beenfound to be a reliable and valid research instrumentfor assessing self-efficacy related to diabetes self-management in low-income, Spanish-speaking pop-ulations (19). The DDS-17 also demonstrates strongreliability, good convergent validity, and excellent crite-rion validity, making it an excellent psychometric in-strument for identifying DD (21). The PHQ-9 is a validatedbrief questionnaire with a sensitivity of 88% and aspecificity of 88% for identifying symptoms ofdepression (22).
Responses from the pre-implementation questionnaireswere loaded into the electronic health record (EHR)system and into an Excel spreadsheet for laterstatistical analysis. If moderate to severe levels ofdepression were found via the PHQ-9, those patientswere automatically referred to the clinic’s mental healththerapy department. Blood was drawn before patientsleft their initial visit and sent to Quest Laboratory forA1C analysis.
Each group session lasted for 1–1.5 hours. For two of thediabetes group sessions, patients were also scheduled tosee their HCP individually for their usual quarterly 15-minute follow-up appointments, which took place eitherjust before or just after the group session, and their bloodwas drawn for A1C measurement as part of these routinevisits. During the months with no group visits scheduled(December and March), all patients were engaged via atelephone medical encounter, and a follow-up motiva-tional text message was sent after those encounters.
VOLUME 38, NUMBER 3, SUMMER 2020 215
FALLAS ET AL.
Additional clinic visitswere addeduponpatient request ornecessity. Make-up sessions were offered in March 2019.
Post-implementation questionnaires were administeredin March and April during patients’ final visit for labo-ratory testing and were entered into the EHR system andExcel spreadsheet.
Data Analysis
