Embed Size (px)
Citation preview
Improvement Methodology IncreasesGuideline Recommended BloodCultures in Children With PneumoniaEileen Murtagh Kurowski, MD, MSa,b, Samir S. Shah, MD, MSCEb,c,d, Joanna Thomson, MD, MPHb,c, Angela Statile, MD, MEdb,c,Brieanne Sheehan, MGSc, Srikant Iyer, MD, MPHa,b,e, Christine White, MD, MATb,c, Lilliam Ambroggio, PhD, MPHb,c
abstract BACKGROUND AND OBJECTIVE: A national evidence-based guideline for themanagement of community-acquired pneumonia (CAP) in childrenrecommends blood cultures for patients admitted with moderate to severeillness. Our primary aim was to increase ordering of blood cultures forchildren hospitalized with CAP from 53% to 90% in 6 months. The secondaryaim was to evaluate the effect of obtaining blood cultures on length of stay(LOS).
METHODS: At a tertiary children’s hospital, interventions to increase bloodcultures focused on 3 key drivers and were tested separately in the emergencydepartment and inpatient units by using multiple plan-do-study-act cycles.The impact of the interventions was tracked over time on run charts. Theassociation of ordering blood cultures and LOS was estimated by using linearregression models.
RESULTS: Within 6 months, the percentage of patients admitted with CAP whohad blood cultures ordered increased from 53% to 100%. This change hasbeen sustained for 12 months. Overall, 239 (79%) of the 303 included patientshad a blood culture ordered; of these, 6 (2.5%) were positive. Patients whohad a blood culture did not have an increased LOS compared with thosewithout a blood culture.
CONCLUSIONS: Quality improvement methods were used to increase adherence toevidence-based national guidelines for performing blood cultures on childrenhospitalized with CAP; LOS did not increase. These results support obtainingblood cultures on all patients admitted with CAP without negative effects onLOS in a setting with a reliably low false-positive blood culture rate.
Community-acquired pneumonia (CAP)is a common cause of hospitalization inchildren. Blood cultures are the mostwidely available diagnostic tool for theidentification of bacterial pathogens inCAP. In 2011, the Pediatric InfectiousDiseases Society (PIDS) and theInfectious Diseases Society of America(IDSA) published a guideline for themanagement of CAP in children olderthan 3 months. This guidelinerecommended that blood cultures beobtained in all children requiringhospitalization for moderate to severe
presumed bacterial CAP, and forpatients whose symptoms progress orwho clinically deteriorate afterinitiation of antibiotic therapy.1 Despitethe consensus recommendation by thePIDS/IDSA, previous work hasdemonstrated variation in bloodculture performance in childrenhospitalized with CAP.2
Though bacteremia is relativelyuncommon,3–6 the PIDS/IDSA guidelinesrecommend blood cultures becauseetiology (ie, bacterial versus viral)
Divisions of aEmergency Medicine, cHospital Medicine, anddInfectious Diseases, Cincinnati Children’s Hospital MedicalCenter, Cincinnati, Ohio; bDepartment of Pediatrics, Collegeof Medicine, University of Cincinnati, Cincinnati, Ohio; andeJames M. Anderson Center for Health Systems Excellence,Cincinnati, Ohio
Dr Murtagh Kurowski participated in the design of thestudy, developed the data collection criteria, carriedout the statistical analysis, performed chart reviews,designed and executed interventions, and drafted theinitial manuscript; Dr Shah participated in the designof the study, participated in the design of theinterventions, developed the data collection criteria,and reviewed all drafts of the manuscript; DrsThomson and Statile participated in the design of thestudy, performed chart reviews, designed andexecuted interventions, and reviewed all drafts of themanuscript; Ms Sheehan participated in the design ofthe study, performed chart reviews, carried outstatistical analysis, and reviewed all drafts of themanuscript; Dr Iyer participated in the design of thestudy, participated in the design of the interventions,supervised the statistical analysis, and reviewed alldrafts of the manuscript; Dr White participated in thedesign of the study, participated in the design of theinterventions, developed the data collection criteria,and reviewed all drafts of the manuscript; DrAmbroggio participated in the design of the study,developed the data collection criteria, performedchart reviews, carried out the statistical analysis,executed interventions, and reviewed all drafts of themanuscript; and all authors approved the finalmanuscript for submission.
