Embed Size (px)
Citation preview
International Journal of Mental Health Nursing (2003) 12, 11–21
INTRODUCTION
Until recently, studies focused on how the fastest-growingsegment of our population, the elderly, would challengethe health-care system to provide them with good-qualitygeriatric nursing care in the future. However, some studiesclearly show that the health-care system already faces dif-ficulties in doing this (Nolan & Tolson 2000; Ordre des
Infirmières et Infirmiers du Québec 2000). Harringtonand colleagues (2000) demonstrated the impact of good-and poor-quality nursing care on the elderly in nursinghomes, citing many significant elements of care: urinarycatheter use, urinary tract infection, frequency of skin care,antibiotic use, hydration, nutritional intake, oral health,physical abuse, morbidity and even mortality. However,these authors did not study the quality of nursing careprovided to the elderly afflicted with mental healthproblems living in the community. They proposed that itwould be beneficial for the quality of care to set standardsfor the level of education among nurses caring for theelderly. At the same time, authorities in Canada, the USAand the United Kingdom have encouraged the improve-ment of training for health professionals involved in
FEATURE ARTICLE
Improving geriatric mental health nursing care:Making a case for going beyond psychotropicmedications
Correspondence: Philippe Voyer, Faculty of Nursing, LavalUniversity, Pavillon Paul-Comtois, Cité Universitaire, QuébecG1K 7P4, Canada. Email: [email protected]
Philippe Voyer, RN, PhD.Lori Schindel Martin, RN, MS (Nursing), PhD (c).Accepted December 2002.
Philippe Voyer1 and Lori Schindel Martin2,3
1Faculty of Nursing, Laval University, Pavillon Paul-Comtois, Cité Universitaire, Québec and 2Ruth Sherman Centrefor Research and Education, Shalom Village Nursing Home and 3McMaster University School of Nursing, Hamilton,Ontario, Canada
ABSTRACT: Providing high-quality mental health nursing care should be an important and contin-uous preoccupation in the gerontological nursing field. As the proportion of elderly people in our societyis growing, the emphasis on high-quality care will receive increasing attention from administrators,politicians, organized groups, researchers and clinical nurses. Recent findings illustrate unequivocallythe important contribution of nurses to achieving the goal of high-quality geriatric care. However, thequality of care for the elderly with psychological difficulties has not been addressed. The objective ofthis article is to illustrate that while nurses can accomplish much to improve the well-being and mentalhealth of the elderly, their skills are often underutilized. Psychotropic drugs are often the first-line inter-ventions used by health-care professionals to treat mental health concerns of elderly persons. Alternativetherapies that could be implemented and evaluated, such as psychological counselling, supportive coun-selling, education and life review, are infrequently used. Nevertheless, current scientific data suggestthat it would be very advantageous if nurses were to play a dominant role in the care of elderly peoplewho are depressed or experiencing sleep pattern disturbances. The same can be said about elderlychronic users of benzodiazepines, as well as those with cognitive impairment. Evidence for the use ofpsychotropic medications as a viable treatment option for the elderly both in the community and in thelong-term care setting who are experiencing mental health challenges is examined. Alternative non-pharmacological approaches that nurses can use to augment care are also briefly discussed.
KEY WORDS: assessment tools, depression, disruptive behaviours, insomnia, psychotropic drugs,supportive therapies, withdrawal.

geriatric care (Birrer et al. 1999; Kizer et al. 1998; MSSS1994; Poncia et al. 2000).
The purpose of the present article is to demonstrate thatcommunity-dwelling elders and those living in long-termcare facilities who have psychological difficulties, such asdepression and insomnia, do not appear to receive optimalnursing care. It seems that a major preoccupation of nurses is to monitor the clinical impact of the initiation ofpsychotropic medication, often sacrificing the implemen-tation of adjunct therapies, despite the fact that studies(e.g. Morin et al. 1999; Teri et al. 1999) have clearly demon-strated their effectiveness. In the paragraphs that follow, aglobal overview of psychotropic drug use in the care ofelderly with mental health problems is presented. A reviewof various studies concerning the elderly suffering fromdepression, insomnia and dependence on benzodiazepinesfollows. In addition, a critique of the care of the elderlysuffering from a cognitive impairment (e.g. Alzheimerdisease) is presented.
The treatment of depression, insomnia and disruptivebehaviours is examined, and specific assessment and man-agement strategies that can be implemented by nurses arerecommended. Finally, it is suggested that the dependenceof the elderly on benzodiazepines is an untreated problem.Consequently, a withdrawal programme is proposed. It isnoteworthy that all assessment tools, as well as the non-pharmacological interventions discussed here, are withinthe boundaries of the nursing discipline, and are presentedin several geriatric-nursing monographs. The reader whowants further details will find them in the followingreferences (Abraham et al. 1999; Burke & Walsh 1997;Lauzon & Adam 1996; Miller 1999; Stone et al. 1999).
Our position, based on clinical and research experi-ences, is that nurses can play an important role during theclinical assessment, particularly psychological evaluation,of elderly clients with mental health concerns. Nurses havethe skills to recognize when an elderly client may be usingpsychotropic drugs inappropriately. They have the abilityto identify a questionable consumption of psychotropicdrugs and to discuss alternative management strategieswith the care team. Finally, nurses can ultimately be inno-vative by choosing state-of-the-art interventions in the fieldof mental health care.
Psychotropic drug use: An overviewThe psychotropic drugs referred to in this article are anx-iolytics and hypnotics (e.g. benzodiazepines), antidepres-sants and neuroleptics (antipsychotics). Psychotropicdrugs are usually given to elderly people living in thecommunity to help them cope with anxiety, depression,psychological distress and/or insomnia. Also, neuroleptics(antipsychotics) are provided to reduce the prevalence ofdisruptive behaviours in cognitively impaired elders.
Except for disruptive behaviour in cognitively impairedelders, elderly people living in the community are less oftenafflicted with such problems than middle-aged people.Indeed, researchers have demonstrated that major depres-sion (Blazer et al. 1987; Blazer 1990; Jorm 2000), anxiety(Folks & Fuller 1997; Jorm 2000), psychological distress(Papillon et al. 2000) and insomnia (Ohayon, & Caulet1995) are less frequent among the elderly. In spite of this,elderly people living in the community constitute theportion of the population among whom the use of psycho-tropic drugs is most prevalent. Elderly people are seven to18 times more likely to use psychotropic drugs thanmiddle-aged adults (Laurier et al. 1992; Ohayon et al. 1998;Ried et al. 1990).
The data available regarding the elderly suffering fromdepression show that, on average, only one depressedelderly person out of 10 receives a prescription for an anti-depressant (Kelman & Mayer-Oakes 1994; [n = 205];Taylor et al. 1998, [n = 483]). The work of Keks andBurrows (1995) confirms these results and highlights thatonly 30% of depressed elderly are treated. Other studiesdemonstrated also that only 20–29% of depressed men and30–53% of depressive elderly women consume psycho-tropic drugs (Dealberto et al. 1997; Paterniti et al. 1999).It appears, therefore, that depending on the mental healthproblems, there is overuse (insomnia) and underuse(depression) of psychotropic drugs.
