Embed Size (px)
Citation preview

Improving clinical practice –a world of experience
The Global Partnership for Effective Diabetes Management, including the development of this slide set, is supported by GlaxoSmithKline

• At diagnosis of type 2 diabetes:
50% of patients already have complications1
up to 50% of -cell function has
already been lost2
• Current management:
two-thirds of patients do not
achieve target HbA1c3,4
majority require polypharmacy
to meet glycaemic goals over time5
Need for an early and intensive approach to type 2 diabetes management
1UKPDS Group. Diabetologia 1991; 34:877–890. 2Holman RR. Diabetes Res Clin Prac 1998; 40 (Suppl.):S21–S25. 3Saydah SH et al. JAMA 2004; 291:335–342. 4Liebl A et al. Diabetologia 2002; 45:S23–S28. 5Turner RC et al. JAMA 1999; 281:2005–2012.

Management of diabetes is evolving
7.0
6.5
6.0
Individualised HbA1c goals
New global guidelines
Tighter HbA1c goals
EVOLVING PRACTICE
Treating to target vs. stepwise
•Comprehensive•Standard•Minimal
Tailoring to health systems

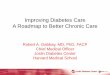
Stepwise approach: delays control and leaves patients at risk of complications
OAD = oral anti-diabetic1Adapted from Del Prato S et al. Int J Clin Pract 2005; 59:1345–1355.
2Stratton IM et al. BMJ 2000; 321:405–412.
Duration of diabetes
Hb
A1c
(%
)1
7
6
9
8
10
Diet andexercise
OADmonotherapy
OAD combination
OAD +basal insulin
OAD monotherapy
uptitration
OAD + multiple daily
insulin injections
Mean
Complications2

Early, intensive intervention: reach glycaemic goals and reduce the risk of complications
OAD = oral anti-diabetic1Adapted from Del Prato S et al. Int J Clin Pract 2005; 59:1345–1355.
2Stratton IM et al. BMJ 2000; 321:405–412.
Duration of diabetes
Hb
A1c
(%
)1
7
6
9
8
10
Complications2
Diet andexercise
OAD monotherapy
OAD combination
OAD uptitration
OAD + basal insulin
OAD + multipledaily insulin
injections
Mean

The Global Partnership recommendations:
*Or fasting/preprandial plasma glucose < 110 mg/dl (6.0 mmol/l) where assessment of HbA1c is not possible
• Aim for good glycaemic control = HbA1c < 6.5%*
< 6.5%< 6.5%• Treat patients intensively to achieve target HbA1c < 6.5%* within 6 months of diagnosis
• After 3 months, if patients are not at target HbA1c < 6.5%,* consider combination therapy
• Monitor HbA1c every 3 monthsin addition to regular glucose self-monitoring
Del Prato S et al. Int J Clin Pract 2005; 59:1345–1355.

Paradigm for early combination treatment
If HbA1c > 6.5%*at 3 months
Initiate combination therapy† in parallel with diet/exercise
If HbA1c 9% at diagnosis
Initiate combination therapy† or insulin
in parallel with diet/exercise
0 1 2 3 4 5 6
If HbA1c < 9% at diagnosis
Initiate monotherapy in parallel with diet/exercise
Months from diagnosis
Treat to goal of
HbA1c < 6.5%* by 6 months
*Or fasting/preprandial plasma glucose < 110 mg/dl (6.0 mmol/l) where assessment of HbA1c is not possible†Combination therapy should include agents with complementary mechanisms of action
Del Prato S et al. Int J Clin Pract 2005; 59:1345–1355.

Encouraging early treatment to glycaemic goal
Happy 7 campaign, Korea

Encouraging early, intensive intervention:Happy 7, Korea
• Initiated in response to poor understanding of HbA1c and importance of quickly achieving glycaemic goals
• Objectives:– Change doctors’ beliefs and
behaviours towards HbA1c measurement
– Increase awareness of HbA1c among patients
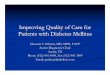
Most Korean patients with T2DM do not have good glycaemic control
HbA1c > 8%
HbA1c
< 7%
HbA1c 7–8%
36%32%
32%

Happy 7: The campaign
• ~20,000 patients with type 2 diabetes in 300 clinics
• 2-day programme in each clinic, including:– Patient and nurse education
– HbA1c measurement using portable testing equipment
– BMI, waist size and plasma glucose
• Detailed report generated for each clinic