www.pediatrics.org/cgi/doi/10.1542/peds.2014-2077
DOI: 10.1542/peds.2014-2077
Accepted for publication Dec 1, 2014
QUALITY REPORT PEDIATRICS Volume 135, number 4, April 2015 by guest on June 20, 2018www.aappublications.org/newsDownloaded from

cannot be readily discerned fromclinical presentation or radiographicfindings.1 The epidemiology of CAPhas changed with an increase in theprevalence of CAP-associatedcomplications, particularly amongyoung children.7 Children whodevelop CAP-associatedcomplications may initially presentwith uncomplicated CAP.5 In thesepatients, a blood culture obtainedbefore antibiotic initiation may be theonly opportunity to identify thecausative pathogen, because pleuraldrainage may not always benecessary and pleural fluid culturesare frequently negative.8,9
Guidelines at our institution before thePIDS/IDSA publication recommendedobtaining blood cultures only forhospitalized patients with severe,resistant, or “other unusual forms ofCAP.”10 This local guidelineemphasized the limited utility of bloodcultures when antibiotics wereadministered before obtaining thespecimen. At our institution, beforethe national guideline publication,blood cultures were obtained in only57.7% of hospitalized patients witha bacteremia rate of ∼6.3% anda “false-positive”/contamination rateof 1.3%.5 To standardize management,we assembled a multidisciplinaryteam to increase the percentage ofpatients admitted with CAP who hada blood culture obtained within 24hours of admission from 53% to 90%within 6 months. A secondary aimexamined the effect of obtaining more
blood cultures on length of stay (LOS),given concerns reported in theliterature that increasing the numberof blood cultures will lead to increasedLOS.3,11–14
METHODS
Setting
Cincinnati Children’s Hospital MedicalCenter (CCHMC) is a free-standing,tertiary-care, academic medicalcenter with 523 inpatient beds. Thisstudy was not considered humansubjects research by the institutionalreview board.
Planning the Intervention
The improvement team consisted of 4pediatric hospital medicine (HM)physicians (Drs Shah, Thomson,Statile, and White), 2 pediatricemergency medicine (EM) physicians(Drs Murtagh Kurowski and Iyer), 2pediatric infectious diseasesphysicians (Drs Rebecca Brady andShah), a clinical epidemiologist (DrAmbroggio), and a research assistant(Ms Sheehan). Process maps werecreated to outline the currentprocesses for obtaining bloodcultures on patients admitted tohospital medicine (HM) from theCCHMC emergency department (ED)or from an outside medical facility(Fig 1). Providers were encouraged,when possible, to obtain the bloodculture before antibioticadministration; however, toencourage universal blood cultures,
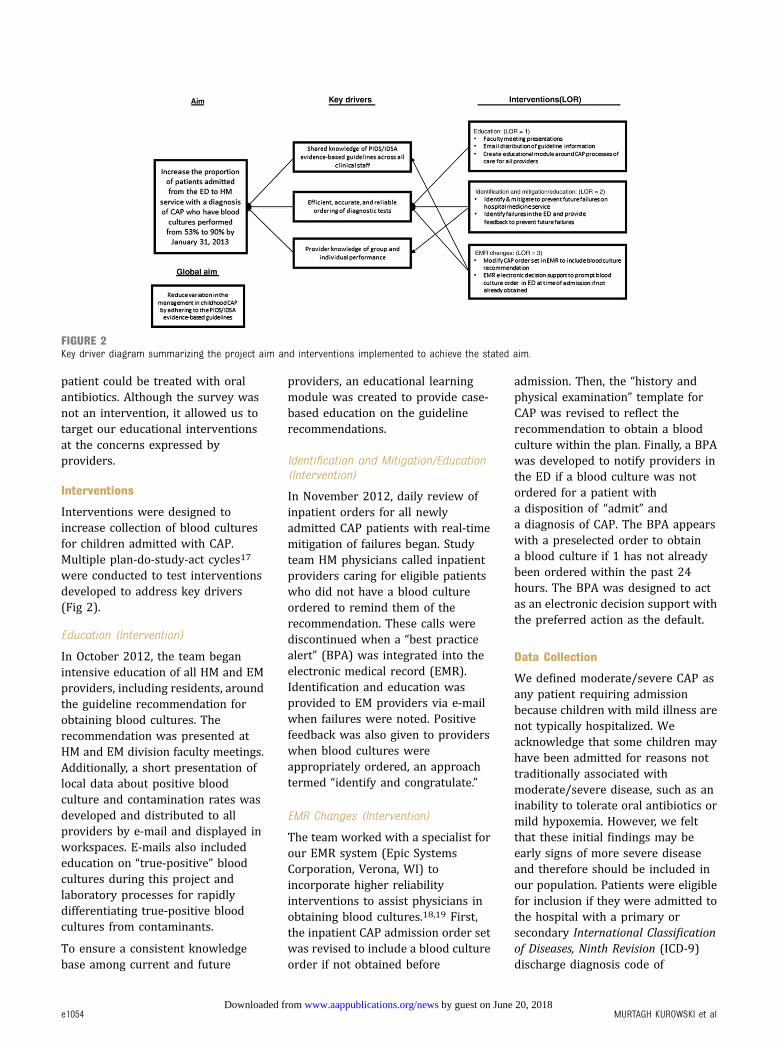
the timing of antibioticadministration was not included onprocess maps. The team used themaps to guide a failure mode andeffects analysis15,16 and constructeda key driver diagram to depict thetheory behind our aim (Fig 2). Keydrivers were as follows: sharedknowledge of the guideline across allproviders; efficient, reliable, andaccurate ordering of diagnostic tests;and provider knowledge of group andindividual performance.