Descriptive statistics were used to summarize the data.Paired t tests were conducted to determine differencesfrom baseline measurements to end-of-program mea-surements. Data analysis was performed with SPSSstatistical software, v. 24.0 (IBM, Armonk, NY) (24).Because female sex and depressive symptoms are po-tential confounders to accurate assessment of DD (25),a repeated-measures ANCOVA (rANCOVA) was per-formed to adjust for these factors. The rANCOVAcompares means across one or more variables that are
based on repeated observations while controlling for aconfounding variable.
Results
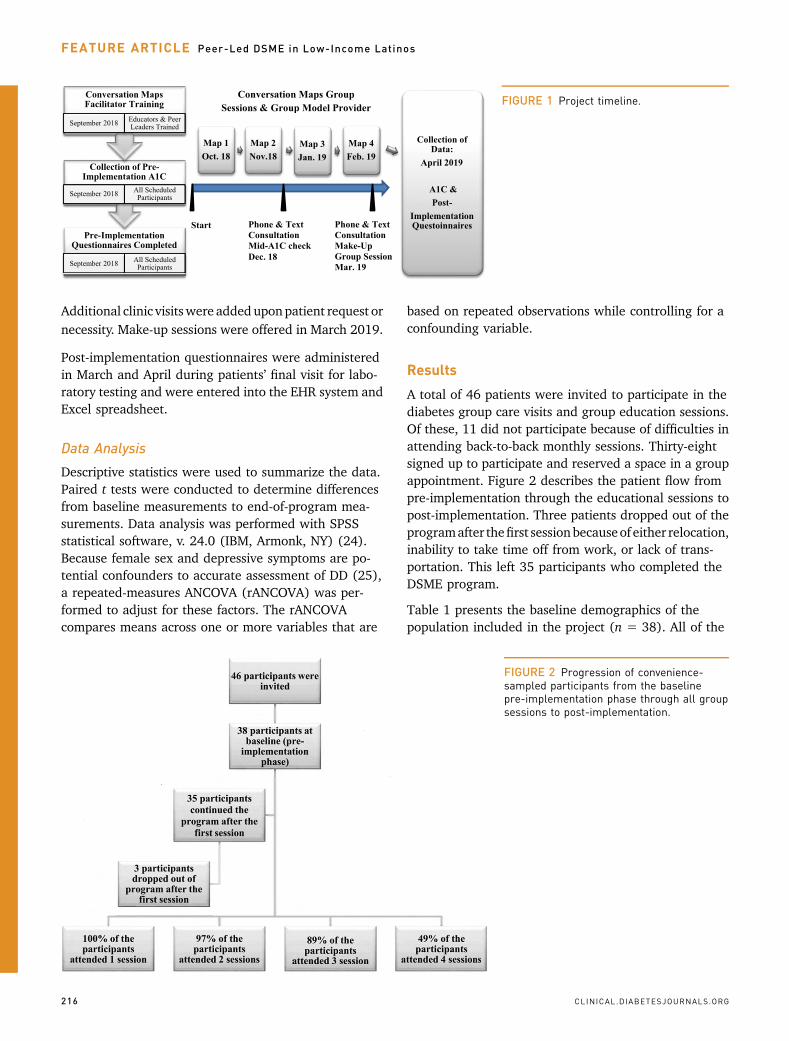
A total of 46 patients were invited to participate in thediabetes group care visits and group education sessions.Of these, 11 did not participate because of difficulties inattending back-to-back monthly sessions. Thirty-eightsigned up to participate and reserved a space in a groupappointment. Figure 2 describes the patient flow frompre-implementation through the educational sessions topost-implementation. Three patients dropped out of theprogramafter thefirst sessionbecauseof either relocation,inability to take time off from work, or lack of trans-portation. This left 35 participants who completed theDSME program.
Table 1 presents the baseline demographics of thepopulation included in the project (n 5 38). All of the
FIGURE 1 Project timeline.
FIGURE 2 Progression of convenience-sampled participants from the baselinepre-implementation phase through all groupsessions to post-implementation.
216 CLINICAL.DIABETESJOURNALS.ORG
FEATURE ARTICLE Peer-Led DSME in Low-Income Latinos
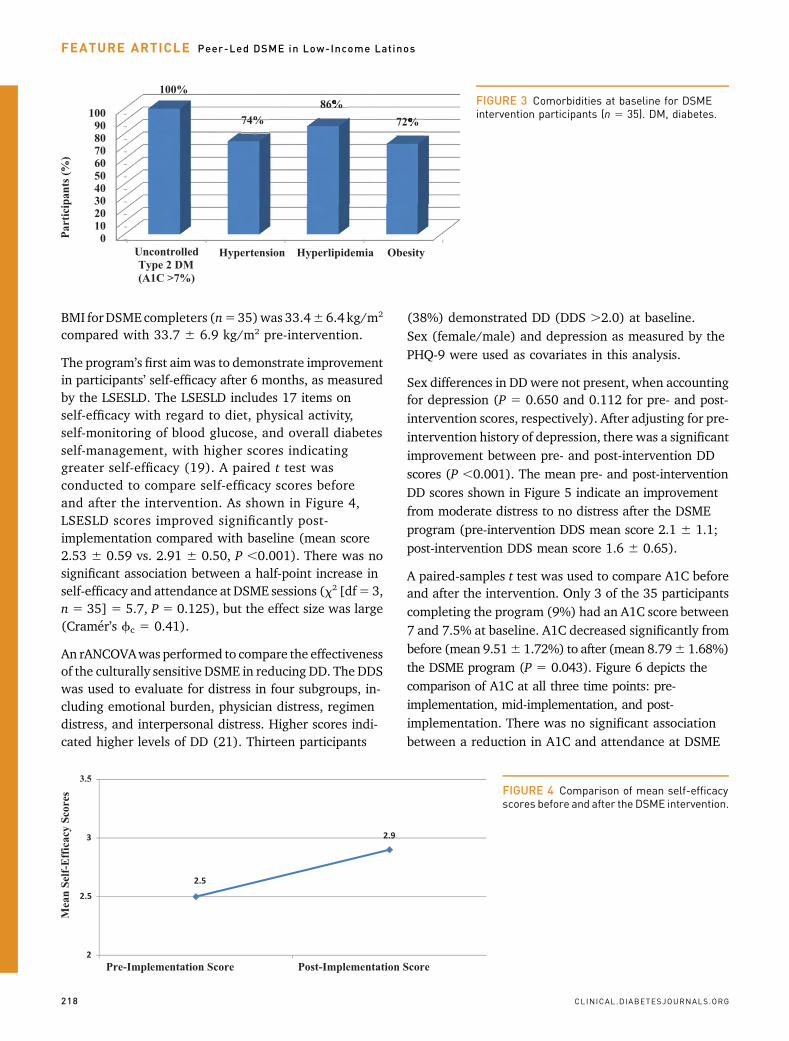
participants were of Latino descent, lacked medicalinsurance, earned less than 200% of the federal povertylevel, and were overweight or obese. The mean durationof diabetes for all 38 participants was 5.68 6 3.2 years.More than half of the participants (58%) used insulin.Most participants had hypertension, hyperlipidemia,uncontrolled blood glucose, and obesity, indicatingthat they were at high risk of developing diabetes
complications. Figure 3 depicts the percentage ofcomorbidities in patients who completed the DSMEintervention.
