Embed Size (px)
Citation preview

©2017 AHIMA’s Intellectual Property. All rights reserved.
Improving Revenue, CMI and Quality Care
with Documentation
Wilbur Lo, MD, CDIP, CCA
AHIMA World Congress Faculty
AHIMA
©2017 AHIMA’s Intellectual Property. All rights reserved.
OBJECTIVES
• Discuss two definitions of case mix index (CMI)
• Differentiate CMI concept with sample calculations
• Discuss complex, clinical case scenarios
– Provide examples of inappropriate vs. appropriate
documentation and the impact on CMI
– Offer insight on analyzing CMI trends, with respect to revenue
and quality care
2
©2017 AHIMA’s Intellectual Property. All rights reserved.
Clinical Definition of CMI
Clinical Definition: For each inpatient facility, CMI reflects
level of sickness of patient population, with respect to the
following:
• Severity of illness
• Risk of mortality
• Prognosis
• Treatment difficulty
• Need for intervention
3
©2017 AHIMA’s Intellectual Property. All rights reserved.
Reimbursement Definition of CMI
Reimbursement Definition: For each inpatient facility, CMI
is a direct measure of amount of resource consumption and
cost to provide patient care
• CMI is a calculation, based on average of sum of relative
weights (values) of DRGs (e.g., IR-DRGs, AR-DRGs,
MS-DRGs) of all patients treated during a specific time
period
• Higher CMIs correspond to increased consumption of
resources, increased cost of patient care and increased
reimbursement to facility from government and private
payers
4
©2017 AHIMA’s Intellectual Property. All rights reserved.
Calculation of CMI: Scenario #1
• Scenario #1: Hospital “X” discharged 200 patients in
August 2017; all discharge diagnoses were documented
correctly
– 100 patients had discharge diagnosis of “sepsis”
[DRG relative weight (value) of 1.05; MS-DRG “872”]
– 100 patients had discharge diagnosis of “septic
shock” [DRG relative weight (value) of 1.81; MS-DRG
“871”]
– CMI calculations for Scenario #1 discussed in next
slide
5
©2017 AHIMA’s Intellectual Property. All rights reserved.
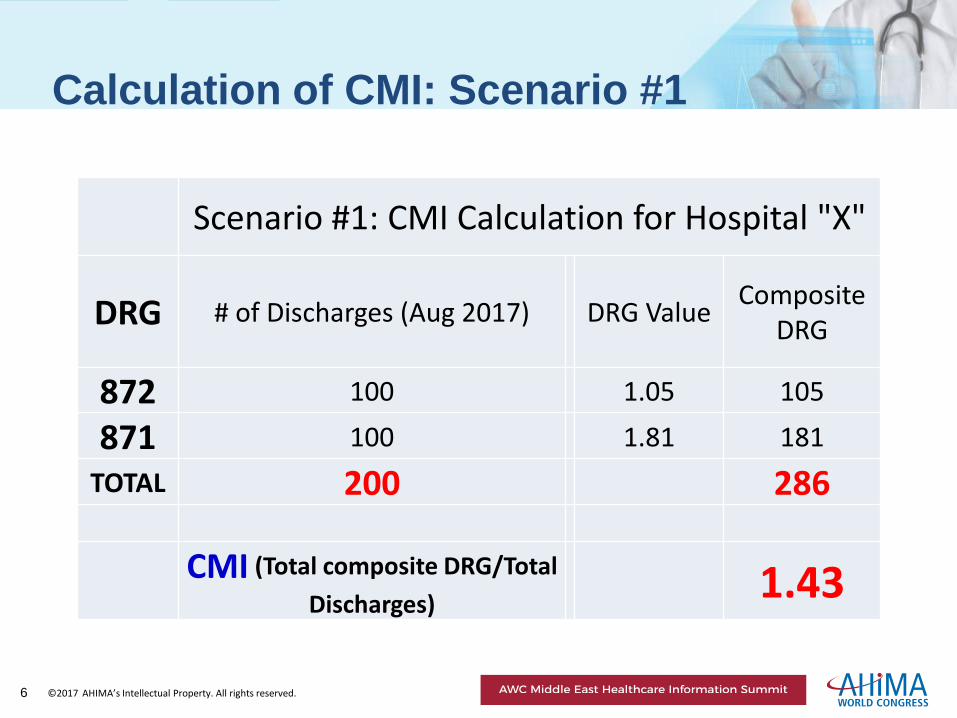
Calculation of CMI: Scenario #1
Scenario #1: CMI Calculation for Hospital "X"
DRG # of Discharges (Aug 2017) DRG Value Composite
DRG
872 100 1.05 105
871 100 1.81 181
TOTAL 200 286
CMI (Total composite DRG/Total
Discharges) 1.43
6
©2017 AHIMA’s Intellectual Property. All rights reserved.
Impact of Clinical Documentation
Improvement on CMI
• In Scenario #1, Hospital “X” discharged 200 patients in August 2017
– 100 patients were discharged with diagnosis of “sepsis” [DRG
relative weight (value) 1.05; MS-DRG “872”]
– 100 patients were discharged with diagnosis of “septic shock”
[DRG relative weight (value) 1.81; MS-DRG “871”]
• In Scenario #2, assume that improper documentation led to
discharge diagnoses of “sepsis” in 150 patients (instead of 100
patients) and “septic shock” in 50 patients (instead of 100 patients)
• CMI calculations for Scenario #2 discussed in next slide
7
©2017 AHIMA’s Intellectual Property. All rights reserved.
