Embed Size (px)
Citation preview
In collaboration with Prof. Dr. med. dent. Bernd Wöstmann Prof. John M. Powers, Ph.D.
Impressioning Compendium
Espertise™
A guideline for excellent impressions in theory and practice

A guideline for excellent impressions in theory and practice
guideline
Espertise™
2 |
Preface
Astheworldwidemarketleaderinimpressioning,3MESPEaspirestobethepartnerofchoiceforprecisionimpressionsinpracticeandteachingestablishments.Ourgoalistoleverageourexpertiseininnovativematerials,technology,andmanufacturingtoprovideourcustomerswiththehighestperformingimpressioningsystemsandworkflowonthemarket.Wehavereceivedaresounding,positiveresponsetothefirstandsecondeditionsof“PrecisionImpressions–AGuidelineforTheoryandPractice”fromdentistsaroundtheworld.Thisconfirmstheimportanceofourprocess-orientedapproachanddemonstratesourcommitmenttocontinuallydelivercustomer-valuedsolutions.
Overthepastnineyears,thousandsofdentistsandtheirteamshavebeenworkingwithourhandbook.Inaddition,manyuniversitiesandtrainingcentresutilisetheguidelinesforprecisionimpressiontakingasabenchmark.Manyofthedentistsespeciallyvaluetheclearandconcisestep-wiseprocedures,aswellasthesupportivefunctionforvocationaltrainingandfurthereducationinpractice.Thisthirdeditionputsevenstrongerfocusontheprocedureofimpressiontakingsincethisisthemostimportantstepforultimatelyproducinghigh-qualityaestheticresto-rations.Theimprovementsachievedthroughmaterialscienceanddentalprocedures,aswellasimportantchangesintheworkflow,promptedustoupdatealmostallthechapters.
3MESPEfeelsverymuchindebtedtoProf.Dr.med.dent.Wöstmann,oneoftheauthorsofthefirstandsecondeditions,forhiscompetent,clinicalandprocess-orientedview.Chapters1,2,4and6–11verymuchbenefitfromhisoutstandingclinicalexpertise.3MESPEwishesalsotothankDr.Powerswhoinchapter3linksthechemistryofimpressioningmaterialstotheirclinicallyrelevantpropertiesinanintelligibleanduser-friendlyway.
3MESPEcomplementstheirworkwithourlongstandingexpertiseinimpressionmaterialmixingtechnologyinchapter5.
Wehopethatyoufindthechangesmadetothelatesteditionwillhelpyoutofurtherimprovethequalityofyourimpressionsandtherestorationsyouproduceinpracticeortraining.
Dr.AlfredViehbeck3MESPEGlobalTechnicalDirectorSt.Paul,MN,USAandSeefeld,GermanyMay2008
Biographical sketch
BerndWöstmann,Prof.Dr.med.dent.Dr.WöstmanngraduatedfromtheUniversityofMünster,Germanyin1985.From1986to1992hewasassistantdoctorandfrom1993to1995assistantmedicaldirectoroftheDepartmentofProsthodonticsoftheWestphalianWilhelms-University,Münster,Germany.In1995hewasappointedassistantprofessorandin1998professorattheJustus-Liebig-UniversityinGiessen,Germany,whereheiscurrentlyholdingalifetimeprofessorshipforClinicalDentalMaterialsSci-encesandGerodontology.Hismainareasofinterestaredentalelastomersandrelatedaspectsofmaterialscience,especiallyimpressiontakingindentistry.Heisalsoworkingingerodontologyandimplantology.Dr.WöstmannisamemberofseveralscientificorganisationsincludingtheIADRandalsoseveralDIN-ISOworkinggroups.HeiscurrentlyPresident-electoftheEuropeanCollegeofGerodontology(ECG)andsecondvicepresidentoftheHeadAssociationoftheGermanGeriatricScientificSocieties(DVGG).Dr.Wöstmannistheauthorofmorethan200scientificarti-cles,abstracts,books,andchapters.Heservesontheeditorialboardsofmanydentaljournalsandhasgivenmorethan400scientificandprofessionalpresentationsandlectures.Dr.WöstmannhasbeenawardedtheFriedrich-Hartmut-DostAwardin1999forexcellenteducationindentistryandco-authoredseveralpresentationsthathavebeenawardedbytheGermanProsthodonticSociety(DGZPW),theGermanGeriatricSociety(DGG)andtheAustrianGeriatricSociety.
Dental Consultants, Inc. (THE DENTAL ADVISOR) 3110 W. Liberty Ann Arbor, MI 48103 Phone: 734-665-2020 (x113) Fax: 734-665-1648 E-mail: [email protected] www.dentaladvisor.com
JohnM.Powers,Ph.D.Dr.PowersgraduatedfromtheUniversityofMichiganwithaB.S.inchemistryin1967andaPh.D.indentalmaterialsandmechanicalengineeringin1972.HeisseniorvicepresidentofDentalConsultants,Inc.,andeditorofTheDentalAdvisor,adentalnewsletter.HeisalsoProfessorofOralBiomaterials,DepartmentofRestorativeDentistryandBiomaterials,andSeniorScientistoftheHoustonBiomaterialsResearchCenterattheUniversityofTexasDentalBranchatHouston.HeisalsoamemberofthefacultyofGraduateSchoolofBiomedicalSciencesandAdjunctPro-fessorattheUniversityofMichiganSchoolofDentistry,UniversityofRegensburgandtheLudwig-Maximilians-UniversityMunich.Heisactiveintheappliedandbasicresearchofbondingtodentalsubstrates,colourandopticalpropertiesofaestheticmaterials,andphysicalandmechanicalpropertiesofdentalcements,compositesandotherrestorativematerials.Dr.PowersiscurrentlytheCounciloroftheDMG/IADRandChairofANSI/ADAWorkingGroupsonwaxesandcements.Dr.Powersistheauthorofmorethan875scientificarticles,abstracts,books,andchapters.Heisco-authorofthetextbook,DentalMaterials–PropertiesandManipulation,andco-editorofCraig’sRestorativeDentalMaterials.Heservesontheeditorialboardsofmanydentaljournals.HehasgivennumerousscientificandprofessionalpresentationsintheUnitedStates,Europe,Asia,MexicoandSouthAmerica.
Prof. Dr. med. dent. Bernd Wöstmann Department of Prosthodontics – Dental Clinic Justus-Liebig-University Giessen Schlangenzahl 14 35392 Giessen Germany Phone: +49 641 99-46 143 /-46 150 Fax: +49 641 99-46 139 E-mail: [email protected].
uni-giessen.de
| 3

4 |
Contents | 5
Aguidelineforexcellentimpressionsintheoryandpractice
Preface 2
Biographical sketch 3
1. Clinical importance of the precision impression 61.1. Introduction 61.2. Reasonsfordiscrepancybetweenlaboratoryresultsandprecisioninclinicalsituations 81.3. Improvementofresultsbystandardisation 81.4. Standardisationinthedailyroutine–dentalpracticeanddentallaboratory 9
2. Clinical parameters influencing impression taking 102.1. Periodontalstatusandoralhygiene 102.2. Waitingperiodbetweenpreparationandimpression 102.3. Preparationoftheoperativefield 112.4. Anaesthesia 122.5. Choiceoftrayandspecificimpressiontechniques 122.6. Removaloftheimpressionfromthemouth 13
3. Properties of today’s impression materials 143.1. Historyofprecisionimpressions 143.2. Additioncuringprecisionimpressionmaterials 153.3. Condensationcuringelastomers 183.4. Impressionmaterialsforpreliminaryimpressions 193.5. Materialincompatibilitiesandimpressiondisposal 203.6. OverviewofmaterialtypesandconsistenciesaccordingtoISO4823:2000 21
4. Impression trays 224.1. Choiceoftray 224.2. Stocktraysforfullarchimpressions 224.3. Stocktrayswithoptimisedfit 244.4. Customtrays 244.5. Dual-archtrays 264.6. Trayadhesive 26
5. Mixing of impression materials 275.1. Hand-mixingofimpressionmaterials 275.2. Handdispensersystem 295.3. Automaticmixingsystem 30
6. Impression techniques 336.1. 1-stepimpressiontechniques 336.2. 2-stepimpressiontechniques 346.3. Takingtheimpression 36
7. Indications 387.1. Orthodonticsplints 387.2. Veneers 387.3. Adhesivebridges 397.4. Inlaysandpartialcrowns 397.5. Singlecrowns 407.6. Bridges 407.7. Combinationdentures 417.8. Implants 427.9. Summaryindicationsandtechniques 43
8. Disinfection 44
9. Storage of the impression and transport to the dental lab 45
10. Fabrication of the stone model 4610.1. Standardisationofthemodelfabrication 4610.2. Modelsystems 4610.3. Timingofthemodelfabrication 47
11. Conclusion 48
12. Impression taking in the clinical workflow – Overview 49
13. Literature 50
14. Glossary 53
15. Overview 3M ESPE impression materials 54
6 | Precisionimpressions
1. Clinical importance of the precision impression (B.Wöstmann)
1.1. IntroductionRestorationswhichfitexactlyandcanbeinsertedwithoutanyfurthercorrectionsarehighonthelistofeverydentist.Exactfittingrestorationsdonotonlyfacilitatemoreefficientandfasterwork-ing,theyalsoaidperiodontalprophylaxis.Furthermore,today’saestheticallysuperiorrestorationsdorequireexactfitting.Afullceramiccrownsurroundedbychronicgingivitiswithitscharacteristicdiscolourationcausedbyawidelyprotrudingcrownmarginistotallyunacceptable.Theimpressionisanimportantstepintheprocedureofobtainingaperfectrestoration.Itistheaimoftheimpressiontoproduceadimensionallystable“negative”whichcanserveasthecastmouldforamodel.Duetothefactthatindirectrestorationsareclassicallyproducedinthedentallaboratory,itisinevitablethatanoptimalprecisefitofthelaboratory-madeapplianceisonlygivenifthemodelexactlymatchestheoriginalsituation.DespiterapidtechnicalprogressinthefieldofCAD/CAMsystems,theimpressionremainsimmenselyimportanttoprostheticdentistry.Atleastinthenearfuture,theimpressionwillcontinueitsvitalroletransportinginformationfromthedentisttothedentallab.MostCAD/CAMsystemsavailabletodaystartfromthemodeland,thus,alsorequireprimarilyanimpression.Despitemanyefforts,theconventionalimpressionprocesshasnotyetbeenreplacedbymoremodernreproductionprocedures–suchas“photo-graphic”impressionwiththehelpofanintra-oralscan,e.g.withtheCEREC(SironaDentalSystems).However,3D-imagingprocedureswillincreasinglybeused(e.g.3MESPELava™Chair-sideOralScannerC.O.S.)inthefuture.Theseinnovationsarequitepromising.However,especiallyfordeepsubgingivalareasandareasdifficulttoaccess,theconventionalimpressionremainsanecessaryandindispensableprocedurestepindentaltreatment.
