Embed Size (px)
Citation preview
Improve Patient Care Through Clinical Research:
Making EBP A Reality Anna C. Kubiczki, MS, LAT, ATC
Monica R. Lininger, PhD, LAT, ATC
1
Goals
• Identify areas of EBP weakness in Athletic Training
•Demonstrate the value of clinical EBP and research
• Provide ideas to help Athletic Trainers (AT) become evidence-based clinicians and clinical researchers
2
Evidence Based Practice
“Without clinical expertise, practice risks becoming tyrannized by evidence, for even excellent external evidence may be inapplicable
to or inappropriate for an individual patient. Without current best evidence, practice risks becoming rapidly out of data, to the
detriment of patients.”1
-David L. Sackett
3
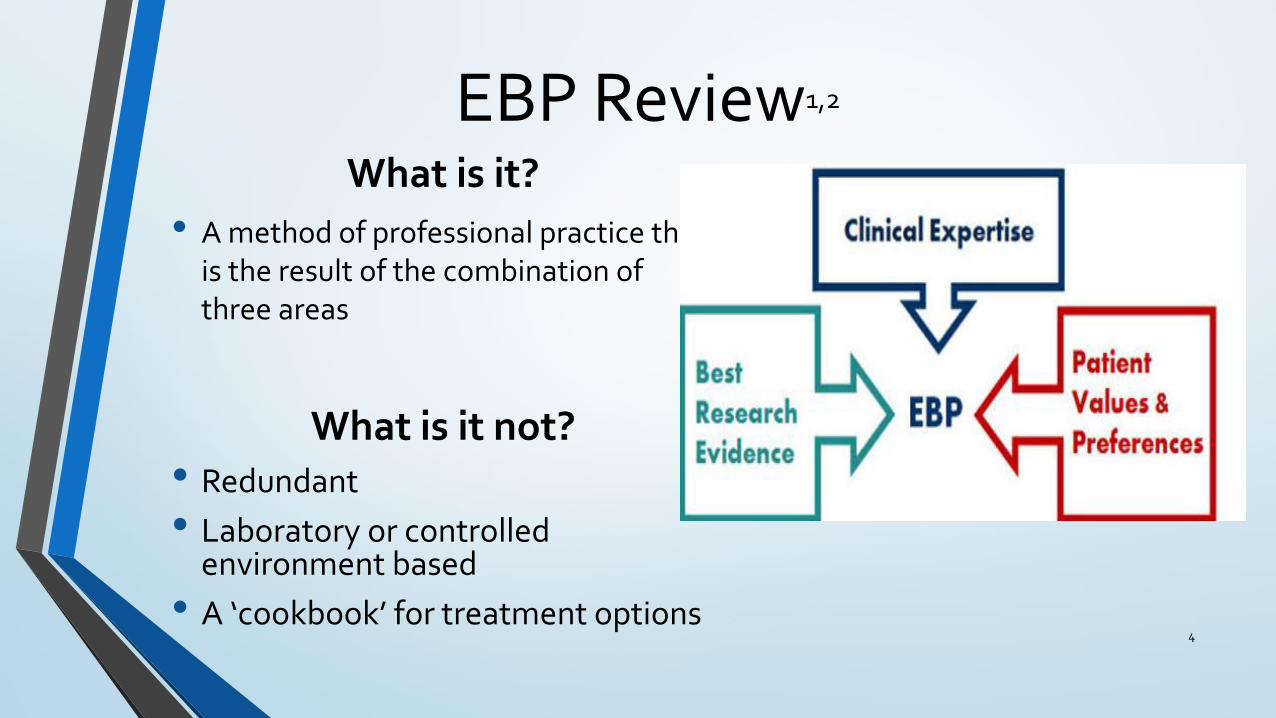
EBP Review1,2
What is it?
• A method of professional practice that is the result of the combination of three areas
What is it not?• Redundant
• Laboratory or controlled environment based
• A ‘cookbook’ for treatment options4
5
Why do healthcare professionals struggle to incorporate EBP?2,3,4
• A problem for all healthcare professionals despite their belief that it is a good idea
• Of ATs –
• Over 97% believe EBP is important to the profession
• 92% believe that EBP improves the quality of patient care
• Less than 20% of clinical AT read professional literature on a regular basis
• 84% believe that they need to increase the use of evidence in their clinical practice
6
What seems to be the problem?2,3,4
• Lack of time
• Lack of confidence in implementing EBP
• Setting/environmental limitations
• Inability to interpret/appraise the literature
• Poor accessibility to literature
• Lack of support from coworkers or administration
• Inability to create answerable clinical questions
• Personal interest in EBP
7
My Perceived EBP Barriers
• Young professional
• New work environment
• Lack of confidence in implementing EBP
• Never attempt to form answerable clinical questions
8
Benefits from EBP Implementation1,2,3
• Improves patient care and compliance
• Dissemination of knowledge
• Promotes professionalism among other healthcare providers
• Cost-effective healthcare
• Support for athletic training state licensure
• Third party reimbursement possibilities
• Continuing education for students, clinicians, researchers, and educators alike
9
Why I Decided to Change
• Improve my patient care
• Improve my patients’ experiences as student-athletes
• Break out of my young professional mindset
• Provide a learning platform for ATP students
10
Making EBP a Clinical RealityHow I overcame the barriers of EBP and helped my patients
and clinical practice
11
Formulating my Clinical Question • Injury reduction of my patient population
• High prevalence in injuries to the lower extremity
• Decided to focus on the ankle joint for various reasons:
oCommon injury to the team according to past data
oStart of the kinetic chain
oPersonal interest
• How could improving ankle function help to reduce injuries to the lower extremity in female collegiate soccer players?