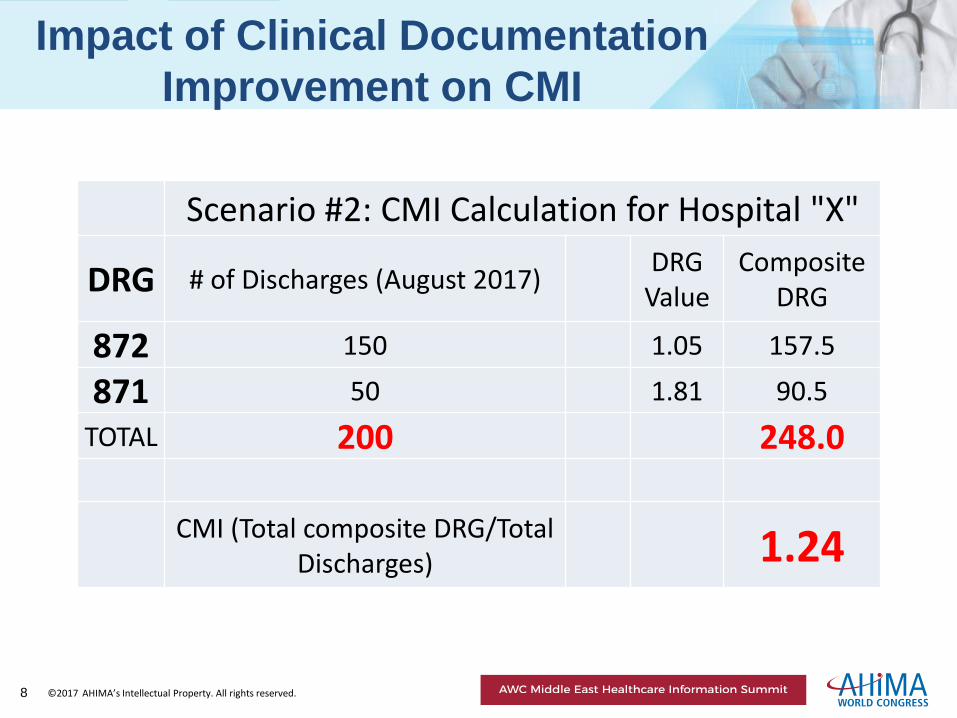
Impact of Clinical Documentation
Improvement on CMI
Scenario #2: CMI Calculation for Hospital "X"
DRG # of Discharges (August 2017) DRG
Value Composite
DRG
872 150 1.05 157.5
871 50 1.81 90.5
TOTAL 200 248.0
CMI (Total composite DRG/Total
Discharges) 1.24
8
©2017 AHIMA’s Intellectual Property. All rights reserved.
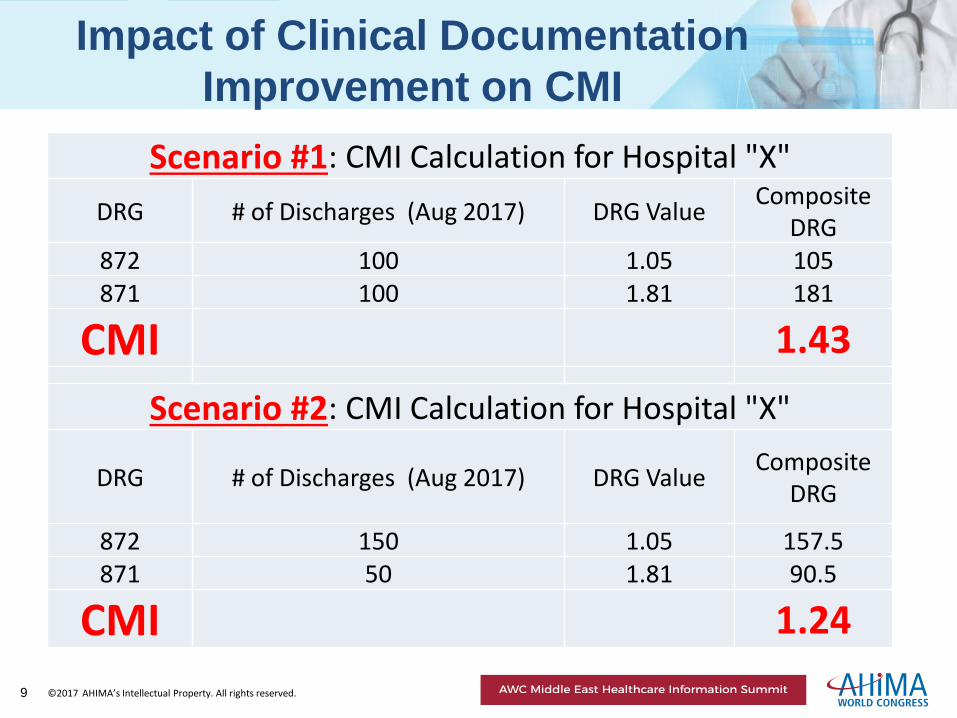
Impact of Clinical Documentation
Improvement on CMI
Scenario #1: CMI Calculation for Hospital "X"
DRG # of Discharges (Aug 2017) DRG Value Composite
DRG 872 100 1.05 105 871 100 1.81 181
CMI 1.43
Scenario #2: CMI Calculation for Hospital "X"
DRG # of Discharges (Aug 2017) DRG Value Composite
DRG
872 150 1.05 157.5 871 50 1.81 90.5
CMI 1.24
9
©2017 AHIMA’s Intellectual Property. All rights reserved.
CDI Case Studies with CMI
• Seven Characteristics of High Quality Clinical
Documentation
• Case Studies with Working DRGs and Target DRGs
• Calculation of CMI
10
©2017 AHIMA’s Intellectual Property. All rights reserved.
