Embed Size (px)
Citation preview

Improving Harm Across the BoardKathleen M. Louth
Director of Quality ManagementMonroe County Hospital
P. O. Box 1068Forsyth, GA 31029
478.994.2521 ext. [email protected]
Hospital Trend Rate in Reducing Harm
2
*HAC harm = inpatient hospital acquired conditions
0%
5%
10%
15%
20%
25%
30%
Q1 11 Q2 11 Q3 11 Q4 11 Q1 12 Q2 12 Q3 12 Q4 12 Q1 13
Harm
s/1
,000 d
isch
arg
es

Number of Harms
3
0
1
2
3
4
5
6
7
8
9
10
Q1 11 Q2 11 Q3 11 Q4 11 Q1 12 Q2 12 Q3 12 Q4 12 Q1 13
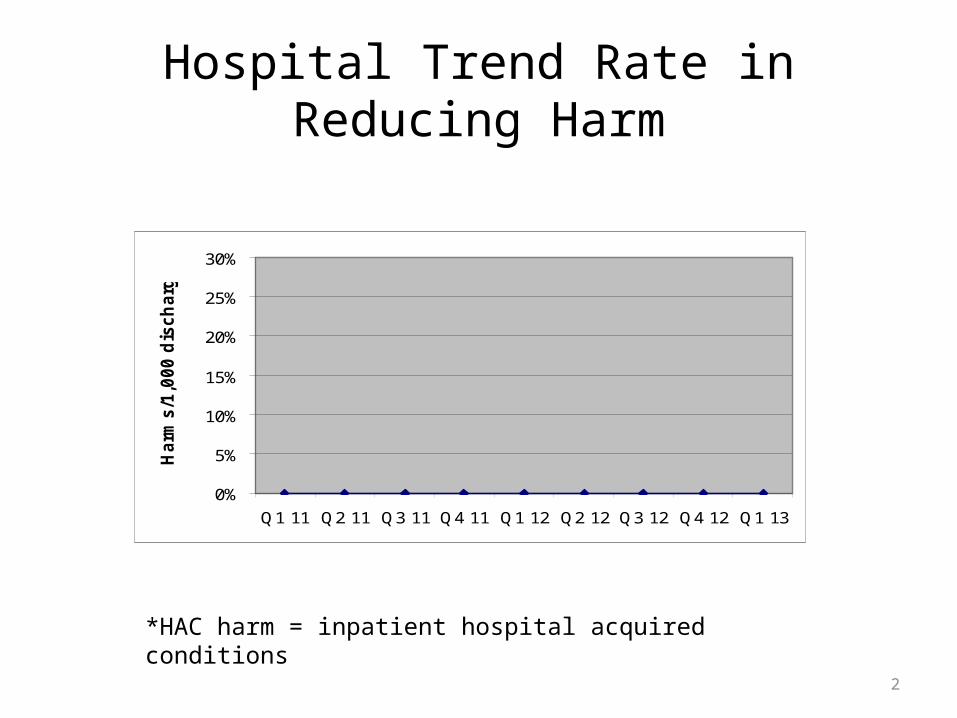
30 Day Total Readmission Rate All Cause
4
*all cause 30 day readmissions
16.36%
11.11%13.16%
27.91%
21.28%
9.09%
18.00%
9.52%
12.96%
0%
5%
10%
15%
20%
25%
30%
Q1 11 Q2 11 Q3 11 Q4 11 Q1 12 Q2 12 Q3 12 Q4 12 Q1 13

Number of Readmissions All Cause
5
9
65
12
10
4
9
4
7
0
2
4
6
8
10
12
14
Q1 11 Q2 11 Q3 11 Q4 11 Q1 12 Q2 12 Q3 12 Q4 12 Q1 13

PearlsMultidisciplinary•It is not just the work of the Quality Improvement Department; all departments must be involved• Must be a collaborative effort from the top-down and bottom-up• Increased communication and input from management staff
Assign ownership and expectations• Establish timelines for project deliverables•Continue to meet with definite reporting timeframes
Educate•Keep the staff, medical staff, and board informed