Why is there such a discrepancy in this age groupbetween the use of psychotropic drugs and the prevalenceof psychological problems that psychotropic drugs are usedto treat? Part of the reason is that while the elderly unde-niably experience fewer major psychological problemsthan middle-aged adults, in contrast, manifestations ofpsychological distress are more common among theelderly. The elderly are confronted with problems natu-rally arising from the ageing process (e.g. sleepingproblems) as well as problems arising from changes to theirenvironment (e.g. death of a spouse and friends, moving,institutionalization). Elderly people experience losses thatresult in sadness, anxiety, depressed moods, insomnia, lossof appetite and other symptoms, but these symptoms couldarise from a temporary crisis, not a major depression.Nurses are in a position to report the psychologicalsymptoms of their patients to physicians, therebybecoming gatekeepers for the initiation of psychotropicmedications. The influence of the nurse over the doctorprescription pattern should not be minimized (Simonson1984; Stevenson et al. 1989). Such a request may result inthe prescription of psychotropic drugs when, in fact, nursescould have provided supportive care, such as counsellingthat would have relieved distress in elderly people, therebyavoiding the unnecessary use of drugs.
It is clear that health-care professionals have difficulty
12 P. VOYER AND L. SCHINDEL MARTIN

recognizing psychological problems afflicting the elderly(Chalifoux et al. 1996). It has been shown that 58% ofelderly people living in public housing who needed mentalhealth services did not have their needs met (Smith Blacket al. 1997). Chalifoux et al. (1996) reported that only 6%of elderly people needing such treatment received out-patient mental health services. It is therefore apparent thatamong the elderly there is a discrepancy between theprevalence of mental health problems, the use of psycho-tropic drugs and the availability of mental health services.Part of the present paper offers some reflections for nurseswho are confronted with elderly people presenting differ-ent psychological health problems in different settings.
Depression afflicting elderly people living in thecommunity, psychotropic drugs use and nursingcareDiagnosing depression in the elderly is a complex chal-lenge. The criteria for the diagnosis of depression are asfollows: depressed mood, decline in interest and pleasure,loss or gain in weight, sleeplessness, insomnia or hyper-somnia, slow down of psychomotor responses or excite-ment, exhaustion, fatigue and loss of energy, sense of guilt,lowered self-esteem, loss of attention capacity and suicidalthoughts. At least five of these symptoms must be presentcontinuously for at least 2 weeks to support the diagnosisof the depression (DSM-IV 1994). Unfortunately, as manyas 85% of depressed elderly are not recognized as such(Bair 2000). One explanation for this poor result lies in thefact that many signs of depression are identical tosymptoms present in different diseases or secondary side-effects to medication consumption or to stressful events.
Some symptoms, such as loss of weight and energy,could follow from a recent acute disease, such as pneu-monia or angina, medical conditions that are commonamong the elderly. In this context, these symptoms andothers might be overlooked and, by default, linked to pneu-monia, while the elderly person is actually suffering froma major depression. On the other hand, these symptomsmay be incorrectly attributed to depression. Sleepproblems and difficulty concentrating could be the conse-quence of the normal ageing process or of medicationinteractions (e.g. benzodiazepine, barbiturates, anti-hypertensives) as well as arising from depression (Berg &Dellasega, 1996; Cassel et al. 1997; Van Gerven et al. 2000).A stressful event, such as a child moving, could tempor-arily lower the self-esteem of an elderly person. It is evidentthat a thorough evaluation needs to be conducted in orderto identify the origin of the symptoms. Nurses are in aposition to conduct comprehensive assessments in orderto distinguish between temporary psychological states, forwhich supportive counselling is indicated, and moreserious conditions. Consequently, it would be beneficial
for nurses to administer the Geriatric Depression Scale tohelp judge the mental state of the elderly (This scale is pre-sented in Hayes & Kan 2000.) The scale is simple to admin-ister and offers the nurse excellent support. However, theclinical judgement of the nurse remains the best means toidentify those elderly persons who suffer from depression,and the resources to which they should be directed.
The consequence of the complexity of recognizingdepression in the elderly is reflected in the pattern ofpsychotropic drug use. Forty-two percent to 75% of elderlypatients prescribed psychotropic drugs do not demonstratespecific psychological problems (Aparasu et al. 1998;Tamblyn, 1996). In contrast, only 10% to 15% of elderlypeople exhibiting depression use antidepressant medi-cation (Kelman & Mayer-Oakes 1994; Taylor et al. 1998).So, it seems that there are too many elderly people withoutsignificant mental health problems who receive psycho-tropic drugs and there is an underprescription of anti-depressants.
Nurses can do something about this situation. First, theyshould be well aware of the difficulties involved in identi-fying depression in the elderly. Thus, either they couldavoid the tendency to turn too fast to psychotropic drugswhen the elderly do not exhibit all the clinical character-istics of a depression, or they could avoid the possibility ofnot recognizing a depression and deprive the elderly of thebenefit they would have received from appropriate treat-ment. The data of Wancata et al. (1997) indirectly supportour point, as 50% of the elderly living in the communityreceived a prescription for psychotropic drugs within2 weeks of their admittance to nursing homes. This meansthat during this transitional period, when it is normal for aperson to exhibit adjustment difficulties, the use of psycho-tropic drugs was chosen to help elderly people cope withtheir new situation. There is no evidence to support thatinitiation of psychotropic drugs is essential to facilitateadjustment to institutionalization. Second, nurses shoulduse a standardized, accepted scale to detect depression inelderly people. This could improve the ratio between thepresence of depression and the use of antidepressants.Finally, nurses should engage in a therapeutic nurse–patient relationship with elderly people they suspect maybe suffering from depression. Such psychotherapeutictreatment is known to be efficient (Bair 2000). Moreover,fewer elderly relapse into depression following such treat-ment in comparison to middle-aged adults (Bair 2000).Previously cited studies suggest that nurses do not alwaysengage in a therapeutic nurse–patient relationship withelderly people exhibiting mental health problems. Nursesshould therefore be encouraged to go back to the essenceof nursing and involve themselves in an interpersonaltherapeutic process with the elderly (Peplau 1998). Theneed for such therapy is highlighted by the already-known
GOING BEYOND PSYCHOTROPIC MEDICATIONS 13

fact that psychological problems are rarely resolved solelythrough the use of psychotropic drugs (Heffern 2000).