Current trends in digital impressioningOverthelast100years,elastomericimpressionmaterialswerecontinuouslydevelopedandoptimizedforimprovedprecision,patientcomfortandeaseofuse.Modernmaterialsarerobust,precise,fast,hydrophilic,andcanbeautomaticallymixed–butstillthepatientneedstokeepafilledimpressiontrayinthemouthforsomeverylongminutes,andexternalfactors,e.g.temperature,canimpactthefinalresult.
Thus,digitalapproachesweremadetocircumventtheseproblems.Thefirstopticalimpressioningsystemwasmarketedinthe1980saspartoftheCERECsystem(SironaDentalSystems).TheLava™ChairsideOralScannerC.O.S.(3MESPE)uses3D-in-MotionTechnology.Thistechnique,incontrasttoknown“pointandclick”systems,capturescontinuous3Dvideoimagesanddisplaystheseimagesinrealtimeonatouchscreenmonitor.Thesedigitalimpressionswillbesenttothedentallabwhereatechnicianwilldigitallycutandmarkthemargin.Modelsforthelabtechnicianwillbemadewithdigitalprecisionusingstereo-lithography.Whilemodelfabricationstillisanecessaryworkstep,itmightbecomelessimportantinthefuture.3MESPEalreadymanufacturesLava™ZirconiacopingswithCAD/CAMtechnology.Inthefuturethesecopingscouldbemilledbasedonadigitalimpression.
Precisionimpressions | 7
Marginal accuracy: what is necessary and what is possible?Duetonumerousmaterial-relatedaspects,anidenticalreplicationoftheoriginalsituationisnotpossiblewiththematerialsandmethodsusedintoday‘sdentistry.Infact,impressioningisaconstanttightropewalkbetweenluminathateithercameouttoosmallortoolarge,andthus,betweenoversizedorundersizedmodelabutments.Theequivalentisinthelumenofacrown,whichiseithertoolargeortoosmall.Crownsthataretoolargehaveintolerablemarginalgapsandiftoosmall,crownsdonotreachthepreparationmargin.
Thebiologicaltoleranceformarginaldiscrepanciesisalmostunknown,althoughboththecorrela-tionbetweenmarginalaccuracyandperiodontaldamage1;2,andtheappearanceofsecondarycariesinthecaseofinaccuratefit3hasbeenproven.
Themarginofarestorationisthecriticalpoint,sinceinadequaterestorationmarginscanhardlybecorrectedafterwards.Occlusalinterferencesaswellasinaccuratefitaroundtheapproximalcon-tactscanbecorrectedmucheasier–independentofwhethertheseareclassicalmetalrestorationsorCAD/CAM-producedzirconiumoxideframeworks.Thus,thereproductionofthepreparationmargininanimpressionisanecessaryrequirementinordertoachievegoodmarginalquality.Invitro,themarginalprecisionofadentalrestorationisapprox.50µmonaverage4–6.However,thislevelofprecisioncanrarelybemetclinically.Thisdivergenceappliesmainlytorestorationswithsubgingivalorparagingivalmarginareas.Ifthecrownmarginiscompletelysupragingival,itispossibletoobtainaccuracieswhicharequitecomparablewiththeresultsfromlabtests.Thishasbeenimpressivelyproveninseveralstudies7–12.
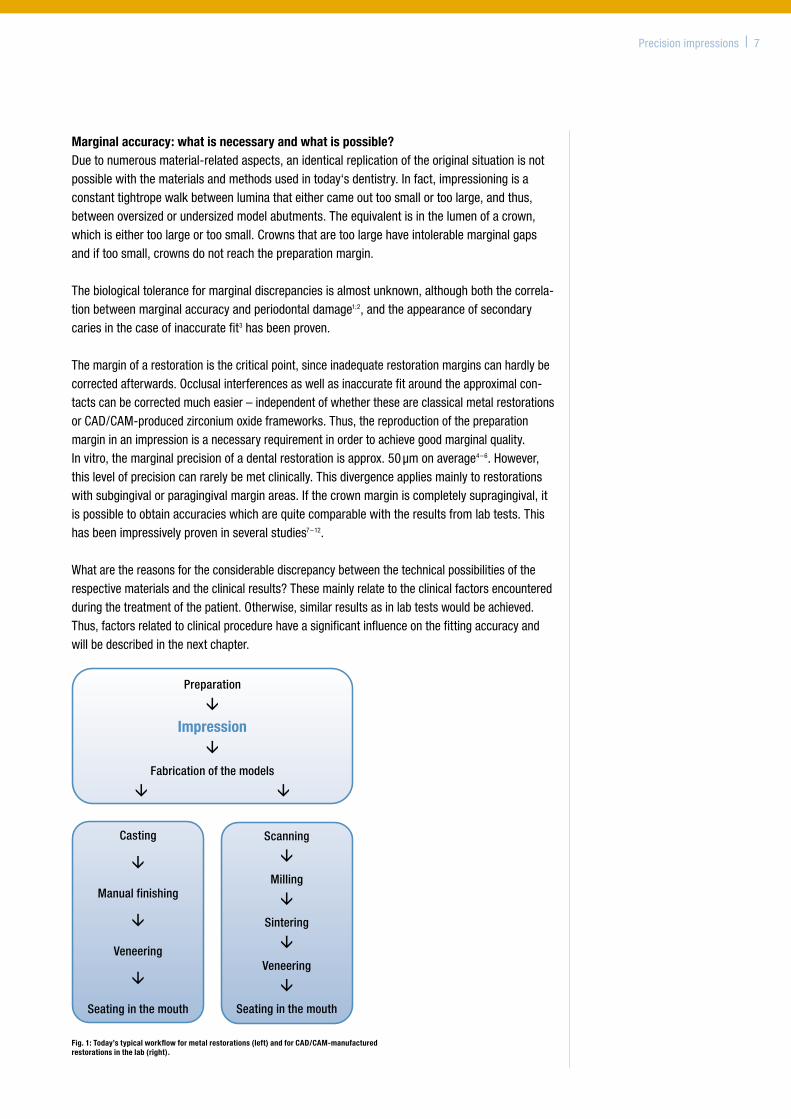
Whatarethereasonsfortheconsiderablediscrepancybetweenthetechnicalpossibilitiesoftherespectivematerialsandtheclinicalresults?Thesemainlyrelatetotheclinicalfactorsencounteredduringthetreatmentofthepatient.Otherwise,similarresultsasinlabtestswouldbeachieved.Thus,factorsrelatedtoclinicalprocedurehaveasignificantinfluenceonthefittingaccuracyandwillbedescribedinthenextchapter.
Preparation
‚
Impression‚
Fabrication of the models
‚ ‚
Scanning
‚
Milling
‚
Sintering
‚
Veneering
‚
Seating in the mouth
Casting
‚
Manual finishing
‚
Veneering
‚
Seating in the mouth
Fig. 1: Today’s typical workflow for metal restorations (left) and for CAD/CAM-manufactured restorations in the lab (right).
8 | Precisionimpressions
1.2. Reasonsfordiscrepancybetweenlaboratoryresultsandprecisioninclinicalsituations
ThepreparationofafixeddentalrestorationwiththehelpofprecisionimpressionmaterialsrequiresseveraltreatmentandlaboratorystepsindependentofwhetheraconventionalorCAD/CAMtechniqueischosen.Thesamesourcesofpotentialerrorapplytoallfixedrestorations.Wewillusetheexampleofacrownforexplanation.
Thelumenofacrownhastobealittlebitlargerthantheoriginalabutmentsothattherestorationcanbecemented,soitisdesirabletoachieveaslightenlargementofthecrownlumeninthecourseoftheworkflowfromimpressiontocrown.However,duetomaterial-relatedreasons(likeshrinkageofcastgypsumorimpressionmaterial)thisisnotpossible.Usually,theknowndimensionalerrorsoftheimpressionarecompensatedbytheexperienceddentallabbyapplyingspacersorchangingthesettingexpansionoftheembeddingmaterialtoachievewell-fittingrestorations.
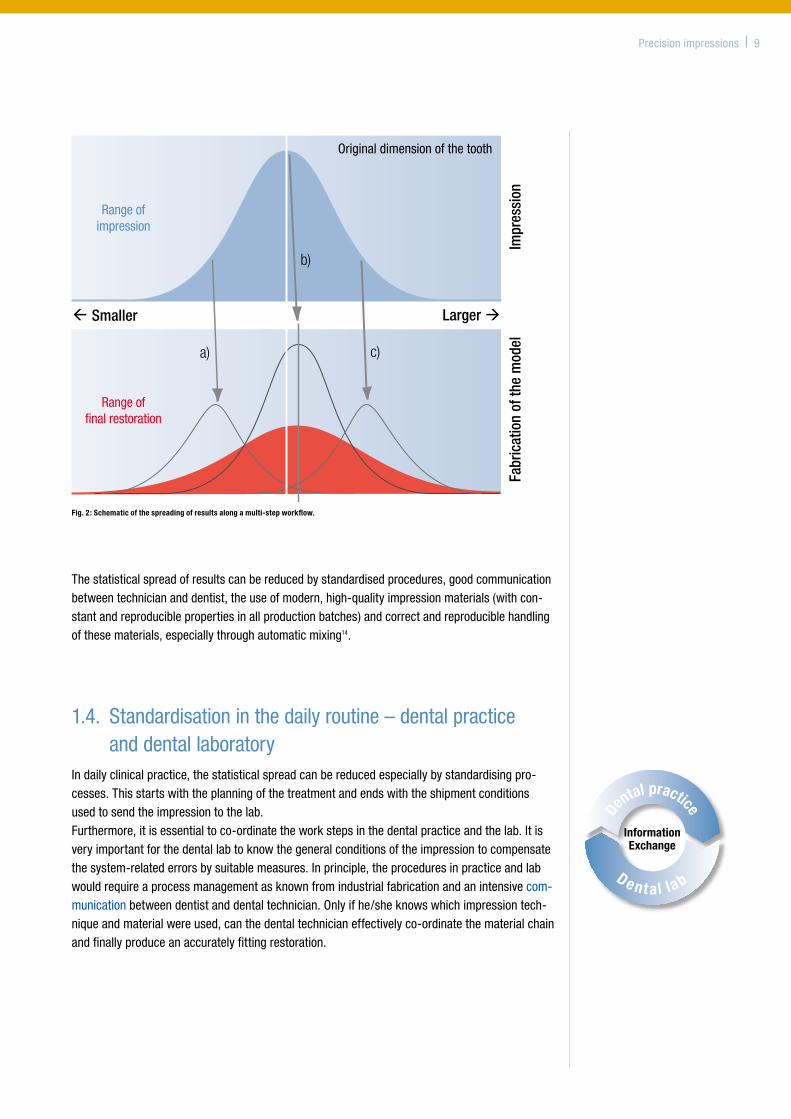
1.3. ImprovementofresultsbystandardisationToachievereproducibleresultswithregardtoaccuratelyfitting,fixedrestorationsonemuststandardisetheprocessfromthepreparationofthetoothtotheseatingofthefinalrestoration13.Fig.2shows–inasimplifiedmanner–thatthedimensionoftheabutment,asitisreproducedintheimpression,approximatelycorrespondstoanormaldistribution(Gaussiandistribution).Itswidthdependsontheconsistencyorrathertheinconsistencyoftheinitialconditionslikeimpres-siontechnique,traychoice,temperature,etc.Indailypracticeitisscarcelypossibletoevaluatetheactualdimensionofthereproducedabutmentintheimpression,sincesuchdiscrepanciesarerarelyobvioustothenakedeye.