Before designing interventions, weconducted a survey to identify howproviders decide when to order bloodcultures for patients admitted withCAP. This survey comprised 3 clinicalscenarios used to elicit therespondent’s presumptive diagnosisand plan for testing (SupplementalMaterial). Additionally, the surveyincluded 2 questions that askedproviders to identify factors thatinfluenced their decision to obtain ornot obtain a blood culture in a patientadmitted with CAP. This paper surveywas anonymously administered toa random sample of practitionersincluding attending physicians,fellows, residents, and nursepractitioners. Surveys werecompleted by 39% of HM and 40% ofemergency medicine (EM) providers.The most common reasons for notobtaining a blood culture wererelated to the clinician: questioningthe applicability of the guideline totheir patient, perceiving a lowseverity of illness, or anticipating the
FIGURE 1Process map for pneumonia patients admitted from the ED. BCX, blood culture; PNA, pneumonia.
PEDIATRICS Volume 135, number 4, April 2015 e1053 by guest on June 20, 2018www.aappublications.org/newsDownloaded from
patient could be treated with oralantibiotics. Although the survey wasnot an intervention, it allowed us totarget our educational interventionsat the concerns expressed byproviders.
Interventions
Interventions were designed toincrease collection of blood culturesfor children admitted with CAP.Multiple plan-do-study-act cycles17
were conducted to test interventionsdeveloped to address key drivers(Fig 2).
Education (Intervention)
In October 2012, the team beganintensive education of all HM and EMproviders, including residents, aroundthe guideline recommendation forobtaining blood cultures. Therecommendation was presented atHM and EM division faculty meetings.Additionally, a short presentation oflocal data about positive bloodculture and contamination rates wasdeveloped and distributed to allproviders by e-mail and displayed inworkspaces. E-mails also includededucation on “true-positive” bloodcultures during this project andlaboratory processes for rapidlydifferentiating true-positive bloodcultures from contaminants.
To ensure a consistent knowledgebase among current and future
providers, an educational learningmodule was created to provide case-based education on the guidelinerecommendations.
Identification and Mitigation/Education(Intervention)
In November 2012, daily review ofinpatient orders for all newlyadmitted CAP patients with real-timemitigation of failures began. Studyteam HM physicians called inpatientproviders caring for eligible patientswho did not have a blood cultureordered to remind them of therecommendation. These calls werediscontinued when a “best practicealert” (BPA) was integrated into theelectronic medical record (EMR).Identification and education wasprovided to EM providers via e-mailwhen failures were noted. Positivefeedback was also given to providerswhen blood cultures wereappropriately ordered, an approachtermed “identify and congratulate.”
EMR Changes (Intervention)
The team worked with a specialist forour EMR system (Epic SystemsCorporation, Verona, WI) toincorporate higher reliabilityinterventions to assist physicians inobtaining blood cultures.18,19 First,the inpatient CAP admission order setwas revised to include a blood cultureorder if not obtained before
admission. Then, the “history andphysical examination” template forCAP was revised to reflect therecommendation to obtain a bloodculture within the plan. Finally, a BPAwas developed to notify providers inthe ED if a blood culture was notordered for a patient witha disposition of “admit” anda diagnosis of CAP. The BPA appearswith a preselected order to obtaina blood culture if 1 has not alreadybeen ordered within the past 24hours. The BPA was designed to actas an electronic decision support withthe preferred action as the default.
Data Collection
We defined moderate/severe CAP asany patient requiring admissionbecause children with mild illness arenot typically hospitalized. Weacknowledge that some children mayhave been admitted for reasons nottraditionally associated withmoderate/severe disease, such as aninability to tolerate oral antibiotics ormild hypoxemia. However, we feltthat these initial findings may beearly signs of more severe diseaseand therefore should be included inour population. Patients were eligiblefor inclusion if they were admitted tothe hospital with a primary orsecondary International Classificationof Diseases, Ninth Revision (ICD-9)discharge diagnosis code of
FIGURE 2Key driver diagram summarizing the project aim and interventions implemented to achieve the stated aim.
e1054 MURTAGH KUROWSKI et al by guest on June 20, 2018www.aappublications.org/newsDownloaded from

pneumonia (480.0-2, 480.8-9, 481,482.0, 482.30-2, 482.41-2, 482.83,482.89-90, 483.8, 484.3, 485, 486,and 487.0) or effusion/empyema(510.0, 510.9, 511.0-1, 511.8-9, and513).20 To avoid inclusion of patientswith suspected viral CAP in the studypopulation, patients who did notreceive antibiotics and patients witha primary diagnosis of asthma, viralCAP, or bronchiolitis were excluded.