Insomnia in the elderly living in the community,psychotropic drug use and nursing careInsomnia is another health problem afflicting the elderlyin which there is a risk of confusing a normal state with apathological problem. Because of normal physiologicalaspects of the ageing process, sleep patterns change amongthe elderly, and increases in sleep latency are common. Itis also common for elderly people to experience an increasein the number and length of waking periods during thenight. Elders usually spend more time in bed and fre-quently take naps during the day (Cassel et al. 1997). Evengiven these changes in sleeping patterns, elderly peopleare not supposed to have any problems achieving the day’sactivities. But, as elderly people realize that their qualityof sleep is no longer the same as when they were younger,they may worry about their sleep patterns. For example,they may complain about their sleep latency, as well as thenumber of waking periods during the night. The situationcould prompt a nurse, sympathetic to an elderly person’scomplaints, to seek medical help for their sleep problems.Unfortunately, an opportunity to educate the person aboutthe impact of the normal ageing process on sleep patternsand to suggest non-pharmacological interventions tosupport rest and sleep is lost.
The complexity inherent in the assessment of sleepproblems among the elderly is reflected by the pattern ofhypnotic drug prescription to that group. Researchers havebeen unable to determine a correlation between the useof hypnotic drugs and sleeping patterns, good or bad, ofelderly people prescribed these drugs (Monane et al.1996). In fact, many studies have shown that hypnoticdrugs do improve quality of sleep among the elderly (Grad
1995; Ohayon & Caulet 1995; Grossberg & Grossberg1998), but only for a limited period of time, usually no morethan 30 days. Moreover, benzodiazepines, in particular,worsen sleep patterns by eliminating the slow-wave andREM essential to the restorative process of sleep (Closser1991). Following these observations, it has been recom-mended that the use of hypnotic drugs to treat sleepproblems must not exceed 30 days (Salzman et al. 1992;Tamblyn et al. 1994; Walsh et al. 1994; Grossberg &Grossberg 1998).
As in the case of depression, nurses are in a uniqueposition to reduce the likelihood that inappropriate med-ications will be introduced to manage sleep. First, they canteach the elderly about the impact of the normal ageingprocess on sleep patterns. This would reduce misinter-pretation and, subsequently, anxiety about the changes inthe quality of sleep that the elderly experience. Second, byapplying the Pittsburgh Sleep Quality Index (Buysse et al.1991), nurses can correctly identify elderly people whosesleep complaints warrant medical treatment. However,even if the index reveals poor quality of sleep and the needfor medical treatment, nurses are encouraged to involvethemselves in treatment by applying behavioural tech-niques to improve the sleep quality of the elderly. In fact,as studies indicate, such techniques should always beattempted before resorting to drug treatment (Grossberg& Grossberg 1998). Behavioural techniques have beenshown to successfully enhance the quality of sleep in theelderly (Cassel et al. 1997; Gatz et al. 1998). Moreover,improvement in sleep patterns is sustained when suchtechniques continue to be applied, contrary to sustaineduse of hypnotic drugs (Morin et al. 1999). Table 1 showssome of the features of behavioural techniques. Nurses candefinitely advocate this treatment for the benefit of theelderly living in both the community and long-term care.
14 P. VOYER AND L. SCHINDEL MARTIN
TABLE 1: Behavioural techniques to improve quality of sleep in elderly people
• Eliminate substances known to deteriorate quality of sleep (e.g. coffee, chocolate, alcohol)• Avoid environmental stimuli (e.g. noise, lighting)Create a stimulus-response process that will increase sleep quality:• Determine a consistent time to go to bed (e.g. 10.00 p.m.) and to get up (e.g. 6.00 a.m.) and maintain this for at least 6 weeks• Cease stimulating activities 1 h before going to bed (e.g. 9.00 p.m.)• Wait for symptoms of sleepiness before going to bed (e.g. yawning, drowsiness)• Create a ritual when symptoms of sleepiness appear (e.g. brushing teeth, locking doors, closing curtains) in order to induce a connection
between the ritual and sleep• Use beds only for sleep and for intimate relations. Avoid watching TV, reading books, eating and so on in bed• If after 20 min in bed the elder is not yet asleep, he or she must leave the room and wait until he or she feels sleepy again before re-entering• If the elder awakes during the night for more than 20 min, he or she must leave the room and wait until he or she feels sleepy again before
re-entering• Make the elder get out of the bed as early as possible before breakfast, in the case of elders living in the community between 6.00 and
7.00 a.m., or before breakfast for those living in a nursing home, regardless of the quality of sleep the night before• Limit naps during the day• Introduce the use of rocking chairs, largo baroque music, massage, aromatherapy, environmental white noise machines to promote relaxation• Elders need a great deal of support in the beginning of care because they may experience insomnia, loss of concentration, loss of energy, and
mood disturbances. Elders must be reassured that such symptoms are a normal stage of adjustment

Chronic use of benzodiazepine drugs in theelderly living in the community and nursing careThe prescription of benzodiazepines for over 30 days isquestionable, as benefits of their use beyond this periodare rare (Mcleod et al. 1997). Furthermore, chronic use ofbenzodiazepines results in the occurrence of significantand debilitating side-effects. Long-term use of benzo-diazepines among the elderly has been linked with cogni-tive deterioration (Berg & Dellasega 1996; Salzman et al.1992), poor functional autonomy (Ried et al. 1998), addic-tion (Murphy & Tyrer 1991; Stewart 1994; Taylor et al.1998; Woods & Winger 1995), falls (Ray et al. 1989) andcar accidents (Folks & Fuller 1997). Nevertheless, amajority of elderly people are prescribed benzodiazepinesfor months, and sometimes years (Damitz 1997; Ohayonet al. 1998; Snowdon 1999; Stewart 1994; Tamblyn et al.1994).
It is the responsibility of the nurse to assess chronicoveruse of benzodiazepines among elderly persons livingin the community. Programmes already exist that areproven to be effective in discontinuing benzodiazepine use(Graves et al. 1997; Tabloski et al. 1998; Voyer et al. 2001),but as most elderly people use benzodiazepines for morethan 30 days, it must be acknowledged that such pro-grammes are not widespread. Nevertheless, the discon-tinuation of this drug is associated with an improvementof cognitive capacity and a reduction in agitation, anxiety,insomnia and falls (Larson et al. 1987; Salzman et al. 1992).Nurses, in association with doctors, can identify elderlypeople’s chronic use of benzodiazepines. Then, when theyagree that it would be beneficial for an elderly person tostop or reduce his or her consumption, the nurse can beginthe discontinuation process. The collaboration betweenthe nurses and doctors is essential because it is difficult toachieve benzodiazepine withdrawal without professionalsupport (Campbell et al. 1999; Graves et al., 1997; Tabloski
et al. 1998). Table 2 describes a typical gerontologicaltitrated withdrawal programme.
Disruptive behaviours, cognitively impairedelders, restraints, neuroleptic drug use andnursing careDisruptive behaviour displayed by cognitively impairedelderly is frequently observed by nursing staff in nursinghomes (e.g. agitation, wandering, vocalizations, aggres-siveness). The prevalence of such behaviour ranges from43% to 93% in cognitively impaired elderly people (Beck& Shue 1994; Forbes 1998; Landreville et al. 1998; Taftet al. 1995; Tariot et al. 1996). Such behaviour resultsfrequently in: (i) the use of restraints and neuroleptics; (ii) isolation of the elderly patient; (iii) falls; and (iv)burnout, absenteeism, injuries and high turnover ratesamong health-care professionals (Beck & Shue 1994).