Thesubsequentworkstepsinthelab(fabricationofthemodel,carving,embedding,casting)inprinciplefollowthesamescheme.Thedifferenceisthatthepositionofthecurvemaximumnolongercorrespondstotheoriginaltoothbuttothepositiondeliveredintheimpression(e.g.positionsa,borc,Fig.2).
Atthispointtheproblemisclear:witheachfurtherworkstepthespreadingoftheresultsbecomeslarger.Itcanneverbecomesmaller(Fig.2redcurvebelow).
Thus,itisawidespreadfallacythatthedeviationsresultingfrominsufficientstandardisation“levelout”ontheirown22.
Precisionimpressions | 9
Thestatisticalspreadofresultscanbereducedbystandardisedprocedures,goodcommunicationbetweentechniciananddentist,theuseofmodern,high-qualityimpressionmaterials(withcon-stantandreproduciblepropertiesinallproductionbatches)andcorrectandreproduciblehandlingofthesematerials,especiallythroughautomaticmixing14.
1.4. Standardisationinthedailyroutine–dentalpracticeanddentallaboratory
Indailyclinicalpractice,thestatisticalspreadcanbereducedespeciallybystandardisingpro-cesses.Thisstartswiththeplanningofthetreatmentandendswiththeshipmentconditionsusedtosendtheimpressiontothelab.Furthermore,itisessentialtoco-ordinatetheworkstepsinthedentalpracticeandthelab.Itisveryimportantforthedentallabtoknowthegeneralconditionsoftheimpressiontocompensatethesystem-relatederrorsbysuitablemeasures.Inprinciple,theproceduresinpracticeandlabwouldrequireaprocessmanagementasknownfromindustrialfabricationandanintensivecom-municationbetweendentistanddentaltechnician.Onlyifhe/sheknowswhichimpressiontech-niqueandmaterialwereused,canthedentaltechnicianeffectivelyco-ordinatethematerialchainandfinallyproduceanaccuratelyfittingrestoration.
Dental practice
D ent al lab
InformationExchange
Fig. 2: Schematic of the spreading of results along a multi-step workflow.
2. Clinical parameters influencing impression taking (B.Wöstmann)
Systematicstandardisationcanreducethenumberofretakesandcorrections.Additionally,thefinalsuccessofanimpressionisstronglyinfluencedbytheclinicalsituationandisindividualforeachpatient.
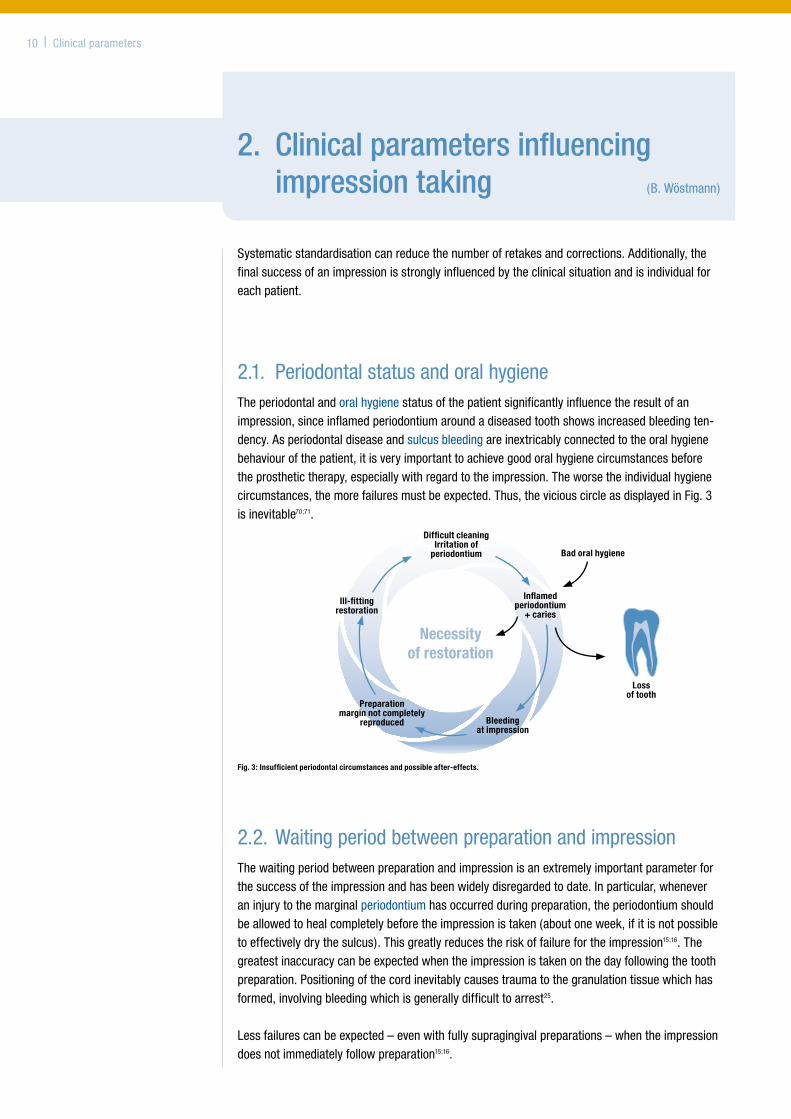
2.1. PeriodontalstatusandoralhygieneTheperiodontalandoralhygienestatusofthepatientsignificantlyinfluencetheresultofanimpression,sinceinflamedperiodontiumaroundadiseasedtoothshowsincreasedbleedingten-dency.Asperiodontaldiseaseandsulcusbleedingareinextricablyconnectedtotheoralhygienebehaviourofthepatient,itisveryimportanttoachievegoodoralhygienecircumstancesbeforetheprosthetictherapy,especiallywithregardtotheimpression.Theworsetheindividualhygienecircumstances,themorefailuresmustbeexpected.Thus,theviciouscircleasdisplayedinFig.3isinevitable70;71.
Fig. 3: Insufficient periodontal circumstances and possible after-effects.
2.2.WaitingperiodbetweenpreparationandimpressionThewaitingperiodbetweenpreparationandimpressionisanextremelyimportantparameterforthesuccessoftheimpressionandhasbeenwidelydisregardedtodate.Inparticular,wheneveraninjurytothemarginalperiodontiumhasoccurredduringpreparation,theperiodontiumshouldbeallowedtohealcompletelybeforetheimpressionistaken(aboutoneweek,ifitisnotpossibletoeffectivelydrythesulcus).Thisgreatlyreducestheriskoffailurefortheimpression15;16.Thegreatestinaccuracycanbeexpectedwhentheimpressionistakenonthedayfollowingthetoothpreparation.Positioningofthecordinevitablycausestraumatothegranulationtissuewhichhasformed,involvingbleedingwhichisgenerallydifficulttoarrest25.
Lessfailurescanbeexpected–evenwithfullysupragingivalpreparations–whentheimpressiondoesnotimmediatelyfollowpreparation15;16.
10 | Clinicalparameters
Inflamed periodontium
+ caries
Necessity of restoration
Preparation margin not completely
reproduced Bleeding at impression
Loss of tooth
Bad oral hygiene
Difficult cleaning Irritation of
periodontium
Ill-fitting restoration
Clinicalparameters | 11
2.3.PreparationoftheoperativefieldRetraction Anessentialrequirementforasuccessfulimpressionistheaccuratereproductionofthepreparedteeth.Onlythencanthepreparationmarginbedefinedunequivocallyonthestonemodel.Youcanonlyreproducewhatisaccessible.Withsupragingivallylocatedpreparationskeepingtheareatobeimpressioneddryandaccessibleisusuallyquiteeasy8;17.However,ifatoothiscrownedtopreserveit,itisoftendeeplydestroyedandthepreparationmarginisfullyoratleastpartlysubgingival.Ifthetoothshouldserveasabridgeabutmentitisthequestionofsufficientretentionofthebridgewhichforcesaparagingivalorsubgingivalpreparation.
Ifthepreparationmarginisnotaccessibleitcaneitherbecomesupragingivalbysurgicaltreatmentand/or–preferably–thesulcuscantemporarilybeextendedwitharetractionmaterial.
Haemostaticpropertiesoftheretractionmaterialarenotrequiredwhenhealthyperiodontalcondi-tionshavebeenachievedwithgoodoralhygieneandsubsequenttissuemanagement.However,sometimesitisnecessarytoworkwithpre-impregnatedretractioncordsdespitetheuseoflocalanaestheticcontainingavasoconstrictor(warning:cardio-vascularriskpatients).Pre-impregnatedretractioncordsoraddedretractionliquids–especiallybasedonmetalsalts–caninteractwithimpressionmaterialsandpreventtheirsettingprocess18;19.
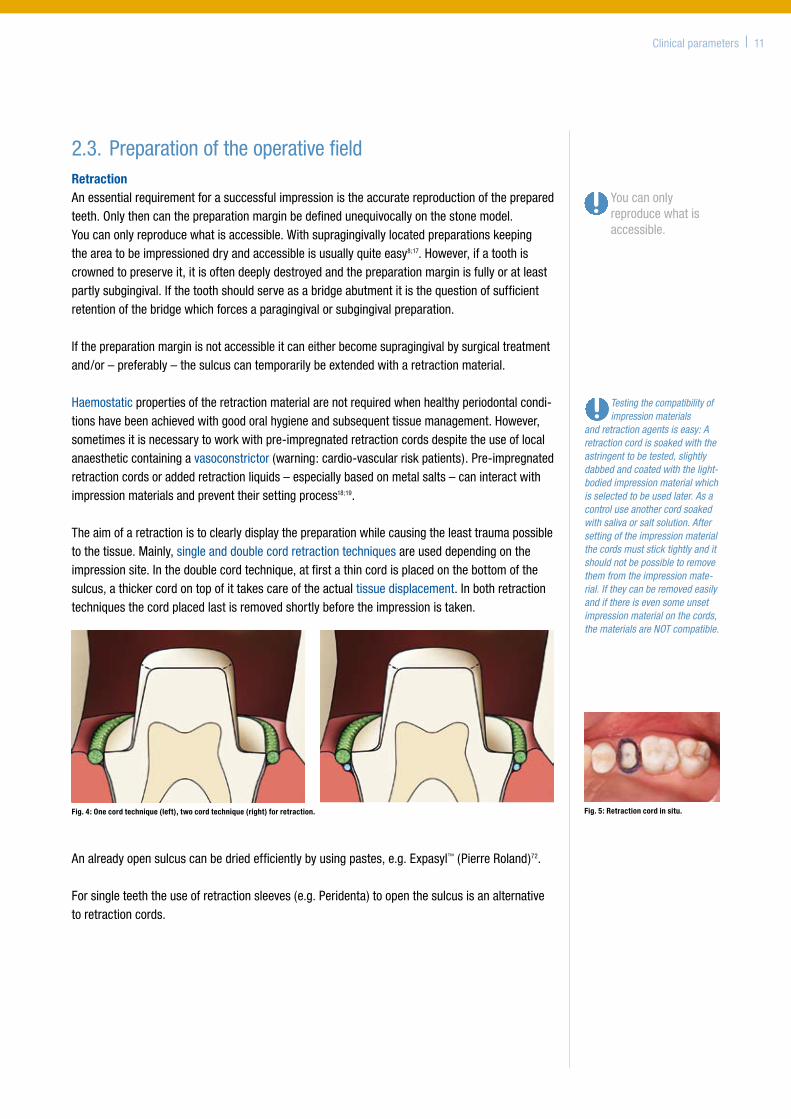
Theaimofaretractionistoclearlydisplaythepreparationwhilecausingtheleasttraumapossibletothetissue.Mainly,singleanddoublecordretractiontechniquesareuseddependingontheimpressionsite.Inthedoublecordtechnique,atfirstathincordisplacedonthebottomofthesulcus,athickercordontopofittakescareoftheactualtissuedisplacement.Inbothretractiontechniquesthecordplacedlastisremovedshortlybeforetheimpressionistaken.