Success was defined as orderinga blood culture, at CCHMC or anoutside medical facility, within24 hours of presentation to CCHMC.Although our preference was to haveblood cultures drawn beforeantibiotic administration, the timingof antibiotics relative to the collectionof the blood culture did not affect thedefinition of success, because theteam’s aim was to achieve universalblood cultures on all admittedpatients with CAP. To determinea baseline percentage of bloodcultures obtained, data of patientsadmitted with CAP between April andSeptember 2012 were retrospectivelycollected. Although the PIDS/IDSAguideline was published in August2011, our interventions did not beginuntil October 2012. During theintervention period, medical recordsof eligible patients were revieweddaily to ensure patient eligibility andto confirm a blood culture order.Reviewer consensus defined“success” or “failure.” Blood cultureresults were verified 5 days afterinitial collection. Run charts wereupdated weekly during theintervention period and continuallydisplayed in the ED offices. They werealso communicated every 1 to 2months at HM and EM staff meetings.Covariates collected from chartreview included the following: age,presence of a complex chroniccondition,21 Emergency SeverityIndex version 4 Triage Level,22 ICUtransfer, supplemental oxygen given,and complete blood cell (CBC) countor chest radiograph (CXR) performed.These characteristics were selecteda priori as clinically important factors
influencing the care of patients withCAP. LOS was defined in hours asdifference between admission anddischarge date and time.
Analysis
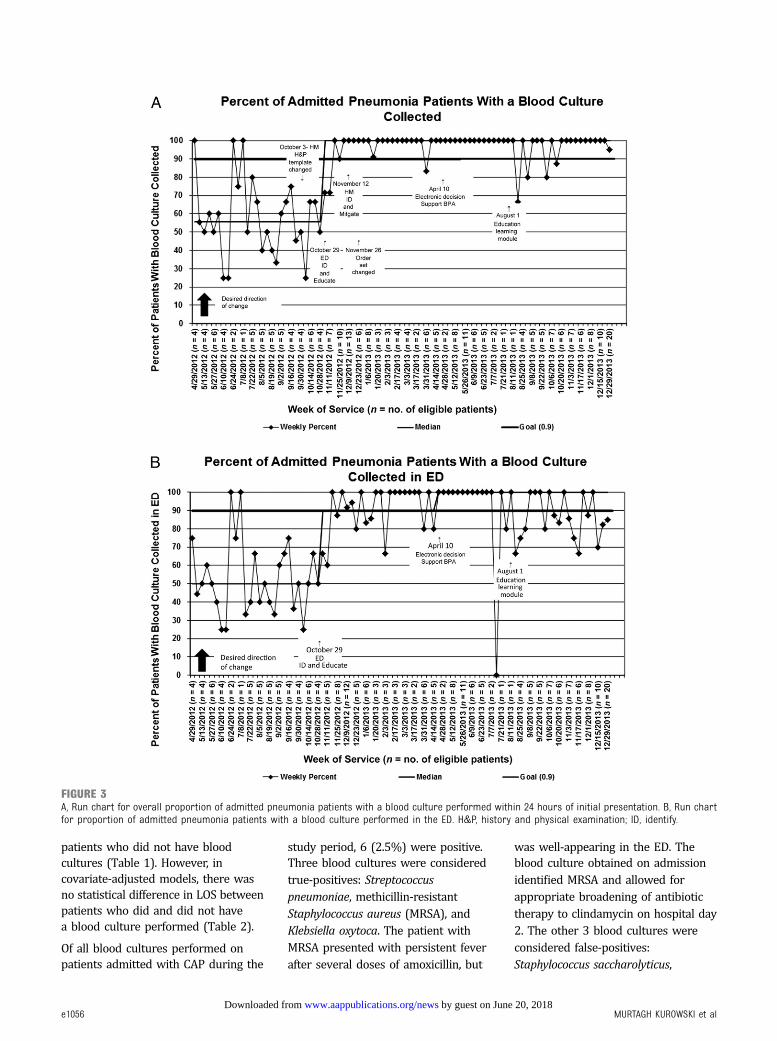
We constructed 2 run charts to trackthe impact of our interventions. Thefirst was an aggregate measure of allblood cultures ordered from either anoutside medical facility, the ED, or onthe inpatient units. The second runchart tracked only blood culturesordered in the ED to more effectivelyassess the impact of our interventionsin the ED setting, where most bloodcultures in our institution are ordered.
Continuous variables were described byusing medians and interquartile ranges(IQRs) and compared across groups byusing Wilcoxon rank-sum test givenpresence of outliers and nonnormaldistributions. Categorical variables weredescribed by counts and frequenciesand compared by using the x2 test.
Multivariable linear regressionanalysis was performed to assess theindependent effect of obtaininga blood culture on LOS whileadjusting for covariates. As LOS wasnonnormally distributed, welogarithmically transformed thesevalues. The resulting b-coefficientswere back-transformed to reflect thepercent change in LOS incurred
between subjects who did and thosewho did not have a blood cultureobtained.23 Covariates were includedin the final model because of theirclinical and biological relevance to theoutcome of LOS (eg, age, ICU transfer,and oxygen requirement) or if theyhad a P value , .1 on univariateanalysis (eg, CBC count performed).All analyses were performed with SASversion 9.3 (SAS Institute, Inc, Cary,NC), and P values , .05 wereconsidered statistically significant.
