Embed Size (px)
Citation preview
Improving Outcomes for Children with HIV-1
Grace John-Stewart
Goals
• Summarize ongoing pediatric HIV-1 studies and new directions
• Discuss some unique issues children face• Introduce investigators with some specific
focus interests to foster networking
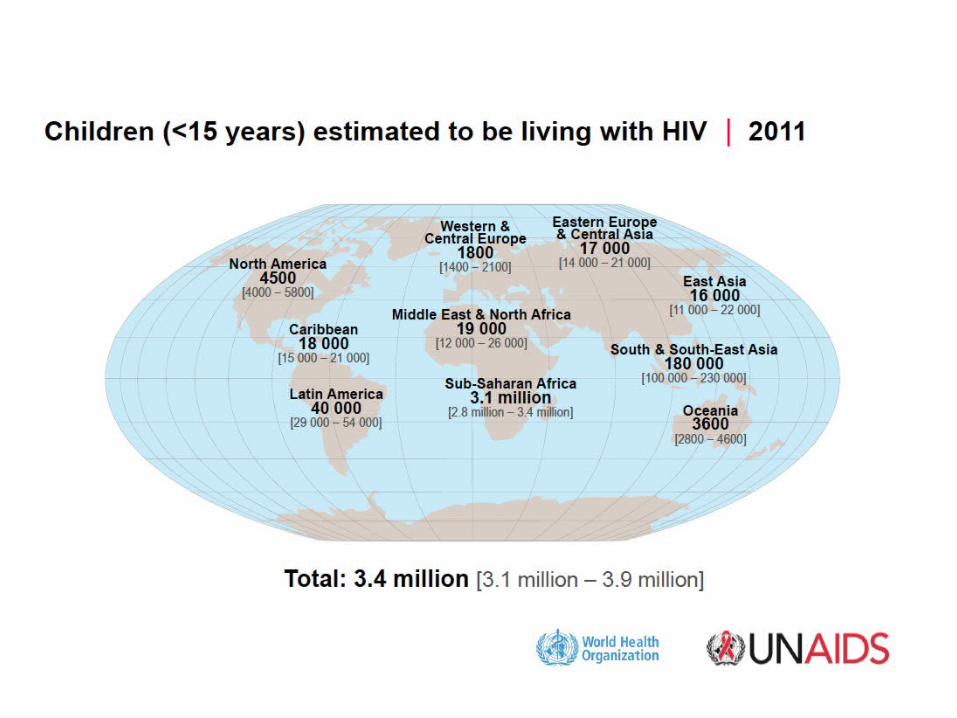
Two Maps

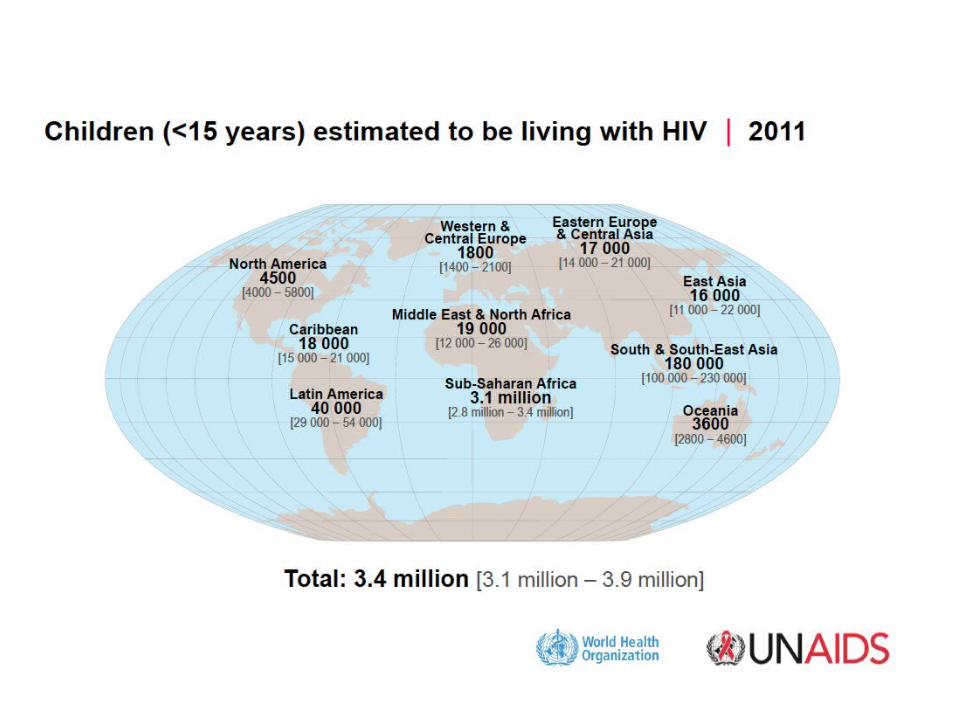

e-MTCT Prevention Momentum
• Global Target 1– Reduce the number of
new infections among children by 90% (<30,000 annually) and MTCT to <5% by 2015
• Global Target 2 – Reduce the number of
AIDS related-maternal deaths by 50%
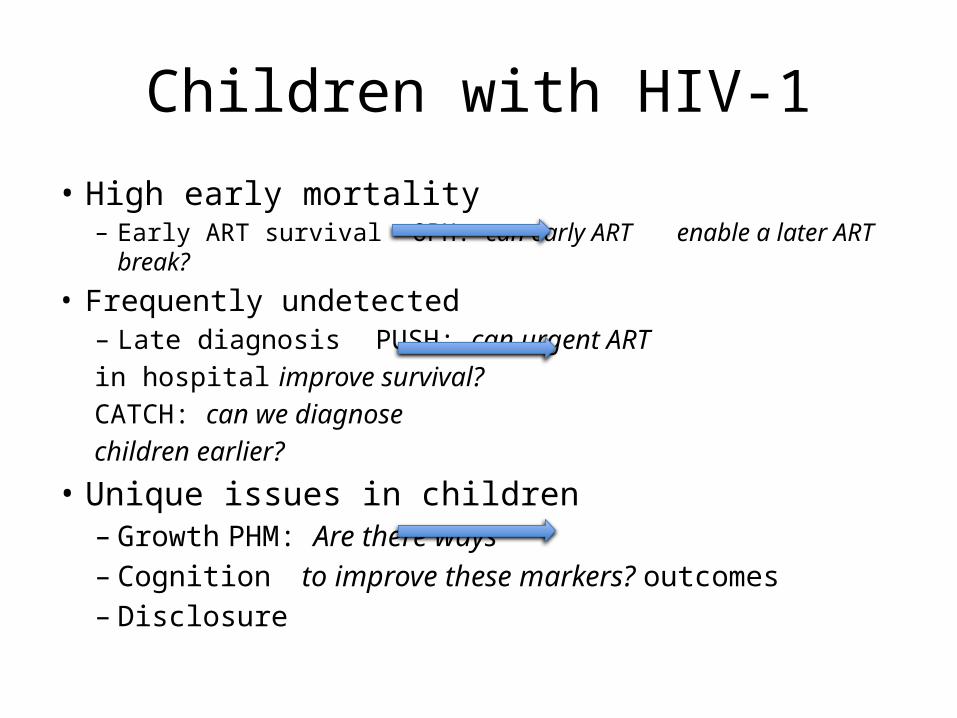
Children with HIV-1
• High early mortality– Early ART survival OPH: can early ART enable a
later ART break?
• Frequently undetected– Late diagnosis PUSH: can urgent ART in hospital improve survival?
CATCH: can we diagnose
children earlier?
• Unique issues in children– Growth PHM: Are there ways – Cognition to improve these markers? outcomes– Disclosure
Optimizing Pediatric HIV-1 Therapy 03
OPH03
Early ART in Infants