Algase et al. (1996) have redefined the concept of dis-ruptive behaviour. During the last decade, the commoninterpretation of dementia behaviour was that it was ‘dis-ruptive’. This is symptomatic of the lack of understandingof the very nature of the behavioural phenomenon associ-ated with dementia. It is clear that behaviours are labelledas disruptive because they disturb the routine of care staff.To correct the situation and reinstitute order to patternsof care, staff attempt to control dementia behaviour,frequently using neuroleptic medications to achieve this. Therefore, Algase et al. (1996) proposed the con-struct ‘Need-driven Dementia-compromised Behaviour’(NDB). This construct represents the nature of suchbehaviour, as symptomatic of an unmet need not solelyderived from cognitive losses and therefore modifiable.Thus, by investigating the cause of the NDB, suchbehaviour could be prevented or corrected, without theuse of neuroleptics or physical restraints.
Unfortunately, health-care professionals still respond to
GOING BEYOND PSYCHOTROPIC MEDICATIONS 15
TABLE 2: Characteristics of a typical withdrawal programme for geriatrics
• A formal preparation should be done before starting withdrawal in regard to:• The procedure (e.g. by how many milligrams the administration of drugs will be reduced [determined in collaboration with the doctor])• Psychological difficulties (e.g. anxiety regarding how the elder will sleep)• The possibility of adverse drug reactions (e.g. tremors. insomnia)• The nurse should teach a technique to control the symptom for which benzodiazepine has been prescribed (e.g. behavioural techniques for
insomnia)• A phone number should be given if the elder needs assistance or if she or he feels anxious about a particular symptomThe procedure• The philosophy of care should be that stopping the use of benzodiazepines is ideal, but reduction is acceptable. This will decrease the
pressure the elderly could feel in a rigid programme• It is usually recommended to diminish the dosage of the benzodiazepine by 25% per week. However, with the elderly, it is better to follow a
feeling of confidence of the elder in order to increase the odds of success. Nevertheless, it is not suggested to decrease the dosage by morethan 25% a week
• The procedure should allow the elder to slightly increase the dosage if he or she feels anxious after a reduction. Then after 1 or 2 weeks, thenurse can reduce the dosage again
• The procedure should not have a time limit. It is never too late to stop the use of these drugs when unneeded

NDB with psychotropic drugs and restraints (Beck & Shue1994; Bradley & Dufton 1995; Buckwalter et al. 1999;Cronin-Stubbs 1997; Forbes 1998; Hagen & Armstrong-Esther 1999; Hardin et al., 1994; Taft et al. 1995).Regardless of the prevalence of such treatment, it mustonly be undertaken as a last resort (Cummings 1995;Gerdner & Buckwalter 1994; Leroi et al. 1999). Nursingtreatments (observation tables for the evaluation of NDB,walking and cognitive stimulation programmes, life history,reminiscence therapy, prosthetic environment andphysical organization) aimed at behaviours and the envi-ronment have been shown to be more effective than drugsand restraints (Cronin-Stubbs 1997; Landreville et al.1998; Lehninger et al. 1998; Teri et al. 1999; Williams-Burgess et al. 1996). Despite this, studies report that 17%to 65% of elderly people in nursing homes are prescribedneuroleptic drugs (Beers et al. 1988; Hagen & Armstrong-Esther 1999; Snowdon 1999).
Need-driven dementia-compromised behaviourand neurolepticsNeuroleptics are incapable of reducing the prevalence ofNDB (Hagen & Armstrong-Esther 1999; Mirski et al.1998). The use of neuroleptics to reduce such behaviouras wandering, pacing, poor self-care, restlessness, impairedmemory, anxiety, insomnia, unsociability, indifference tosurroundings, fidgeting, nervousness, depression, unco-operativeness, agitation, difficult personality traits,spitting, constant requests, compulsively hiding thingsand/or lack of inhibitions (Lehninger et al. 1998), is notrecommended because of their limited effectiveness inmodifying such behaviour (Falsetti 2000; Hagen &Armstrong-Esther 1999; Leroi et al. 1999). Bair (2000) alsosuggested that delusions, paranoia and hallucinations arevery difficult to manage with neuroleptics, while Lamy(1993) suggested the contrary. In double-blind studies, theeffectiveness of neuroleptics has not been evident (Leroiet al. 1999). After reviewing this issue, Falsetti (2000)determined that not one neuroleptic was more effectivethan a placebo. In another study, it was demonstrated thatit is possible to reduce the use of neuroleptics in cogni-tively impaired elderly people without resulting in anincrease of NDB (Hagen & Armstrong-Esther 1999).Other studies suggest that neuroleptics can be helpful in18% to 40% of situations (Bair 2000; Buckwalter et al. 1999;Lamy 1993; Schneider et al. 1990) and counterproductivein another 10% of cases (Lamy 1993). But the addition ofbehavioural treatment as an adjunct to neurolepticsincreases the effectiveness of decreasing the manifesta-tions of NDB to 80% (Bair 2000).
It must be taken into account that the use of neuro-leptics is not without risk. For example, neuroleptic malig-nant syndrome is a very serious complication, one that can
even lead to death (Pelonero et al. 1998). There are alsothe more frequent anticholinergic effects. These couldcause cognitive impairment, constipation, urinary disor-ders, tachycardia, orthostatic hypotension, falls, fractures,syncope, stroke, cardiac effect, arrhythmia and heartblocks (Cummings 1995; Leroi et al. 1999). The ageingprocess itself increases the risk of being afflicted by theseside-effects. It is estimated that 50% of people aged65 years and older are at risk of anticholinergic effects(Falsetti 2000). But depending on the dementia experi-enced by the elderly, the risk can be even greater. Forexample, the destruction of dopaminergic receptorsamong those afflicted with Alzheimer’s disease increasesthe risk of anticholinergic effects. Moreover, 80% of elderlypeople afflicted by Lewy-body dementia developed sensi-tivity to a standard dosage of traditional neuroleptics, whichsubsequently increased the mortality rate (Falsetti 2000).Given these studies, the use of neuroleptics is question-able.
Need-driven dementia-compromised behaviourand restraintsThe same conclusions could be drawn about the use ofphysical restraints, as an average of 50% of the elderly arerestrained in nursing homes (Mayhew et al. 1999). Thereduction of the prevalence of physical restraints is still animportant challenge in nursing homes (Mayhew et al.1999). Physical restraints aim to reduce NDB and falls, butstudies have shown them to be counterproductive byactually increasing them (Landreville et al. 1998; Mayhewet al. 1999). Also, physical restraints are contributors todelirium among the elderly (Inouye 1998). The reductionof physical restraints must therefore be a goal for nursesin all nursing homes.