RESULTS
Blood cultures were performed in239 (79%) of 303 patients admittedto the HM service between April 2012and June 2013 with a diagnosis ofCAP. Median age was 3.0 years (IQR:1– 6) and 46% were boys. Only 3%(n = 10) of patients were transferredto the ICU (Table 1).
The median proportion of patientswho had blood cultures obtained atbaseline was 53% (Fig 3 A and B). Asa result of improvement efforts, themedian shifted to 100% by thebeginning of November 2012 and wassustained for 12 months.
In unadjusted analysis, patients whohad a blood culture performed weremore likely to have a CBC countperformed and a longer LOS than
TABLE 1 Patient Characteristics
Overall, n = 303 Blood Culture Ordered,n = 239 (79)
Blood Culture Not Ordered,n = 64 (21)
P
DemographicsAge, y 3.0 (1–6) 2.0 (1–6) 4.0 (1–6) .46Boy 140 (46) 115 (48) 25 (39) .20
Chronic complex conditions 4 (1.3) 3 (1.3) 1 (1.3) .999CXR ordered 102 (78) 55 (73) 47 (84) .15Emergency Severity Index2 125 (45) 99 (45) 26 (45) .983 129 (46) 102 (46) 27 (47)4 26 (9) 21 (81) 5 (9)
ICU transfer 10 (3) 7 (3) 3 (5) .48CBC count performed 169 (56) 157 (66) 12 (19) ,.01Oxygen requirementED requirement 135 (47) 110 (48) 25 (43) .50Inpatient requirement 299 (99) 237 (99) 62 (97) .20
OutcomesLOS, d 1.29 (0.88–2.13) 1.42 (0.92–2.42) 1.06 (0.75–1.81) ,.01
Categorical variables presented as n and percent. Continuous variables presented as median and IQR.
PEDIATRICS Volume 135, number 4, April 2015 e1055 by guest on June 20, 2018www.aappublications.org/newsDownloaded from
patients who did not have bloodcultures (Table 1). However, incovariate-adjusted models, there wasno statistical difference in LOS betweenpatients who did and did not havea blood culture performed (Table 2).
Of all blood cultures performed onpatients admitted with CAP during the
study period, 6 (2.5%) were positive.Three blood cultures were consideredtrue-positives: Streptococcuspneumoniae, methicillin-resistantStaphylococcus aureus (MRSA), andKlebsiella oxytoca. The patient withMRSA presented with persistent feverafter several doses of amoxicillin, but
was well-appearing in the ED. Theblood culture obtained on admissionidentified MRSA and allowed forappropriate broadening of antibiotictherapy to clindamycin on hospital day2. The other 3 blood cultures wereconsidered false-positives:Staphylococcus saccharolyticus,
FIGURE 3A, Run chart for overall proportion of admitted pneumonia patients with a blood culture performed within 24 hours of initial presentation. B, Run chartfor proportion of admitted pneumonia patients with a blood culture performed in the ED. H&P, history and physical examination; ID, identify.
e1056 MURTAGH KUROWSKI et al by guest on June 20, 2018www.aappublications.org/newsDownloaded from

coagulase-negative Staphylococcusspecies, and viridans groupStreptococcus. Only 2 of 3 patients witha true-positive blood culture hada pleural effusion identified on CXR,and only 1 of those was present onthe initial CXR. Because of thesmall number of cases, no risk factorsfor blood culture positivity wereidentified.
DISCUSSION
We used improvement methodologyto sustainably increase the percentageof children admitted with CAP whohave a blood culture performed from53% to 100% in 6 months. Differencesin LOS between patients with andwithout blood cultures were notsignificant. This improvement toa median of 100% was sustained for12 months after the completion of theproject although wider variation wasnoted in the ED-specific run chartafter completion of this project. Wehypothesized that this increasedvariation was due to the introductionof additional projects in the ED.
Three groups of interventionsallowed us to impact our key driversand obtain our goal of rapidlyincreasing the rate of blood culturesfor patients admitted with CAP: (1)education; (2) identification andeducation/mitigation; and (3) EMRchanges. Reliability principles havepreviously been used to decrease therate of system failure in health care.24
Interventions can be classified bytheir level of reliability (LOR), whichtranslates to the expected failure ratethat can be achieved with theintervention (for example, a LOR 1intervention should yield a 1021
failure rate).24 In our study, thistranslated to decreasing the numberof patients admitted for CAP without
a blood culture performed in the first24 hours of their visit. We startedwith a LOR 1 intervention, educationand training, which laid thegroundwork necessary for our higherlevel interventions to succeed.Progressing to LOR 2 interventions(identification and education/mitigation) allowed us to achieve ourgoal rate for blood cultures. The LOR3 interventions (EMR changes) wereessential to redesigning our system;providing the ability to scale back ontime-intensive interventions andsustain improvement. Althoughelectronic decision support shouldtheoretically yield a failure rate of1023, we were unable to achieve thislow of a failure rate in our system.This is likely because of the specificcontext of our setting, including alertfatigue from multiple existing BPAs.