Of those who completed the DSME program(n 5 35), 89% attended three sessions, and 49%attended four sessions. Although lowering BMI was nota primary aim of the program, mean post-intervention
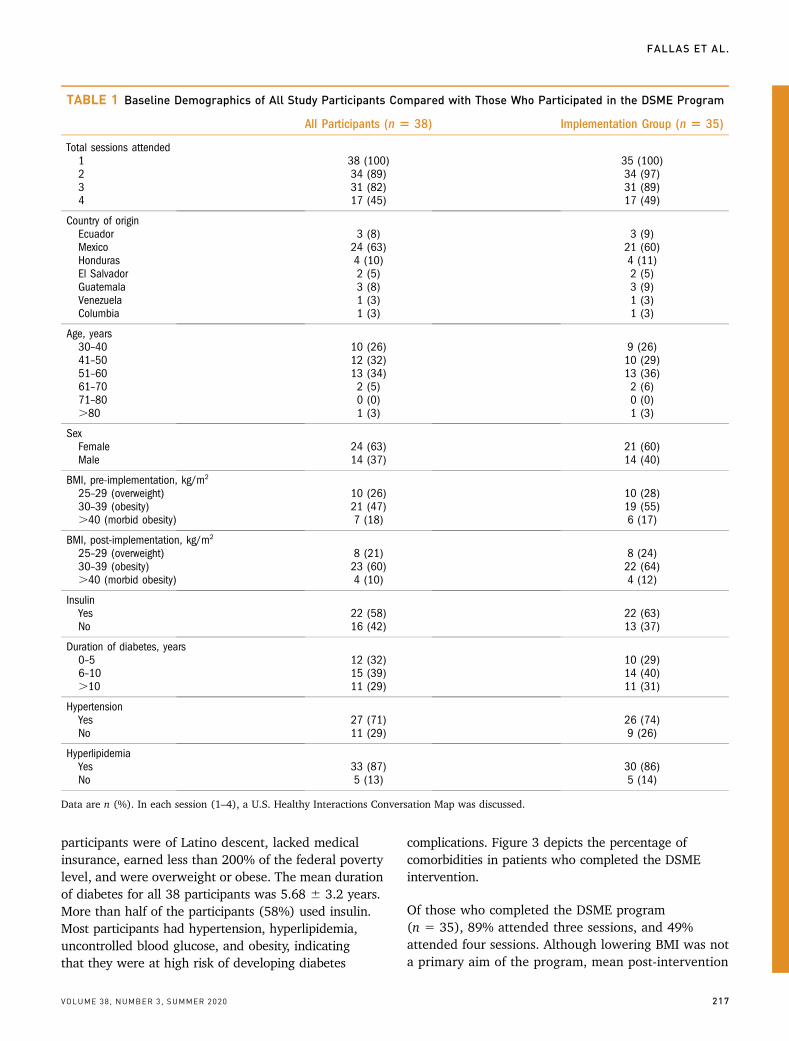
TABLE 1 Baseline Demographics of All Study Participants Compared with Those Who Participated in the DSME Program
All Participants (n 5 38) Implementation Group (n 5 35)
Total sessions attended1 38 (100) 35 (100)2 34 (89) 34 (97)3 31 (82) 31 (89)4 17 (45) 17 (49)
Country of originEcuador 3 (8) 3 (9)Mexico 24 (63) 21 (60)Honduras 4 (10) 4 (11)El Salvador 2 (5) 2 (5)Guatemala 3 (8) 3 (9)Venezuela 1 (3) 1 (3)Columbia 1 (3) 1 (3)
Age, years30–40 10 (26) 9 (26)41–50 12 (32) 10 (29)51–60 13 (34) 13 (36)61–70 2 (5) 2 (6)71–80 0 (0) 0 (0).80 1 (3) 1 (3)
SexFemale 24 (63) 21 (60)Male 14 (37) 14 (40)
BMI, pre-implementation, kg/m2
25–29 (overweight) 10 (26) 10 (28)30–39 (obesity) 21 (47) 19 (55).40 (morbid obesity) 7 (18) 6 (17)
BMI, post-implementation, kg/m2
25–29 (overweight) 8 (21) 8 (24)30–39 (obesity) 23 (60) 22 (64).40 (morbid obesity) 4 (10) 4 (12)
InsulinYes 22 (58) 22 (63)No 16 (42) 13 (37)
