Embed Size (px)
Citation preview

Sleep Medicine 14 (2013) 1334–1340
Contents lists available at ScienceDirect
Sleep Medicine
journal homepage: www.elsevier .com/locate /s leep
Original Article
Improvement of intensive care unit sound environment and analysesof consequences on sleep: an experimental study
1389-9457/$ - see front matter � 2013 Elsevier B.V. All rights reserved.http://dx.doi.org/10.1016/j.sleep.2013.07.011
⇑ Corresponding author. Tel.: +46 (0) 31 786 3604; fax: +46 (0) 31 409 728.E-mail address: [email protected] (K. Persson Waye).
Kerstin Persson Waye a,⇑, Eva-Maria Elmenhorst b, Ilona Croy a, Eja Pedersen c
a Department of Occupational and Environmental Medicine, Gothenburg University, Medicinaregatan 16, 405 30 Göteborg, Swedenb German Aerospace Center (DLR), Institute of Aerospace Medicine, 51170 Cologne, Germanyc Environmental Psychology, Department of Architecture and Built Environment, Lund University, P.O. Box 118, SE-221 00 Lund, Sweden
a r t i c l e i n f o a b s t r a c t
Article history:Received 28 February 2013Received in revised form 19 July 2013Accepted 26 July 2013Available online 3 September 2013
Keywords:Intensive careNoiseSoundSleepCortisolArousalExperimental
Objective: Uninterrupted sleep is of vital importance for restoration and regaining health. In intensivecare units (ICUs) where recovering and healing is crucial, patients’ sleep often is fragmented and dis-turbed due to noise from activities from oneself, other patients, and alarms. The aim of our study wasto explore if sleep could be improved by modifying the sound environment in a way that is practicallyfeasible in ICUs.Methods: We studied the effects of originally recorded ICU noise and peak reduced ICU noise on sleep inhealthy male participants. Sleep was registered with polysomnography (PSG) during four nights: oneadaptation night, one reference (REF) night, and the two exposed nights with similar equivalent soundlevels (47 dB LAeq) but different maximum sound levels (56- vs 64-dB LAFmax). The participants answeredquestionnaires and saliva cortisol was sampled in the morning.Results: During ICU exposure nights, sleep was more fragmented with less slow-wave sleep (SWS), morearousals, and more time awake. The effects of reduced maximum sound level were minor. The subjectivedata supported the polysomnographic findings, though cortisol levels were not significantly affected bythe exposure conditions.Conclusions: Noise in ICUs impairs sleep and the reduction of maximal A-weighted levels from 64 to56 dB is not enough to have a clear improved effect on sleep quality.
� 2013 Elsevier B.V. All rights reserved.
1. Introduction
Since the 1970s, numerous articles have reported that patientsin intensive care units (ICUs) have fragmented or otherwise dis-turbed sleep patterns. More than 60% of patients treated in ICUs re-port insomnia or sleep deprivation [1,2]. It is well-established thatuninterrupted sleep is important for recovery and sustained health[3,4], and experimental studies in animals and healthy volunteersshowed that sleep deprivation affects several physiologic parame-ters which may adversely affect the recovery of patients undercare. Examples of outcomes due to sleep deprivation are glucoseintolerance, increased insulin resistance, activation of the hypotha-lamic–pituitary–adrenal axis, increase of inflammatory cytokines[5–7], and reduced consolidation of memory and certain cognitivefunction [8].
The cause of sleep disturbance in ICUs is multifactorial andaside from the patient’s medical conditions, medication, respira-tory care and care procedures, environmental factors includingnoise play a role. Although the relative contribution often is not
possible to assess [9], it was concluded in a review of currentknowledge about sleep in the ICU that noise is a notable contribu-tor to sleep disorders [10]. Importantly, noise-induced sleep distur-bance can be diminished in contrast to most other sleep disturbingfactors in ICUs. Specific data were provided by Freedman et al. [10]who reported that approximately 11–17% of the respective awak-enings of the arousals were caused by noise and Gabor et al. [11]who found that noise and patient care activities were responsiblefor up to 30% of the arousals and awakenings in a small study.Other studies linking the acoustic environment in health care withsleep disturbance point to its influence on physiologic arousalsduring sleep, increase of awakenings, and increased respiratoryactivity during sleep [12–14]. The interpretations of these findingsare complex. Critically ill patients have disturbed electroencepha-lographic patterns caused by possible cerebral metabolic changesas seen in sepsis, electrolytic disorders, neurologic pathology, andmedication, among others, and the sleep staging in accordancewith the American Association of Sleep Medicine 2007 criteria[15] cannot be met. Therefore, it is advantageous to study the ef-fects of sleep structures due to alterations of the acoustic environ-ment in healthy participants in a simulated ICU situation.