Happy 7: the results
A positive response… but more work to do
Committed to morefrequent HbA1c testing…
…in the majority (~80%) of their patients…
… but, HbA1c is only asupplementary test
• On follow-up, some clinics had not maintained changes and hadreverted to old habits
Consistent, co-ordinated and complementary programme of activities needed to produce effective and enduring changes
% of doctors
0 10010 20 30 40 50 60 70 80 90

Role of guidelines in encouraging early, intensive intervention
Adapted from: Wood D et al. Eur Heart J 1998; 19:1434 1503. NCEP Expert Panel. JAMA 2001; 285:24862497. Erhardt L et al. Vascular Disease Prevention 2004; 1:167174.
Objectives
Simplify management, improve quality of care
Summarise scientific consensus
Provide best advice available
Define patients at risk, set goals for prevention/therapy

ADA 2004†
IDF Global IDF Western
Pacific
ALAD 2000
CDA*ADA 2003
AACE Roadmap
Global Partnership
ALAD 2007§
CDA* ADA 2004†
ADA/EASD‡
Guidelines and the drive for tighter glycaemic control
*CDA: goal 7%, or < 6% in individuals “in whom it can be achieved safely”. †ADA: from 2004 onwards, goal for ‘patients in general’ is < 7%, while goal for ‘individual patients’ is ‘as close to normal (< 6%) as possible without significant hypoglycaemia. ‡ADA/EASD Consensus Statement: “Target HbA1c as close to
the non-diabetic range as possible, minimum < 7%”. §ALAD 2007: unpublished.
Hb
A1c
6.0%
6.5%
7.0%
7.5%
1999 2000 2001 2003 2004 2005 2006 2007

For guidelines to work, they need to be implemented
• Guidelines are designed to improve the care of patients
• It takes a lot of time and effort to develop good management guidelines
• Despite this, guidelines are often not followed in routine clinical practice
• The barriers to guideline implementation must be understood and addressed if patient care is to improve

Common barriers to implementing guidelines
Lack of reimbursement
Inability to reconcile guidelines with patient
preferences
Lack of adherence to lifestyle modifications
Organisational constraints
Inadequate staffing resource and
specialist support
Lack of awareness, familiarity and
agreement
Low motivation and/or outcome expectancy
Lack of awareness and understanding
Limited access to care
Insufficient time and/or resource
Increasedlegal liability
Poor compliance; reluctance to take
life-long medication
Healthcare Systems Doctors Patients
Adapted from Erhardt L et al. Vascular Disease Prevention 2004; 1:167174 Cabana MD et al. JAMA 1999; 282:14581465.

Barriers to physician uptake
Adapted from Cabana MD et al. JAMA 1999; 282:14581465.
“I didn’t know there were guidelines”
“I haven’t read the
guidelines”
“It’s all good in theory, but
practice is different”
“I know what’s best
for my patients”
“My patients are happy
with their care as it is”
“It takes time – time I
haven’t got”
Knowledge Improved outcomes
Attitudes Behaviour
“My patients are better
controlled now”
“I’m more confident I’m
doing the best for my patients”

Improving implementation of treatment guidelines
Canadian Diabetes Association guidelines, The GIANT Study & Project Ideal

Development and communication of guidelines: Canadian Diabetes Association 2003
• Advocated early and intensive management
• Multi-disciplinary team approach• Plans for dissemination integral
to development• Practical tool: cross-referencing,
clinical tools, links• Fed into government initiatives• Partners in Progress: work with
industry to disseminate CDA-verified materials
• Available online, with downloadable slides
Canadian Diabetes Association. Can J Diabetes 2003; 27 (Suppl 2):S1152.Canadian Diabetes Association E-guidelines. http://www.diabetes.ca/cpg2003/

Does following guidelines impact patient care?The GIANT study
General practitioner
Implementation in
Asia of
Normoglycaemic
Targets
100 family doctors
*Based on International Diabetes Federation Western Pacific Region guidelines and involving: initial educational symposiumand follow-up continuing medical education symposium at 3 months; reminders about guidelines sent to doctors every 3 months;desktop reminder cards; patient diary cards to prompt discussion/record information
Randomisation
Education onguidelines*
No education onguidelines
Four subjects with T2DM for each doctor
Primary outcome: HbA1c change at 6 months
Secondary outcomes:FPG, blood pressure, adverse events, healthcare use, treatment escalation
Study due to complete
by end 2008
General Practitioner Implementation in Asia of Normoglycaemic Targets. http://www.clinicaltrial.gov/ct/show/NCT00499824?order=4