Duration of diabetes, years0–5 12 (32) 10 (29)6–10 15 (39) 14 (40).10 11 (29) 11 (31)
HypertensionYes 27 (71) 26 (74)No 11 (29) 9 (26)
HyperlipidemiaYes 33 (87) 30 (86)No 5 (13) 5 (14)
Data are n (%). In each session (1–4), a U.S. Healthy Interactions Conversation Map was discussed.
VOLUME 38, NUMBER 3, SUMMER 2020 217
FALLAS ET AL.
BMI forDSME completers (n535)was 33.466.4 kg/m2
compared with 33.7 6 6.9 kg/m2 pre-intervention.
The program’s first aimwas to demonstrate improvementin participants’ self-efficacy after 6 months, as measuredby the LSESLD. The LSESLD includes 17 items onself-efficacy with regard to diet, physical activity,self-monitoring of blood glucose, and overall diabetesself-management, with higher scores indicatinggreater self-efficacy (19). A paired t test wasconducted to compare self-efficacy scores beforeand after the intervention. As shown in Figure 4,LSESLD scores improved significantly post-implementation compared with baseline (mean score2.53 6 0.59 vs. 2.91 6 0.50, P ,0.001). There was nosignificant association between a half-point increase inself-efficacy and attendance at DSME sessions (x2 [df5 3,n 5 35] 5 5.7, P 5 0.125), but the effect size was large(Cramer’s fc 5 0.41).