K. Persson Waye et al. / Sleep Medicine 14 (2013) 1334–1340 1335
Sound levels in health care have sharply risen since the 1960s[16]. On average, the noise level has increased by approximately4 dB per 10-year interval between 1960 and 2005, which approxi-mates a doubling of the perceived loudness over a 20-year period.The sound environment at ICUs is characterized as highly intermit-tent with an average of 150–200 sound peaks above 80 dBA be-tween midnight and 6:00 am [17]. A more recent study extendedthose results to identify the occurrence of periods <45 dB LAeq
[18], which can be considered as restorative according to theWorld Health Organization guidelines [19]. During one measure-ment week there were no such restorative periods during thenight. The mean length of periods of less than 50 dB LAeq was13 min, and the longest nocturnal restorative period during thewhole week was 50 min. Particularly high levels of noise can befound at technology intensive wards such as ICUs and operatingrooms. Primary sources of noise are medical equipment such ascardiac monitors and ventilators, caregiving activities, sounds fromother patients, and other staff activity (e.g., talking, walking, tele-phone conversations) [20]. Sudden loud noise is mainly generatedfrom medical equipment and the alarms and occurs in combinationwith activity noise in the care and movement of patients and calls.Such signals and sounds induce immediate but relatively shortduration autonomic reactions in humans [21], which are knownto be even greater during sleep [22].
The abundant and seemingly increasing noise level and its seri-ous health impacts suggests that it would be useful to try to min-imize noise levels in ICUs. Such attempts have been evaluated in ahandful of studies where sound levels were slightly reduced byadding ceiling panels [23] or where the impact was modified byintroducing white noise [14]. Further studies are needed to deter-mine what sound quality changes are required in ICUs to promoteadequate sleep quality and restoration. Our study aimed to initiatethis process by investigating if recorded sounds from an ICU in-duced sleep disturbance among healthy individuals and if sleepcan be improved by making simple alterations in the ward affect-ing some sound quality aspects.
2. Methods
2.1. Sleep laboratory and design
Sounds recorded at ICUs were played back in the bedrooms ofthe sound laboratory at Environmental and Occupational Medicine,Gothenburg University, Sweden. The laboratory is built as an apart-ment to which the participants have their own key. The apartmentcomprises a hall, a combined television room and kitchen,bathrooms, and three bedrooms and a toilet on the top floor. Thebedrooms are constructed so that sounds or vibrations from thesurroundings are completely prevented and the background noiselevel with full ventilation is less than 15 dBA. The sound exposuresare transmitted from the control room to the bedrooms via hiddenloudspeaker systems in the ceiling and on the walls. For thepurpose of our study, the bedrooms were sparsely furnished toresemble a patient room. Healthy male participants slept in thelaboratory for four consecutive nights. The first night served asadaptation, i.e., the participants followed the same procedure anddata (not to be used in the analyses) were collected just as in thefollowing nights (Table 1). The second night was the baseline night,followed by exposure to two modes of ICU sound on nights 3 and 4.Half of the participants were exposed in the order A and half in theorder B. Data were collected by polysomnography (PSG) at night,saliva sampling in the mornings, and questionnaires in the morn-ings. Analyses of PSG and saliva were blinded, with assessing staffunaware of the exposure. Eighteen participants were originallyrecruited; however, 17 completed the study after a late dropout.
All measurements were successfully collected except for two ofthe PSG recordings during the control night. Therefore, the numberof participants for most of the reported values was 17; however,the number was reduced to 15 when the physiologic data fromthe control night were included in the analyses.
2.2. Participants
Male participants aged 18–30 years were recruited by posters atthe university campus. Exclusion criteria were (1) reduced hearingacuity (>20-dB hearing loss at a single frequency, as tested withaudiometer Entomed SA 201), (2) a body mass index of >28, (3)self-reported snoring, (4) self-reported allergies or hypersensitiv-ity, and (5) smokers or ‘‘snuffers’’. Eighteen participants were se-lected and 17 participants completed the experiment (age, 19–29 years; mean age, 22.9 years). They were instructed to come tothe sleep laboratory at 8:00 pm and go to bed at 11:00 pm; theywere woken up at 06:46 am but otherwise could attend their nor-mal daily activities. The participants were not allowed to drink cof-fee, tea, energy drinks, or cola after 3:00 pm during theexperiment. The PSG equipment was attached between 8:00 and11:30 pm, and the participants were then free to move around inthe laboratory apartment before going to bed. All participantssigned an informed consent according to the Declaration of Hel-sinki. The study was approved by the Ethics Committee of Göte-borg, Sweden. The participants were reimbursed for theirparticipation.
2.3. Sound exposures
The exposure sounds used in our study were recorded duringnights in the ICU at Borås hospital using a Head Squadriga sin-gle-channel system (Head acoustics), with the microphone hang-ing from the ceiling approximately 40 cm above a patient.Representative sequences were selected from nighttime recordingsand included (1) sound from a respirator comprising a dominantportion at approximately 100 Hz and its harmonics from a fan aswell as high frequency components from air fluids and respiration;and (2) a variety of alarms, doors closing, human voices, and rus-tling. The sounds were played back in two modes, one with the ori-ginal sound quality aspects but reduced with LAeq 7-dB (ICU) andone with modified sound quality (ICU_peak reduced) equally re-duced with LAeq 7 dB. For the ICU_peak reduced mode we simu-lated a realistic scenario by lowering the levels of the loudestalarms but keeping them audible and achieving a quiet closing ofthe door using a door stopper. Therefore, we excluded all alarmsexceeding LAFmax 55 dB and all the sounds of the doors closing,though voices and rustling were the same in both modes. We esti-mated that such changes could be feasible in real situations. Duringthe adaptation night and reference night, a background sound rep-resenting a quiet ventilation system (LAeq, 20.0 dB; LAFmax, 20.9 dB)was played back to prevent the room from being quiet. Acousticdescription of the background sound and the exposure soundsare presented in Table 2, as measured by 10 cm above the pillowin the bedroom before the beginning of the experiment. Calibrationof the sound levels was done before the beginning of each week.