12
Searching for Evidence
• Accessed a variety of sources
• Google scholar
• PubMed
• Peer-reviewed journal articles
• Searched for prevalence of ankle injuries in soccer players
• Searched for ankle injury prevention and rehabilitation tools
• Search for objective ways to measure
13
Prevalence of Ankle Injuries in Soccer Players
• Extremely common5-9
• 15-30% of all injuries sustained in sports
• Soccer has one of the highest incidence rates of 6.52 per 1000 person-hours
• Highly susceptible to re-injury10-13
• 80% of patients who experience an ankle injury will sustain another one on the same side
• Variety of factors5,7,8,10,11,12,13,14,15,17
• Intrinsic: kinematics, range of motion (ROM), functional instability, leg dominance, postural control
• Extrinsic: direct contact, artificial turf, shoe type, inadequate warm-up
• Soccer specific: muscular imbalances, ROM, and neuromuscular imbalances due to leg-dominance 14

Ankle Injury Prevention and Treatment15,16,20,21,22,25
Prevention Tools
• Very few recommendations due to a lack of evidence/research:
• Exercise therapy
• Taping or bracing
• Preventative footwear
Rehabilitation Tools
15
• Numerous studies with strong evidence supported recommendations:
• Exercise therapy
• Joint mobilizations
• Functional bracing
Objective Ways to Measure Function10,11,12,18,27
• Star-Excursion Balance Test (SEBT)
• Y-Balance Test
• ROM
• Landing biomechanics
• Instrumented arthrometer
• Single-leg hop-stabilization task
• Radiographs 16
…Now What?
• Asked my clinical question
• Accessed information related to my clinical question
• Appraised the data I found
• How do I start to apply it?17
Collaboration
• Sound design and methodology
• Excited to assist
• Research process through the institution
18
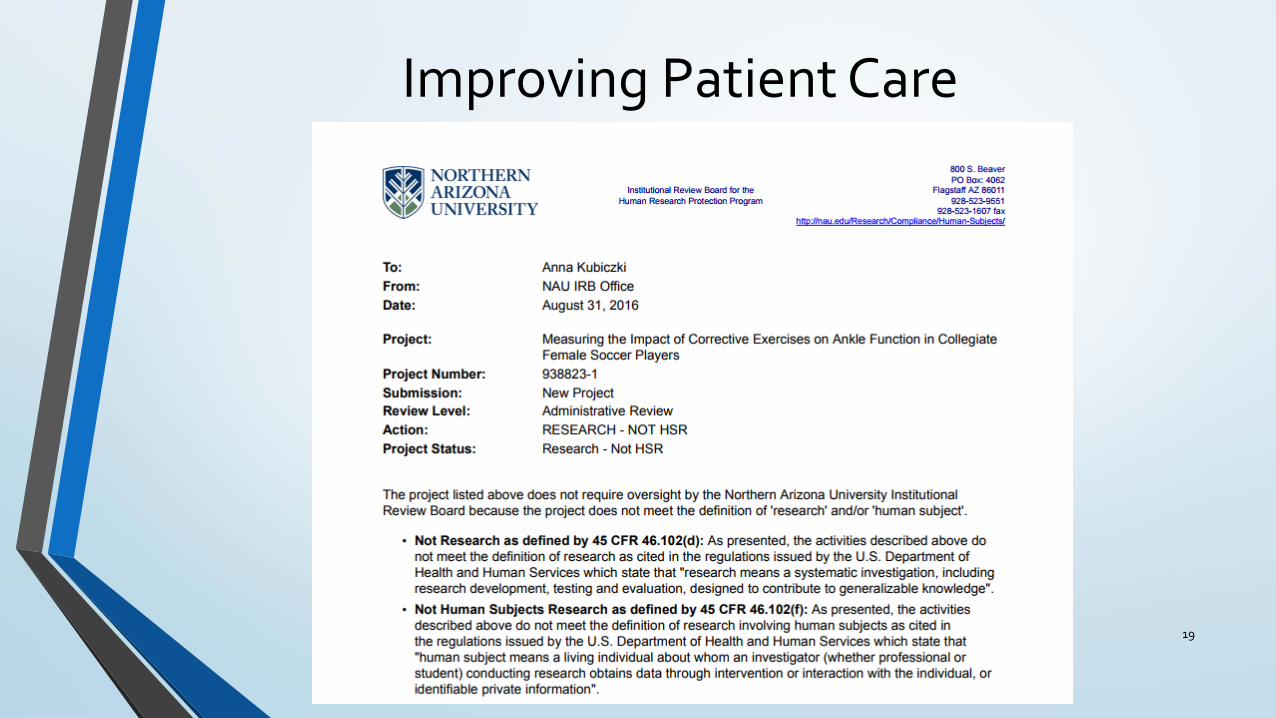
Improving Patient Care
19
Disseminate to the Profession
20
Hypothesis
• The implementation of corrective exercises specific to the ankle joint will improve ankle ROM and scores on the SEBT and thereby reduce the incidence of injury to the lower extremity in female collegiate soccer players