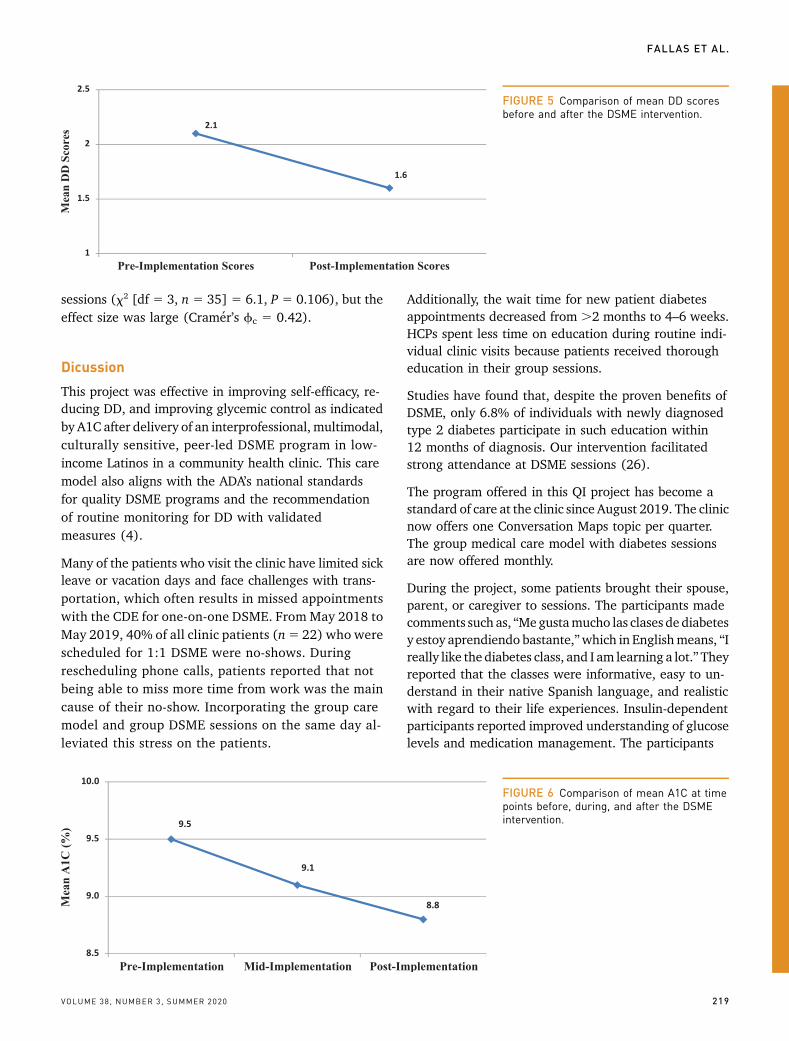
An rANCOVAwas performed to compare the effectivenessof the culturally sensitive DSME in reducing DD. The DDSwas used to evaluate for distress in four subgroups, in-cluding emotional burden, physician distress, regimendistress, and interpersonal distress. Higher scores indi-cated higher levels of DD (21). Thirteen participants
(38%) demonstrated DD (DDS .2.0) at baseline.Sex (female/male) and depression as measured by thePHQ-9 were used as covariates in this analysis.
Sex differences in DD were not present, when accountingfor depression (P 5 0.650 and 0.112 for pre- and post-intervention scores, respectively). After adjusting for pre-intervention history of depression, there was a significantimprovement between pre- and post-intervention DDscores (P ,0.001). The mean pre- and post-interventionDD scores shown in Figure 5 indicate an improvementfrom moderate distress to no distress after the DSMEprogram (pre-intervention DDS mean score 2.1 6 1.1;post-intervention DDS mean score 1.6 6 0.65).
A paired-samples t test was used to compare A1C beforeand after the intervention. Only 3 of the 35 participantscompleting the program (9%) had an A1C score between7 and 7.5% at baseline. A1C decreased significantly frombefore (mean 9.516 1.72%) to after (mean 8.796 1.68%)the DSME program (P 5 0.043). Figure 6 depicts thecomparison of A1C at all three time points: pre-implementation, mid-implementation, and post-implementation. There was no significant associationbetween a reduction in A1C and attendance at DSME
FIGURE 3 Comorbidities at baseline for DSMEintervention participants (n 5 35). DM, diabetes.
FIGURE 4 Comparison of mean self-efficacyscores before and after the DSME intervention.
218 CLINICAL.DIABETESJOURNALS.ORG
FEATURE ARTICLE Peer-Led DSME in Low-Income Latinos
sessions (x2 [df 5 3, n 5 35] 5 6.1, P 5 0.106), but theeffect size was large (Cramer’s fc 5 0.42).
Dicussion
This project was effective in improving self-efficacy, re-ducing DD, and improving glycemic control as indicatedby A1C after delivery of an interprofessional, multimodal,culturally sensitive, peer-led DSME program in low-income Latinos in a community health clinic. This caremodel also aligns with the ADA’s national standardsfor quality DSME programs and the recommendationof routine monitoring for DD with validatedmeasures (4).