• Survival benefit of early ART in infants (CHER)• Early ART may preserve thymic function in infancy • Is this sufficient to allow children to have a
treatment interruption (TI)?
OPH03
1Violari et al. (CHER) 2008
Balancing Issues for Infant ARTOPH03
↑CD4, growth benefit↑ resistance, failure,
toxicityLifelong ART
↑ treatment options↑ VL, immune activation
Interruption after CD4 reconstitution
Potential treatment options for infant ART

Methods
Aim To compare growth and morbidity among infants randomized to continued versus interrupted ART
Design Non-blinded RCTEligibility ART at <13 months, on ART for > 24 months,
normalized growth and CD4 (CD4% ≥ 25%)
Follow-up Monthly- growth, 3-monthly CD4 : 18 monthsEndpoints Growth (Weight for Height), SAEsRestart criteria CD4 <25%*, OI, poor growth
Birth 0-13 months
Continue ART
Interrupt ART
24 months
ART
18 months
Start ART
Randomize
OPH03

Study Flow Diagram
http://pregnancy.amuchbetterway.com/files/2011/12/iStock_000002051524XSmall.jpg
Started ART < 13 months Eligible (n=121)
On ART ≥24 mos (n=75)
Randomized (n=42)
Continued (n=21) Interrupted (n=21)
Withdrawn (n=1)LTFU (n=1)
Withdrawn* (n=1)
18 mos FU (n=19) 18 mos FU (n=20)
*temporarily withdrew from study protocol at 6 months