Analreadyopensulcuscanbedriedefficientlybyusingpastes,e.g.Expasyl™(PierreRoland)72.
Forsingleteeththeuseofretractionsleeves(e.g.Peridenta)toopenthesulcusisanalternativetoretractioncords.
Testing the compatibility of impression materials
and retraction agents is easy: A retraction cord is soaked with the astringent to be tested, slightly dabbed and coated with the light-bodied impression material which is selected to be used later. As a control use another cord soaked with saliva or salt solution. After setting of the impression material the cords must stick tightly and it should not be possible to remove them from the impression mate-rial. If they can be removed easily and if there is even some unset impression material on the cords, the materials are NOT compatible.
Youcanonlyreproducewhatisaccessible.
Fig. 5: Retraction cord in situ.Fig. 4: One cord technique (left), two cord technique (right) for retraction.
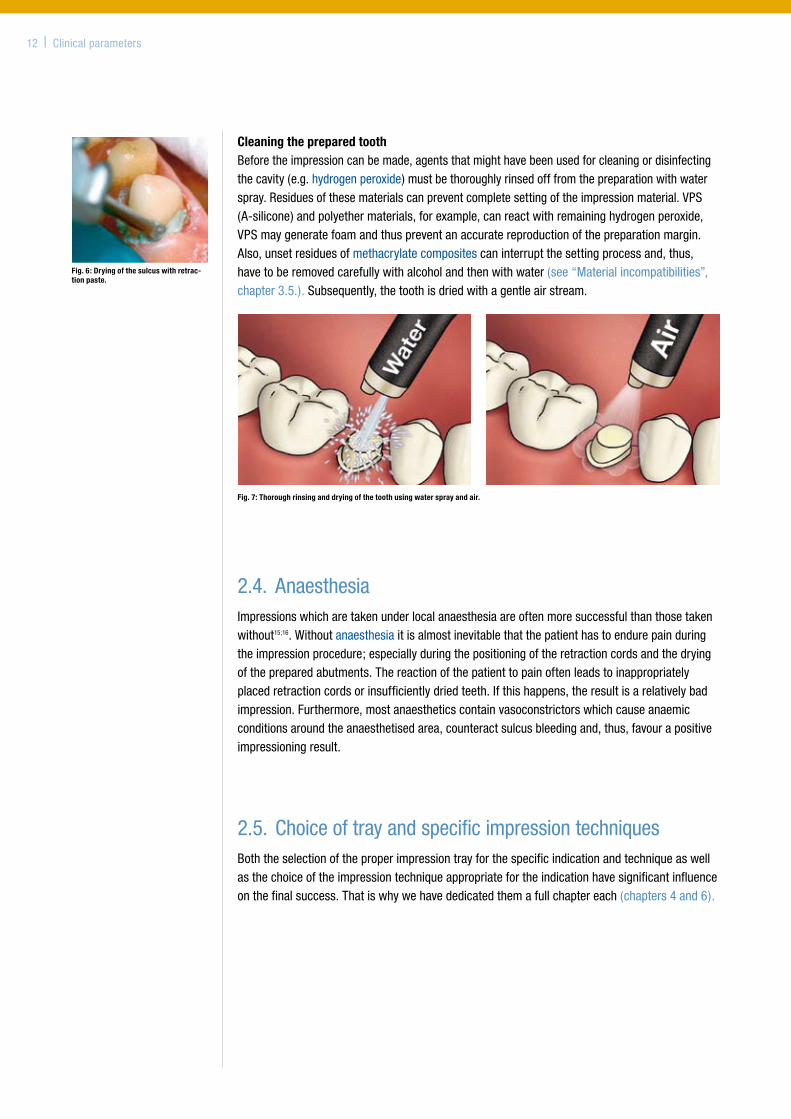
Cleaning the prepared toothBeforetheimpressioncanbemade,agentsthatmighthavebeenusedforcleaningordisinfectingthecavity(e.g.hydrogenperoxide)mustbethoroughlyrinsedofffromthepreparationwithwaterspray.Residuesofthesematerialscanpreventcompletesettingoftheimpressionmaterial.VPS(A-silicone)andpolyethermaterials,forexample,canreactwithremaininghydrogenperoxide,VPSmaygeneratefoamandthuspreventanaccuratereproductionofthepreparationmargin.Also,unsetresiduesofmethacrylatecompositescaninterruptthesettingprocessand,thus,havetoberemovedcarefullywithalcoholandthenwithwater(see“Materialincompatibilities”,chapter3.5.).Subsequently,thetoothisdriedwithagentleairstream.
Fig. 7: Thorough rinsing and drying of the tooth using water spray and air.
2.4. AnaesthesiaImpressionswhicharetakenunderlocalanaesthesiaareoftenmoresuccessfulthanthosetakenwithout15;16.Withoutanaesthesiaitisalmostinevitablethatthepatienthastoendurepainduringtheimpressionprocedure;especiallyduringthepositioningoftheretractioncordsandthedryingofthepreparedabutments.Thereactionofthepatienttopainoftenleadstoinappropriatelyplacedretractioncordsorinsufficientlydriedteeth.Ifthishappens,theresultisarelativelybadimpression.Furthermore,mostanaestheticscontainvasoconstrictorswhichcauseanaemicconditionsaroundtheanaesthetisedarea,counteractsulcusbleedingand,thus,favourapositiveimpressioningresult.
2.5.ChoiceoftrayandspecificimpressiontechniquesBoththeselectionoftheproperimpressiontrayforthespecificindicationandtechniqueaswellasthechoiceoftheimpressiontechniqueappropriatefortheindicationhavesignificantinfluenceonthefinalsuccess.Thatiswhywehavededicatedthemafullchaptereach(chapters4and6).
Fig. 6: Drying of the sulcus with retrac-tion paste.
12 | Clinicalparameters
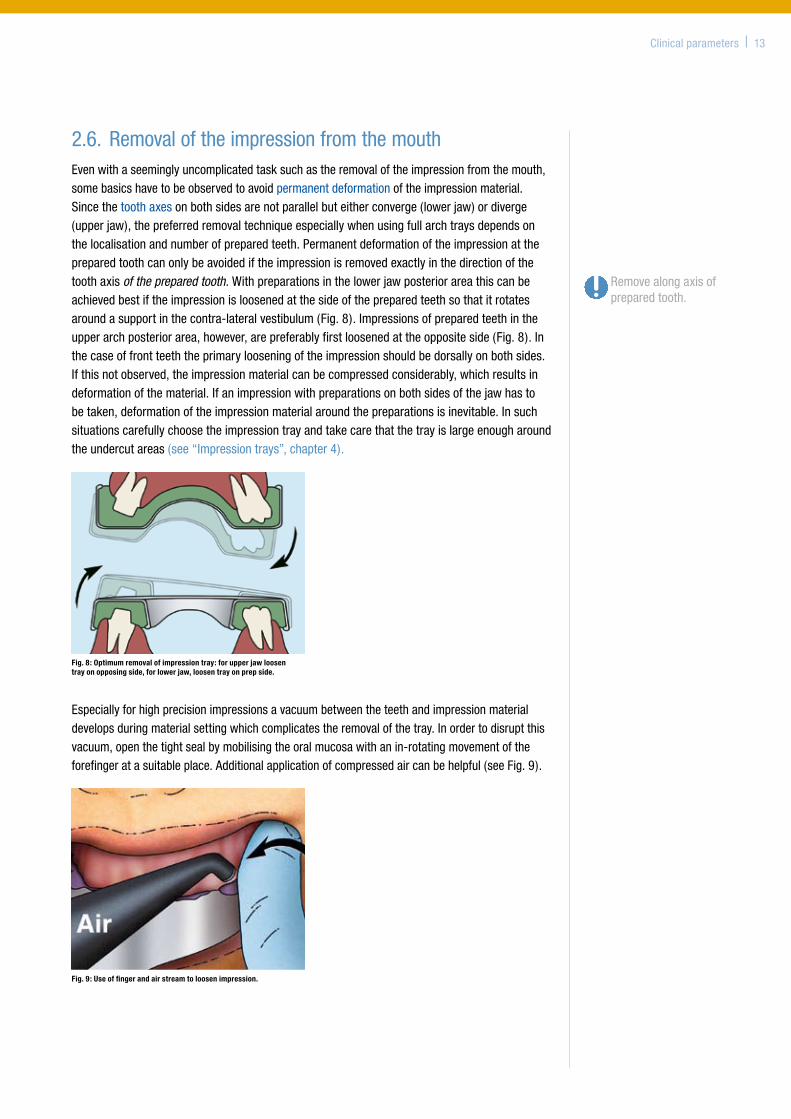
2.6.RemovaloftheimpressionfromthemouthEvenwithaseeminglyuncomplicatedtasksuchastheremovaloftheimpressionfromthemouth,somebasicshavetobeobservedtoavoidpermanentdeformationoftheimpressionmaterial.Sincethetoothaxesonbothsidesarenotparallelbuteitherconverge(lowerjaw)ordiverge(upperjaw),thepreferredremovaltechniqueespeciallywhenusingfullarchtraysdependsonthelocalisationandnumberofpreparedteeth.Permanentdeformationoftheimpressionatthepreparedtoothcanonlybeavoidediftheimpressionisremovedexactlyinthedirectionofthetoothaxisof the prepared tooth.Withpreparationsinthelowerjawposteriorareathiscanbeachievedbestiftheimpressionisloosenedatthesideofthepreparedteethsothatitrotatesaroundasupportinthecontra-lateralvestibulum(Fig.8).Impressionsofpreparedteethintheupperarchposteriorarea,however,arepreferablyfirstloosenedattheoppositeside(Fig.8).Inthecaseoffrontteeththeprimarylooseningoftheimpressionshouldbedorsallyonbothsides.Ifthisnotobserved,theimpressionmaterialcanbecompressedconsiderably,whichresultsindeformationofthematerial.Ifanimpressionwithpreparationsonbothsidesofthejawhastobetaken,deformationoftheimpressionmaterialaroundthepreparationsisinevitable.Insuchsituationscarefullychoosetheimpressiontrayandtakecarethatthetrayislargeenougharoundtheundercutareas(see“Impressiontrays”,chapter4).