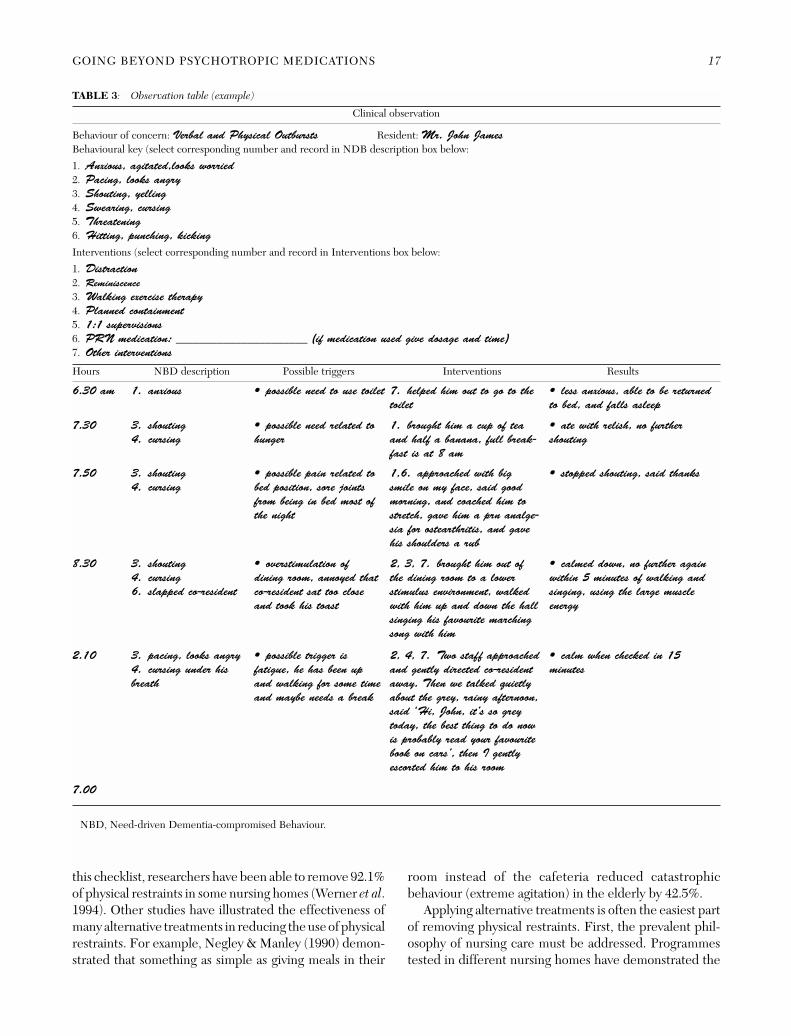
To achieve this goal, nurses must identify the factorscausing agitation among the elderly. Such identification isthe best way to prevent the occurrence of NDB. The useof an observation table with the aim of identifying under-lying causes of the NDB is often very effective (adaptedfrom (Arcand & Hébert 1997) (Table 3). The short versionof the Cohen-Mansfield Agitation Inventory could alsosupport the clinical judgement of nurses to identify thefactors responsible for agitation. However, the obser-vational skill of the nurse turns out to be the crucial factorin the evaluation of such behaviour.
Nurses must also be aware of alternative treatments tophysical restraints in order to remove restraints from elderlypeople currently undergoing such treatment. Knowledgeof such alternative treatments has been shown to be limitedamong nurses (Hardin et al. 1994). Nurses wanting tosupport the process of removing restraints could use theChecklist for Implementation of Alternatives to restraints(CIAR) (Werner et al. 1994). With the implementation of
16 P. VOYER AND L. SCHINDEL MARTIN
this checklist, researchers have been able to remove 92.1%of physical restraints in some nursing homes (Werner et al.1994). Other studies have illustrated the effectiveness ofmany alternative treatments in reducing the use of physicalrestraints. For example, Negley & Manley (1990) demon-strated that something as simple as giving meals in their
room instead of the cafeteria reduced catastrophicbehaviour (extreme agitation) in the elderly by 42.5%.
Applying alternative treatments is often the easiest partof removing physical restraints. First, the prevalent phil-osophy of nursing care must be addressed. Programmestested in different nursing homes have demonstrated the
GOING BEYOND PSYCHOTROPIC MEDICATIONS 17
TABLE 3: Observation table (example)
6.30 am 1. anxious • possible need to use toilet 7. helped him out to go to the
toilet
• less anxious, able to be returned
to bed, and falls asleep
7.30 3. shouting
4. cursing
• possible need related to
hunger
1. brought him a cup of tea
and half a banana, full break-
fast is at 8 am
• ate with relish, no further
shouting
7.50 3. shouting
4. cursing
• possible pain related to
bed position, sore joints
from being in bed most of
the night
1,6. approached with big
smile on my face, said good
morning, and coached him to
stretch, gave him a prn analge-
sia for ostearthritis, and gave
his shoulders a rub
• stopped shouting, said thanks
8.30 3. shouting
4. cursing
6. slapped co-resident
• overstimulation of
dining room, annoyed that
co-resident sat too close
and took his toast
2, 3, 7. brought him out of
the dining room to a lower
stimulus environment, walked
with him up and down the hall
singing his favourite marching
song with him
• calmed down, no further again
within 5 minutes of walking and
singing, using the large muscle
energy
2.10 3. pacing, looks angry
4. cursing under his
breath
• possible trigger is
fatigue, he has been up
and walking for some time
and maybe needs a break
2, 4, 7. Two staff approached
and gently directed co-resident
away. Then we talked quietly
about the grey, rainy afternoon,
said ‘Hi, John, it’s so grey
today, the best thing to do now
is probably read your favourite
book on cars’, then I gently
escorted him to his room
• calm when checked in 15
minutes
7.00
NBD, Need-driven Dementia-compromised Behaviour.
Clinical observation
Behaviour of concern: Verbal and Physical Outbursts Resident: Mr. John James
Behavioural key (select corresponding number and record in NDB description box below:
1. Anxious, agitated,looks worried
2. Pacing, looks angry
3. Shouting, yelling
4. Swearing, cursing
5. Threatening
6. Hitting, punching, kicking
Interventions (select corresponding number and record in Interventions box below:
1. Distraction
2. Reminiscence
3. Walking exercise therapy
4. Planned containment
5. 1:1 supervisions
6. PRN medication: ______________________ (if medication used give dosage and time)
7. Other interventions
Hours NBD description Possible triggers Interventions Results

effectiveness of implementing a different vision of nursingcare. Such a programme can include the use of videos,intensive courses, nurse coordinators, consultationservices, periodic visits by experts, help line and instit-utional journals sharing success stories. Using these strat-egies, Neufeld and colleagues (Neufeld et al. 1995) haveachieved a rate of physical restraint usage as low as 5%.One study almost entirely removed physical restraints fromthe elderly in nursing homes. At the beginning of theprogramme, 31.2% were restrained; only 1.6% remainedrestrained at the programme’s end (Werner et al. 1994).