OPH03
PMTCT programs18000 mother-infant
Newly diagnosed hospitalized infants
HIV treatment ClinicInfants on ART
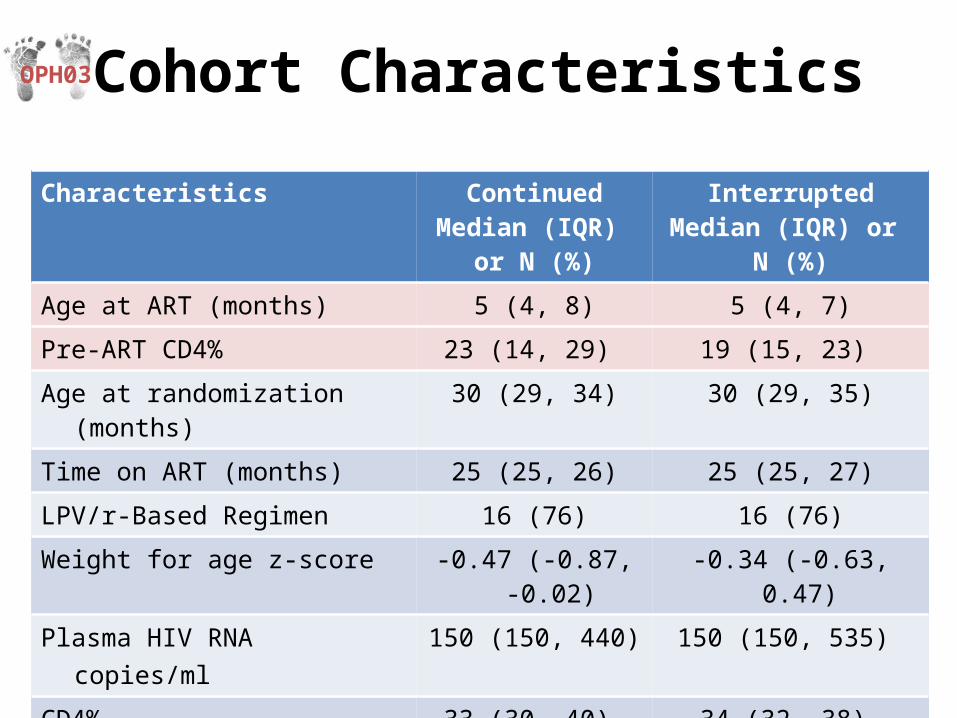
Cohort Characteristics
Characteristics ContinuedMedian (IQR)
or N (%)
InterruptedMedian (IQR) or
N (%)
Age at ART (months) 5 (4, 8) 5 (4, 7)Pre-ART CD4% 23 (14, 29) 19 (15, 23)
Age at randomization (months) 30 (29, 34) 30 (29, 35)Time on ART (months) 25 (25, 26) 25 (25, 27)
LPV/r-Based Regimen 16 (76) 16 (76)
Weight for age z-score -0.47 (-0.87, -0.02) -0.34 (-0.63, 0.47)
Plasma HIV RNA copies/ml 150 (150, 440) 150 (150, 535)
CD4% 33 (30, 40) 34 (32, 38)
CD4 count (cells/μL) 1750 (1547, 2299) 1654 (1300, 1924)
OPH03
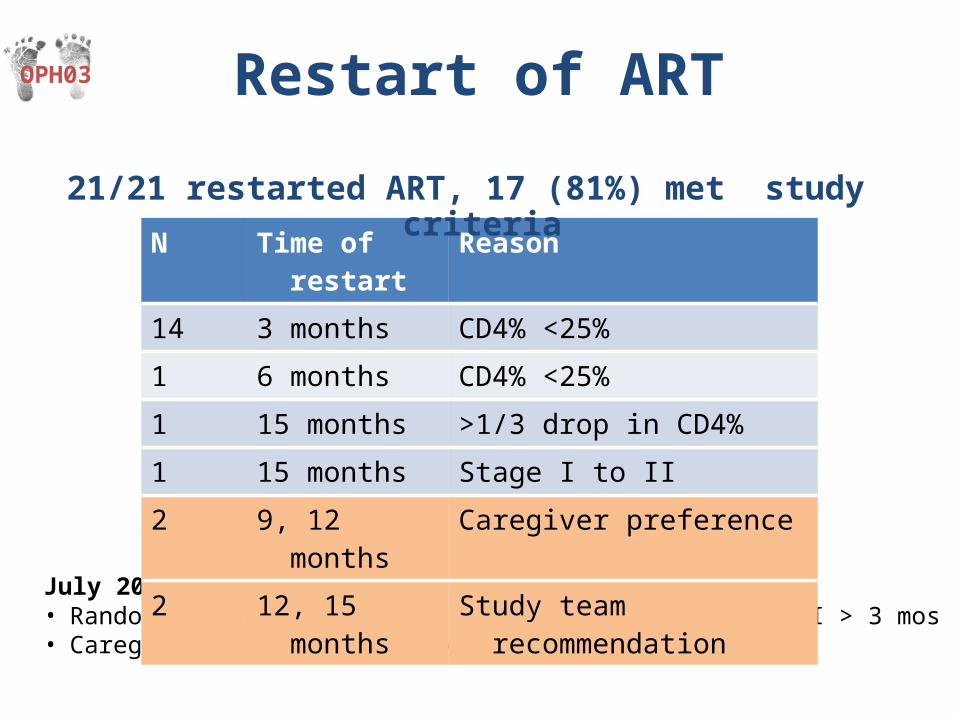
July 2011 DSMB• Randomization discontinued, safe but too few with TI > 3 mos• Caregivers were given option to restart
N Time of restart Reason
14 3 months CD4% <25%
1 6 months CD4% <25%
1 15 months >1/3 drop in CD4%
1 15 months Stage I to II
2 9, 12 months Caregiver preference
2 12, 15 months Study team recommendation
OPH03 Restart of ART
21/21 restarted ART, 17 (81%) met study criteria
-1.5
-1-.