Since the publication of the PIDS/IDSAguidelines, several studies haveaddressed the controversy regardingthe utility of blood cultures in childrenwith CAP.3,5,12,25,26 Heine et al3
described 330 patients seen ata pediatric hospital for CAP, of which40% were discharged from the ED and60% were admitted. Blood cultureswere performed in 47% of thepatients in their cohort and 3.2% grewpathogenic bacteria.3 Based on theirresults, the authors advocatedinstitutional guidelines for limitingblood cultures to a subset of pediatricpatients admitted with CAP.3 ThePIDS/IDSA guideline recommendsblood cultures in all patients withmoderate/severe CAP, which our teaminterpreted to include all patientsrequiring admission for CAP. Theutility of routine blood cultures inchildren admitted with CAP is thatchildren with bacteria not covered bytypical first-line antibiotics (ampicillinat our institution) would be identified
earlier. Blood cultures may alsoprovide the only opportunity toidentify the causative bacterium inchildren with subsequent clinicaldeterioration. Better methods ofidentifying the cause of CAP or thoseat risk for deterioration may result ina more targeted approach to bloodcultures in the future.
Our study was designed to evaluate ifimprovement methodology could beused to rapidly increase thepercentage of patients admitted withCAP who have a blood cultureperformed without an unintendedincrease in LOS. We did not finda significant difference in LOS when100% of patients admitted with CAPhad blood cultures performed.Central to the success of this projectis the low rate of blood culturecontamination in our population(1%), which is substantially lowerthan rates (3.2%–3.9%) reported inother studies evaluating the utility ofblood cultures in children withCAP.3,5,12 Our study suggests thatblood cultures can be obtained in allpediatric patients admitted with CAPin a setting with a low rate of bloodculture contamination without fear ofincreased LOS.
We identified a true-positive bloodculture rate of 1.3% that, althoughsimilar to previous studies, issubstantially lower than ourpreintervention rate (6.3%). Thisdifference may be due to ourapproach of obtaining blood cultureson all patients rather than selectively inpatients perceived to be more severelyill.3,4,6,27–30 This may be a closerestimate of the true rate of bacteremiain admitted patients with CAP.
There are several limitations to thisstudy. First, because this project wasperformed at a single institution,
TABLE 2 Association of LOS With Ordering of Blood Cultures for Patients Admitted With CAP
Unadjusted b Coefficient (95% CI) Adjusted b Coefficient (95% CI) Adjusted Percentage Change in Outcome (95% CI)
LOS 0.27 (0.03 to 0.51) 0.18 (20.06 to 0.42) 20.13 (25.82 to 52.20)a
CI, confidence interval.a Adjusted for age, complex chronic conditions, CBC count performed, blood culture positivity, and transfer to ICU.
PEDIATRICS Volume 135, number 4, April 2015 e1057 by guest on June 20, 2018www.aappublications.org/newsDownloaded from

results may not be generalizable toother institutions. The CCHMC hasa strong history of improvement workand a robust infrastructuresupporting improvement effortsincluding easy access to timely data,ability to construct and interpretstatistical process control charts, anda culture of continuous improvement.We hypothesize that these contextualfactors assisted in the rapidity ofuptake and sustainability of ourimprovement. A quality improvementmethods approach, however, could beadapted and used at otherinstitutions to increase the rate ofblood cultures in children admittedwith CAP. Secondly, we identifiedeligible patients, those admitted withsuspected bacterial CAP, by ICD-9codes, which could bias our
population. We limited potential biasby using a previously establishedICD-9 algorithm for patientidentification and verifying eligibilitythrough chart review.20,31 Althoughwe attempted to exclude patientswith suspected viral CAP on chartreview, the degree of suspicion forbacterial CAP is based on clinicaljudgment, because currently there isno highly sensitive and specific test todifferentiate bacterial and viraletiologies. It is possible that inclusionof patients with viral CAP in our studypopulation artificially decreased ourrate of bacteremia. Finally, thecurrent study was not designed toaddress all possible unintendednegative consequences of universalblood cultures in patients admittedwith CAP (eg, increased cost because
of extraneous laboratory tests), butthis will be important in futurestudies.
The PIDS/IDSA CAP guidelineprovided recommendations forevaluation and management, butadherence to this guideline has beenvariable.3,5,25,26,32,33 Our studyhighlights that blood cultures can beroutinely performed in childrenadmitted for CAP without increasingLOS in a setting with a low false-positive blood culture rate.