Most importantly, many studies confirm that it ispossible to reduce the use of physical restraints withoutincreases in costs, falls, psychotropic drug use and numberof staff (Bradley & Dufton 1995; Evans et al. 1997; Mayhewet al. 1999). Mental health nurse specialists are thenencouraged to take a leadership role and apply these pro-grammes. Nurses are part of the solution, since a studydemonstrated that the number of nurses in nursing homesin eight countries was inversely associated with the amountof physical restraints used (Ljunggren et al. 1997).
Again, it seems clear that nurses possess the knowledgeand experience needed to enormously reduce chemicaland physical restraint use in the cognitively impairedelderly in nursing homes. Neuroleptic and physicalrestraint reduction is known to improve the mental healthof the elderly.
Concluding commentsHigh-quality mental health nursing care of elderly clientsis a goal that does not seem to have yet been widely realized.In this article, it was illustrated that nurses can providemore expansive care for elderly patients using psychotropicdrugs if they implement non-pharmacological, supportiveinterventions, either as an alternative strategy or as adjuncttherapy. Whatever the reason for which psychotropic drugshave been prescribed, it has been demonstrated that nursespossess the knowledge to help the elderly person to copewith the problem. In certain cases, non-pharmacologicalinterventions are preferable to the use of psychotropicdrugs. Nurses must be concerned that 10% of geriatric hos-pitalizations are related to the use of benzodiazepines(Closser 1991). Nurses have the skills to play a significantrole in the initial assessment and treatment of any mentalhealth problems experienced by the elderly. This involvestaking a careful history, including the use of documentationand behavioural analysis systems, and screening tools suchas the Geriatric Depression Scale and the Pittsburgh SleepQuality Index mentioned in this article. As a result, nurseswould be in the unique position to implement and evaluatenon-pharmacological interventions that would reduce theinitiation of unnecessary psychotropic medications. It ispossible that unfortunate outcomes associated with the
misuse of psychotropic drugs, such as hospitalization, couldbe decreased by high-quality nursing care.
REFERENCES
Abraham, I., Bottrell, M. M., Fulmer, T. & Mezey, M. D. (1999).Geriatric Nursing Protocols for Best Pratice. New York:Springer.
Algase, D. L., Beck, C., Kolanowski, A., Whall, A., Berent, S.,Richards, K. & Beattie, E. (1996). Need-driven dementia-compromised behavior: An alternative view of disruptivebehavior. American Journal of Alzheimer’s Disease,November/December, 10–19.
Aparasu, R. R., Mort, J. R. & Sitzman, S. (1998). Psychotropicprescribing for the elderly in office-based practice. ClinicalTherapy, 20, 603–616.
Arcand, M. & Hébert, R (Eds). (1997). Précis Pratique de Gériatrie,2nd edn. Québec: Bibliothèque nationale du Québec.
Bair, B. D. (2000). Presentation and recognition of commonpsychiatric disorders in the elderly. Clinical Geriatrics, 8,26–48.
Beck, C. K. & Shue, V. M. (1994). Interventions for treating dis-ruptive behavior in demented elderly people. Nursing Clinicsof North America, 29, 143–155.
Beers, M., Avorn, J., Soumerai, S. B., Everitt, D. E., Sherman, D. S.& Salem, S. (1988). Psychoactive medication use in inter-mediate-care facility residents. Journal of the AmericanMedical Association, 260, 3016–3020.
Berg, S. & Dellasega, C. (1996). The use of psychoactivemedications and cognitive function in older adults. Journal ofAging and Health, 8, 136–149.
Birrer, R., Singh, U. & Kumar, D. N. (1999). Disability anddementia in the emergency department. Ethical Issues inClinical Emergency Medicine, 17, 505–519.
Blazer, D. (1990). The epidemiology of depression in late life.Journal of Geriatric Psychiatry, 22, 35–52.
Blazer, D., Hughes, D. C. & George, L. K. (1987). The epi-demiology of depression in an elderly community population.Gerontologist, 27, 281–287.
Bradley, L. & Dufton, B. (1995). Breaking Free. The CanadianNurse, 91, 36–40.
Buckwalter, K. C., Stolley, J. M. & Farran, C. J. (1999). Managingcognitive impairment in the elderly: Conceptual, interventionand methodological issues. The Online Journal of KnowledgeSynthesis for Nursing, 6, 10.
Burke, M. M. & Walsh, M. B. (1997). Gerontologic Nursing,Wholistic Care of the Older Adult. London: Mosby.
Buysse, D. J., Reynolds, C. F., Monk, T. H., Hoch, C. C.,Yeager, A. L. & Kupfer, D. J. (1991). Quantification of sub-jective sleep quality in healthy elderly men and women usingthe Pittsburgh Sleep Quality Index (PSQI). Sleep, 14,331–338.
Campbell, A. J., Robertson, M. C., Gardner, M. M., Norton, R. N.& Bushner, D. M. (1999). Psychotropic medication with-drawal and a home-based exercise program to prevent falls: arandomized, controlled trial. Journal of American GeriatricsSociety, 47, 850–853.
18 P. VOYER AND L. SCHINDEL MARTIN

Cassel, C. K., Cohen, H. J., Larson, E. B., Meier, D. E.,Resnick, N. M., Rubenstein, L. Z. & Sorensen, L. B. (1997).Geriatric Medicine, 3rd edn. New York: Springer.
Chalifoux, Z., Neese, J. B., Buckwalter, K. C., Litwak, E. &Abraham, I. L. (1996). Mental health services for rural elderly:Innovative service strategies. Community Mental HealthJournal, 32, 463–480.
Closser, M. H. (1991). Benzodiazepines and the elderly. Journalof Substance Abuse Treatment, 8, 35–41.
Cronin-Stubbs, D. (1997). Interventions for cognitive impair-ment and neurobehavioral disturbances of older adults.Annual Review of Nursing Research, 15, 35–56.
Cummings, J. L. (1995). Dementia: the failing brain. The Lancet,345, 1481–1484.
Damitz, B. M. (1997). Drug utilization by elderly patients inBremen old age and nursing homes with special reference topsychotropic drugs. Gesundheitswesen, 59, 83–86.
Dealberto, M. J., Seeman, T., McAvay, G. J. & Berkman L. (1997).Factors related to current and subsequent psychotropic druguse in an elderly cohort. Journal of Clinical Epidemiology, 50,357–364.
Diagnostic and Statistical Manual of Mental Disorders, 4th edn(DSM-IV). (1994). Washington DC: American PsychiatricAssociation.
Evans, L. K., Strumpf, N. E., Allen-Taylor, S. L., Capezuti, E.,Maislin, G. & Jacobsen, B. (1997). A clinical trial to reducerestraints in nursing homes. Journal of the AmericanGeriatrics Society, 45, 675–681.
Falsetti, A. E. (2000). Rispiridone for control of agitation indementia patients. American Journal of Health-SystemPharmacy, 57, 862–870.
Folks, D. G. & Fuller, W. C. (1997). Anxiety disorders andinsomnia in geriatric patients. Geriatric Psychiatry, 20,137–164.