50
.51
1.5
We
ight
for
Heig
ht Z
-sco
re
0 3 6 9 12 15 18Months Post-Randomization
-1.5
-1-.
50
.51
1.5
Heig
ht fo
r A
ge
Z-s
core
0 3 6 9 12 15 18Months Post-Randomization
-1.5
-1-.
50
.51
1.5
We
igh
t fo
r A
ge
Z-s
core
0 3 6 9 12 15 18Months Post-Randomization
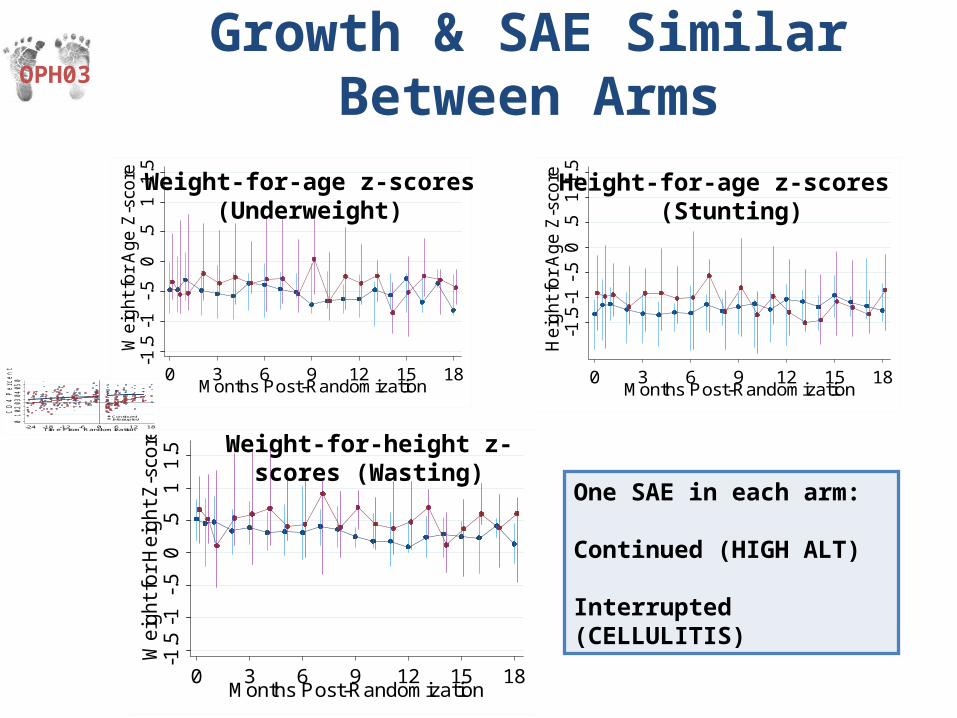
Growth & SAE Similar Between Arms
Weight-for-age z-scores (Underweight)
Height-for-age z-scores (Stunting)
Weight-for-height z-scores (Wasting)
OPH03
ContinuedInterrupted
01
02
03
04
05
0
CD
4 P
erce
nt
-24 -18 -12 -6 0 6 12 18Time From Randomization
One SAE in each arm:
Continued (HIGH ALT)
Interrupted (CELLULITIS)
010
2030
4050
CD
4 P
erce
nt
0 3 6 9 12 15 18Months Post-Randomization
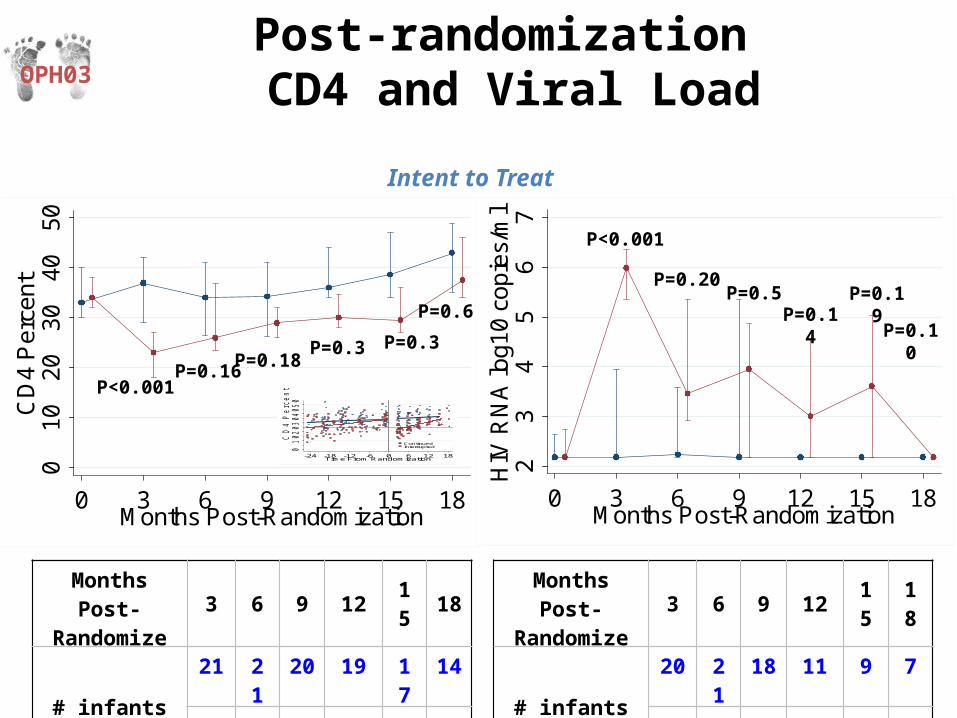
Post-randomization CD4 and Viral LoadOPH03
Intent to Treat
P<0.001P=0.16
P=0.3 P=0.3P=0.18
23
45
67
HIV
RN
A lo
g10
copi
es/m
l0 3 6 9 12 15 18
Months Post-Randomization
P<0.001
P=0.20
P=0.14P=0.19P=0.5
ContinuedInterrupted
01020304050
CD
4 P
ercent
-24 -18 -12 -6 0 6 12 18Time From Randomization
Months Post-
Randomize3 6 9 12 1
518
# infants
21
21
20
19 17
14
21
20
21
21 20
18
Months Post-
Randomize3 6 9 12 1
518
# infants
20
21
18
11 9 7
21
18
17
16 12
9
P=0.6P=0.10
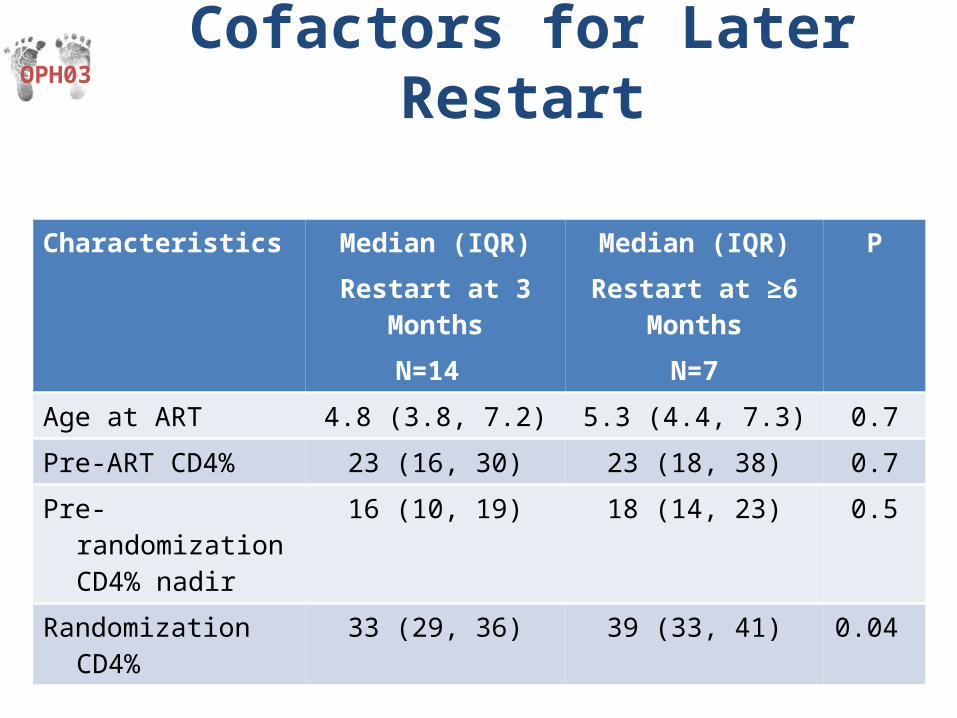
Characteristics Median (IQR)Restart at 3 Months
N=14
Median (IQR)Restart at ≥6 Months
N=7
P
Age at ART 4.8 (3.8, 7.2) 5.3 (4.4, 7.3) 0.7