Defining Moments In Our JourneyDefining Moments & Commitment to Patient Safety:• 2009-New CEO who had experience in Quality & Patient Safety; new Director of Quality Management hired
• 2010- Patient Safety Plan & Commitment to Patient Safety developed; revised incident reporting system & tools; fall team formed; medication error team formed; Quality Council & reporting revised; education of changes to all (hospital wide); Culture of Patient Safety Survey implemented; Patient Safety Week recognized
•2011-Fall prevention program revised; education of changes to all (hospital wide); Glycemic Control team formed; CLABSI team formed
7

Defining Moments In Our Journey• 2012- Participation in the Hospital Engagement Network (HEN) &
education to management team; Regrouped on readmissions due to data issues; formation of Readmission Reduction team; OATS team formed; HCAHPS training; CAUTI team formed; Marketing of Patient Safety through website, banners, boards, & local newspaper
• 2013-Strategies to reduce readmissions implemented-bedside shift reporting, white boards, rounding (hourly, nurse manager, leadership), discharge follow up calls, follow up appointments made, discharge folder, pharmacist educating high risk patients, follow up calls for ER patients, working with hospice and home heath agencies, participating in GMCF Care Transitions, participating in MATCH, Patient & Family Engagement; Case Manager position job duties aligned with reducing readmission efforts to include discharge process