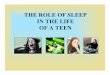
The sound files of the two exposures were repeated every60 min (Fig. 1). The playback started at 12:00 am with an 8 minrise time to full volume, and it was kept at the same overall volumeuntil 6:45 am when it was stopped with a wakeup call.
2.4. PSG and cortisol sampling
Polysomnographic recordings included electroencephalogram,electrooculogram and submental electromyogram, breathing,pulse, and oxygen saturation. The position of the electrodes and

Table 1Design of the experimental study.
Sequence Night 1 2 3 4subjects a Adaptation Control Exposure Exposure
A 9 Background BackgroundREFb
SoundICUc
SoundICU_peakreducedd
B 8 Background BackgroundREFb
SoundICU_peakreducedd
SoundICUc
Abbreviations: REF, reference night; ICU, intensive care unit.a Remaining for the analyses of cortisol and questionnaires.b Background sound representing a quiet ventilation system (REF).c Sound from ICU with original quality aspects.d Sound from ICU with modified sound quality (fewer and attenuated peak levels
of the alarms and without the sounds of doors closing).
Table 2Exposure characterization of the sounds during the experiment nights.
LAeq LAFmax No. of eventsLAFmax P50 dB/h
No. of eventsLAFmax >55 dB/h
REF 20.0 20.9 0 0ICU_peak reduced 46.9 55.9 18 0ICU 47.2 64.0 21 7
Abbreviations: No., number; h, hour; REF, reference night; ICU, intensive care unit.
1336 K. Persson Waye et al. / Sleep Medicine 14 (2013) 1334–1340
the polysomnographic analyses were performed in accordance tothe American Association of Sleep Medicine criteria [15]. The scor-ing of total sleep time; and the duration of the sleep stages 1, 2, and3, slow-wave sleep (SWS), and REM sleep; as well as the number ofarousals, which were classified corresponding to the guidelines ofthe American Sleep Disorders Association [24]; and awakeningswere manually performed by a qualified sleep technician. To repre-sent the duration and thereby potential sleep disturbing character-istic of the arousals, extended arousals were calculated. Hereby, wedefined an extended arousal as an arousal lasting 30 s or longer.Saliva samples were collected each morning in 15-min intervalsstarting directly at wakeup time (6:45 am), and then at 15, 30,and 45 min after awakening using a cylindrical shaped inert poly-mer swab during 60 s of chewing. The saliva was collected by
Fig. 1. The LAF distribution over time (60 min) for the exposure sounds used. The soundrepresentative sequences of respiratory sounds, alarms, closing doors, and activity soundaspects but reduced with LAeq 7-dB ICU (left) and one with modified sound quality (ICU
chewing on a Salivette� cotton swab (Sarstedt Ltd., UK) that thesubject chewed for 3 min, after which the subject placed the Sali-vette� cotton swab in a sterile plastic tube. The samples were thenfrozen at �70 �C until analyzed. Saliva was recovered from the cot-ton dental swab by centrifugation at 1000 g and cortisol was deter-mined by the commercial high sensitivity enzyme immunoassaykit ELISA (Salimetrics�), with interassay coefficient of variation at3.75–6.41% and intra-assay coefficient of variation at 3.35–3.65%.Saliva samples for cortisol analysis were taken every morning;samples from the adaptation night were only taken for the purposeof practicing the procedure with the participants and thereforewere not analyzed.
2.5. Questionnaires
Subjective estimation of sleep and sleep disturbance was as-sessed by a morning questionnaire. The questionnaire comprisedquestions that were answered on a 5-grade verbal ratings of sleepquality during the previous night (very good to very bad), level ofalertness right now (very alert to very tired), level of irritation rightnow (very glad to very irritated), and difficulties with falling asleepnight or sleep onset (not at all to very much). Questions on sleeponset, sleep quality, perceived depth of sleep, and frequency ofwaking up (never to often) were posed using 11-grade numericscales. Questions were then posed on noise and annoyance or dis-turbance using a 5-grade verbal scale (not at all to extremely) aswell as if noise interfered with the sleep, woke them up, or madeit difficult to fall asleep once awoken. The morning questionnairewas answered each morning within 15 min after wakeup time. Inthe analyses we formed four indexes of questions tapping on thesame dimensions by averaging the individual items (after trans-forming the 11-grade scales into 5-point scales). The four indexeswere sleep quality (four items: morning tiredness, morning alert-ness, and two slightly different questions on general sleep quality);sleep onset (two items: difficulties falling asleep on a 5-point scaleand a polarized 11-point scale from easy to difficult to fall asleep);perceived depth of sleep (two items: sleep depth and frequency ofwaking up); and noise interference (four items: noise annoyanceduring the night, noise causing bad sleep, noise causing awaken-ings, and noise interfering with falling asleep after awakenings).The internal reliabilities for the 12 times the indexes were used(four indexes after three exposure modes) were >.7 (Cronbach a)for eight of the times and for two of the times close to .7 (.65
s were based on recordings in an intensive care unit (ICU) and modeled to includes. The sounds were played back in two modes: one with the original sound quality_peak reduced) equally reduced with LAeq7 dB (right).