Pre-ART CD4% 23 (16, 30) 23 (18, 38) 0.7
Pre-randomization CD4% nadir
16 (10, 19) 18 (14, 23) 0.5
Randomization CD4% 33 (29, 36) 39 (33, 41) 0.04
Cofactors for Later Restart
OPH03

Summary
• High proportion of infants with early restart• Growth and SAE incidence similar • Infants with earlier restart had a lower CD4% at
randomization but not pre-ART or nadir
OPH03
Conclusions and Context
• Interruption was not feasible for this population– WHO guidelines CD4 25% vs. 20% in previous
pediatric RCT- PENTA leading to earlier restart– Successful PMTCT with fewer HIV infections
detected in PMTCT programs and higher proportion identified when symptomatic
– Infants detected while asymptomatic or with higher CD4% at TI may be a better group for TI
OPH03
2013• Mississippi baby
– Very early ART followed by unscheduled TI with viral control
• CHER follow-up (Lancet Aug 22, 2013)– 377 infants CD4 >25% asymptomatic <12 wks
• Early then TI at 40 or 96 wks• Restart at CD4 20% • 40W TI 33 wks, 19% remained off ART at end of study • 96W TI 70 wks, 36% remained off ART at end of study
• Visconti trial– ~15% post-treatment controllers (starting within 10 wks acute infection)– Viral control for median 89 months
• New directions– Replicate early detection and rapid ART– Therapeutic vaccines or other strategies in cure agenda

Where are children diagnosed?