Project IDEAL
• Community-based initiative among low-income residents of North Carolina, USA
• Assessed the impact of 14 programmes designed to improve adherence to guidelines and quality of care
• Programmes included:– New education/care programmes at existing healthcare facilities– Mobile screening, education and healthcare units– Advice in community pharmacies/physicians’ offices– Diabetes educator/nurse practitioner visits to residential facilities
Bell RA et al. NC Med J 2005; 66:96102.
Improving Diabetes Education, Access to care, and Living

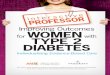
Project IDEAL: Overcoming barriers to guideline implementation
*Blood pressure < 140 mmHg systolic and < 90 mmHg diastolic; †LDL-c < 100 mg/dL
HbA1c tested
HbA1c control:< 8.0%
< 7.0%
Lipids tested
LDL-c control†
Nephropathy assessed
Dilated eye exam
Blood pressure tested
Blood pressure control*
Complete foot exam
Baseline (1998) Patients (%)
0 10010 20 30 40 50 60 70 80 90Follow-up (2001)
Bell RA et al. NC Med J 2005; 66:96102.

The benefits of themultidisciplinary approach

Key function of the multidisciplinary team
To provide:
Continuous, accessible and consistent care focused on the needs of individuals with type 2 diabetes

Additional functions of a multidisciplinary team
• Provide input at diagnosis of condition and continually thereafter to:– agree standards of care
– discuss rational therapeutic suggestions
– monitor guideline adherence and short-term outcomes
– avoid early complications or provide timely intervention to decrease diabetes-related complications
• Enable long-term patient
self-management
Codispoti C et al. J Okla State Med Assoc 2004; 97:201–204.

The multidisciplinary team:core members
DieticianDietician
Diabetes specialist
nurse
Diabetes specialist
nursePatientPatient
PhysicianPhysician
PodiatristPodiatrist
National Diabetes Education Program. Team care: comprehensive lifetime management for diabetes. www.ndep.nih.gov/resources/health.htm.

The multidisciplinary team: additional members
Pharmacist
Diabetologist/endocrinologist
Other specialists
DieticianDietician
Diabetes specialist
nurse
Diabetes specialist
nursePatientPatient
PhysicianPhysician
PodiatristPodiatrist
National Diabetes Education Program. Team care: comprehensive lifetime management for diabetes. www.ndep.nih.gov/resources/health.htm.

Benefits of the multidisciplinary approach
Kaiser Permanente & PEDNID LA studies

Improvements in patient care: Kaiser Permanente Medical Care Program, California
• Individuals with poorly controlled diabetes randomised to outpatient care from:– multidisciplinary nurse led team
(diabetes nurse educator, psychologist, nutritionist and pharmacist) (n=97)
– or primary care physician (n=88)
• After 6 months, multidisciplinary team approach associated with:
significant improvements in glycaemic control
significant reductions in hospital admissions and outpatient visits
Sadur CN et al. Diabetes Care 1999; 22:2011–2017 Copyright © 1999 American Diabetes Association
Adapted with permission from The American Diabetes Association
–1.4–1.2
–1.0
–0.8–0.6
–0.4
–0.2
0
Multidisciplinaryteam
Control
Cha
nge
in H
bA1
c fr
om b
ase
line
(%)
HbA1cHbA1c
30
25
20
15
10
5
0
Hos
pita
lisat
ions
/10
00
per
son-
mon
ths
HospitalisationHospitalisation
Multidisciplinaryteam
Control

Improved cost-effectiveness: Co-operative Latin American implementation study (PEDNID LA)
• Educational model designed/adapted to local conditions by multidisciplinary team in 10 Latin American countries (n = 446)
• Four weekly teaching units plus reinforcement session at 6 months
• Family members and spouses encouraged to attend
Significant improvements in FPG, HbA1c, body weight, blood pressure, cholesterol, triglycerides
Reduction in pharmacotherapy → 62% decrease in treatment costs
Gagliardino JJ & Etchegoyen G. Diabetes Care 2001; 24:1001–1007.
0
20,000
40,000
60,000
80,000
100,000
120,000
Baseline 12 months
Cos
t of
pha
rmac
othe
rapy
/yea
r (U
S$)
Costs↓ 62%

Key steps for improving clinical practice
Disease management programmes can improve management of chronic disorders, includingtype 2 diabetes
Achieve glycaemic goals as quickly as possible using early, intensive intervention
Tailor education about the importance of achieving glycaemic goals to the target audience
Make recommendations practical and engage all relevant parties
Use co-ordinated and complementary campaigns to build long-term improvements in care