Embed Size (px)
Citation preview
Method
All neonates born after gestational
week 37 that are admitted to the
Neonatal Intensive Care Unit at
Stavanger University Hospital, Norway,
with suspected Early onset Sepsis
(start of antibiotic before 72 hours of
age) are clinically evaluated by a nurse
every hour using a standardized
assessment form.
Results
Process Change: “how good by when?”
Process-Background:
Neonatal sepsis is associated with high mortality and morbidity (1) but symptoms are unspecific.
No diagnostic tools are available at the time antibiotic treatment is started.
Empirical antibiotics given to 2-10 % of all term neonates in Europe and USA are implemented because of the fear
of sepsis (1)
Antibiotics given in the first year of life are linked to an increased risk for death, nosocomial infection, Chronic lung
disease, Asthma, eczema and Juvenile Arteritis (2,3). In addition to the increasing concern for multi resistant bacteria.
Process-Aim:
To reduce the use of antibiotics administered to term neonates within the first 4 days of life in a single Norwegian
NICU within August 2016 by:
1. Reduce the use of antibiotics administered to term healthy neonates to below 1 %
Healthy neonates = neonates treated with antibiotic and treated for less than 5 days without proven sepsis
2. Reduce the total use of antibiotics to less than 3,0 % of neonates
3. Balancing question (4): No increase in mortality or delay in start of treatment to neonates with infection
Change: Improved assessment sheet of neonates to predict if the neonate has sepsis or other common postnatal condition
The assessment form for neonates with suspected early onset
sepsis is an efficient and safe tool to reduce the use of antibiotics to
term healthy neonates in the Neonatal Intensive Care.
Conclusions
Further information contact: [email protected]
Consultant Anlaug Vatne (1), Solfrid Orre (1), Eli Sanne (1), Karin Jensvold (2), Knut Øymar (1,3).1.Pediatric Department, Stavanger University Hospital, Stavanger, Norway2. Department of Patient safety and Quality, Stavanger University Hospital, Stavanger, Norway
3- Department of Clinical science, University of Bergen, Bergen, Norway
Achievements
Increased knowledge among staff in
neonatal observations and assessments
Increased knowledge and use of Plan-Do-
Study-Act circles
Focus on correct use of antibiotics in the
NICU
Change takes time: multiple small steps will
gradually deliver results as knowledge
increases, cultures develop and people
adapt
Involvement is key to success: engagement
and involvement bring commitment,
ownership and willingness
Reducing variations is a goal: to maintain
stability and predictability. Variations should
be limited to increased patient safety.
“ If I had to reduce my message for
management to just a few words, I’d say
that it all had to do with variations” (5)
Key Learning Points
Key Reference Materials
(1) Fjalstad, J.W, Early-onset sepsis and antibiotic exposure in term infants: a nationwide population-based study in Norway. Pediatr Infect Dis J, 2016. (2)
Johson, C.C et al. Antibiotic exposure in early infancy and risk for childhood atopy. J Allergy Clin Immunol, 2005.(3) Antiobiotic Exposure and Juvenile
Idiopathic Artheritis, Pediatrics, 2015 (4)Quality Health Care, Robert Loyd. (5) Out of the crisis, W.E.Deming. (6)The Improvement Guide. Langley J et al
Improved antibiotic treatment in Neonatal Intensive Care – a Quality
Improvement project among term infants at Stavanger University Hospital
Next steps
• Evaluation of project August 2016 to show reliability and sustainability
over time
• Publish project
• Continue improvement work in Unit
• Increased focus on patient’s involvement
«I think that we put too many babies on
antibiotics. It is difficult to clinically assess if
a baby has an early infection or not. I think
that we can now better evaluate this. I feel
this is safer and I hope we can treat less
babies with antibiotics» Junior doctor «« I have been afraid that the junior doctors
on duty wouldn’t pay attention to my
concern if a baby is getting increasingly ill.