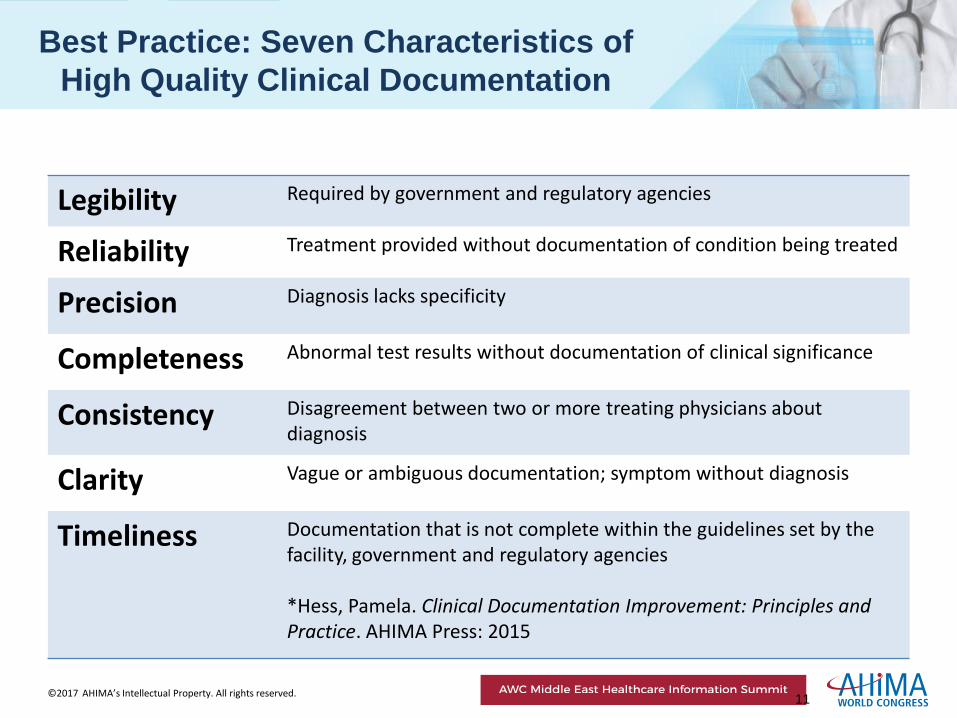
Best Practice: Seven Characteristics of
High Quality Clinical Documentation
Legibility Required by government and regulatory agencies
Reliability Treatment provided without documentation of condition being treated
Precision Diagnosis lacks specificity
Completeness Abnormal test results without documentation of clinical significance
Consistency Disagreement between two or more treating physicians about diagnosis
Clarity Vague or ambiguous documentation; symptom without diagnosis
Timeliness Documentation that is not complete within the guidelines set by the facility, government and regulatory agencies *Hess, Pamela. Clinical Documentation Improvement: Principles and Practice. AHIMA Press: 2015
11
©2017 AHIMA’s Intellectual Property. All rights reserved.
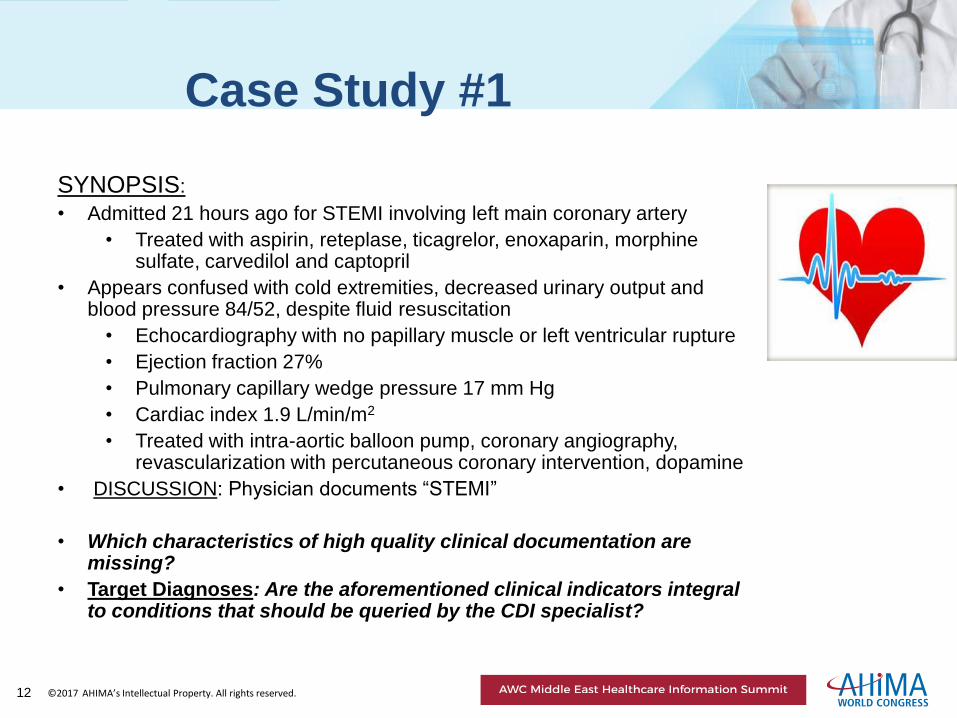
Case Study #1
SYNOPSIS:
• Admitted 21 hours ago for STEMI involving left main coronary artery
• Treated with aspirin, reteplase, ticagrelor, enoxaparin, morphine sulfate, carvedilol and captopril
• Appears confused with cold extremities, decreased urinary output and blood pressure 84/52, despite fluid resuscitation
• Echocardiography with no papillary muscle or left ventricular rupture
• Ejection fraction 27%
• Pulmonary capillary wedge pressure 17 mm Hg
• Cardiac index 1.9 L/min/m2
• Treated with intra-aortic balloon pump, coronary angiography, revascularization with percutaneous coronary intervention, dopamine
• DISCUSSION: Physician documents “STEMI”
• Which characteristics of high quality clinical documentation are missing?
• Target Diagnoses: Are the aforementioned clinical indicators integral to conditions that should be queried by the CDI specialist?
12
©2017 AHIMA’s Intellectual Property. All rights reserved.