Table 3Sleep stage duration, number of arousals, and number of awakenings (measured with polysomnography), perception of sleep, and current stress/energy and mood (self-reportedin the morning) for the three modes of noise exposure, including reference night, intensive care unit, and intensive care unit_peak reduced mode.
REF mean (SD) ICU_peak reduced mean (SD) ICU mean (SD)
Polysomnography (n = 15)N1, min 40.3 (7.3) 44.1 (9.8) 44.0 (9.2)N2, min 186.8 (18.8) 204.7 (20.9)* 197.3 (28.8)N3, min 68.4 (23.0) 51.9 (17.4)* 52.0 (25.9)*
REM, min 90.6 (23.1) 74.0 (17.7)* 83.4 (19.1)Arousals, n 76.2 (22.6) 79.9 (18.6) 88.3 (28.6)Extended arousals, n 7.9 (6.6) 10.1 (5.3) 11.3 (7.8)*
Awakenings, n 14.9 (6.6) 20.1 (8.4)* 19.5 (9.0)*
Saliva cortisol (n = 17)AUCG 36.0 (7.6) 36.3 (10.1) 33.5 (9.4)
Self-reported (n = 17)Sleep quality index (good ? bad) 2.2 (0.4) 2.9 (0.8)* 2.8 (0.9)*
Sleep onset index (easy ? difficult) 2.4 (1.1) 2.8 (1.3) 2.3 (0.9)Depth of sleep index (deep ? shallow) 2.9 (0.8) 3.6 (0.9)* 3.2 (0.8)Noise interference index (low ? high) 1.2 (0.4) 3.0 (1.0)* 3.0 (1.1)*
Onset, min 25.0 (18.8) 21.4 (15.4) 22.6 (21.2)Wakeups, n 2.2 (1.6) 4.1 (3.3)* 3.5 (2.8)
Abbreviations: REF, reference night; ICU, intensive care unit; SD, standard deviation; min, minutes; REM, rapid eye movement sleep; AUCG, area under the curve in relation tothe ground.* Statistically significantly difference from REF; P < .05 (paired t tests used as post hoc tests when the results from the linear model were statistically significant).
K. Persson Waye et al. / Sleep Medicine 14 (2013) 1334–1340 1337
and .67, respectively). The internal reliability was high except fortwo occasions: perceived sleep onset the morning after exposureto the ICU_peak reduced sound, which had a Cronbach a of .6;and sleep quality after the reference (REF) night of .5.
2.6. Statistical analyses
Data were analyzed using SPSS 19. Cortisol concentrations wereanalyzed as the square root of the measurements to better normal-ize initially skewed distributions. The integral of the area undercurve sample 1–4 were calculated in relation to the ground (AUCG)[25,26]. The three exposure modes were compared using a generallinear model of repeated measures for results of the polysomno-graphic and self-reported measurements.
An interaction term comprising the studied variable and the or-der of which the sound had been presented (sequence A or B) wasincluded to test possible order effects. If the order effect was signif-icant, it was considered in the analysis. In case of significant overalleffects, post hoc tests were performed with paired t tests. Relation-ships between variables were tested using Pearson product mo-ment correlation coefficients. All tests were two sided and a Pvalue of <.05 was considered significant.
Fig. 2. Number of wakeups (measured with polysomnography) for the 15 partic-ipants during the control night and the two exposure nights.
3. Results
3.1. Sleep stages duration, arousals, and awakenings
There was a significant main effect of exposure for duration ofN3 and REM sleep, with a shorter duration during nights withICU sounds compared to the REF night (N3, F[2,26] = 5.41,P = .011 and REM sleep, F[2,28] = 4.87, P = .015; Table 3). Post hoctests showed that N3 sleep was significantly reduced during eachof the ICU sounds compared to REF night, though REM sleep wasonly significantly shorter for ICU_peak reduced modes comparedto REF night. There also was a tendency for the duration of N2 sleepto be longer in the ICU sounds compared to REF night(F[2,28] = 3.30; P = .052). No differences in duration of sleep stageswere found for the two modes of ICU sounds. The numbers of reg-istered arousals and awakenings were higher during the exposednight than during the REF night. The increase in arousals did notreach the significant level; however, we observed a significant ef-
fect (F[2,28] = 4.71; P = .017) for the number of awakenings. Posthoc testing showed a significant difference between both ICUsounds and REF night. No significant difference was found betweenthe two modes of ICU sounds (Fig. 2).
Interestingly, we also observed a significant linear effect be-tween the nocturnal sound level and the number of extendedarousals (F[1,12] = 5.06; P = .044; Fig. 3), indicating that the num-ber of extended arousals increased with greater or more frequentmaximal sound levels. Post hoc testing showed a significant differ-ence between ICU sound and REF night.