21
Justification10,11,12,15,16,18,20,21,22,23,24,25
• Decided on corrective exercises because it was supported by evidence as both a preventative and rehabilitative technique
• Created 2 exercises designed to overcome deficits in ankle ROM, muscular strength, and dynamic neuromuscular control
• Progress was measured objectively with the SEBT and ROM due to the ease, speed, and cost of performing these tests
22
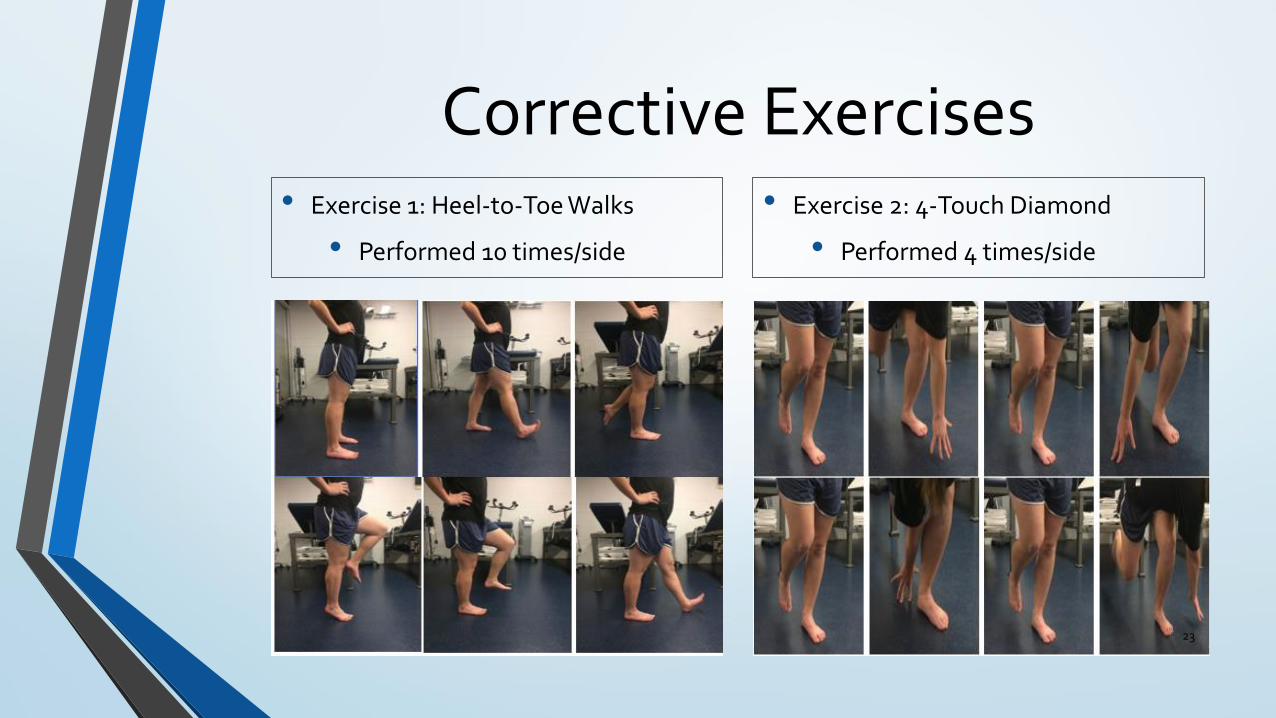
Corrective Exercises• Exercise 1: Heel-to-Toe Walks
• Performed 10 times/side
• Exercise 2: 4-Touch Diamond
• Performed 4 times/side
23
Objective Measurements
Ankle ROM
Standard goniometric measurements
• Short-seated active plantarflexion and dorsiflexion
SEBT
Leg length-ASIS to ipsilateral medial malleolus
Directional diagram create with 1.5” athletic tape
• Anterior, posteromedial, and posterolateral23,24