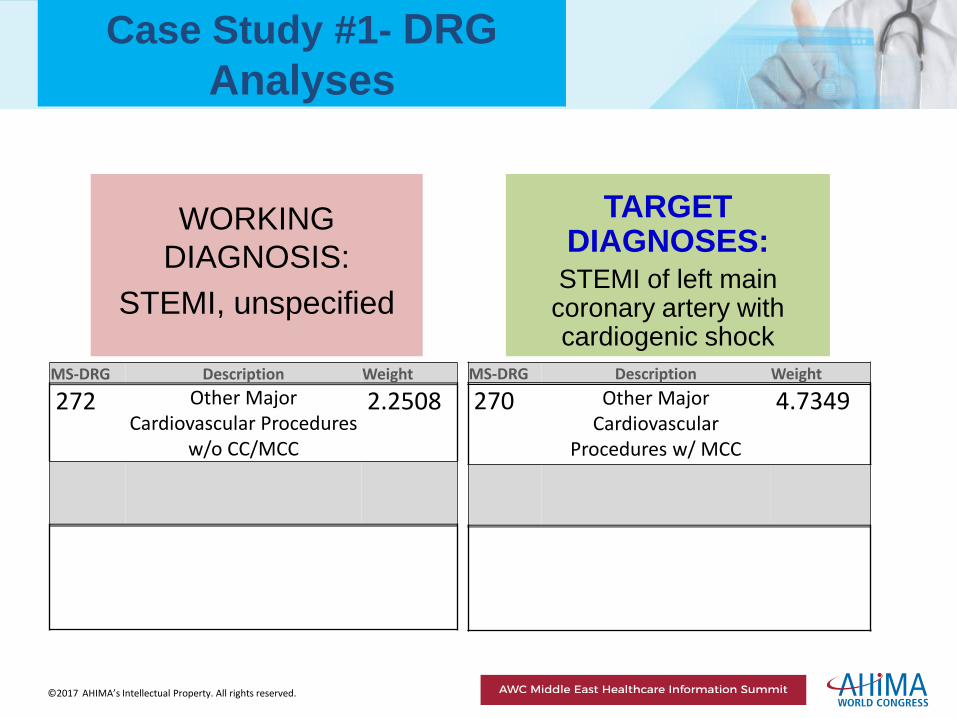
Case Study #1- DRG
Analyses
WORKING
DIAGNOSIS:
STEMI, unspecified
TARGET DIAGNOSES:
STEMI of left main coronary artery with cardiogenic shock
MS-DRG Description Weight
272 Other Major Cardiovascular Procedures
w/o CC/MCC
2.2508
MS-DRG Description Weight
270 Other Major Cardiovascular
Procedures w/ MCC
4.7349
©2017 AHIMA’s Intellectual Property. All rights reserved.
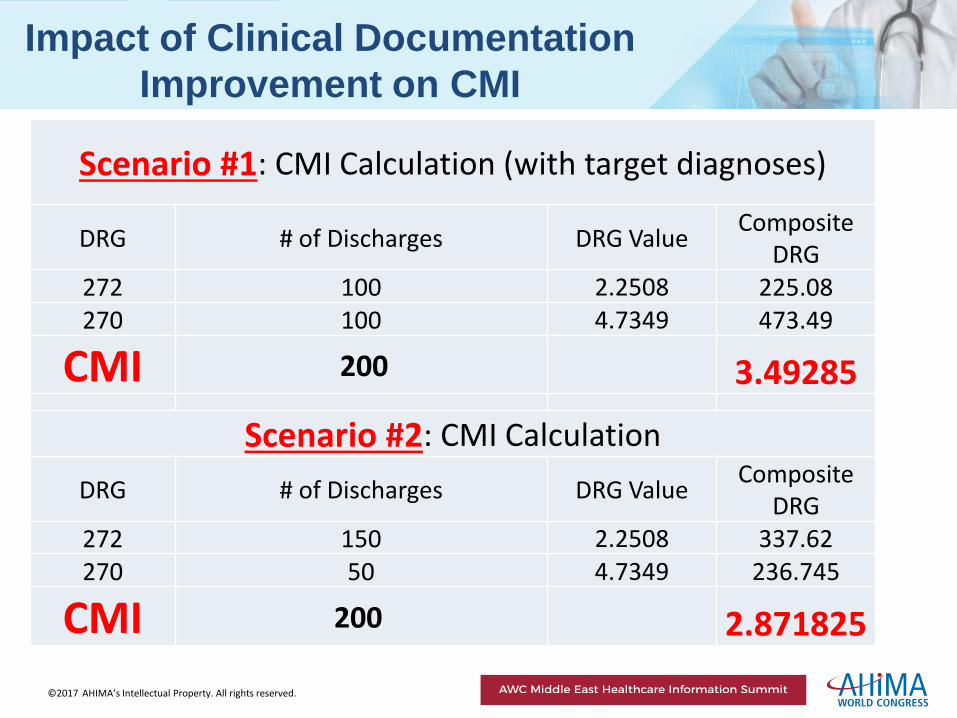
Impact of Clinical Documentation
Improvement on CMI
Scenario #1: CMI Calculation (with target diagnoses)
DRG # of Discharges DRG Value Composite
DRG 272 100 2.2508 225.08 270 100 4.7349 473.49
CMI 200 3.49285
Scenario #2: CMI Calculation
DRG # of Discharges DRG Value Composite
DRG 272 150 2.2508 337.62 270 50 4.7349 236.745
CMI 200 2.871825

©2017 AHIMA’s Intellectual Property. All rights reserved.
Case Study #2
Synopsis: • Admitted for paralysis and sensory loss of right face
and right upper extremity; bilateral visual loss in right hemifields
• Drowsiness, slurring of speech, unable to speak complete sentences; episode lasts 85 minutes; BP 158/96
• Diagnostic Tests:
• computed tomography- no acute intracranial hemorrhage
• electrocardiogram- no AMI or erratic atrial activity
• magnetic resonance angiography scheduled
• Treatment: recombinant tissue plasminogen activator, mannitol, anti-hypertensive medications
DISCUSSION: Physician documents “stroke”.