Many of the patients who visit the clinic have limited sickleave or vacation days and face challenges with trans-portation, which often results in missed appointmentswith the CDE for one-on-one DSME. From May 2018 toMay 2019, 40% of all clinic patients (n5 22) who werescheduled for 1:1 DSME were no-shows. Duringrescheduling phone calls, patients reported that notbeing able to miss more time from work was the maincause of their no-show. Incorporating the group caremodel and group DSME sessions on the same day al-leviated this stress on the patients.
Additionally, the wait time for new patient diabetesappointments decreased from .2 months to 4–6 weeks.HCPs spent less time on education during routine indi-vidual clinic visits because patients received thorougheducation in their group sessions.
Studies have found that, despite the proven benefits ofDSME, only 6.8% of individuals with newly diagnosedtype 2 diabetes participate in such education within12 months of diagnosis. Our intervention facilitatedstrong attendance at DSME sessions (26).
The program offered in this QI project has become astandard of care at the clinic since August 2019. The clinicnow offers one Conversation Maps topic per quarter.The group medical care model with diabetes sessionsare now offered monthly.
During the project, some patients brought their spouse,parent, or caregiver to sessions. The participants madecomments such as, “Megustamucho las clases de diabetesy estoy aprendiendo bastante,”which in Englishmeans, “Ireally like the diabetes class, and I am learning a lot.”Theyreported that the classes were informative, easy to un-derstand in their native Spanish language, and realisticwith regard to their life experiences. Insulin-dependentparticipants reported improved understanding of glucoselevels and medication management. The participants
FIGURE 5 Comparison of mean DD scoresbefore and after the DSME intervention.
FIGURE 6 Comparison of mean A1C at timepoints before, during, and after the DSMEintervention.
VOLUME 38, NUMBER 3, SUMMER 2020 219
FALLAS ET AL.

enjoyed hearing testimonies from their peer educators.During each session, patients were offered healthfulsnacks or meals to try that were often cooked by the peereducators themselves. Sample foods included homemadevegan tortillas, quinoa salad with reduced-carbohydratetortilla chips, black rice, Greek yogurt, and fruits.
Patients had an opportunity towrite their short- and long-term goals and to plan and document how they wouldengage with a support network or their health care teamto improve their diabetes control and overcome barriersthey faced. As a result, patients reporting financialdifficulties with regard to purchasing groceries werereferred to the community center’s food pantry. Otherpatientswere referred to theNCMedassist Pharmacy (27)for free medications or provided with free samples fromthe medical assistance program Americares (28). Thosewho reported a lack of access to exercise equipment wereoffered a monthly subscription to the community center’sCamino Fitness gym, which was conveniently locatedbeside the clinic.
Limitations
A few limitations to this project that should beacknowledged. Group sessions were clustered back-to-back in a 6-month time period. However, each U.S.Healthy Interactions Conversation Map has a separatefocus, and the maps do not have to be used in a specificsequence. Thus, it would be easy for patients to attenddiabetes group sessions every 3months on the samedayastheir routine follow-up medical appointment. Thisscheduling change was permanently implemented afterthepilot project, starting inAugust 2019,which facilitatedsustainable, comprehensive care without requiring pa-tients to miss additional time from work.
Screening questionnaires were offered in both paper andelectronic formats. However, it was quickly noticed thatpatients were having great difficulties in completing theirforms electronically via the tablet because of eitherliteracy challenges or discomfort with the technology.Future sessions will assign a staff person to assist patientswith questionnaires.
Public safety was one social determinant of health thataffected patients during their group DSME program.During the last 3 months of the program, local immi-gration laws were heavily enforced in the Charlotte, NC,region creating fear and safety concerns for many of ourparticipants. These concerns led many to refuse to leavetheir home to pick up their prescriptions at the pharmacy.On a more positive note, the clinic provides compre-hensive services for patients who cannot overcome other
social determinants of health. For example, the clinicoffered quick access to the light rail transportation systemlocated just behind the community center. The center alsoprovided an array of professional and social supportduring the group sessions thatmay not have been practicalto provide in other settings.