Especiallyforhighprecisionimpressionsavacuumbetweentheteethandimpressionmaterialdevelopsduringmaterialsettingwhichcomplicatestheremovalofthetray.Inordertodisruptthisvacuum,openthetightsealbymobilisingtheoralmucosawithanin-rotatingmovementoftheforefingeratasuitableplace.Additionalapplicationofcompressedaircanbehelpful(seeFig.9).
Clinicalparameters | 13
Removealongaxisofpreparedtooth.
Fig. 8: Optimum removal of impression tray: for upper jaw loosen tray on opposing side, for lower jaw, loosen tray on prep side.
Fig. 9: Use of finger and air stream to loosen impression.
3. Properties of today’s impression materials (J.M.Powers)
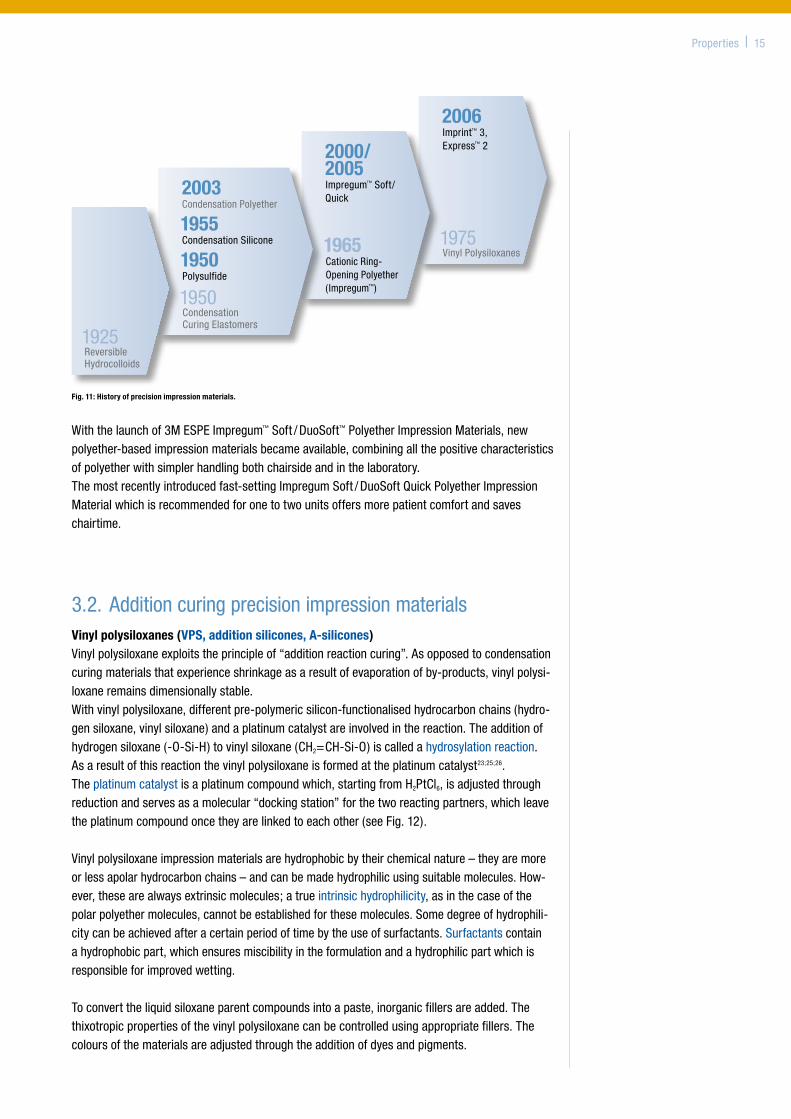
3.1. HistoryofprecisionimpressionsTheintroductionofreversiblehydrocolloidsinthemid-1930sheraldedanewageintheimpressionsector.Forthefirsttimetheimpressionofundercutsbecamepossible.Withtheappearanceofpolysulfidesatthebeginningofthe1950s,anelastomericimpressionmaterialwasusedinden-tistryforthefirsttime.Around55yearsagotheworldofdentistrysawtheintroductionofacate-goryofmaterials–theC-typesilicones(condensation-cured)–which,likeanothercondensation-curedclassofmaterials,thepolysulfides,werenotoriginallyintendedfororalapplications.
Thegreatdisadvantageoftheseproductsstillremains:shrinkageintrinsictothesystem–beitduetotheevaporationofwaterwiththehydrocolloidsoroflow-molecularside-productsinthecaseofthecondensationcuredelastomers20;21.
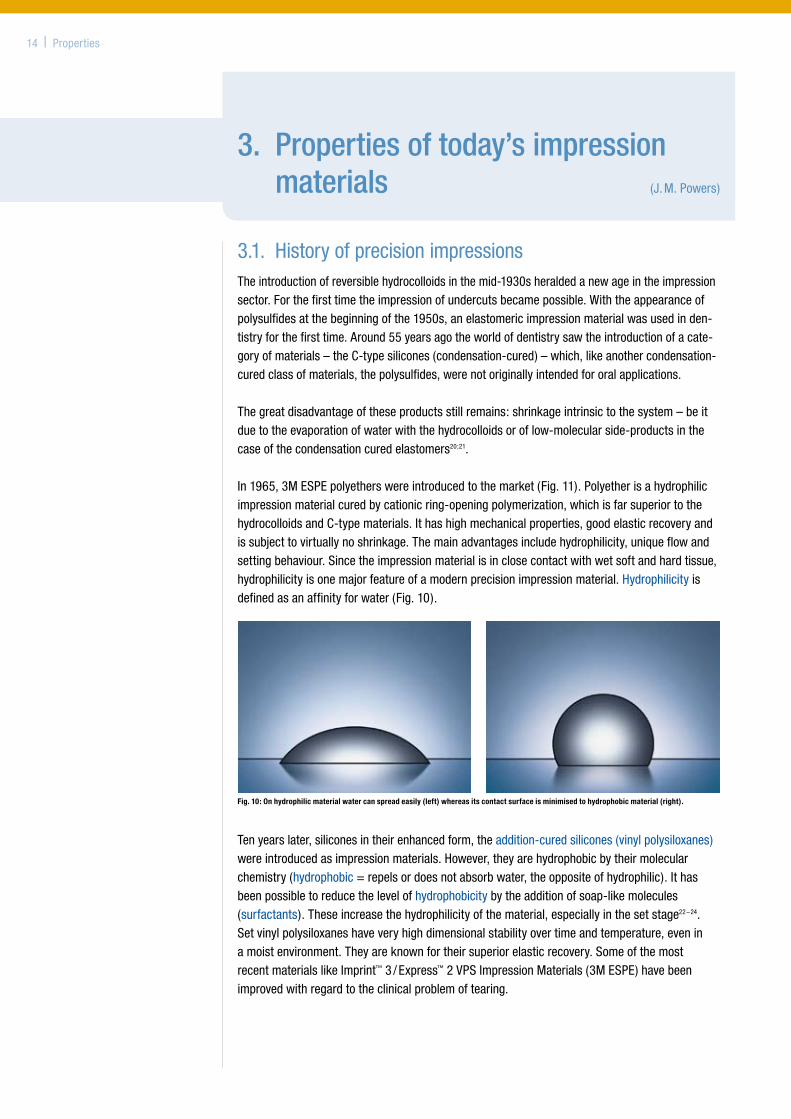
In1965,3MESPEpolyetherswereintroducedtothemarket(Fig.11).Polyetherisahydrophilicimpressionmaterialcuredbycationicring-openingpolymerization,whichisfarsuperiortothehydrocolloidsandC-typematerials.Ithashighmechanicalproperties,goodelasticrecoveryandissubjecttovirtuallynoshrinkage.Themainadvantagesincludehydrophilicity,uniqueflowandsettingbehaviour.Sincetheimpressionmaterialisinclosecontactwithwetsoftandhardtissue,hydrophilicityisonemajorfeatureofamodernprecisionimpressionmaterial.Hydrophilicityisdefinedasanaffinityforwater(Fig.10).
Tenyearslater,siliconesintheirenhancedform,theaddition-curedsilicones(vinylpolysiloxanes)wereintroducedasimpressionmaterials.However,theyarehydrophobicbytheirmolecularchemistry(hydrophobic=repelsordoesnotabsorbwater,theoppositeofhydrophilic).Ithasbeenpossibletoreducethelevelofhydrophobicitybytheadditionofsoap-likemolecules(surfactants).Theseincreasethehydrophilicityofthematerial,especiallyinthesetstage22–24.Setvinylpolysiloxaneshaveveryhighdimensionalstabilityovertimeandtemperature,eveninamoistenvironment.Theyareknownfortheirsuperiorelasticrecovery.SomeofthemostrecentmaterialslikeImprint™3/Express™2VPSImpressionMaterials(3MESPE)havebeenimprovedwithregardtotheclinicalproblemoftearing.
14 | Properties
Fig. 10: On hydrophilic material water can spread easily (left) whereas its contact surface is minimised to hydrophobic material (right).
1975VinylPolysiloxanes
2006 Imprint™3,Express™22000/
2005 Impregum™Soft/Quick
1965 CationicRing-OpeningPolyether( Impregum™)
Withthelaunchof3MESPEImpregum™Soft/DuoSoft™PolyetherImpressionMaterials,newpolyether-basedimpressionmaterialsbecameavailable,combiningallthepositivecharacteristicsofpolyetherwithsimplerhandlingbothchairsideandinthelaboratory.Themostrecentlyintroducedfast-settingImpregumSoft/DuoSoftQuickPolyetherImpressionMaterialwhichisrecommendedforonetotwounitsoffersmorepatientcomfortandsaveschairtime.