Remember the baby that died in November
from Sepsis, I’ve been afraid that this can
happen again. The new assessment sheet
gives me a better tool to communicate my
concerns for the baby to the doctor on duty
to secure correct treatment» Neonatal
nurse
«I feel the assessment sheet is much safer. I
can safely postpone start of antibiotic in a
non-critically-ill neonate and assesss if the
symptoms are caused by other common after-
birth conditions and wait for bloodtests. It
feels more safe for the baby» Consultant
Neonatology
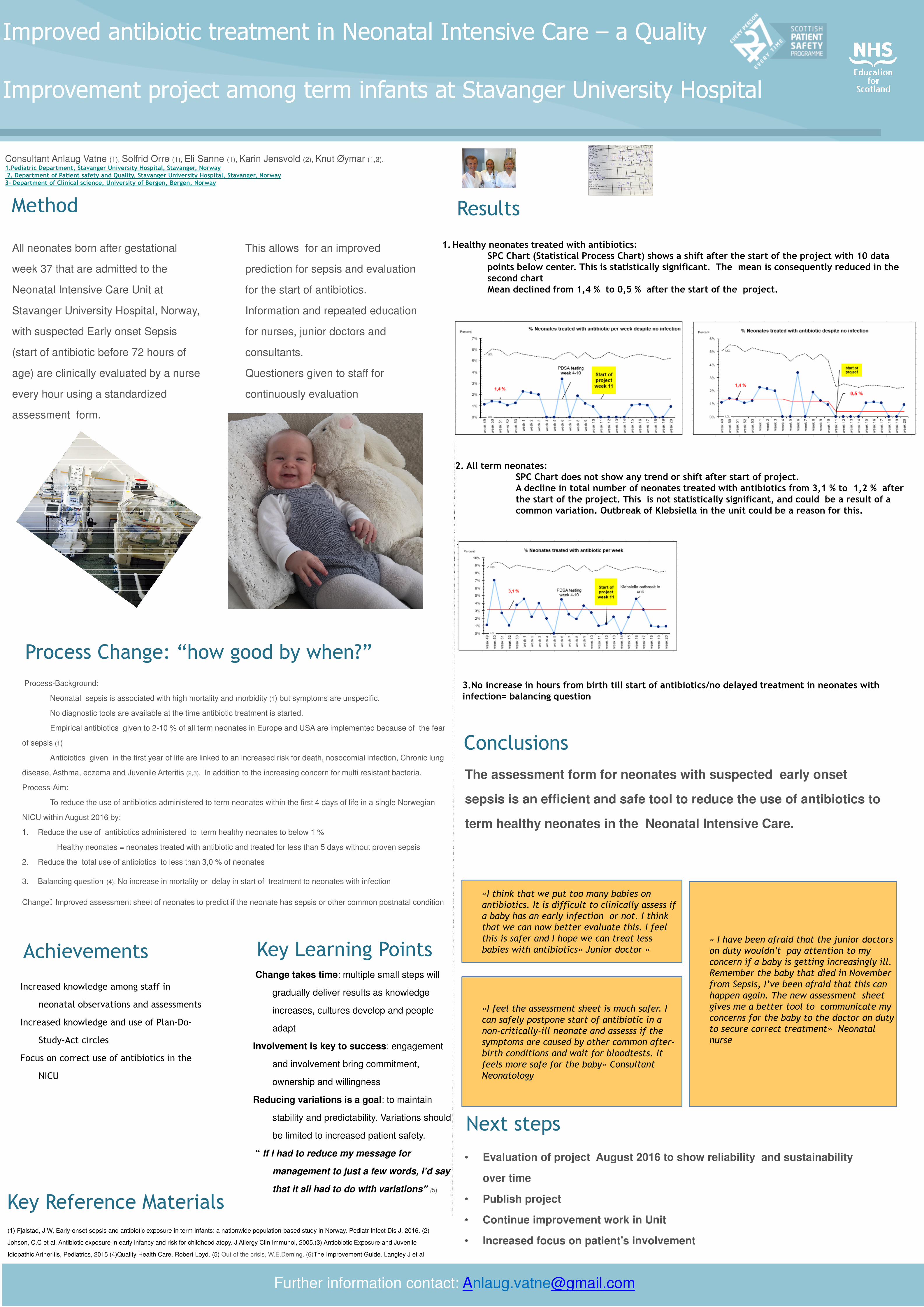
1. Healthy neonates treated with antibiotics:SPC Chart (Statistical Process Chart) shows a shift after the start of the project with 10 data points below center. This is statistically significant. The mean is consequently reduced in the second chartMean declined from 1,4 % to 0,5 % after the start of the project.
2. All term neonates: SPC Chart does not show any trend or shift after start of project.A decline in total number of neonates treated with antibiotics from 3,1 % to 1,2 % afterthe start of the project. This is not statistically significant, and could be a result of a common variation. Outbreak of Klebsiella in the unit could be a reason for this.
3.No increase in hours from birth till start of antibiotics/no delayed treatment in neonates withinfection= balancing question
This allows for an improved
prediction for sepsis and evaluation
for the start of antibiotics.
Information and repeated education
for nurses, junior doctors and
consultants.
Questioners given to staff for
continuously evaluation





