A final limitation was the project’s small sample size.Repeating this QI project with a larger population ofpatients could provide more information to inform bestpractices for implementation.
Conclusion
Self-efficacy scores, A1C, and DD all improved in patientswho attended this culturally sensitive, peer-led DSMEprogram. Free community clinics serving Latinos shouldconsider implementing group care models with culturallysensitive DSME programs to help reduce delays inaccess to care, offset barriers associated with trans-portation or missed work time, and improve attendanceat follow-up appointments.
Our population earned ,200% of the federal povertylevel. Despite facing difficult social determinants ofhealth, these patients improved their self-efficacy, workedto expand their support network, and becamemore awareof the importance of asking for assistance. Programparticipants openly communicated their concerns and, inturn, received additional resources to improve theirquality of care. This process supports the SCT tenet thatindividuals with high self-efficacy will be more likely tochange their behavior and make healthier choices as theyacquire knowledge and gain confidence (6).
ACKNOWLEDGMENTS
The authors thank the administration and staff of CaminoCommunity Center for their continued support and for assistancewith this study. Theauthors also acknowledgeElenaTurner andJulie Thompson at Duke University and Eugene Wright at theDuke Southern Regional Area Health Education Center fortheir contributions.
DUALITY OF INTEREST
No potential conflicts of interest relevant to this article werereported.
AUTHOR CONTRIBUTIONS
C.R.F. researched data, wrote the manuscript, contributed todiscussion, and reviewed and edited the manuscript. K.P. wrotethe manuscript, contributed to discussion, and reviewed andedited the manuscript. B.I.P., I.F., and C.P. contributed to dis-cussion and reviewed and edited the manuscript. S.A. reviewedand edited the manuscript. C.R.F. is the guarantor of this work
220 CLINICAL.DIABETESJOURNALS.ORG
FEATURE ARTICLE Peer-Led DSME in Low-Income Latinos

and, as such, had full access to all the data in the study and takesresponsibility for the integrity of the data and the accuracy ofthe data analysis.
REFERENCES
1. Daviglus ML, Pirzada A, Talavera GA. Cardiovascular diseaserisk factors in the Hispanic/Latino population: lessons from theHispanic Community Health Study/Study of Latinos (HCHS/SOL).Prog Cardiovasc Dis 2014;57:230–236
2. Saydah S, Cowie C, Eberhardt MS, De Rekeneire N, NarayanKM. Race and ethnic differences in glycemic control amongadults with diagnosed diabetes in the United States. Ethn Dis2007;17:529–535
3. BanduraA. Self-efficacy: towardaunifying theory of behavioralchange. Psychol Rev 1977;84:191–215
4. American Diabetes Association. 5. Facilitating behaviorchange and well-being to improve health outcomes: Standards ofMedical Care in Diabetes—2020. Diabetes Care 2020;43(Suppl. 1):S48–S65
5. PintaudiB,LucisanoG,GentileS, et al.;BENCH-DStudyGroup.Correlatesofdiabetes-relateddistress in type2diabetes:findingsfrom the benchmarking network for clinical and humanisticoutcomes in diabetes (BENCH-D) study. J Psychosom Res 2015;79:348–354
6. Leyva B, Zagarins SE, Allen NA, Welch G. The relative impactof diabetesdistress vsdepressiononglycemiccontrol inHispanicpatients following a diabetes self-management education in-tervention. Ethn Dis 2011;21:322–327
7. Perrin NE, Davies MJ, Robertson N, Snoek FJ, Khunti K. Theprevalence of diabetes-specific emotional distress in peoplewithtype 2 diabetes: a systematic review and meta-analysis. DiabetMed 2017;34:1508–1520