3.2. Self-reported sleep indexes, awakenings, stress or energy, andmood
The participants reported worse sleep quality after the nightwith exposure to the ICU sound and after exposure to the ICU_peakreduced sound (F[2,32] = 6.04; P = .006; Table 3) in comparison tothe REF night. No differences were found for perceived sleep onset,neither as reported on a ranking scale nor when reported in min-utes, which is in line with the study design in which the playbackof the sounds started one hour after bedtime. The participants de-scribed their sleep as more shallow after the exposed night thanafter the REF night (F[2,30] = 4.92; P = .014), with the difference be-tween REF night and ICU_peak reduced mode being statisticallysignificant. Noise interference was higher in both exposure nights

Fig. 3. Average number of extended arousals per night. A significant increase ofextended arousals with increasing sound characteristics was observed (P = .02).Note: Error bars represent the 95% confidence interval.
1338 K. Persson Waye et al. / Sleep Medicine 14 (2013) 1334–1340
in comparison to the REF night (F[2,32] = 28.35; P < .001). Themean number of perceived awakenings was higher during thetwo nights of exposure than during the REF night (F[2,30] = 5.99;P = .006), with the ICU_peak reduced mode being significantly dif-ferent from REF night. No differences between the two modes ofICU exposures were found for any of the indexes.
3.3. Relationships between differences in self-reported andphysiologically measured sleep
Variables that were found to be significantly statistically differ-ent for the REF night and any of the ICU exposure nights were fur-ther explored. The most consistent relationship was foundbetween sleep quality and the sleep structures in N3 sleep, REMsleep, and awakenings, though they all missed the level of signifi-cance. We often found that the median decrease of 8% (0.4 points)on the 5-point sleep quality scale during exposure to the ICU soundin comparison to the REF night tended to be associated with areduction of N3 sleep with 23.5 min (r = �.50; P = .058) and REMsleep with 10.5 min (r = �.50; P = .057) and an increase of fourawakenings (r = .47; P = .077). Apart from this tendency only sleepdepth was found to be significantly associated with awakening,with the median difference of 0.2 being associated with an increaseof four awakenings (r = .54; P = .037). No relationships betweenpolysomnographic and self-reported variables were found for thedifferences between ICU_peak reduced mode and REF night.
3.4. Saliva cortisol
Data from the saliva tests of cortisol concentration showed anormal peak 30 min after morning wakeup. Although the levelsof the AUCG were somewhat lower after nights with ICU soundsas opposed to REF night (Table 3), it did not reach significance.
When exploring the saliva cortisol in relation to objective andsubjective sleep, morning cortisol response was not found to besignificantly related to any specific sleep stage during the nights.However, low saliva cortisol levels were associated with lower re-ported sleep quality and increased tiredness. Specifically signifi-cant associations were found between saliva cortisol levels andsleep quality index (r = �.49; P = .045) and sleep-onset index(r = �.48; P = .051). Accordingly participants also felt less energeticin the morning, with a lower cortisol level on awakening (r = �.54;
P = .026). Interestingly, these associations were only found to besignificant after nights with ICU sounds.
3.5. Order effects
An interaction effect was found between the sequence in whichthe participants were exposed to the ICU sounds and duration ofN3 sleep and in the number of extended arousals (N3 sleep:F[2,26] = 3.89, P = .033; extended arousals: F[2,24] = 4.15,P = .028). If the ICU sounds exposure was preceded by the REFnight, the participants had less deep sleep and more extendedarousals compared to when it was preceded by the other ICU soundexposure. A similar interaction effect pointing in the same direc-tion was found for two of the self-reported variables, such as per-ceived sleep depth (F[2,30] = 8.02; P = .002) and perceived numberof awakenings (F[2,30] = 5.51; P = .009).
4. Discussion
In our study we examined the potential benefit for patients’sleep and recuperation caused by a selective attenuation of themaximal signals in the ICU environment. We especially focusedon noise events that are frequent and have a realistic possibilityto be reduced in ICUs, i.e., a level decrease of the loudest alarmsand the elimination of sounds from closing doors. Both of the ICUsound conditions significantly impaired the restorative functionsof sleep, as seen in lower sleep quality reduced duration of stagesN3 sleep and REM sleep and an increased number of extendedarousals and awakenings. These findings were established bothby PSG and by participants’ self-reports. There was a reduction ofN3 sleep by 16.5 min, which indicates that SWS was reduced byas much as 24% during the ICU sound conditions. Furthermore,the increase of awakenings by 33% in the ICU noise conditionsand the increase of the number of extended arousals shows thatsleep in noise conditions recorded at the ICU was less restorativeand more fragmented compared to the quiet reference condition.Although there is no consensus on the relative functions of the var-ious sleep stages, N3 sleep generally is considered to be importantfor physical restoration [27–29] and memory [30] and accordinglySWS tends to be prioritized after sleep deprivation [31], thoughREM sleep also is believed to be important for cognition [32]. Onthe other hand, awakenings and arousals can accelerate the heartrate, and significant elevations of up to 10 beats per minute havebeen found in relation to acoustic events [33–35]. Because dis-turbed sleep in other studies has been linked to ventriculararrhythmias [36], blood pressure increase [37], and coronary heartdisease [38], we concluded that the increased number of awaken-ings and extended arousals found in the ICU noise conditions mayimpair the recuperation process needed for patients under treat-ment in ICUs. Furthermore, the order effect indicated that partici-pants needed to regain sleep after exposure nights; however, it isimportant to note that the sample size was relatively low.