• Posteromedial and posterolateral were angled 1350 off of the anterior
24ALL MEASUREMENTS AND TESTING TOOK BETWEEN 4-7 MINUTE TO PERFORM
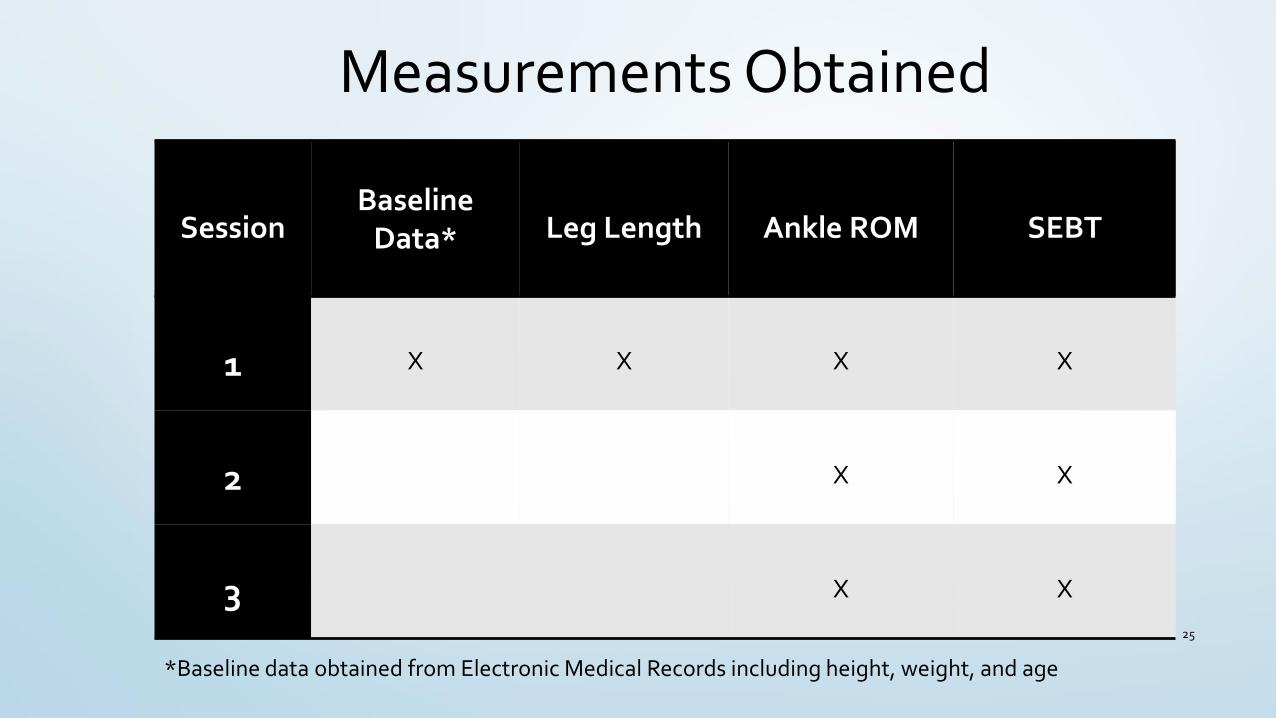
Measurements Obtained
SessionBaseline
Data* Leg Length Ankle ROM SEBT
1 X X X X
2 X X
3 X X
*Baseline data obtained from Electronic Medical Records including height, weight, and age
25
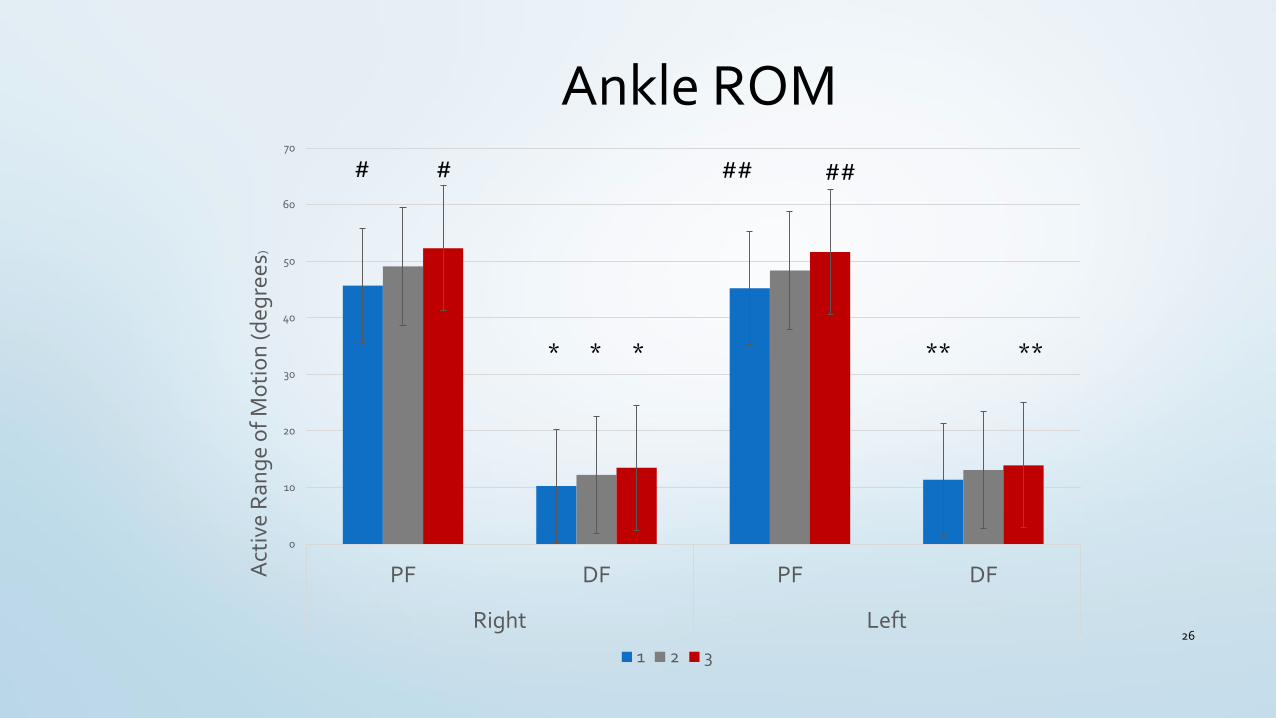
Ankle ROM
0
10
20
30
40
50
60
70
PF DF PF DF
Right Left
Act
ive
Ran
ge
of
Mo
tio
n (d
egre
es)
1 2 3
*
26
* * ****
### # ##
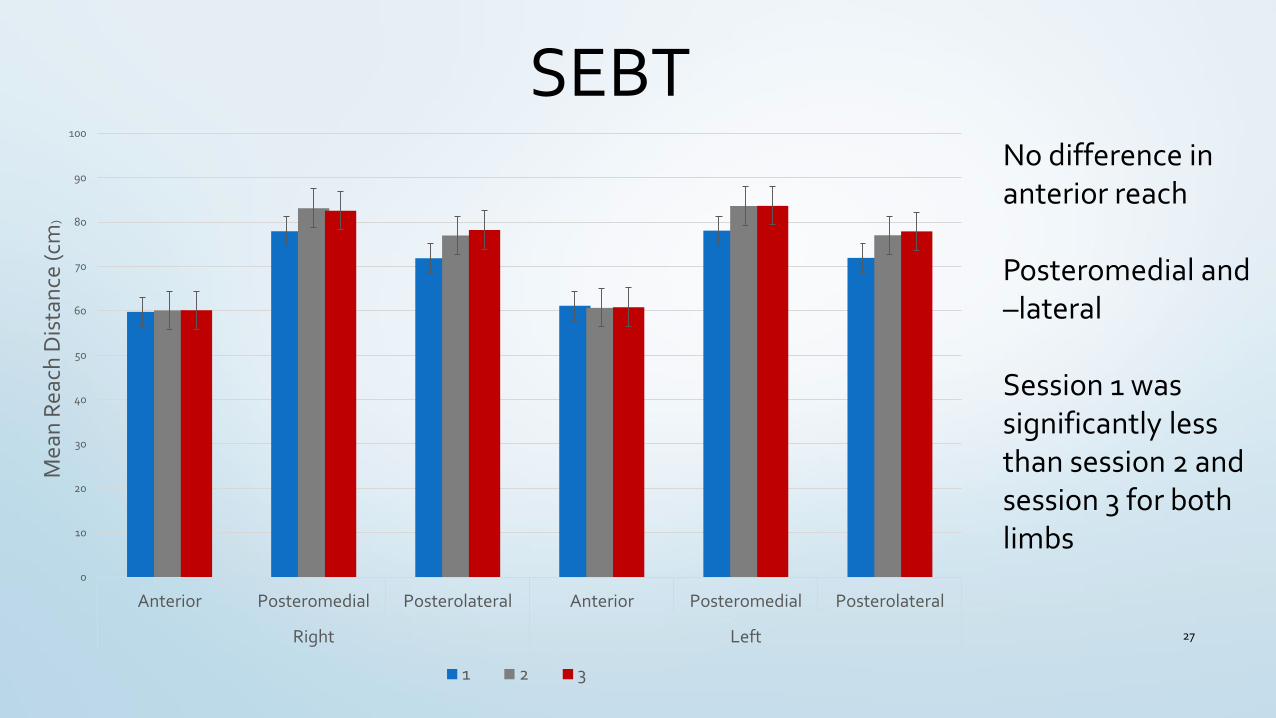
SEBT
27
0
10
20
30
40
50
60
70
80
90
100
Anterior Posteromedial Posterolateral Anterior Posteromedial Posterolateral
Right Left
Mea
n R
each
Dis
tan
ce (c
m)
1 2 3
No difference in anterior reach
Posteromedial and –lateral
Session 1 was significantly less than session 2 and session 3 for both limbs
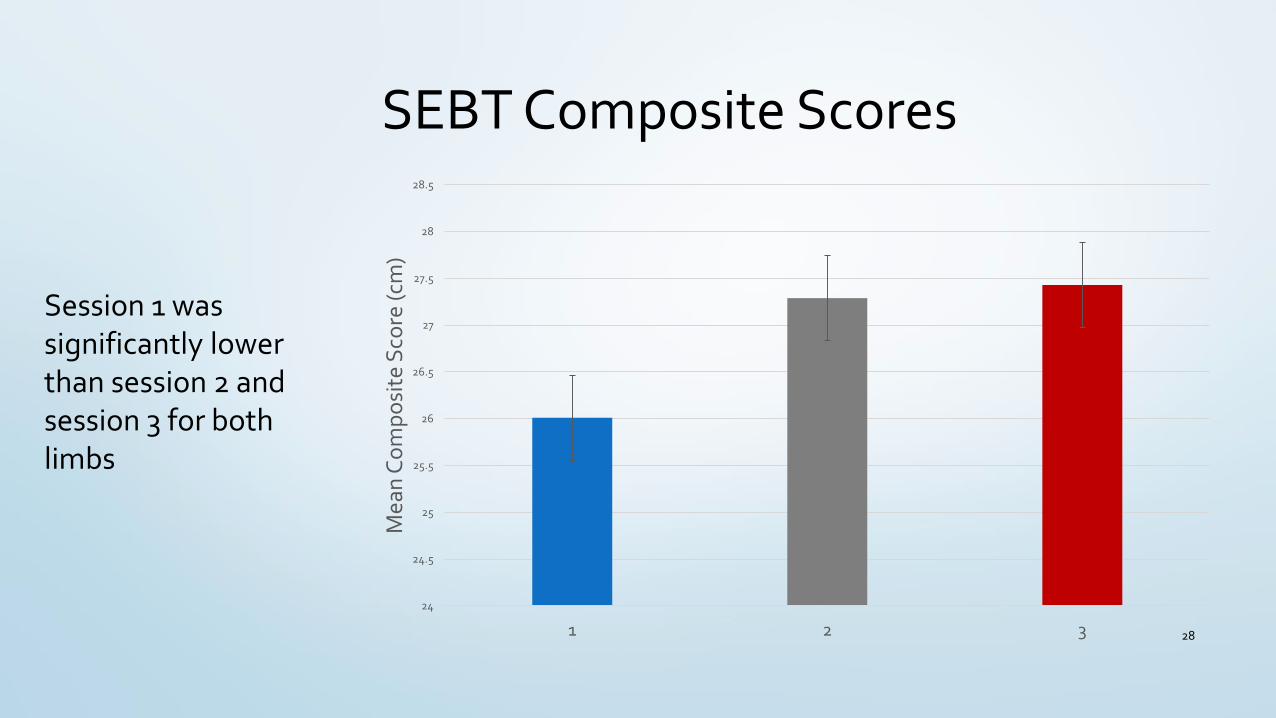
SEBT Composite Scores
28
24
24.5
25
25.5
26
26.5
27
27.5
28
28.5
1 2 3
Mea
n C
om
po
site
Sco
re (c