ACKNOWLEDGMENTS
The authors thank Dr Rebecca Brady,Dr Camille Graham, and JoshuaCourter for their support and contentexpertise during this project.
Address correspondence to Eileen Murtagh Kurowski, MD, MS, Division of Emergency Medicine, Cincinnati Children’s Hospital Medical Center, 3333 Burnet Ave, MLC
2008, Cincinnati, OH 45229-3039. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2015 by the American Academy of Pediatrics
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: Drs Ambroggio and Thomson were supported by funds from the National Research Service Award T32HP10027-14, and Dr Shah was supported by funds
from the National Institute of Allergy and Infectious Diseases K01A173729.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
REFERENCES
1. Bradley JS, Byington CL, Shah SS, et alExecutive summary: the management ofcommunity-acquired pneumonia in infantsand children older than 3 months of age:clinical practice guidelines by thePediatric Infectious Diseases Society andthe Infectious Diseases Society of America.Clin Infect Dis. 2011;53(7):617–630
2. Brogan TV, Hall M, Williams DJ, et al.Variability in processes of care andoutcomes among children hospitalizedwith community-acquired pneumonia.Pediatr Infect Dis J. 2012;31(10):1036–1041
3. Heine D, Cochran C, Moore M, Titus MO,Andrews AL. The prevalence ofbacteremia in pediatric patients withcommunity-acquired pneumonia:guidelines to reduce the frequency ofobtaining blood cultures. Hosp Pediatr.2013;3(2):92–96
4. Hickey RW, Bowman MJ, Smith GA. Utilityof blood cultures in pediatric patientsfound to have pneumonia in theemergency department. Ann Emerg Med.1996;27(6):721–725
5. Myers AL, Hall M, Williams DJ, et al.Prevalence of bacteremia in hospitalizedpediatric patients with community-acquired pneumonia. Pediatr Infect Dis J.2013;32(7):736–740
6. Shah SS, Dugan MH, Bell LM, et al.Blood cultures in the emergencydepartment evaluation of childhoodpneumonia. Pediatr Infect Dis J. 2011;30(6):475–479
7. Lee GE, Lorch SA, Sheffler-Collins S,Kronman MP, Shah SS. Nationalhospitalization trends for pediatricpneumonia and associatedcomplications. Pediatrics. 2010;126(2):204–213
8. Gollomp K, Rankin SC, White C, et alBroad-range bacterial polymerase chainreaction in the microbiologic diagnosisof complicated pneumonia. J Hosp Med.2012;7(1):8–13
9. Cohen E, Mahant S, Dell SD, et al. Thelong-term outcomes of pediatric pleuralempyema: a prospective study. ArchPediatr Adolesc Med. 2012;166(11):999–1004
10. CAPGT. Evidence-Based Care Guideline forMedical Management of Community-Acquired Pneumonia in Children 60 Daysto 17 Years of Age. Cincinnati, OH:Cincinnati Children’s Hospital MedicalCenter; 2005
11. Bates DW, Goldman L, Lee TH.Contaminant blood cultures andresource utilization. The trueconsequences of false-positive results.JAMA. 1991;265(3):365–369
e1058 MURTAGH KUROWSKI et al by guest on June 20, 2018www.aappublications.org/newsDownloaded from

12. Hall RT, Domenico HJ, Self WH, Hain PD.Reducing the blood culturecontamination rate in a pediatricemergency department and subsequentcost savings. Pediatrics. 2013;131(1).Available at: www.pediatrics.org/cgi/content/full/131/1/e292
13. Sard B, Bailey MC, Vinci R. An analysis ofpediatric blood cultures in thepostpneumococcal conjugate vaccineera in a community hospital emergencydepartment. Pediatr Emerg Care. 2006;22(5):295–300
14. Surdulescu S, Utamsingh D, Shekar R.Phlebotomy teams reduce blood-culturecontamination rate and save money. ClinPerform Qual Health Care. 1998;6(2):60–62
15. Cohen MR, Senders J, Davis NM. Failuremode and effects analysis: a novelapproach to avoiding dangerousmedication errors and accidents. HospPharm. 1994;29(4):319–330
16. DeRosier J, Stalhandske E, Bagian JP,Nudell T. Using health care Failure Modeand Effect Analysis: the VA NationalCenter for Patient Safety’s prospectiverisk analysis system. Jt Comm J QualImprov. 2002;28(5):248–267, 209
17. Langley G, Nolan K, Nolan T, Norman C,Provost L. The Improvement Guide. APractical Approach to EnhancingOrganizational Performance. SanFrancisco, CA: Jossey-Boss; 1996
18. Luria JW, Muething SE, Schoettker PJ,Kotagal UR. Reliability science andpatient safety. Pediatr Clin North Am.2006;53(6):1121–1133