8. Cheng L, Sit JW, Choi KC, Chair SY, Li X, He XL. Effectivenessof interactive self-management interventions in individualswith poorly controlled type 2 diabetes: a meta-analysis ofrandomized controlled trials. Worldviews Evid Based Nurs2017;14:65–73
9. Ferguson S, Swan M, Smaldone A. Does diabetes self-management education in conjunctionwithprimary care improveglycemic control in Hispanic patients? A systematic review andmeta-analysis. Diabetes Educ 2015;41:472–484
10. Wang ML, Lemon SC, Whited MC, Rosal MC. Who benefitsfrom diabetes self-management interventions? The influence ofdepression in the Latinos en Control trial. Ann Behav Med 2014;48:256–264
11. SpencerMS,KiefferEC,SincoB,etal.Outcomesat18monthsfrom a community health worker and peer leader diabetes self-management program for Latino adults. Diabetes Care 2018;41:1414–1422
12. Piatt GA, Rodgers EA, Xue L, Zgibor JC. Integration andutilizationofpeer leaders fordiabetesself-managementsupport:results from project SEED (Support, Education, and Evaluationin Diabetes). Diabetes Educ 2018;44:373–382
13. Welch G, Allen NA, Zagarins SE, Stamp KD, Bursell SE,Kedziora RJ. Comprehensive diabetesmanagement program for
poorly controlled Hispanic type 2 patients at a community healthcenter. Diabetes Educ 2011;37:680–688
14. Fan L, Sidani S. Effectiveness of diabetes self-managementeducation interventionelements:ameta-analysis.CanJDiabetes2009;33:18–26
15. Housden L, Wong ST, Dawes M. Effectiveness of groupmedical visits for improving diabetes care: a systematic reviewand meta-analysis. CMAJ 2013;185:E635–E644
16. Healthy Interactions.ConversationMaps,2018.Available fromhttps://healthyinteractions.com. Accessed 20 September 2017
17. Eichorst B, Raia R. Meta-analysis of the glycemic outcomeswith the use of the Conversation Map tools to delivery diabetesself-managementeducationandsupport (DSME/S). Available fromhttps://healthyinteractions.com/assets/files/AADE_Poster.pdf.Accessed 21 September 2017
18. Yang Q, Fang P. Impact of the conversation map tools inpatients with type 2 diabetes mellitus: a PRISMA-compliantmeta-analysis of randomized controlled trials. Medicine(Baltimore) 2016;95:e4664
19. Wang ML, Lemon SC, Welch G, Rosal MC. Development andvalidation of the Lifestyle Self-Efficacy Scale for Latinos withDiabetes (LSESLD). Ethn Dis 2013;23:428–435
20. PolonskyWH,FisherL,EarlesJ, et al. Assessingpsychosocialdistress in diabetes: development of the diabetes distress scale.Diabetes Care 2005;28:626–631
21. SchmittA,ReimerA,KulzerB,HaakT,EhrmannD,HermannsN. How to assess diabetes distress: comparison of the ProblemAreas in Diabetes Scale (PAID) and the Diabetes Distress Scale(DDS). Diabet Med 2016;33:835–843
22. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of abrief depression severity measure. J Gen Intern Med 2001;16:606–613
23. Camino Community Center. Homepage. Available fromhttps://caminocommunitycenter.org. Accessed 21 September2017
24. Corporation IBM. IBM Stastistics GradPak, 2006. Availablefrom https://www.ibm.com/us-en/marketplace/spss-statistics-gradpack. Accessed 30 August 2017
25. Beck J, Greenwood DA, Blanton L, et al.; 2017 StandardsRevision Task Force. 2017 National Standards for Diabetes Self-Management Education and Support. Diabetes Educ 2017;43:449–464
26. Powers MA, Bardsley J, Cypress M, et al. Diabetes self-management education and support in type 2 diabetes: ajoint position statement of the American Diabetes Association,the American Association of Diabetes Educators, and theAcademy of Nutrition and Dietetics. Diabetes Care 2015;38:1372–1382
27. NC MedAssist. NC MedAssist pharmacy. Available fromhttps://medassist.org. Accessed 10 May 2019
28. Americares. Americares US access. Available from https://usaccess.americares.org/index.php. Accessed 10 May 2019
VOLUME 38, NUMBER 3, SUMMER 2020 221
FALLAS ET AL.