• Which characteristics of high quality clinical documentation are missing?
• Target Diagnoses: Are the aforementioned clinical indicators integral to conditions that should be queried by the CDI specialist?
©2017 AHIMA’s Intellectual Property. All rights reserved.
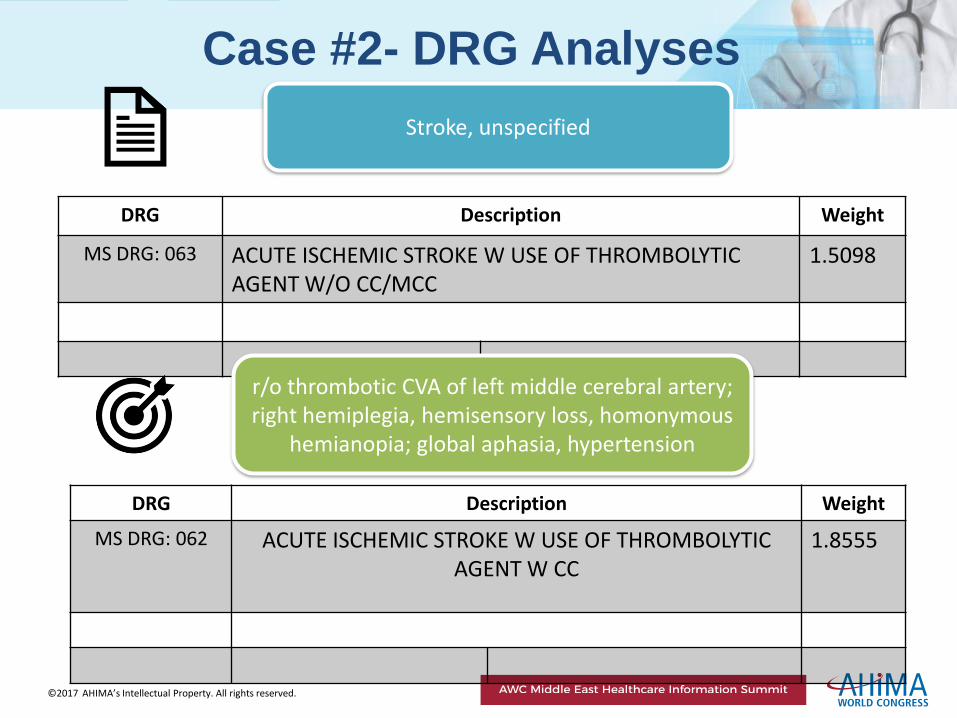
DRG Description Weight
MS DRG: 063 ACUTE ISCHEMIC STROKE W USE OF THROMBOLYTIC AGENT W/O CC/MCC
1.5098
Case #2- DRG Analyses
DRG Description Weight
MS DRG: 062 ACUTE ISCHEMIC STROKE W USE OF THROMBOLYTIC AGENT W CC
1.8555
Stroke, unspecified
r/o thrombotic CVA of left middle cerebral artery; right hemiplegia, hemisensory loss, homonymous
hemianopia; global aphasia, hypertension
©2017 AHIMA’s Intellectual Property. All rights reserved.
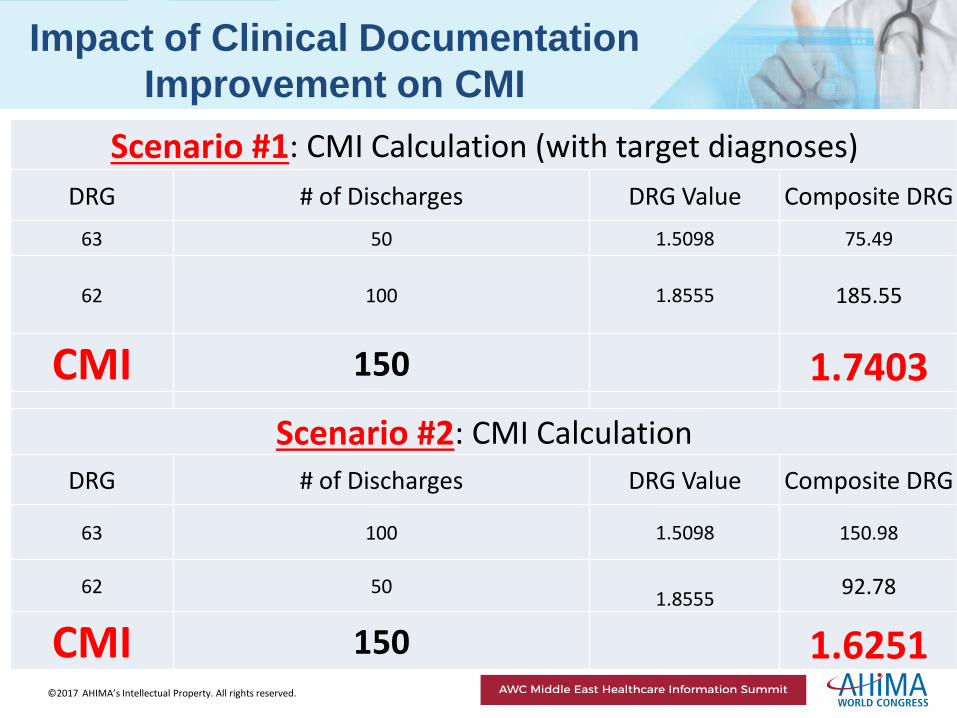
Impact of Clinical Documentation
Improvement on CMI
Scenario #1: CMI Calculation (with target diagnoses)
DRG # of Discharges DRG Value Composite DRG
63 50 1.5098 75.49
62 100
1.8555
185.55
CMI 150 1.7403
Scenario #2: CMI Calculation
DRG # of Discharges DRG Value Composite DRG
63 100 1.5098 150.98
62 50
1.8555 92.78
CMI 150 1.6251
©2017 AHIMA’s Intellectual Property. All rights reserved.