• PMTCT programs– <5% transmission risk
• EID– 15%– 6 wks, 9 mos, 18 mos
• Older children infected before PMTCT scale-up– 28% ART in ART-eligible children– Symptomatic presentation

Pediatric Urgent Start of HAART (PUSH)
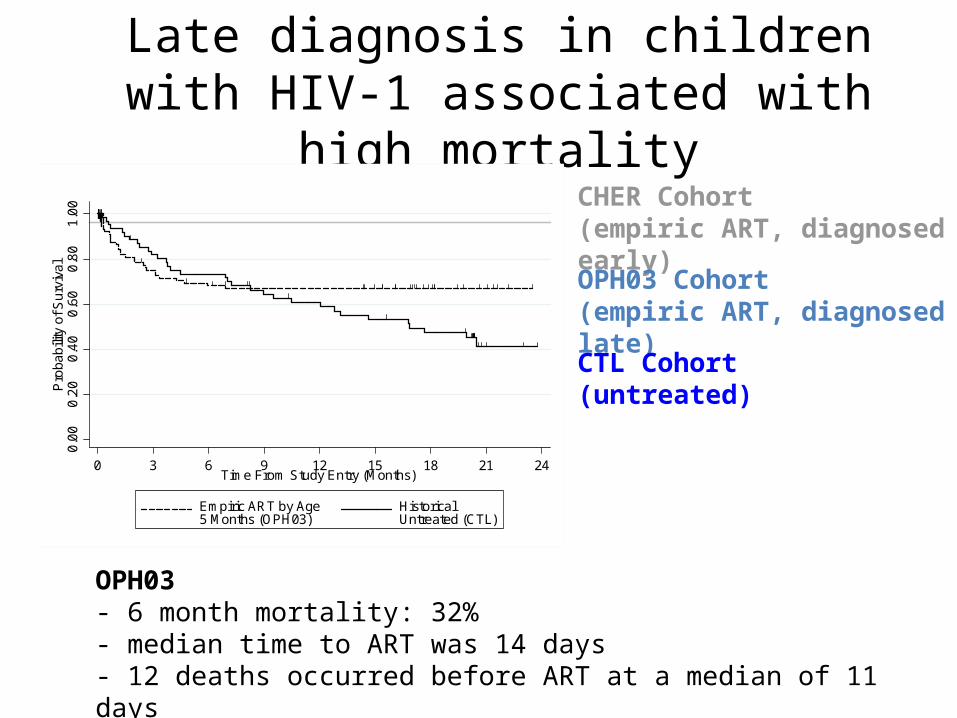
Late diagnosis in children with HIV-1 associated with high mortality
0.0
00
.20
0.4
00
.60
0.8
01
.00
Pro
babi
lity
of S
urv
ival
0 3 6 9 12 15 18 21 24Time From Study Entry (Months)
Empiric ART by Age5 Months (OPH03)
HistoricalUntreated (CTL)
CHER Cohort(empiric ART, diagnosed early)
OPH03 Cohort(empiric ART, diagnosed late)
CTL Cohort (untreated)
OPH03- 6 month mortality: 32% - median time to ART was 14 days- 12 deaths occurred before ART at a median of 11 days

Early ART during OI Useful
• Early/deferred OI (ACTG A1564)– 14 days vs. deferred
Zolopa PLoS ONE 4(5): e5575
HR = 0.53 Early versus Deferred ART [95%CI 0.30–0.92 p = 0.023]
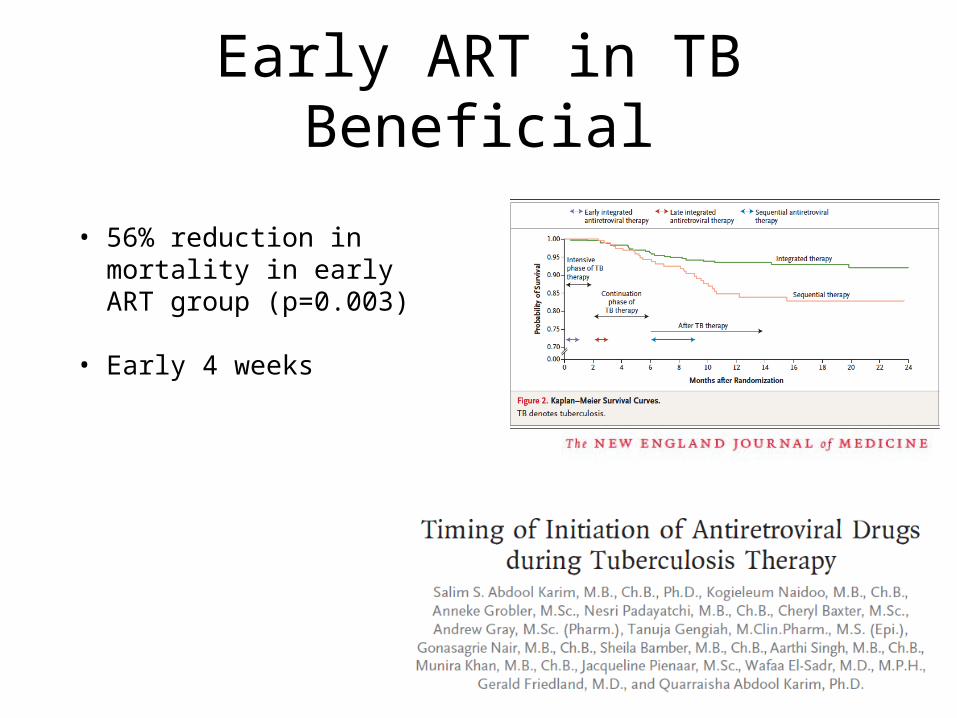
Early ART in TB Beneficial
• 56% reduction in mortality in early ART group (p=0.003)
• Early 4 weeks
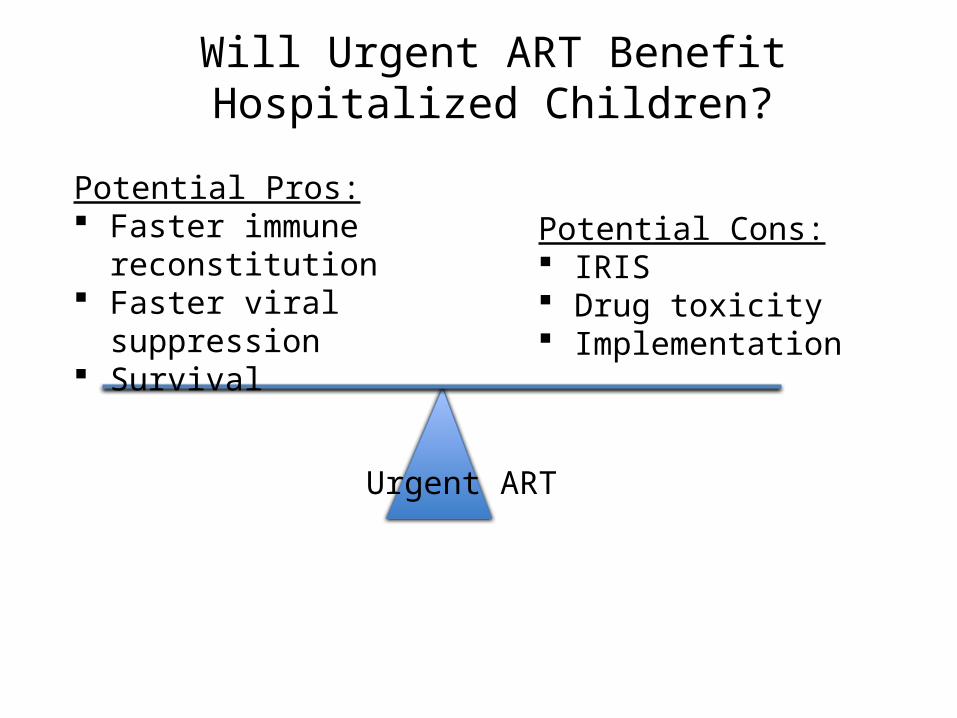
Will Urgent ART Benefit Hospitalized Children?