The sounds and levels used in our study were not exceptionallyhigh, as the equivalent levels used in our study were reduced by7 dB from the recorded levels in an actual ICU environment. Thislowering was done for healthy participants to be able to take partin the study and to be able to sleep. The modifications of the ICU_-peak reduced sound made resulted in a reduction of A-weightedmaximal sound levels from 64 to 56 dB. This change must be con-sidered as a substantial reduction, as Ryherd et al. [18] found thatmaximal A-weighted levels exceeded 80 dB during the night in anearlier study and that 60 dBAFmax was being exceeded 50% of thetime during a normal night in the ICU. This substantial thoughrather realistic reduction did not seem to be enough to have a clearpositive effect on sleep, as no differences in subjective response or

K. Persson Waye et al. / Sleep Medicine 14 (2013) 1334–1340 1339
sleep stages to the two modes of sounds (ICU vs ICU_peak reduced)were found. The World Health Organization recommends thataveraged sound pressure levels measured over time should not ex-ceed 30 dBA in patient ward rooms or 35 dBA in patient treatmentand observation rooms [19]. However, no measured hospital levelspublished after the 1960s complied to those levels [16]. From theliterature on road traffic noise, it can be determined that sleepmay be disturbed at levels above 45 dBAFmax [39]. Basner et al.[40] have even reported enhanced awakening probabilities dueto aircraft noise at levels as low as 33 dBASmax. Much less is knownof sleep disturbance due to alarms, doors closing, and other activ-ities in a hospital ward, and the studies performed to date areinconclusive. A recent elaborate experimental study [41] evaluatedthe probability of arousals from various hospital sounds byincreasing the noise levels of short-term noise signals until subjectawoke or the noise reached 70 dBAFmax.
The arousal probability was more than 80% for electronicsounds and conversation from 40 dBAFmax, indicating that thesesounds may be even more sleep disturbing than previously foundfor road traffic noise. Hence it can be more clearly understood thatthe ICU_peak reduced sound in our study also negatively affectedsleep and sleep structure, as it comprised 18 events per hour thatexceeded 50 dB LAFmax. In contrast, a study [23] of 12 participantswhich took place in a refurbished former surgical ward, found thatthe installation of sound-absorptive ceiling tiles significantly re-duced the number of arousals during sleep, even though the soundlevels were only marginally attenuated by 1–2 dB. The noise levelsafter the installation of ceiling tiles ranged from 29 to 57 dBAFmax,derived from both continuous and impulsive sources, such asdropped plates, traffic noise, fan noise, machine noise, doors clos-ing, and radios. As previously has been observed for transportationnoise, awakening responses for ICU sounds seem to not only be re-lated to the actual peaks but also to the relation between the peaksand the background sound level. In 2005 Stanchina et al. [14] ex-posed five participants to recorded sounds from an ICU with andwithout white noise. The average A-weighted level of the ICU noisewas only 57.9 dB, and the combined ICU and white noise averaged61.1 dBA. In spite of the average sound level increasing with 3 dB,the authors found that the addition of the white noise lowered thenumber of sleep arousals caused by ICU noise. It should be notedthat Stanchina et al. [14] found most of their changes in arousalsfor noise events with a peak to noise level of 17 dB, which is con-siderably higher than the change that was obtained between ICUand ICU_peak reduced being in the order of 8 dB.
It may be imprudent to report a definite conclusion of lack ofimprovement in sleep with the peak reduced sound, as there weresome indications of an effect of the ICU_peak reduced sound seenin the differences in strengths of relationships between subjectivesleep and sleep structures and the increasing number of extendedarousals between the conditions. Further indications were given inthe relationships between the saliva cortisol response and theoverall sleep quality and sleep onset indexes, which were only ob-served after nights with ICU sound. Earlier studies on the awaken-ing cortisol response have confirmed that a decreased level ofsaliva cortisol response on morning awakening is associated withtiredness in the morning [42] and decreased subjective sleepamong patients with insomnia [43]. Results from studies in whichthe effect of noise-induced sleep disturbance have been investi-gated, have though shown inconsistent results [40,44–47]. The factthat no one has been able to establish a connection between distur-bance of specific sleep structure and a reduced morning awakeningsaliva cortisol response [48] may represent a complex relationshipbetween the circadian pattern of cortisol and sleep disturbanceincluding mechanisms that are still not fully understood.
We must stress that the results were obtained from a smallsample, and the high effect size suggests that significance level
was not always reached, due to the lack of power. Further thereis no correct or simple way to generalize healthy participants topatients being under medical care with the influence of medica-tion. As we stated in the introduction, noise is only one of severalfactors that impaired sleep under ICU care; nevertheless, our studyprovides clear indications to the importance of making substantialreductions of the sound environment at ICUs to combat unneces-sary sleep disturbance, prolonged recovery, and hospital stay. Al-beit weak, out study does give implications that minor andpractically feasible changes to the sound environment also maybe beneficial for health and recovery. As previously stated, an envi-ronment supporting restorative sleep is of highest importance forpatients in their recovery process. Further studies are clearlyneeded to elucidate health-supporting sound environments inthe hospitals.