m)
Session 1 was significantly lower than session 2 and session 3 for both limbs
Assessing the Results
• The 2 corrective exercises improved ankle ROM
• Supports other findings that corrective exercises can restore normal ankle ROM
• The 2 corrective exercises improved the scores of the SEBT
• Only direction of no improvement was the anterior direction
• Improvement in the composite score demonstrates that the corrective exercises helped to reduce the risk of lower-extremity injury
• 50% of the participants experienced an injury to the lower-extremity
• There are not enough data to support that the addition of corrective exercises reduced the incident of lower-extremity injury
29
My EBP Challenges
• Patient compliance
• The data collection process
• Re-learning about statistics
• Emotional reaction to injuries
30
Making EBP YOUR Clinical RealityHelpful hints and tricks to find your way through the maze of EBP
31
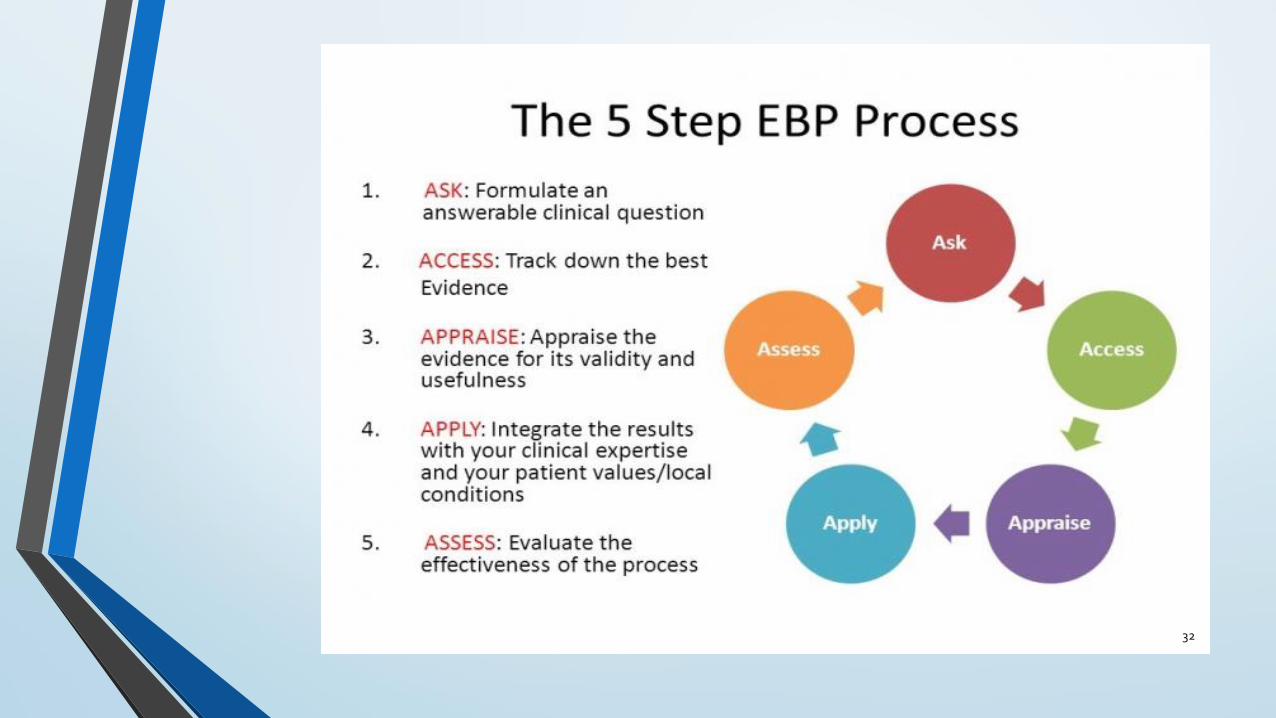
32
What do I need to ASK?