Breakthrough Strategy• Major Challenges Encountered
– Limited Resources (human, time, financial)– Implementation of EHR– Culture change – Training
• Strategies to Overcome– Time management, utilizing resources from the HEN– Constant education and re- education, dedicated point person for EHR– Reinforcement of rationales, hearing stories from peers at other facilities– Make it fun, pertinent, convenient, personal, and using personalized teaching
methods
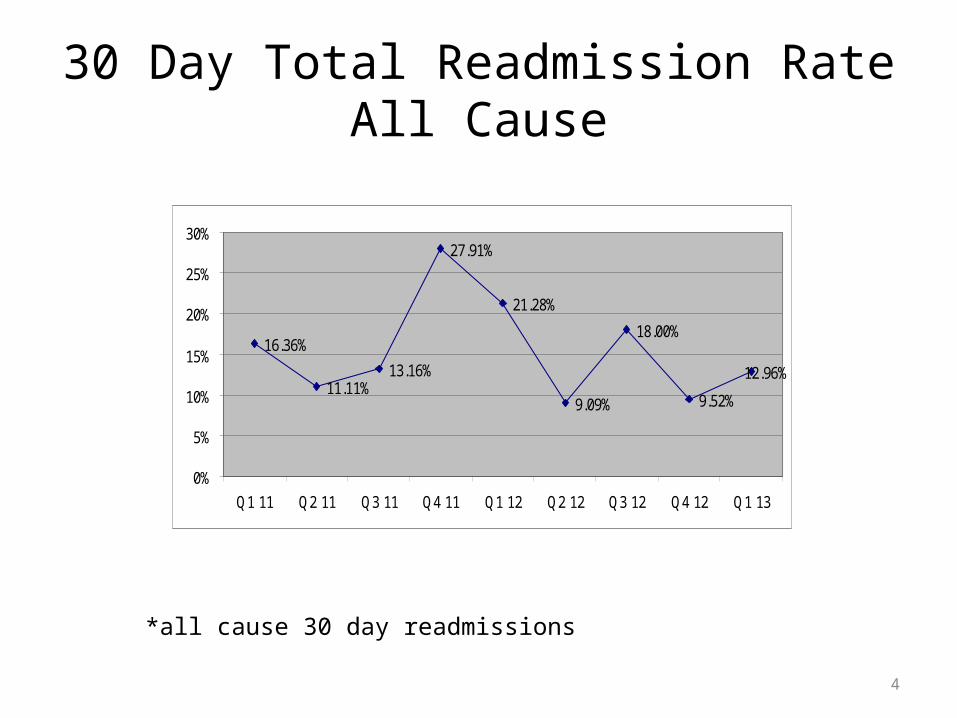
Slide 10HACs Estimated annual number of patients at risk in each area Number of Opportunities
ADE # of discharges: 378
CAUTI # pts in IP units with catheter in place: 127
CLABSI # pts in IP units with central lines: 0
Falls # of discharges: 378
Ob AE # of women with deliveries: 0
Pr Ulcer # of discharges: 378
SSI # of inpatient surgeries: 15
VAP # of patients on a ventilator: 0
VTE # of discharges: 378
EED # of women with elective deliveries 0
TOTAL Risk opportunities for harm across the board 1654
Readmit # of inpatients at risk of readmit: 378
Annual discharges: 378 year 2010 HAC risk opportunities/discharge: 4.37
Risk Profile: The Areas of Risk We Are Committed To Controlling
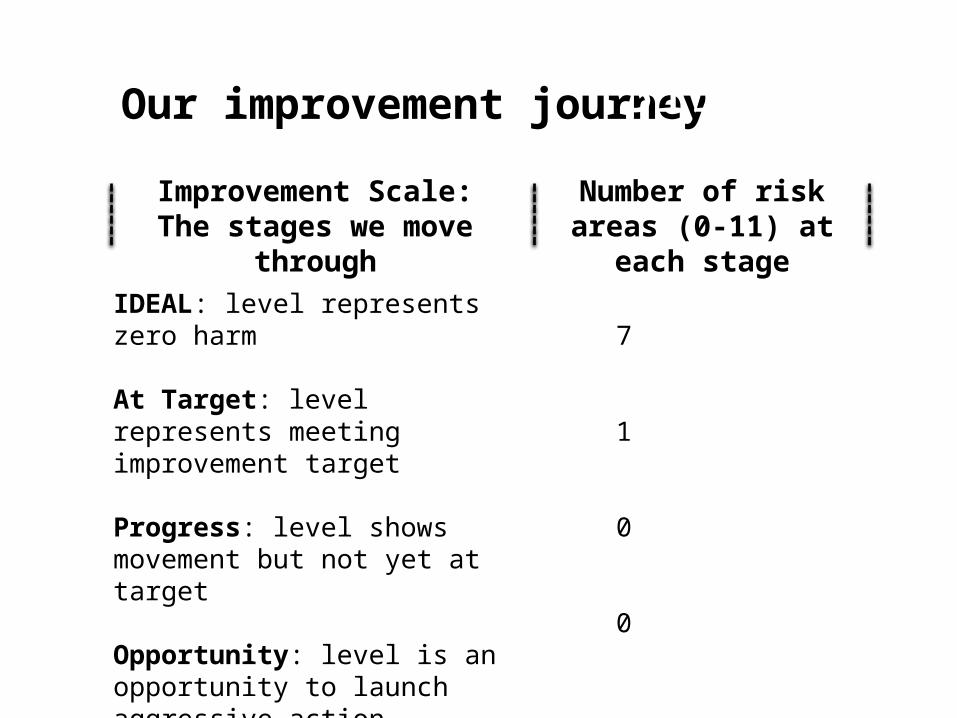
Our improvement journey
IDEAL: level represents zero harm
At Target: level represents meeting improvement target
Progress: level shows movement but not yet at target
Opportunity: level is an opportunity to launch aggressive action
7
1
0
0
Number of risk areas (0-11) at each stage
Improvement Scale:The stages we move through
Slide 11