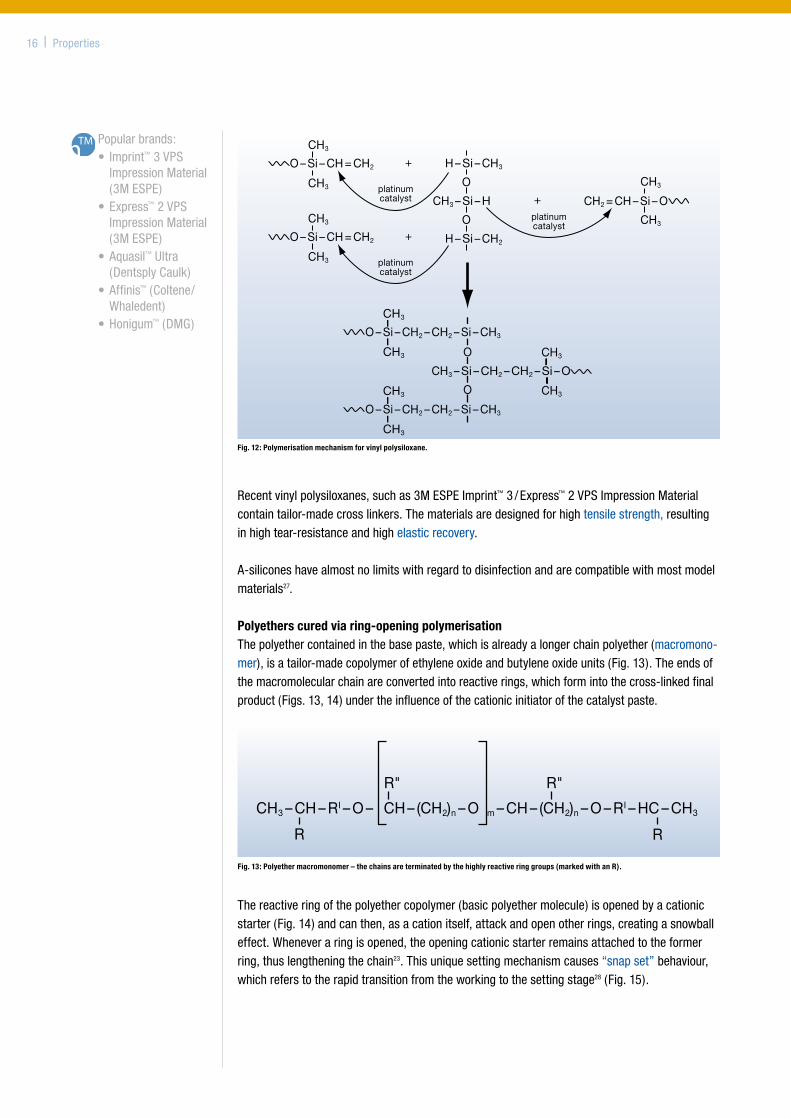
3.2.AdditioncuringprecisionimpressionmaterialsVinyl polysiloxanes (VPS, addition silicones, A-silicones)Vinylpolysiloxaneexploitstheprincipleof“additionreactioncuring”.Asopposedtocondensationcuringmaterialsthatexperienceshrinkageasaresultofevaporationofby-products,vinylpolysi-loxaneremainsdimensionallystable.Withvinylpolysiloxane,differentpre-polymericsilicon-functionalisedhydrocarbonchains(hydro-gensiloxane,vinylsiloxane)andaplatinumcatalystareinvolvedinthereaction.Theadditionofhydrogensiloxane(-O-Si-H)tovinylsiloxane(CH2=CH-Si-O)iscalledahydrosylationreaction.Asaresultofthisreactionthevinylpolysiloxaneisformedattheplatinumcatalyst23;25;26.Theplatinumcatalystisaplatinumcompoundwhich,startingfromH2PtCl6,isadjustedthroughreductionandservesasamolecular“dockingstation”forthetworeactingpartners,whichleavetheplatinumcompoundoncetheyarelinkedtoeachother(seeFig.12).
Vinylpolysiloxaneimpressionmaterialsarehydrophobicbytheirchemicalnature–theyaremoreorlessapolarhydrocarbonchains–andcanbemadehydrophilicusingsuitablemolecules.How-ever,thesearealwaysextrinsicmolecules;atrueintrinsichydrophilicity,asinthecaseofthepolarpolyethermolecules,cannotbeestablishedforthesemolecules.Somedegreeofhydrophili-citycanbeachievedafteracertainperiodoftimebytheuseofsurfactants.Surfactantscontainahydrophobicpart,whichensuresmiscibilityintheformulationandahydrophilicpartwhichisresponsibleforimprovedwetting.
Toconverttheliquidsiloxaneparentcompoundsintoapaste,inorganicfillersareadded.Thethixotropicpropertiesofthevinylpolysiloxanecanbecontrolledusingappropriatefillers.Thecoloursofthematerialsareadjustedthroughtheadditionofdyesandpigments.
Properties | 15
Fig. 11: History of precision impression materials.
1925ReversibleHydrocolloids
1950CondensationCuringElastomers
2003 CondensationPolyether
1955 CondensationSilicone
1950 Polysulfide
CH3 – CH – RI – O – CH – (CH2)n – O m – CH – (CH2)n – O – RI – HC – CH3
R R
R" R"
Recentvinylpolysiloxanes,suchas3MESPEImprint™3/Express™2VPSImpressionMaterialcontaintailor-madecrosslinkers.Thematerialsaredesignedforhightensilestrength,resultinginhightear-resistanceandhighelasticrecovery.
A-siliconeshavealmostnolimitswithregardtodisinfectionandarecompatiblewithmostmodelmaterials27.
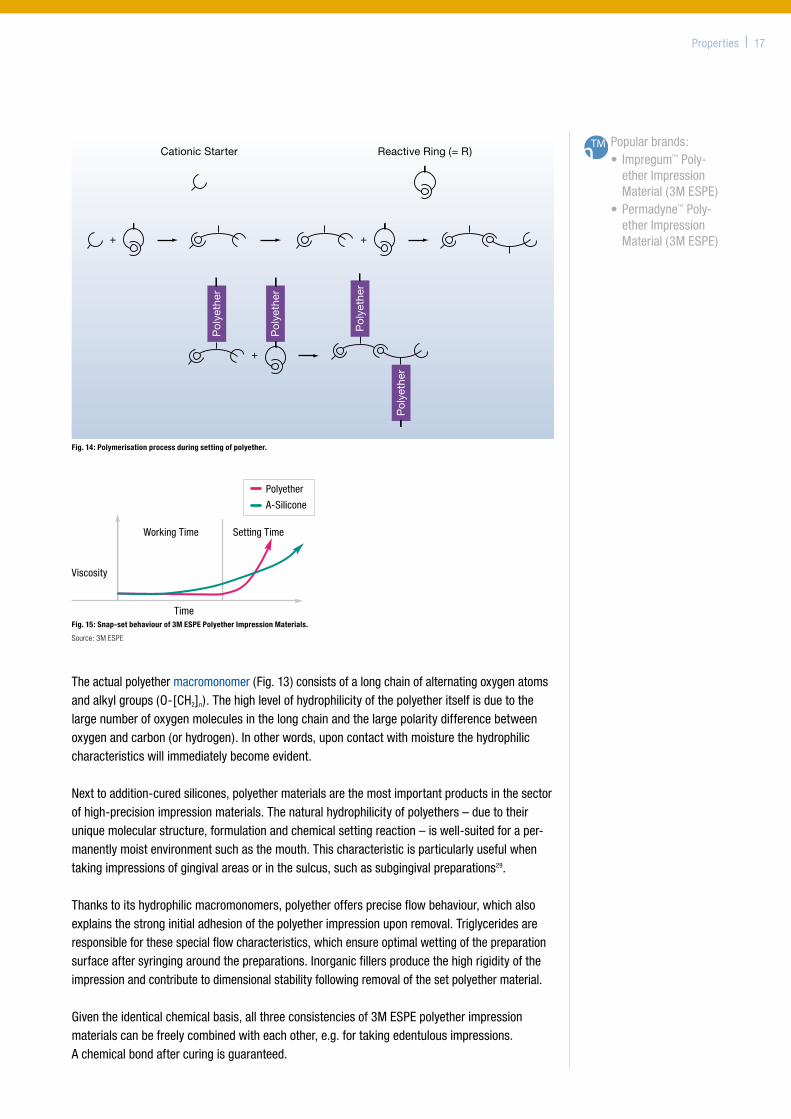
Polyethers cured via ring-opening polymerisationThepolyethercontainedinthebasepaste,whichisalreadyalongerchainpolyether(macromono-mer),isatailor-madecopolymerofethyleneoxideandbutyleneoxideunits(Fig.13).Theendsofthemacromolecularchainareconvertedintoreactiverings,whichformintothecross-linkedfinalproduct(Figs.13,14)undertheinfluenceofthecationicinitiatorofthecatalystpaste.
16 | Properties
Popularbrands:• Imprint™3VPS
ImpressionMaterial(3MESPE)
•Express™2VPSImpressionMaterial(3MESPE)
•Aquasil™Ultra(DentsplyCaulk)
•Affinis™(Coltene/Whaledent)
•Honigum™(DMG)
Fig. 13: Polyether macromonomer – the chains are terminated by the highly reactive ring groups (marked with an R).
CH3
H – Si – CH3
O
CH3 – Si – H
O
H – Si – CH2
CH3
O – Si – CH = CH2
O – Si – CH = CH2
CH3
CH3
+
platinumcatalyst
+
platinumcatalyst
CH3
CH2 = CH – Si – O
CH3
platinumcatalyst
+
CH3
CH3
O – Si – CH2 – CH2 – Si – CH3
O – Si – CH2 – CH2 – Si – CH3
CH3
CH3
O
CH3 – Si – CH2 – CH2 – Si – O
O CH3
CH3
Fig. 12: Polymerisation mechanism for vinyl polysiloxane.
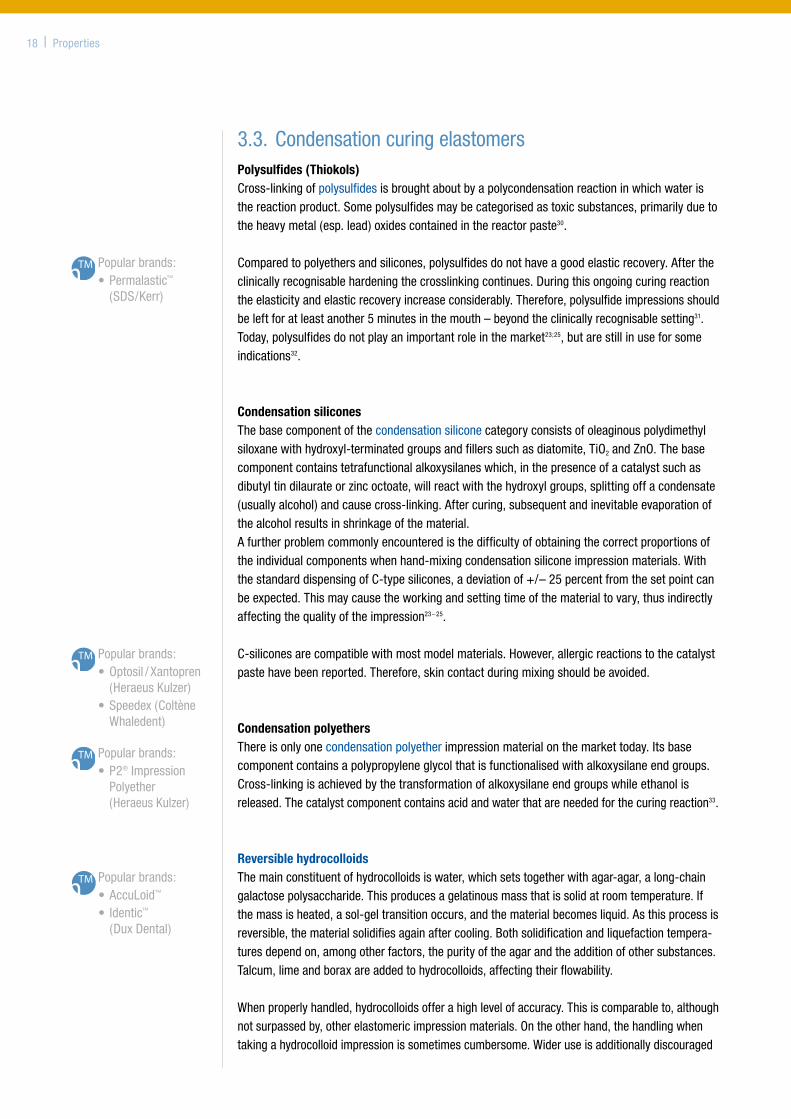
Thereactiveringofthepolyethercopolymer(basicpolyethermolecule)isopenedbyacationicstarter(Fig.14)andcanthen,asacationitself,attackandopenotherrings,creatingasnowballeffect.Wheneveraringisopened,theopeningcationicstarterremainsattachedtotheformerring,thuslengtheningthechain23.Thisuniquesettingmechanismcauses“snapset”behaviour,whichreferstotherapidtransitionfromtheworkingtothesettingstage28(Fig.15).