Potential Pros: Faster immune
reconstitution Faster viral suppression Survival
Potential Cons: IRIS Drug toxicity Implementation
Urgent ART
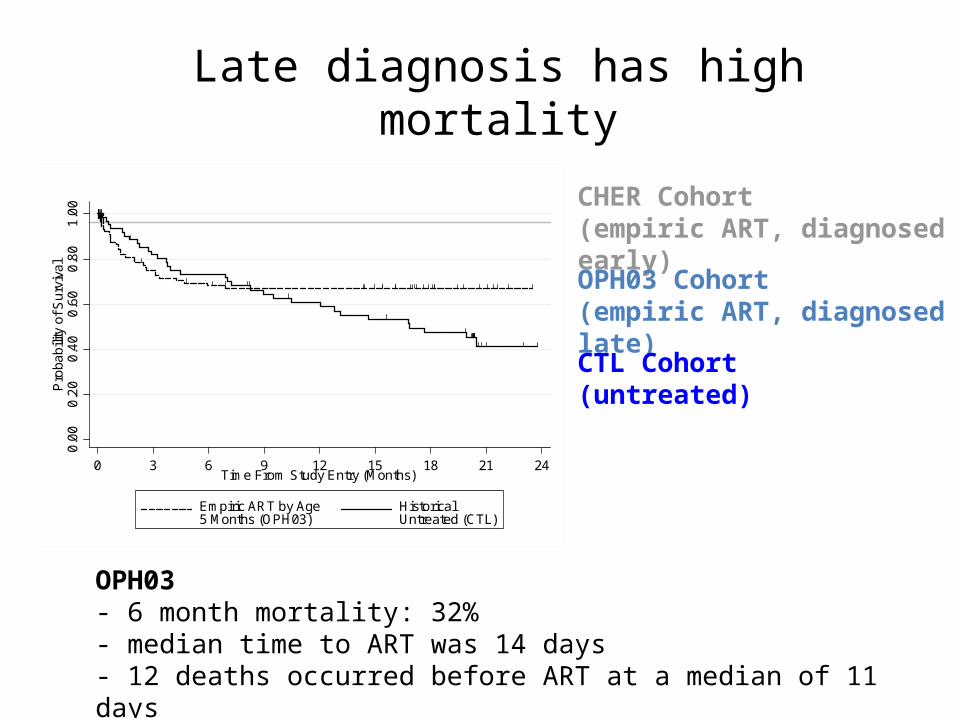
Late diagnosis has high mortality0
.00
0.2
00
.40
0.6
00
.80
1.0
0P
roba
bilit
y of
Su
rviv
al
0 3 6 9 12 15 18 21 24Time From Study Entry (Months)
Empiric ART by Age5 Months (OPH03)
HistoricalUntreated (CTL)
CHER Cohort(empiric ART, diagnosed early)
OPH03 Cohort(empiric ART, diagnosed late)
CTL Cohort (untreated)
OPH03- 6 month mortality: 32% - median time to ART was 14 days- 12 deaths occurred before ART at a median of 11 days
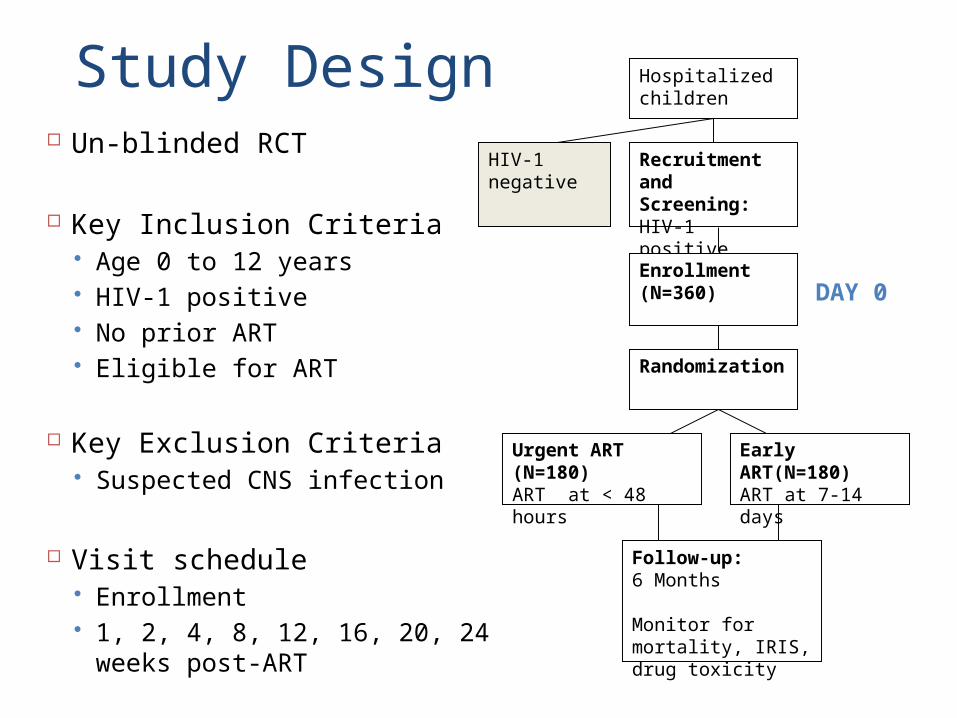
Hospitalized children
Recruitment and Screening:HIV-1 positive
Enrollment (N=360)
Randomization
Early ART(N=180)ART at 7-14 days
HIV-1 negative
Urgent ART (N=180)ART at < 48 hours
Follow-up: 6 Months
Monitor for mortality, IRIS, drug toxicity
DAY 0
Study Design Un-blinded RCT
Key Inclusion Criteria Age 0 to 12 years HIV-1 positive No prior ART Eligible for ART
Key Exclusion Criteria Suspected CNS infection
Visit schedule Enrollment 1, 2, 4, 8, 12, 16, 20, 24 weeks post-
ART
Study Sites
Kenyatta National Hospital (KNH)
Jaramogi Oginga Odinga Teaching & Referral Hospital (JOOTRH) [Kisumu Provincial General Hospital]
Kisumu East District Hospital (KEDH)
http://www.destination360.com/africa/kenya/map
Issues in the study
• Quick turnaround for diagnosis• Family diagnosis and disclosure• Costs of HIV diagnosis in hospital• Belief in ART/HIV efficacy
Early Detection of HIV: CATCHAnjuli Wagner, Jenn Slyker, Irene Njuguna
• Adults with HIV: test children– Clinic– Home
• Ethical issues

Disclosure of HIV diagnosisGrace Wariua, Kristin Beima-Sofie, Maureen Kelley
• Practitioners– Time to disclose– Revealing process– Risks of current messages
• Children• Caregivers
Growth and cognitionChristine McGrath, Sarah Benki-Nugent, Claudia Crowell, Dalton Wamalwa
• Early ART improves growth
• Role of nutritional supplementation
• PI-ART faster milestones
Improving Outcomes for Children with HIV-1
• Early ART• Preserve regimens• Improve survival for those
diagnosed late• Find undiagnosed• Comprehensive approach
– Social, growth, cognitive, disclosure, co-infection issues