19. Nolan T, Resar R, Haraden C, Griffin FA.Improving the Reliability of Health Care.
IHI Innovation Series White Paper.Boston, MA: Institute for HealthcareImprovement; 2004:1–16
20. Williams DJ, Shah SS, Myers A, et al.Identifying pediatric community-acquired pneumonia hospitalizations:accuracy of administrative billingcodes. JAMA Pediatr. 2013;167(9):851–858
21. Feudtner C, Christakis DA, Connell FA.Pediatric deaths attributable to complexchronic conditions: a population-basedstudy of Washington State, 1980-1997.Pediatrics. 2000;106(1 pt 2):205–209
22. Gilboy N, United States Agency forHealthcare Research and Quality.Emergency Severity Index (ESI). Version4 Implementation Handbook: A TriageTool for Emergency Department. AHRQpublication number 12-0014. Rockville,MD: Agency for Healthcare Research andQuality; 2012
23. Vittinghoff E, Glidden DV, Shiboski SC,McCulloch CE. Regression Methods inBiostatistics: Linear, Logistic, Survival,and Repeated Measures Models. NewYork, NY: Springer; 2005
24. Nolan TW, Resar R, Haraden C, Griffin F.Improving the Reliability of Health Care.IHI Innovation Series White Paper.Boston, MA: Institute for HealthcareImprovement; 2004
25. Parikh K, Davis AB, Pavuluri P. Do weneed this blood culture? Hosp Pediatr.2014;4(2):78–84
26. Williams DJ. Do all children hospitalizedwith community-acquired pneumoniarequire blood cultures? Hosp Pediatr.2013;3(2):177–179
27. Bonadio WA. Bacteremia in febrilechildren with lobar pneumonia andleukocytosis. Pediatr Emerg Care. 1988;4(4):241–242
28. Esposito S, Marchese A, Tozzi AE, et al;Italian Pneumococcal CAP Group.Bacteremic pneumococcal community-acquired pneumonia in children lessthan 5 years of age in Italy. Pediatr InfectDis J. 2012;31(7):705–710
29. Grant CC, Emery D, Milne T, et al. Riskfactors for community-acquiredpneumonia in pre-school-aged children.J Paediatr Child Health. 2012;48(5):402–412
30. Shah SS, Alpern ER, Zwerling L, McGowanKL, Bell LM. Risk of bacteremia in youngchildren with pneumonia treated asoutpatients. Arch Pediatr Adolesc Med.2003;157(4):389–392
31. Ambroggio L, Thomson J, MurtaghKurowski E, et al. Quality improvementmethods increase appropriate antibioticprescribing for childhood pneumonia.Pediatrics. 2013;131(5). Available at:www.pediatrics.org/cgi/content/full/131/5/e1623
32. Neuman MI, Hall M, Hersh AL, et al.Influence of hospital guidelines onmanagement of children hospitalizedwith pneumonia. Pediatrics. 2012;130(5).Available at: www.pediatrics.org/cgi/content/full/130/5/e823
33. Newman RE, Hedican EB, Herigon JC,Williams DD, Williams AR, Newland JG.Impact of a guideline on management ofchildren hospitalized with community-acquired pneumonia. Pediatrics. 2012;129(3). Available at: www.pediatrics.org/cgi/content/full/129/3/e597
PEDIATRICS Volume 135, number 4, April 2015 e1059 by guest on June 20, 2018www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2014-2077 originally published online March 16, 2015; 2015;135;e1052Pediatrics
Sheehan, Srikant Iyer, Christine White and Lilliam AmbroggioEileen Murtagh Kurowski, Samir S. Shah, Joanna Thomson, Angela Statile, Brieanne
in Children With PneumoniaImprovement Methodology Increases Guideline Recommended Blood Cultures
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/135/4/e1052including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/135/4/e1052#BIBLThis article cites 26 articles, 7 of which you can access for free at:
Subspecialty Collections
ine_subhttp://www.aappublications.org/cgi/collection/evidence-based_medicEvidence-Based Medicinesubhttp://www.aappublications.org/cgi/collection/quality_improvement_Quality Improvemente_management_subhttp://www.aappublications.org/cgi/collection/administration:practicAdministration/Practice Managementfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on June 20, 2018www.aappublications.org/newsDownloaded from
DOI: 10.1542/peds.2014-2077 originally published online March 16, 2015; 2015;135;e1052Pediatrics
Sheehan, Srikant Iyer, Christine White and Lilliam AmbroggioEileen Murtagh Kurowski, Samir S. Shah, Joanna Thomson, Angela Statile, Brieanne
in Children With PneumoniaImprovement Methodology Increases Guideline Recommended Blood Cultures
http://pediatrics.aappublications.org/content/135/4/e1052located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://pediatrics.aappublications.org/content/suppl/2015/03/11/peds.2014-2077.DCSupplementalData Supplement at:
ISSN: 1073-0397. 60007. Copyright © 2015 by the American Academy of Pediatrics. All rights reserved. Print the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on June 20, 2018www.aappublications.org/newsDownloaded from





