Improving Harm Rates (per discharge)
HACs Baseline Rate[2010]
Target Rate
ADE 0% 0%
CAUTI 0% 0%
CLABSI 0% 0%
Falls 0% 0%
Ob AE 0% 0%
Pr Ulcer 0% 0%
SSI 0% 0%
VAP 0% 0%
VTE 0% 0%
EED 0% 0%
Total 0% 0%
Readmit 15.15% 15.24%
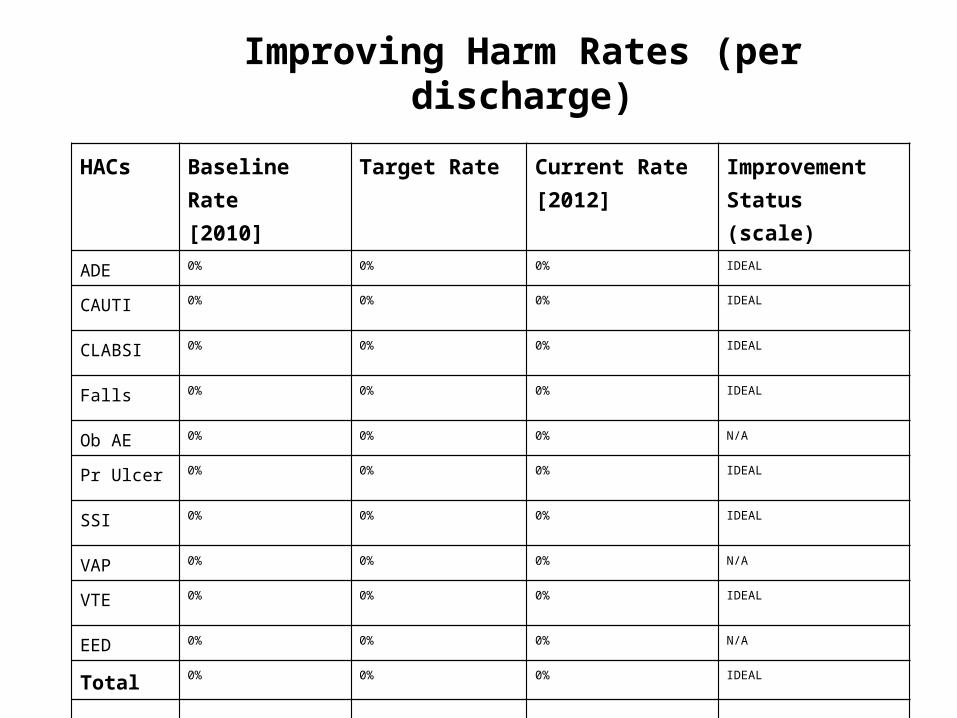
Improving Harm Rates (per discharge)
HACs Baseline Rate[2010]
Target Rate Current Rate[2012]
Improvement Status (scale)
ADE 0% 0% 0% IDEAL
CAUTI 0% 0% 0% IDEAL
CLABSI 0% 0% 0% IDEAL
Falls 0% 0% 0% IDEAL
Ob AE 0% 0% 0% N/A
Pr Ulcer 0% 0% 0% IDEAL
SSI 0% 0% 0% IDEAL
VAP 0% 0% 0% N/A
VTE 0% 0% 0% IDEAL
EED 0% 0% 0% N/A
Total 0% 0% 0% IDEAL
Readmit 15.15% 15.24% 14.47% Target

Our Hospital Risk Score CardOur Safety Mandate
Annual Volume (Discharges) 378
Total risk: annual harm opportunities 1654Risks per patients (Total Opportunities)/Discharges) 4.37
Number of Risk AreasNumber of PfP Risk Areas Applicable (0 – 11) 8Number of PfP Risk Areas Applicable & Adopted 8
Our ProgressNumber of PfP Areas with Major Improvement Opportunity 0Number of PfP Areas at Improvement Target 1Number of PfP Areas at IDEAL 7
Pictured 1st row left to right:Shawnelle Lupton, Operating Room Nurse Manager; Dr. Dana Peterman, PT, DPT; Casey Fleckenstein, Medical/Surgical Nurse Manager
Pictured 2nd row left to right:Dr. Craig Caldwell, Past President of the Medical Staff/Hospital Authority Board Member; Sherry Mays, Clinical Coordinator; Kathleen Louth, Director of Quality Management; and Tim Allen, Director of Engineering and Environmental Services.
Not pictured:Kay Floyd, CEO; Tony Ussery, Chairman of the Quality Council/Vice Chairman of the Hospital Authority Board; Megan Randall, Director of Radiology; Pam Lankford, Emergency Room Nurse Manager; Hugh Cromer, Director of Pharmacy; Laura Roush, Director of Laboratory; Jean Riley, Director of Respiratory Therapy/Infection Control; Cindy Renno, Dietary Manager; Ticia Hicks, Case Management; Michelle Wiggins, Swing Bed Coordinator; and Mamie Patterson, Diabetes Support Group.

Next big step to Reduce Harm
• Continue our efforts that we already started
• Enhance patient & family engagement
• Implement teach back