Forbes, D. A. (1998). Strategies for managing behavioral symp-tomatology associated with dementia of the alzheimer type:A systematic overview. Canadian Journal of NursingResearch, 30, 67–86.
Gatz, M., Fiske, A., Fox, L. S., Kaskie, B., Kasl-Godley, J. E.,McCallum, T. J. & Wetherell, L. J. (1998). Empirically vali-dated psychological treatments for older adults. Journal ofMental Health and Aging, 4, 9–46.
Gerdner, L. A. & Buckwalter, K. C. (1994). A nursing challenge.Assessment and management of agitation in Alzheimer’spatients. Journal of Gerontological Nursing, 20, 11–20.
Grad, R. M. (1995). Benzodiazepines for insomnia in community-dwelling elderly: A review of benefit and risk. Journal ofFamily Practice, 41, 473–481.
Graves, T., Hanlon, J. T., Schmader, K. E., Landsman, P. B.,Samsa, G. P., Pieper, C. F. & Wienberger, M. (1997). Adverseevents after discontinuing medications in elderly outpatients.Archive in Internal Medicine, 157, 2205–2210.
Grossberg, G. T. & Grossberg, J. A. (1998). Epidemiology ofpsychotherapeutic drug use in older adults. Clinics inGeriatric Medicine, 14, 1–5.
Hagen, B. & Armstrong-Esther, C. (1999). The question ofneuroleptic use in LTC. Canadian Nursing Home, 10, 9–17.
Hardin, S. B., Magee, R., Stratmann, D., Vinson, M. H., Owen, M.& Hyatt, E. C. (1994). Extended care and nursing home staffattitudes toward restraints. Moderately positive attitudesexist. Journal of Gerontological Nursing, 20, 23–31.
Harrington, C., Kovner, C., Mezey, M., Kayser-Jones, J., Burger, R.& Zimmerman, D. (2000). Experts recommend minimumnurse staffing standards for nursing facilities in the UnitedStates. The Gerontologist, 40, 5–16.
Hayes, K. S. & Kan, I. (2000). Challenges in emergency care: Thegeriatric patient. Journal of Emergency Nursing, 26, 430–435.
Heffern, W. A. (2000). Psychopharmacological and electro-convulsive treatment of anxiety and depression in the elderly.Journal of Psychiatric and Mental Health Nursing, 7, 199–204.
Inouye, S. K. (1998). Delirium in hospitalized older patients.Clinics in Geriatric Medicine, 14, 745–764.
Jorm, A. F. (2000). Does old age reduce the risk of anxiety anddepression? Review of epidemiological studies across theadult life span. Psychological Medicine, 30, 11–22.
Keks, N. A. & Burrows, G. D. (1995). Use of psychotropic drugsin the community. The Medical Journal of Australia, 163,62–63.
Kelman, G. & Mayer-Oakes, S. A. (1994). Relationships betweendepression and the use of antidepressants and benzo-diazepines in older community dwelling Southern-Californians. Clinical Gerontologist, 14, 71–72.
Kizer, K. W. & Vassar, M. J. (1998). Emergency department diag-nosis of abdominal disorders in the elderly. American Journalof Emergency Medicine, 16, 357–362.
Lamy, P. P. (1993). Understanding and managing Alzheimer’sdisease. The Journal of Practical Nursing, June, 45–58.
Landreville, P., Bordes, M., Dicaire, L. & Verreault, R. (1998).Behavioral approaches for reducing agitation in residents oflong-term-care facilities: Critical review and suggestions forfuture research. International Psychogeriatrics, 10, 397–419.
Larson, E. B., Kukull, W. A., Buchner, D. & Reifler, B. V. (1987).Adverse drug reactions associated with global cognitiveimpairment in elderly persons. Annals of Internal Medicine,107, 169–173.
Laurier, C., Dumas, J. & Grégoire, J. P. (1992). Factors relatedto benzodiazepine use in Quebec – A secondary analysis ofsurvey data. Journal of Pharmacoepidemiology, 2, 73–86.
Lauzon, S. & Adam, E. (1996). La personne âgée et ses besoins.Interventions infirmières. Montréal: ERPI.
Lehninger, F. W., Ravindran, V. L. & Stewart, J. T. (1998).Management strategies for problem behaviors in the patientwith dementia. Geriatrics, 53, 55–57.
Leroi, I., Steele, C. & Lyketsos, G. (1999). The care of patientswith dementia. Reviews in Clinical Gerontology, 9, 235–255.
Ljunggren, G., Philips, C. D. & Sgadari, A. (1997). Comparisonsof restraint use in nursing homes in eight countries. Age andAgeing, 26, 43–47.
Mayhew, P. A., Christy, K., Berkebile, J., Miller, C. & Farrish, A.(1999). Restraint reduction: Research utilisation and casestudy with cognitive impairment. Geriatric Nursing, 20,305–308.
Mcleod, P. J., Hung, A. R., Tamblyn, A. R. & Gayton, D. C. (1997).Defining inappropriate practice in prescribing for elderly
GOING BEYOND PSYCHOTROPIC MEDICATIONS 19
people: a national consensus panel. Canadian MedicalAssociation Journal, 156, 385–391.
Miller, C. A. (1999). Nursing care of older adults, Theory andPractice. Baltimore: Lippincott.
Ministère de la Santé et des Services Sociaux (MSSS). (1994).L’utilisation rationelle des médicaments chez les personnesâgées. Stratégie d’action. Québec: Bibliothèque nationale duQuébec.
Mirski, D. F., Brawman-Mintzer, O. & Mintzer, J. E. (1998).Pharmacological treatment of aggressive agitation inpatients with Alzheimer’s dementia. Clinical Geriatrics, 6,47–63.
Monane, M., Glynn, R. J. & Avorn, J. (1996). The impact ofsedative-hypnotic use on sleep symptoms in elderly nursinghome residents. Clinical Pharmacology Therapy, 59, 83–92.
Morin, C. M., Colecchi, C., Stone, J., Sood, R. K. & Brink, D.(1999). Behavioral and pharmacological therapies for late-lifeinsomnia: A randomized controlled trial. Journal of theAmerican Medical Association, 281, 991–999.
Murphy, S. M. & Tyrer, P. (1991). A double-blind comparison ofthe effects of gradual withdrawal of lorazepam, diazepam andbromazepam in benzodiazepine dependence. British Journalof Psychiatry, 158, 511–516.
Negley, E. N. & Manley, J. T. (1990). Environmental interven-tions in assaultive behavior. Journal of GerontologicalNursing, 16, 29–33.
Neufeld, R. R., Libow, L. S., Foley, W. & White, H. (1995). Canphysically restrained nursing-home residents be untiedsafely? Intervention and evaluation design. Journal of theAmerican Geriatrics Society, 43, 1264–1268.
Nolan, M. & Tolson, D. (2000). Gerontological nursing 1: chal-lenges in nursing older people in acute care. British Journalof Nursing, 9, 39–42.