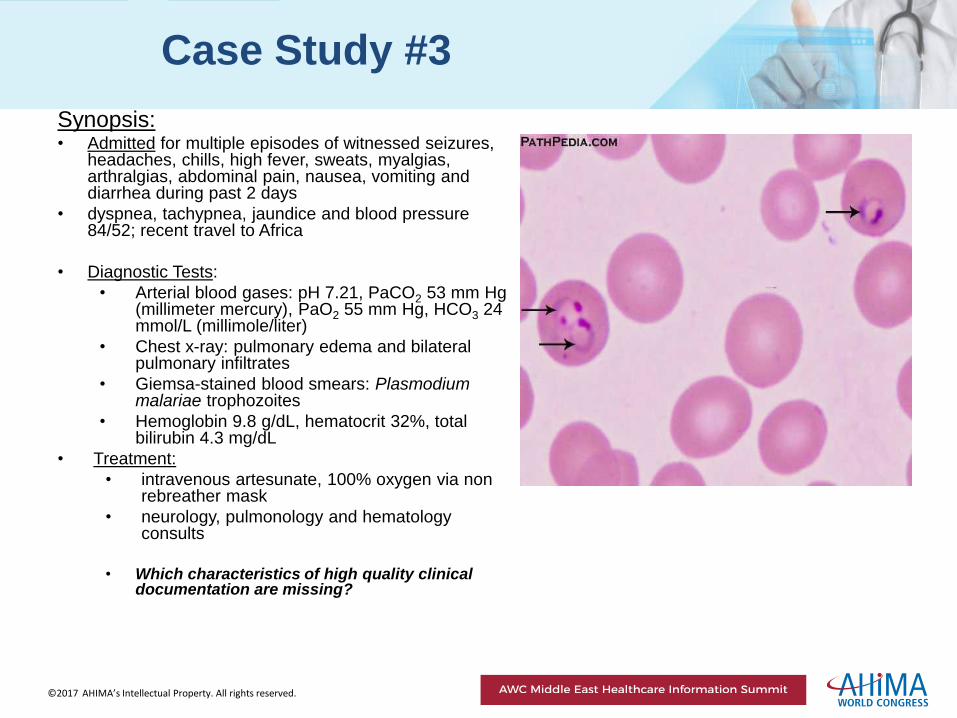
Case Study #3
Synopsis: • Admitted for multiple episodes of witnessed seizures,
headaches, chills, high fever, sweats, myalgias, arthralgias, abdominal pain, nausea, vomiting and diarrhea during past 2 days
• dyspnea, tachypnea, jaundice and blood pressure 84/52; recent travel to Africa
• Diagnostic Tests:
• Arterial blood gases: pH 7.21, PaCO2 53 mm Hg (millimeter mercury), PaO2 55 mm Hg, HCO3 24 mmol/L (millimole/liter)
• Chest x-ray: pulmonary edema and bilateral pulmonary infiltrates
• Giemsa-stained blood smears: Plasmodium malariae trophozoites
• Hemoglobin 9.8 g/dL, hematocrit 32%, total bilirubin 4.3 mg/dL
• Treatment:
• intravenous artesunate, 100% oxygen via non rebreather mask
• neurology, pulmonology and hematology consults
• Which characteristics of high quality clinical
documentation are missing?
©2017 AHIMA’s Intellectual Property. All rights reserved.
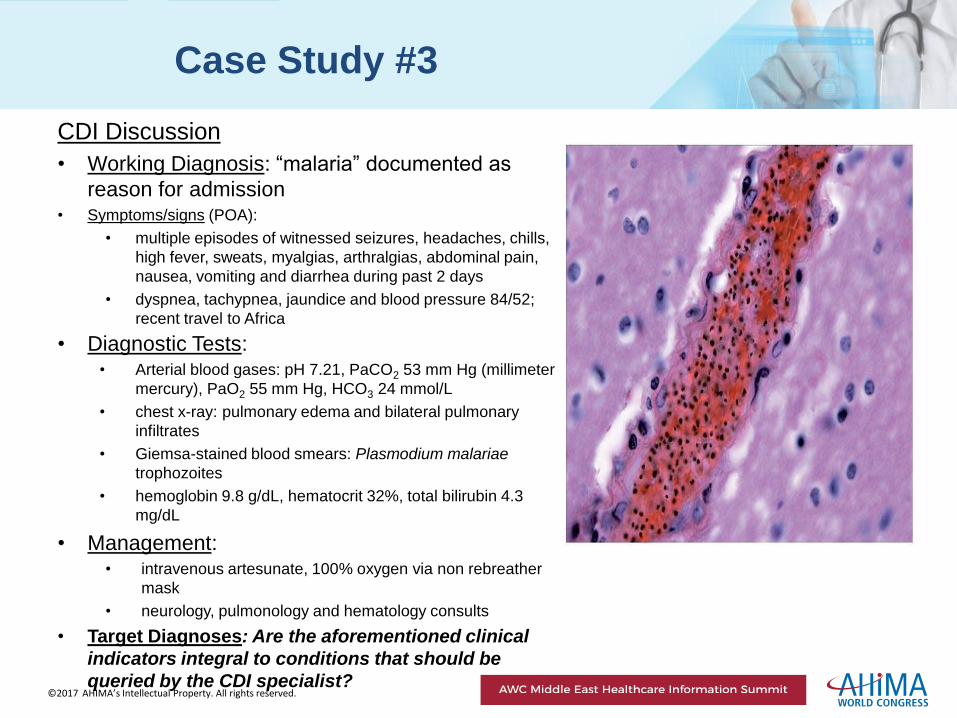
Case Study #3
CDI Discussion
• Working Diagnosis: “malaria” documented as
reason for admission • Symptoms/signs (POA):
• multiple episodes of witnessed seizures, headaches, chills,
high fever, sweats, myalgias, arthralgias, abdominal pain,
nausea, vomiting and diarrhea during past 2 days
• dyspnea, tachypnea, jaundice and blood pressure 84/52;
recent travel to Africa
• Diagnostic Tests: • Arterial blood gases: pH 7.21, PaCO2 53 mm Hg (millimeter
mercury), PaO2 55 mm Hg, HCO3 24 mmol/L
• chest x-ray: pulmonary edema and bilateral pulmonary
infiltrates
• Giemsa-stained blood smears: Plasmodium malariae
trophozoites
• hemoglobin 9.8 g/dL, hematocrit 32%, total bilirubin 4.3
mg/dL
• Management: • intravenous artesunate, 100% oxygen via non rebreather
mask
• neurology, pulmonology and hematology consults
• Target Diagnoses: Are the aforementioned clinical
indicators integral to conditions that should be
queried by the CDI specialist?