•Who?
• Who would benefit the most from my intervention?
• Who can help me accomplish my intervention?
• Who do I need permission from to perform my clinical research?
•What?
• What is a problem/area of concern in my patient population?
• What is my intervention?
• What do I need to perform my intervention?
33
What do I need to ASK?
•Why?
• Why do I believe an intervention is necessary?
• Why do I believe my intervention will work?
•How?
• How long do I want to perform my intervention?
• How do I make my intervention patient-centered?
• How can I determine if my intervention is working?
34
How can I ACCESS literature?
• Online search engines
• MEDLINE
• PubMed
• Professional literature or peer-reviewed journal articles
• Systematic reviews and meta-analyses
• NATA Position Statements
• Websites
• Textbooks
• Athletic Training Educators/Faculty35
How do I APPRAISE the literature I find?• Is the source reliable and valid?
• Clinical prediction rules
• Statistical analysis
• Does the source provide information to support or disprove my intervention?
• Do I need to gather more information about the source before deeming is valuable and useful information?
• Does the source help me implement my intervention?
• Does the source support or disprove my measurement tools?
• Do I need to ask for help?36
How do I APPLY my intervention?
• Always should be patient-centered
• Several options:
• Apply to a specific population (one team, males, females, etc…)
• Apply to a specific season (competitive, off-season, pre-season, etc…)
• Apply to a specific type of injury (AC joint sprain, ACL sprain, quadricpes strain, etc...)
37
How do I APPLY my intervention?
• Have both subjective and objective ways to measure how the intervention is working
• Find tools that are quick, easy, and inexpensive!
• Can measure at Pre-participation exams, end-of-season exams, following an injury, etc…
• All of your patients do not have to participate to collect meaningful data
• Do not be discouraged by non-compliance or drop-outs
• Allow the patients to provide feedback as to why they decided to not participate
38
Examples of Measurement Tools
Subjective26
• Visual analog scale
• Numeric rating scale
• McGill Pain Questionnaire
• Short-form McGill Questionnaire
• Short Form-36 Bodily Pain Scale
• Measurement of Intermittent and Constant Osteoarthritis Pain
• http://dx.doi.org/10.1002/acr.20543
Objective27,28
• Square-hop test (Lower extremity injury)
• Drop vertical jump task (ACL sprain)
• Hamstring:Quadriceps strength ratio (Hamstring strains)
• Hip adduction:Hip Abduction strength ratio (Groin strains)
• Closed Kinetic Chain Upper Extremity Stability Test (General Shoulder
• http://doi.org/10.1177/1941738114523239
• https://doi.org/10.1007/BF03262295 39
How do I ASSESS the results?
• Compare pre-intervention measurements to post-intervention
• Did the patient(s) improve after receiving the intervention?
• Compare intervention data to non-intervention data
• How do the patients who received the intervention compare to those who did not?
• Perform statistical analysis of the results
• DO NOT BE AFRAID TO ASK FOR HELP HERE!
• Helps to determine if your intervention improved patient care
• Clinical significance is also important!
• Small sample sizes can be statistically insignificant but not clinically insignificant!40
Thank you!Any questions?
41
References 1. Sackett, D.L., Rosenberg, W.M.C., Haynes, R.B., Richardson, W.S. Evidence based medicine: what it is and what it
isn’t. British Medical Journal. 1996;312:71-72.
2. Hankemeier, D. A., Walter, J. M., McCarty, C. W., Newton, E. J., Walker, S. E., Pribesh, S. L., … Van Lunen, B. L. Use of evidence-based practice among athletic training educators, clinicians, and students, part 1: perceived importance, knowledge, and confidence. Journal of Athletic Training. 2013;48(3):394–404. http://doi.org/10.4085/1062-6050-48.2.16
3. Manspeaker, S., Van Lunen, B. Overcoming barriers to implementation of evidence-based practice concepts in athletic training education: perceptions of select educators. Journal of Athletic Training. 2011;46(5):514–522.
4. McCarty, C.W., Hankemeier, D. A., Walter, J. M., Newton, E. J., Van Lunen, B. L. Use of evidence-based practice among athletic training educators, clinicians, and students, part 2: attitudes, beliefs, accessibility, and barriers. Journal of Athletic Training. 2013;48(3):405–415. http://doi.org/10.4085/1062-6050-48.2.19
5. Fong DTP, Hong Y, Chan LK, Yung PSH, Chan KM. A systematic review on ankle injury and ankle sprain in sports. Sports Medicine. 2007;37(1):73-94.