Ohayon, M. M. & Caulet, M. (1995). Insomnia and psychotropicdrug consumption. Progress in Neuro-Psychopharmacologyand Biological Psychiatry, 19, 421–431.
Ohayon, M. M., Caulet, M., Priest, R. G. & Guilleminault, C.(1998). Psychotropic medication consumption patterns in theUK general population. Journal of Clinical Epidemiology, 51,273–283.
Ordre des Infirmières et Infirmiers du Québec (2000). Ordre desinfirmières et infirmiers du Québec. L’exploitation des aînés.Québec: Dépôt Légal, Bibliothèque Nationale du Québec.
Papillon, M. J., Laurier, C., Bernard, L. & Baril, J. (2000).Consommation de médicaments. In Daveluy, C., Pica, L.,Audet, N., Courtemanche, R., Lapointe, F (Eds.) EnquêteSociale et de Santé 1998. (pp. 445–460) Collection la santé etle bien-être (Ch. 22). Québec: Institut de la statistique.
Paterniti, S., Dufouil, C., Bisserbe, J.-C. & Alperovitch A. (1999).Anxiety, depression, psychotropic drug use and cognitiveimpairment. Psychological Medicine, 29, 421–428.
Pelonero, A. L., Levenson, J. L. & Pandurangi, A. K. (1998).Neuroleptic Malignant Syndrome: A review. PsychiatricServices, 49, 1163–1172.
Peplau, H. E. (1998). Interpersonal Relations in Nursing: AConceptual Frame of Reference for Psychodynamic Nursing.London: Macmillan Education.
Poncia, H. D. M., Ryan, J. & Carver, M. (2000). Next-day tele-phone follow-up of the elderly: a needs assessment and criticalincident monitoring tool for the accident and emergencydepartment. Journal of Accident and Emergency Medicine,17, 337–340.
Ray, W. A., Griffin, M. R. & Downey, W. (1989). Benzodiazepinesof long and short elimination half-life and the risk of hipfracture. Journal of the American Medical Association, 262,3303–3307.
Ried, L. D., Christensen, D. B. & Stergaghis, A. (1990). Medicaland psychological factors predictive of psychotropic drug usein elderly patients. American Journal of Public Health, 80,1349–1353.
Ried, L. D., Johnson, R. E. & Gettman, D. A. (1998).Benzodiazepine exposure and functional status in olderpeople. Journal of American Geriatrics Society, 46, 71–76.
Salzman, C., Fisher, J., Nobel, K., Glassman, R., Wolfson, A. &Kelley, M. (1992). Cognitive improvement following benzo-diazepine discontinuation in elderly nursing home residents.International Journal of Geriatric Psychiatry, 7, 89–93.
Schneider, L. S., Pollock, V. E. & Lyness, S. A. (1990). A meta-analysisof controlled trials of neuroleptic treatment in dementia.Journal of the American Geriatrics Society, 38, 553–563.
Simonson, W. (1984). Medications & the Elderly. A Guide forPromoting Proper Use. Rockville: Aspen Publication.
Smith Black, B., Rabins, P. V., German, P., McGuire, M. & Roca, R.(1997). Needs and unmet needs for mental health care amongelderly public housing residents. The Gerontologist, 37,717–728.
Snowdon, J. (1999). Research – a follow-up survey of psycho-tropic drug use in Sydney nursing homes. Medical Journal ofAustralia, 170, 299–304.
Stevenson, G., Kellogg, L. A., Ernst, V. I. & Whinney, P. P. (1989).Medication Use and Elderly People. Senior Drug ActionProgram. British Columbia: Ministry of Health.
Stewart, R. B. (1994). Benzodiazepine use in an ambulatoryelderly population: a 14-year overview. Clinical Therapeutics,16, 118–124.
Stone, J. T., Wyman, J. F. & Salisbury, S. A. (1999). ClinicalGerontological Nursing, A Guide to Advanced Practice, 2ndedn. Tokyo: W.B. Saunders company.
Tabloski, P. A., Cooke, K. M. & Thoman, E. B. (1998). A proce-dure for withdrawal of sleep medication in elderly women whohave been long-term users. Journal of Gerontological Nursing,24, 20–28.
Taft, L. B. & Cronin-Stubbs, D. (1995). Behavioral symptoms indementia: An update. Research in Nursing and Health, 18,143–163.
Tamblyn, R. M. (1996). Medication use in seniors: Challengesand solutions. Therapie, 51, 269–282.
Tamblyn, R. M., McLeod, P. J., Abrahamowicz, M., Monette, J.,Gayton, D. C., Berkson, L. et al. (1994). Questionable pre-scribing for elderly patients in Quebec. Canadian MedicalAssociation Journal, 150, 1801–1809.
Tariot, P. N., Porsteinsson, A., Teri, L. & Weiner, M. F. (1996).Measuement of behavioral disturbance in chronic carepopulations. Journal of Mental Health and Aging, 2, 213–229.
20 P. VOYER AND L. SCHINDEL MARTIN

Taylor, S., McCracken, C. F. M., Wilson, K. C. M. & Copeland, J. R. M. (1998). Extent and appropriateness ofbenzodiazepine use. British Journal of Psychiatry, 173,433–438.
Teri, L., Logsdon, R. G. & Schindler, R. J. (1999). Treatment ofbehavioral and mood disturbances in dementia. Generations,Fall, 50–56.
Van Gerven, P. W. M., Paas, F. G. W. C., Van Merriënboer, J. J. G.& Schmidt, H. G. (2000). Cognitive load theory and the acqui-sition of complex cognitive skills in the elderly: towards anintegrative framework. Educational Gerontology, 26,503–521.
Voyer, P., Richard, L. & Dupont, L. (2001). Un programme desevrage personnalisé chez les aînés, changer une habitudepour gagner en latitude. L’infirmière Canadienne, 2, 10–15.
Walsh, J. K., Hartman, P. G. & Kowall, J. P. (1994). Insomnia. InS. Chokroverty (Ed), Sleep Disorders, Medicine: Basic
Science, Technical Considerations and Clinical Aspects(pp. 219–239). Boston: Butterworth-Heinemann.
Wancata, J., Bend, N. & Müller, C. (1997). Psychotropic drugintake in residents newly admitted to nursing homes.Psychopharmacology, 134, 115–120.
Werner, P., Koroknay, V., Braun, J. & Cohen-Mansfield, J. (1994).Individualized care alternatives used in the process ofremoving physical restraints in the nursing home. Journal ofthe American Geriatrics Society, 42, 321–325.
Williams-Burgess, C., Ugarriza, D. & Gabbai, M. (1996).Agitation in older persons with dementia: A research synthe-sis. The Online Journal of Knowledge synthesis for Nursing,3 (13).
Woods, J. H. & Winger, G. (1995). Current benzodiazepineissues. Psychopharmacology, 118, 107–115.
GOING BEYOND PSYCHOTROPIC MEDICATIONS 21