©2017 AHIMA’s Intellectual Property. All rights reserved.
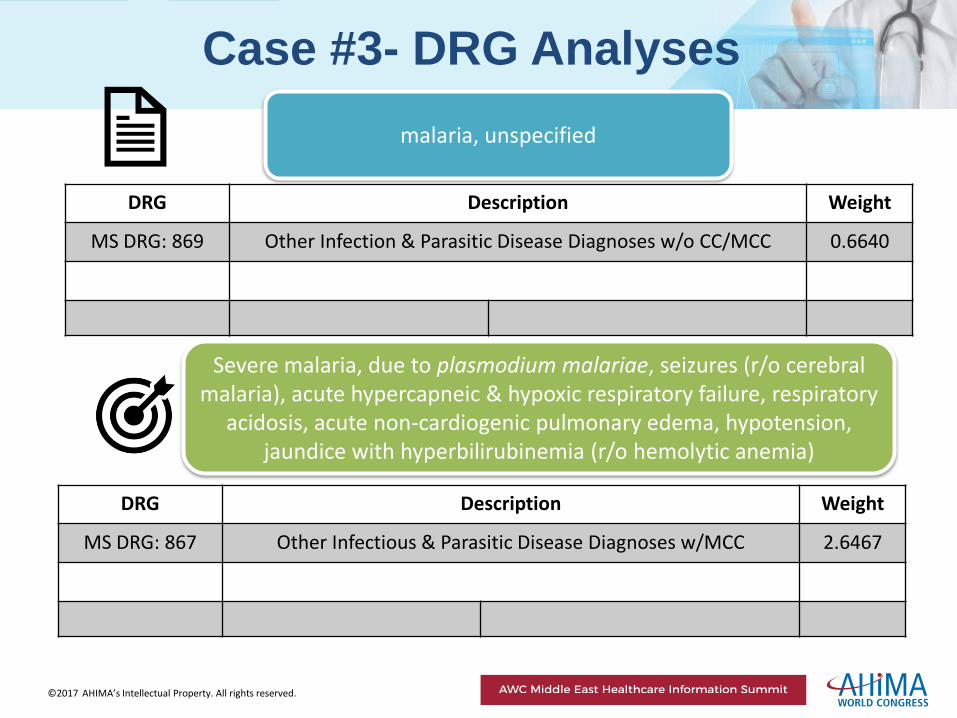
DRG Description Weight
MS DRG: 869 Other Infection & Parasitic Disease Diagnoses w/o CC/MCC 0.6640
Case #3- DRG Analyses
DRG Description Weight
MS DRG: 867 Other Infectious & Parasitic Disease Diagnoses w/MCC 2.6467
malaria, unspecified
Severe malaria, due to plasmodium malariae, seizures (r/o cerebral malaria), acute hypercapneic & hypoxic respiratory failure, respiratory
acidosis, acute non-cardiogenic pulmonary edema, hypotension, jaundice with hyperbilirubinemia (r/o hemolytic anemia)
©2017 AHIMA’s Intellectual Property. All rights reserved.
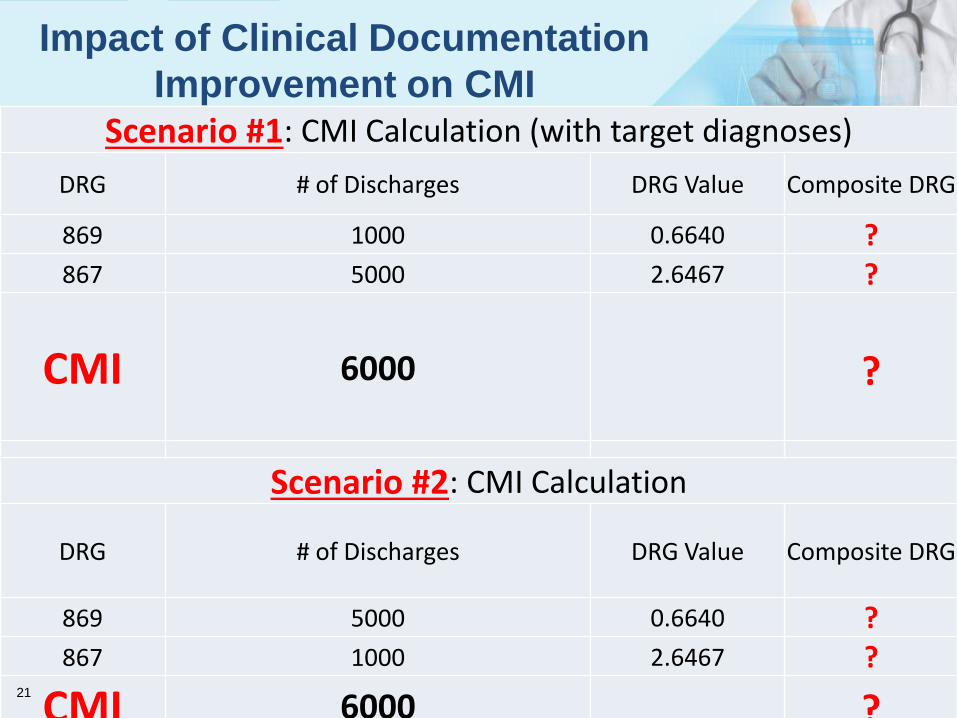
Impact of Clinical Documentation
Improvement on CMI Scenario #1: CMI Calculation (with target diagnoses)
DRG # of Discharges DRG Value Composite DRG
869 1000 0.6640 ? 867 5000 2.6467 ?