Properties | 17
Popularbrands:• Impregum™Poly-
etherImpressionMaterial(3MESPE)
•Permadyne™Poly-etherImpressionMaterial(3MESPE)
Working Time
Viscosity
Time
Setting Time
Polyether
A-Silicone
Fig. 15: Snap-set behaviour of 3M ESPE Polyether Impression Materials.
Source: 3M ESPE
Theactualpolyethermacromonomer(Fig.13)consistsofalongchainofalternatingoxygenatomsandalkylgroups(O-[CH2]n).Thehighlevelofhydrophilicityofthepolyetheritselfisduetothelargenumberofoxygenmoleculesinthelongchainandthelargepolaritydifferencebetweenoxygenandcarbon(orhydrogen).Inotherwords,uponcontactwithmoisturethehydrophiliccharacteristicswillimmediatelybecomeevident.
Nexttoaddition-curedsilicones,polyethermaterialsarethemostimportantproductsinthesectorofhigh-precisionimpressionmaterials.Thenaturalhydrophilicityofpolyethers–duetotheiruniquemolecularstructure,formulationandchemicalsettingreaction–iswell-suitedforaper-manentlymoistenvironmentsuchasthemouth.Thischaracteristicisparticularlyusefulwhentakingimpressionsofgingivalareasorinthesulcus,suchassubgingivalpreparations29.
Thankstoitshydrophilicmacromonomers,polyetherofferspreciseflowbehaviour,whichalsoexplainsthestronginitialadhesionofthepolyetherimpressionuponremoval.Triglyceridesareresponsibleforthesespecialflowcharacteristics,whichensureoptimalwettingofthepreparationsurfaceaftersyringingaroundthepreparations.Inorganicfillersproducethehighrigidityoftheimpressionandcontributetodimensionalstabilityfollowingremovalofthesetpolyethermaterial.
Giventheidenticalchemicalbasis,allthreeconsistenciesof3MESPEpolyetherimpressionmaterialscanbefreelycombinedwitheachother,e.g.fortakingedentulousimpressions.Achemicalbondaftercuringisguaranteed.
Fig. 14: Polymerisation process during setting of polyether.
Pol
yeth
er
Pol
yeth
er
Pol
yeth
er
Pol
yeth
er
Cationic Starter Reactive Ring (= R)
Popularbrands:•AccuLoid™
• Identic™(DuxDental)
3.3.CondensationcuringelastomersPolysulfides (Thiokols)Cross-linkingofpolysulfidesisbroughtaboutbyapolycondensationreactioninwhichwateristhereactionproduct.Somepolysulfidesmaybecategorisedastoxicsubstances,primarilyduetotheheavymetal(esp.lead)oxidescontainedinthereactorpaste30.
Comparedtopolyethersandsilicones,polysulfidesdonothaveagoodelasticrecovery.Aftertheclinicallyrecognisablehardeningthecrosslinkingcontinues.Duringthisongoingcuringreactiontheelasticityandelasticrecoveryincreaseconsiderably.Therefore,polysulfideimpressionsshouldbeleftforatleastanother5minutesinthemouth–beyondtheclinicallyrecognisablesetting31.Today,polysulfidesdonotplayanimportantroleinthemarket23;25,butarestillinuseforsomeindications32.
Condensation siliconesThebasecomponentofthecondensationsiliconecategoryconsistsofoleaginouspolydimethylsiloxanewithhydroxyl-terminatedgroupsandfillerssuchasdiatomite,TiO2andZnO.Thebasecomponentcontainstetrafunctionalalkoxysilaneswhich,inthepresenceofacatalystsuchasdibutyltindilaurateorzincoctoate,willreactwiththehydroxylgroups,splittingoffacondensate(usuallyalcohol)andcausecross-linking.Aftercuring,subsequentandinevitableevaporationofthealcoholresultsinshrinkageofthematerial.Afurtherproblemcommonlyencounteredisthedifficultyofobtainingthecorrectproportionsoftheindividualcomponentswhenhand-mixingcondensationsiliconeimpressionmaterials.WiththestandarddispensingofC-typesilicones,adeviationof+/–25percentfromthesetpointcanbeexpected.Thismaycausetheworkingandsettingtimeofthematerialtovary,thusindirectlyaffectingthequalityoftheimpression23–25.
C-siliconesarecompatiblewithmostmodelmaterials.However,allergicreactionstothecatalystpastehavebeenreported.Therefore,skincontactduringmixingshouldbeavoided.
Condensation polyethersThereisonlyonecondensationpolyetherimpressionmaterialonthemarkettoday.Itsbasecomponentcontainsapolypropyleneglycolthatisfunctionalisedwithalkoxysilaneendgroups.Cross-linkingisachievedbythetransformationofalkoxysilaneendgroupswhileethanolisreleased.Thecatalystcomponentcontainsacidandwaterthatareneededforthecuringreaction33.
Reversible hydrocolloidsThemainconstituentofhydrocolloidsiswater,whichsetstogetherwithagar-agar,along-chaingalactosepolysaccharide.Thisproducesagelatinousmassthatissolidatroomtemperature.Ifthemassisheated,asol-geltransitionoccurs,andthematerialbecomesliquid.Asthisprocessisreversible,thematerialsolidifiesagainaftercooling.Bothsolidificationandliquefactiontempera-turesdependon,amongotherfactors,thepurityoftheagarandtheadditionofothersubstances.Talcum,limeandboraxareaddedtohydrocolloids,affectingtheirflowability.
Whenproperlyhandled,hydrocolloidsofferahighlevelofaccuracy.Thisiscomparableto,althoughnotsurpassedby,otherelastomericimpressionmaterials.Ontheotherhand,thehandlingwhentakingahydrocolloidimpressionissometimescumbersome.Wideruseisadditionallydiscouraged
Popularbrands:•Permalastic™
(SDS/Kerr)
Popularbrands:•Optosil/Xantopren
(HeraeusKulzer) •Speedex(Coltène
Whaledent)
Popularbrands:•P2®Impression
Polyether(HeraeusKulzer)
18 | Properties
bylimitedshelflifeandinsufficienttear-resistance.Asaresult,theuseofhydrocolloidshasdwindledtoasmallnumberofusersovertheyears,andagarimpressionmaterialsarebynomeansasimportantastheyusedtobebeforetheintroductionofpolyetherandvinylpolysiloxane23;25.Hydrocolloidimpressionsneedtobecastimmediately(within20minutes).
3.4. ImpressionmaterialsforpreliminaryimpressionsForthefabricationofaprostheticrestorationamodeloftheopposingarchisnecessary,asthereisnootherwaytoensureacorrectocclusion.Itisimportantthereforethatmaterialsusedforpreliminaryimpressionsarediscussed:
Alginates – irreversible hydrocolloidsAlginatesareirreversibleelasticimpressionmaterials.Thebasicsubstanceofalginatesisalginicacid,apolyglycosideofD-mannuronicandL-gulonicacidwhichitselfisnotsolubleinwater.Usualalginatepowderscontain,besidesfillers,sodiumorpotassiumalginate,calciumsulphateasareagentandsodiumorpotassiumphosphateasaretarder.Alginatesareusuallymixedbyhand.Withtheavailablemixingdevices–dependingonthetypeofdevice–thematerialpropertiescanonlybeslightlyimproved.
Alginateimpressionsshouldbecastwithin15–30minutes,sinceduringfurtherstoragetheimpressioninevitablyshrinksduetosyneresisandevaporationofwaterfromthealginategel.Additionally,alginateimpressionscannotbestored,showalowtear-resistance22andtheelasticrecoveryafterdeformationisnotasgoodaswithprecisionimpressionmaterials34.Theuseofsuchanimpressionforthepreparationoftemporaryrestorationsislimitedsinceitcannotbestoredoveraprolongedperiodoftime.Althoughthehandlingofalginatesaswellastheirmaterialpropertiesarealtogethernotveryefficient,theirlowtear-resistanceoffersadvantagesinsomesituations,i.e.whentakinganimpressionofaperiodontallyaffectedtoothoroverfixedorthodonticapplianceswhichcannotbereproducedwithtear-resistantmaterialssincetheimpressioncouldnotberemovedfromthemouth.
Alginate replacement materialsToavoidthedescribeddisadvantagesofalginates,so-calledalginatereplacementmaterials(e.g.Position™Penta™VPSAlginateReplacement,3MESPE)weredeveloped.Sincetheyareprocessedwithautomaticmixingsystems(e.g.Pentamix™3AutomaticMixingUnit,3MESPE,seechapter5.3.),mixingandprocessingerrorscanalmostbeexcluded.Alginatereplacementmaterialsarecost-effectiveVPSmaterialswhich,asotherVPSmaterials,haveahighdimensionalstability.Whenusedwithprefabricatedsingle-useimpressiontrays(Position™Tray,3MESPE)(seechapter4),alginatereplacementmaterialsquicklyandefficientlyprovidepreliminaryimpressions.
Popularbrands:•Palgat™Plus/Quick
AlginateImpressionMaterial(3MESPE)
Properties | 19
Especiallyforthefabricationoftemporaryrestorations,theuseofalginatereplacementmaterialsincombinationwithsuchtraysoffersseveraladvantages:theirsmoothsiliconesurfacefacilitatesthetrimmingoftemporaryrestorationsconsiderably;duetotheunlimitedshelflifeoftheimpression,temporariescanberenewedlaterwithoutproblems.Nofurtherimpressionshavetobemade.Thepreparationofthetray(adhesive,customisationetc.)aswellasitscleaningandsterilisationisnotnecessary.