Funding sources
Funding was provided by regional university hospital funding(ALFGBG – 145501).
Conflict of interest
The ICMJE Uniform Disclosure Form for Potential Conflicts ofInterest associated with this article can be viewed by clicking onthe following link: http://dx.doi.org/10.1016/j.sleep.2013.07.011.
Acknowledgments
We thank the colleagues from Division of Flight Physiology fortheir support of this work, especially Stefan Schmitt, Norbert Luks,and Gernot Plath. We also would like to thank the colleagues atOccupational and Environmental Medicine, Richard Walleniusand Agneta Agge, for their analytical work and assistance withthe test procedure and Mikael Ögren for the sound exposuremodifications.
References
[1] Freedman NS, Kotzer N, Schwab RJ. Patient perception of sleep quality andetiology of sleep disruption in the intensive care unit. Am J Respir Crit CareMed 1999;159(4 pt. 1):1155–62.
[2] Simini B. Patient’s perceptions of intensive care. Lancet 1999;354:571–2.[3] Ekstedt M, Åkerstedt T, Söderström M. Microarousals during sleep are
associated with increased levels of lipids, cortisol and blood pressure.Psychosom Med 2004;66:925–32.
[4] Spiegel K, Knutson K, Leproult R, Tasali E, Van Vauter E. Sleep low: a novel riskfactor for insulin resistance and Type 2 diabetes. J Appl Physiol2005;99:2008–19.
[5] Spiegel K, Leproult R, Van Cauter E. Impact of sleep debt on metabolic andendocrine function. Lancet 1999;354:1435–9.
[6] Spiegel K, Sheridan J, Van Cauter E. Effects of sleep deprivation on response toimmunization. JAMA 2002;288:1471–2.
[7] Ozturk L, Pelin Z, Karadeniz D, Kaynak H, Cakar L, Gozukirmizi E. Effects of48 hours sleep deprivation on human immune profile. Sleep Res Online1999;2:107–11.
[8] Boyko Y, Ording H, Jennum P. Sleep disturbances in critically ill patients in ICU:how much do we know? Acta Anaesthesiol Scand 2012;56:950–8.
[9] Hardin K. Sleep in the ICU. Chest 2009;136:284–94.[10] Freedman NS, Gazendam J, Levan L, Pack AI, Schwab RJ. Abnormal sleep/wake
cycles and the effect of environmental noise on sleep disruption in theintensive care unit. Am J Respir Crit Care Med 2001;163:451–7.
[11] Gabor JY, Cooper AB, Crombach SA, Lee B, Kadikar N, Bettger HE, et al.Contribution of the intensive care unit environment to sleep disruption inmechanically ventilated patients and healthy subjects. Am J Respir Crit CareMed 2003;167:708–15.
[12] Carley DW, Applebaum R, Basner RC, Onal E, Lopata M. Respiratory and arousalresponses to acoustic stimulation. Chest 1997;112:1567–71.
[13] Parthasarathy S, Tobin MJ. Sleep in the intensive care unit. Intensive Care Med2004;30:197–206 [published online ahead of print October 16, 2003].

1340 K. Persson Waye et al. / Sleep Medicine 14 (2013) 1334–1340
[14] Stanchina ML, Abu-Hijleh M, Chaudhry BK, Carlisle CC, Millman RP. Theinfluence of white noise on sleep in subjects exposed to ICU noise. Sleep Med2005;6:423–8.
[15] Iber C, Ancoli-Israel S, Chesson A, Quan S. The AASM manual for the scoring ofsleep and associated events. Rules, terminology and technical specifications.Am Acad Sleep Med 2007.
[16] Busch-Vishniac IJ, West JE, Barnhill C, Hunter T, Orellana D, Chivukula R. Noiselevels in Johns Hopkins Hospital. J Acoust Soc Am 2005;118:3629–45.
[17] Meyer TJ, Eveloff SE, Bauer MS, Schwartz WA, Hill NS, Millman RP. Adverseenvironmental conditions in the respiratory and medical ICU settings. Chest1994;105:1211–6.
[18] Ryherd E, Persson Waye K, Ljungkvist L. Characterizing noise and perceivedwork environment in a neurological intensive care unit. J Acoust Soc Am2008;123:747–56.
[19] Berglund B, Lindvall T, Schwela DH. Guidelines for communitynoise. Geneva: World Health Organisation [WHO]; 1999.
[20] Hsu T, Ryherd E, Persson Waye K, Ackerman J. Noise pollution in hospitals:impact on patients. J Clin Outcome Manage 2012;19:1–10.
[21] Folkow B. Mental stress and its importance for cardiovascular disorders;physiological aspects, ‘‘from-mice-to-man’’. Scand Cardiovasc J2001;35:163–72.
[22] Di Nisi J, Muzet A, Ehrhart J, Libert JP. Comparison of cardiovascular responsesto noise during waking and sleeping in humans. Sleep 1990;13:108–20.
[23] Berg S. Impact of reduced reverberation time on sound-induced arousalsduring sleep. Sleep 2001;24:289–92.
[24] Bonnet MH, Carley DW, Carskadon M, Easton P, Guilleminault C, Harper R. EEGarousals: scoring rules and examples. A preliminary report from the SleepDisorders Atlas Task Force of the American Sleep Disorders Association, 1992.