CMI 6000
?
Scenario #2: CMI Calculation
DRG # of Discharges DRG Value Composite DRG
869 5000 0.6640 ? 867 1000 2.6467 ?
CMI 6000 ? 21
©2017 AHIMA’s Intellectual Property. All rights reserved.
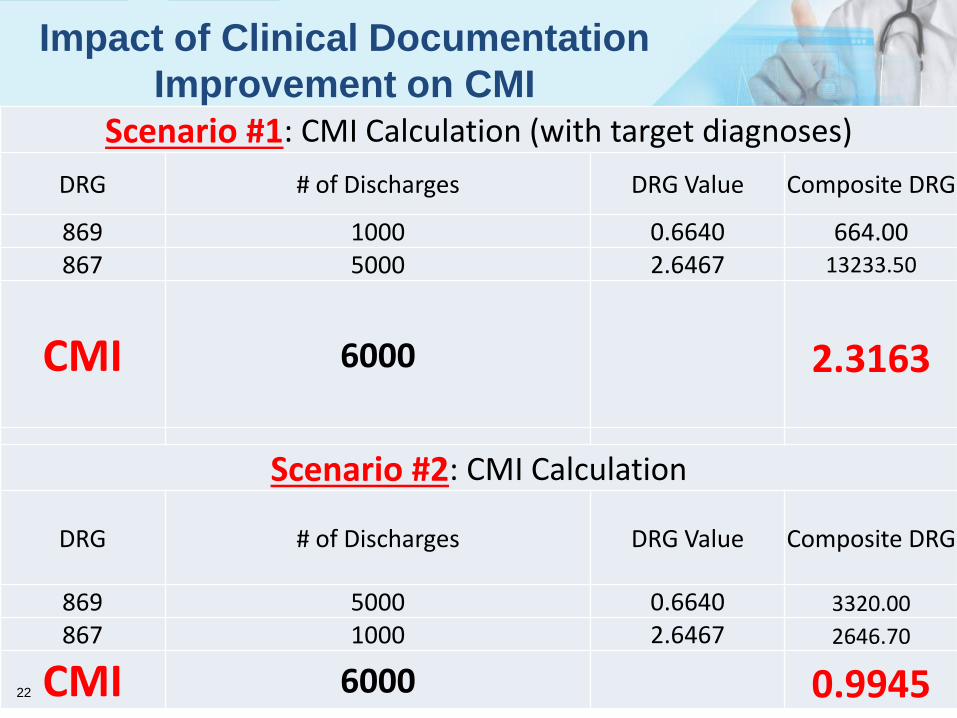
Impact of Clinical Documentation
Improvement on CMI Scenario #1: CMI Calculation (with target diagnoses)
DRG # of Discharges DRG Value Composite DRG
869 1000 0.6640 664.00 867 5000 2.6467 13233.50
CMI 6000
2.3163
Scenario #2: CMI Calculation
DRG # of Discharges DRG Value Composite DRG
869 5000 0.6640 3320.00
867 1000 2.6467 2646.70
CMI 6000 0.9945 22
©2017 AHIMA’s Intellectual Property. All rights reserved.
Summary of Key Points
• CMI with clinical and reimbursement definitions
• Proper calculation of CMI is crucial
• Inappropriate documentation adversely impacts CMI
• Slight shifts in CMI have tremendous financial impact
• Analyses of CMI trends utilized for revenue, patient complexity,
patient care and documentation practices
23
©2017 AHIMA’s Intellectual Property. All rights reserved.
References
• AHA Coding Clinic® for ICD-10-CM/PCS. Chicago: AHA Central Office, 2017.
• Casto, Anne B. ICD-10-CM Code Book, 2017. Chicago: AHIMA Press, 2017.
• Casto, Anne B. ICD-10-PCS Code Book, 2017. Chicago: AHIMA Press, 2017.
• Casto, Anne B. and Forrestal, Elizabeth. Principles of Healthcare
Reimbursement, Fifth Edition. Chicago: AHIMA Press, 2015.
• Hess, Pamela Carroll. Clinical Documentation Improvement- Principles and
Practice. Chicago: AHIMA Press, 2015.
• Kasper, Dennis et al. Harrison'sTM Principles of Internal Medicine, Nineteenth
Edition. Columbus: McGraw-Hill Education, 2015.
• Leon-Chisen, Nelly. ICD-10-CM and ICD-10-PCS Coding Handbook 2017.
Chicago: AHA Central Office, 2017.
• Papadakis, Maxine A. et al. 2017 Current Medical Diagnosis & Treatment- Fifty
Sixth Edition. Columbus: McGraw-Hill Education, 2017.
24

©2017 AHIMA’s Intellectual Property. All rights reserved.
Questions?
©2017 AHIMA’s Intellectual Property. All rights reserved.
Contact Information
Wilbur Lo, MD, CDIP, CCA
AHIMA-Approved ICD-10-CM/PCS Trainer
AHIMA World Congress Faculty
Thank you for participating!

©2017 AHIMA’s Intellectual Property. All rights reserved.
Thank You!