6. Hootman JM, Dick R, Agel J. Epidemiology of collegiate injuries for 15 sports: summary and recommendations for injury prevention initiatives. Journal of Athletic Training. 2007;42(2)311-319.
7. McKeon PO, Hertel J. Systematic review of postural control and lateral ankle instability, part 1: can deficits be detected with instrumented testing?. Journal of Athletic Training. 2008;43(3)293-304
8. Fousekis K, Tsepis E, Vagenas G. Intrinsic risk factors of noncontact ankle sprains in soccer: a prospective study on 100 professional players. The American Journal of Sports Medicine. 2012;40(8):1842-1850.
9. Sobhani S, Dekker R, Postema K, Dijkstra PU. Epidemiology of ankle and foot overuse injuries in sports: a systematic review. Scandinavian Journal of Medicine and Science in Sports. 2013;23:669-686.
42
References 10. Gribble PA, Hertel J, Denegar CR. Chronic ankle instability and fatigue create proximal joint alterations during
performance of the star excursion balance test. International Journal of Sports Medicine. 2007;28:236-242.
11. Gribble PA, Hertel J, Plisky P. Using the star excursion balance test to assess dynamic postural-control deficits and outcomes in lower extremity injury. Journal of Athletic Training. 2012;47(3):339-357.
12. de Noronha M, Franca LC, Haupenthal A, Nunes GS. Intrinsic predictive factors for ankle sprain in active university atudents: a prospective study. Scandinavian Journal of Medicine and Science in Sports. 2013;23:541-547.
13. Denegar CR, Hertel J, Fonseca J. The effect of lateral ankle sprain on dorsiflexion range of motion, posterior talarglide, and joint laxity. Journal of Orthopaedic and Sports Physical Therapy. 2002;32(4)166-173.
14. Wikstrom EA, Tillman MD, Chmielewski TL, Cauraugh JH, Naugle KE, Borsa PA. Dynamic postural control but not mechanical instability differs among those with and without chronic ankle instability. Scandinavian Journal of Medicine and Science in Sports. 2010;20:137-144.
15. Kerkhoffs GM, van den Bekerom M, Elders LAM, et al. Diagnosis, treatment, and prevention of ankle sprains: an evidence-based clinical guide. British Journal of Sports Medicine. 2012;46:854-860.
16. Fong CM, Blackburn JT, Norcross MF, McGrath M, Padua DA. Ankle-Dorsiflexion range of motion and landing biomechanics. Journal of Athletic Training. 2011;46(1):5-10
17. Fullam K, Caulfield B, Coughlan GF, Delahunt E. Kinematic analysis of selected reach directions of the star excursion balance test compared with the y-balance test. Journal of Sport Rehabilitation. 2014;23:27-35.
18. Plisky PJ, Rauh MJ, Kaminski TW, Underwood FB. Star excursion balance test as a predictor of lower extremity injury in high school basketball players. Journal of Orthopaedic and Sports Physical Therapy. 2006;36(12):911-919.
19. Hupperets MDW, Verghagen EALM, van Mechelen W. Effect of unsupervised home based proprioceptive training on recurrences of ankle sprain: randomised control trial. British Medical Journal. 2009;339:b2684.
43
References 20.van der Wees PJ, Lenssen AF, Hendriks EJM, Stomp DJ, Dekker J, de Bie RA. Effectiveness of exercise therapy and
manual mobilisation in acute ankle sprain and functional instability: a systematic review. Australian Journal of Physiotherapy. 2006;52:27-37.
21.Verhagen EALM, van Mechelen W, de Vente W. The effect of preventive measures on the incidence of ankle sprain. Clinical Journal of Sports Medicine. 2000;10(4)291-296.
22.Hetel J, Braham RA, Hale SA, Olmstead-Kramer LC. Simplifying the star excursion balance test: analyses of subjects with and without chronic ankle instability. Journal of Orthopaedic Sports Physical Therapy. 2006;36:131-137.
23.Hertel J, Miller SJ, Denegar CR. Intratester and intertester reliability during the star excursion balance test. Journal of Sports Rehabilitation. 2000;9:104-116.
24.Kim KJ, Kim YE, Jun HJ, Lee JS, Ji SH, Ji SG, et al. Which treatment is more effective for functional ankle instability: strengthening or combined muscle strengthening and proprioceptive exercises? J.Phys.Ther.Sci. 2014;26:385-388.
25.Masafumi T, Pietrosimone BG, Gribble PA. Therapeutic interventions for increasing ankle dorsiflexion after ankle sprain: a systematic review. JAT. 2013;48(5):696-709.
26.Hawker, G. A., Mian, S., Kendzerska, T.,French, M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Research. 2011;63:S240–S252.
27.Dallinga, J.M., Benjaminse, A., Lemmink, K.A.P.M. Which screening tools can predict injury to the lower extremities in team sports? Sports Medicine. 2012; 42(9):791-815.
28.Pontillo, M., Spinelli, B.A., Sennett, B.J. Prediction of in-season shoulder injury from preseason testing in division 1 collegiate football players. Sports Health. 2014; 6(6): 497-503.
44