[25] Fekedulegn DB, Andrew ME, Burchfiel CM, Violanti JM, Hartley TA, Charles LE,et al. Area under the curve and other summary indicators of repeated wakingcortisol measurements. Psychosom Med 2007;69:651–9 [published onlineahead of print August 31, 2007].
[26] Pruessner JC, Kirschbaum C, Meinlschmid G, Hellhammer DH. Two formulasfor computation of the area under the curve represent measures of totalhormone concentration versus time-dependent change.Psychoneuroendocrinology 2003;28:916–31.
[27] Bonnet MH. Effect of sleep disruption on sleep, performance, and mood. Sleep1985;8:11–9.
[28] Borbely AA. A two process model of sleep regulation. Hum Neurobiol1982;1:195–204.
[29] Young JS, Bourgeois JA, Hilty DM, Hardin KA. Sleep in hospitalized medicalpatients, part 1: factors affecting sleep. J Hosp Med 2008;3:473–82.
[30] Diekelmann S, Wilhelm I, Born J. The whats and whens of sleep-dependentmemory consolidation. Sleep Med Rev 2009;13:309–21.
[31] Spiegel R, Köberle S, Allen S. Significance of slow wave sleep: considerationsfrom a clinical viewpoint. Sleep 1986;9:66–79.
[32] Walker MP, Liston C, Hobson JA, Stickgold R. Cognitive flexibility across thesleep–wake cycle: REM-sleep enhancement of anagram problem solving. BrainRes Cogn Brain Res 2002;14:317–24.
[33] Basner M, Griefahn B, Berg M. Aircraft noise effects on sleep: mechanisms,mitigation and research needs. Noise Health 2010;12:95–109.
[34] Basner M, Fomberstein KM, Razavi FM, Banks S, William JH, Rosa RR, et al.American time use survey: sleep time and its relationship to waking activities.Sleep 2007;30:1085–95.
[35] Smith M, Croy I, Ögren M, Persson Waye K. On the influence of freight trains onhumans: a laboratory investigation of the impact of nocturnal low frequencyvibration and noise on sleep and heart rate. PLoS One 2013;8:e55829[published online ahead of print February 7, 2013].
[36] Conn V. Patient reaction to noise in CCU. University of Missouri; 1981.[37] Sonnenberg A, Donga M, Erckenbrecht JF, Wienbeck M. The effect of mental
stress induced by noise on gastric acid secretion and mucosal blood flow.Scand J Gastroenterol Suppl 1984;89:45–8.
[38] Hoevenaar-Blom MP, Spijkerman AM, Kromhout D, van den Berg JF,Verschuren WM. Sleep duration and sleep quality in relation to 12-yearcardiovascular disease incidence: the MORGEN study. Sleep 2011;34:1487–92.
[39] Öhrström E. Effects of low levels of road traffic noise during the night: alaboratory study on number of events, maximum noise levels and sensitivity. JSound Vib 1995;179:603–15.
[40] Basner M, Samel A, Isermann U. Aircraft noise effects on sleep: application ofthe results of a large polysomnographic field study. Journal Acoust Soc Am2006;119(5 pt. 1):2772–84.
[41] Buxton OM, Ellenbogen JM, Wang W, Carballeira A, O’Connor S, Cooper D, et al.Sleep disruption due to hospital noises: a prospective evaluation. Ann InternMed 2012;157:170–9.
[42] Kumari M, Badrick E, Chandola T, Adam EK, Stafford M, Marmot MG, et al.Cortisol secretion and fatigue: associations in a community based cohort.Psychoneuroendocrinology 2009;34:1476–85.
[43] Backhaus J, Junghanns K, Hohagen F. Sleep disturbances are correlated withdecreased morning awakening salivary cortisol. Psychoneuroendocrinology2004;29:1184–91.
[44] Persson Waye K, Clow A, Edwards S, Hucklebridge F, Rylander R. Effects ofnighttime low frequency noise on the cortisol response to awakening andsubjective sleep quality. Life Sci 2003;72:863–75.
[45] Persson Waye K, Agge A, Clow A, Hucklebridge F. Cortisol response andsubjective sleep disturbance after low-frequency noise exposure. J Sound Vib2004;277:453–7.
[46] Griefahn B, Robens S. Experimental studies on the effects of nocturnal noise oncortisol awakening response. Noise Health 2010;12:129–36.
[47] Michaud DS, Miller SM, Ferrarotto C, Konkle AT, Keith SE, Campbell KB. Wakinglevels of salivary biomarkers are altered following sleep in a lab with nofurther increase associated with simulated night-time noise exposure. NoiseHealth 2006;8:30–9.
[48] Steiger A. Sleep and the hypothalamo–pituitary–adrenocortical system. SleepMed Rev 2002;6:125–38.
















![Metabolic consequences of sleep and sleep loss · problems, chronic sleep deprivation is increasingly common in our hectic modern society [I ,2]. Societal changes, such as an increase](https://img.pdfslide.us/doc/110x75/5fd2be10fcb79f7b3c1a6018/metabolic-consequences-of-sleep-and-sleep-loss-problems-chronic-sleep-deprivation.jpg)