3.5.MaterialincompatibilitiesandimpressiondisposalGeneral incompatibilitiesMetalsaltswhicharecontainedinmanyastringentsusedforhaemostasiscaninhibitthesettingofimpressionmaterials.Theresultis–atleastpartly–aninsufficientsettingofthematerialespeciallyinthecriticalsulcusregion(seealsochapter2.3.).Generally,onlymaterialsofthesamematerialclassshouldbeusedtogether(seee.g.chapter4.2.1.Customisationofstocktraysorchapter6.1.1-stepimpressiontechniques).All3MESPEpolyethers(cationicring-openingpolymerisation,chapter3.2.)canbecombinedwitheachother,yet,notwithothermaterialclasses.Ifamethacrylatecompositematerialhasbeenusedforabutmentcompletionorcorebuild-up,oratemporaryrestorationofmethacrylatesorcompositeswasproducedbeforetheimpression,theresultingsmearlayerhastoberemovedwithalcoholandcottonpellet,otherwisetheimpressionmaterialwillnotsetatthecontactareas.Grindingandpolishingisnotenoughinthiscase.Therefore,theimpressionareashouldalwaysbethoroughlycleanedanddriedbeforetheimpres-sionistaken(chapter2.3.).Whenworkingwithhand-mixVPSputtymaterialsithastobeobservedthatthecontentsoftheglovescannegativelyinfluencethesettingbehaviouroftheimpressionmaterials(chapter5.1.).
DisposalImpressionmaterialscanbedisposedofinthehouseholdwaste,speciallocalregulationsmightapply.Withregardtowastepreventionthematerialsfilledinfoilbagsandusedinautomaticmixingdevicesareespeciallyenvironmentallyfriendly,sincetheycanbeexactlydosedandonlylittlepackagingwasteisgenerated.
Popularbrands:•Position™VPS
AlginateReplace-ment(3MESPE)
•AlgiNot(Kerr)
Warning:Incompatibilitiesmayariseduring–Retraction( 2.9.)
–Traycustomisation( 4.2.)
–Puttywashtechnique( 6.1.)
–Aftercorebuild-uporfabricationoftemporaries
20 | Properties
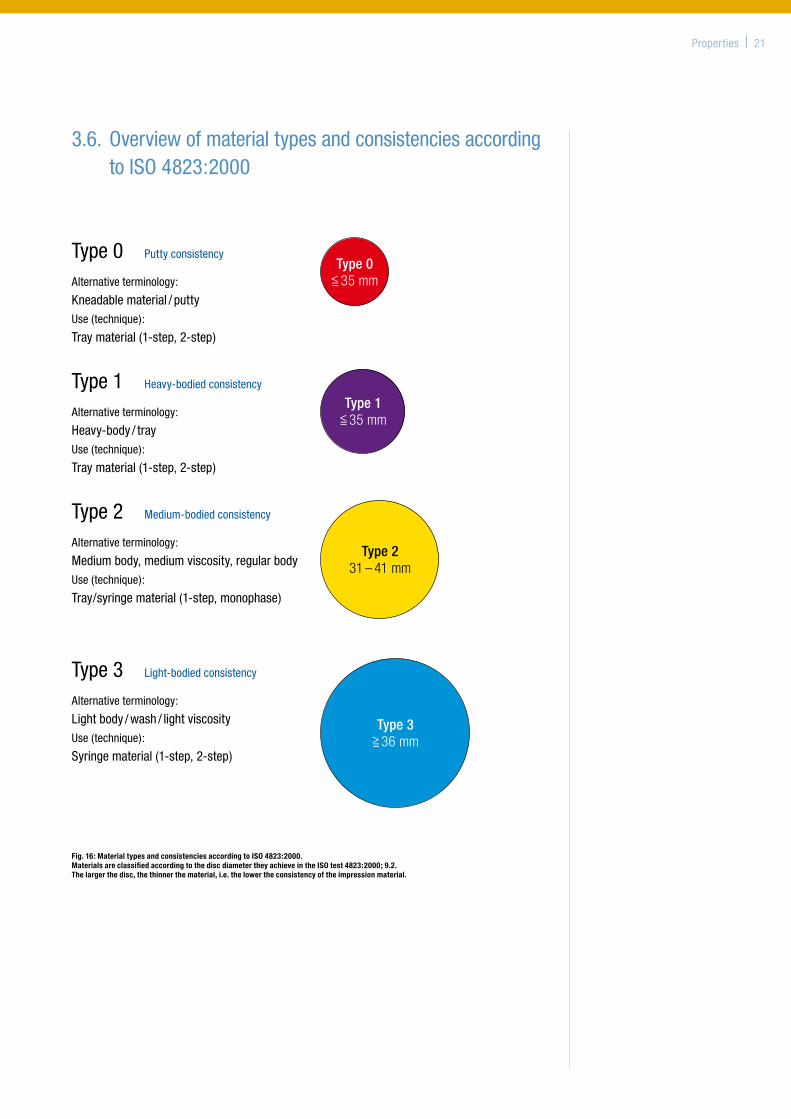
3.6.OverviewofmaterialtypesandconsistenciesaccordingtoISO4823:2000
Fig. 16: Material types and consistencies according to ISO 4823:2000. Materials are classified according to the disc diameter they achieve in the ISO test 4823:2000; 9.2. The larger the disc, the thinner the material, i.e. the lower the consistency of the impression material.
Type0 Puttyconsistency
Alternativeterminology:
Kneadablematerial/puttyUse(technique):
Traymaterial(1-step,2-step)
Type 0<= 35 mm
Type1 Heavy-bodiedconsistency
Alternativeterminology:
Heavy-body/trayUse(technique):
Traymaterial(1-step,2-step)
Type 1<= 35 mm
Type2 Medium-bodiedconsistency
Alternativeterminology:
Mediumbody,mediumviscosity,regularbodyUse(technique):
Tray/syringematerial(1-step,monophase)
Type 231 – 41 mm
Type3 Light-bodiedconsistency
Alternativeterminology:
Lightbody/wash/lightviscosityUse(technique):
Syringematerial(1-step,2-step)
Type 3>=36 mm
Properties | 21
4. Impression trays (B.Wöstmann)
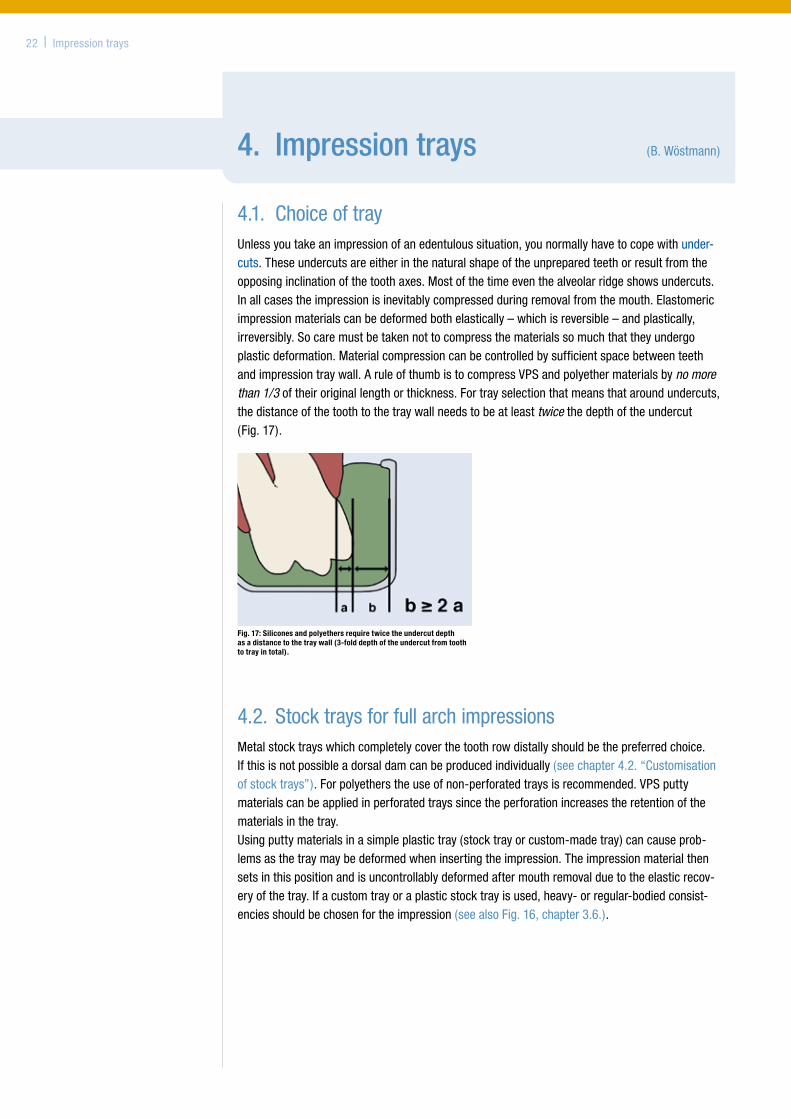
4.1. ChoiceoftrayUnlessyoutakeanimpressionofanedentuloussituation,younormallyhavetocopewithunder-cuts.Theseundercutsareeitherinthenaturalshapeoftheunpreparedteethorresultfromtheopposinginclinationofthetoothaxes.Mostofthetimeeventhealveolarridgeshowsundercuts.Inallcasestheimpressionisinevitablycompressedduringremovalfromthemouth.Elastomericimpressionmaterialscanbedeformedbothelastically–whichisreversible–andplastically,irreversibly.Socaremustbetakennottocompressthematerialssomuchthattheyundergoplasticdeformation.Materialcompressioncanbecontrolledbysufficientspacebetweenteethandimpressiontraywall.AruleofthumbistocompressVPSandpolyethermaterialsbyno more than 1/3 oftheiroriginallengthorthickness.Fortrayselectionthatmeansthataroundundercuts,thedistanceofthetoothtothetraywallneedstobeatleasttwicethedepthoftheundercut(Fig.17).
4.2.StocktraysforfullarchimpressionsMetalstocktrayswhichcompletelycoverthetoothrowdistallyshouldbethepreferredchoice.Ifthisisnotpossibleadorsaldamcanbeproducedindividually(seechapter4.2.“Customisationofstocktrays”).Forpolyetherstheuseofnon-perforatedtraysisrecommended.VPSputtymaterialscanbeappliedinperforatedtrayssincetheperforationincreasestheretentionofthematerialsinthetray.Usingputtymaterialsinasimpleplastictray(stocktrayorcustom-madetray)cancauseprob-lemsasthetraymaybedeformedwheninsertingtheimpression.Theimpressionmaterialthensetsinthispositionandisuncontrollablydeformedaftermouthremovalduetotheelasticrecov-eryofthetray.Ifacustomtrayoraplasticstocktrayisused,heavy-orregular-bodiedconsist-enciesshouldbechosenfortheimpression(seealsoFig.16,chapter3.6.).
22 | Impressiontrays
Fig. 17: Silicones and polyethers require twice the undercut depth as a distance to the tray wall (3-fold depth of the undercut from tooth to tray in total).
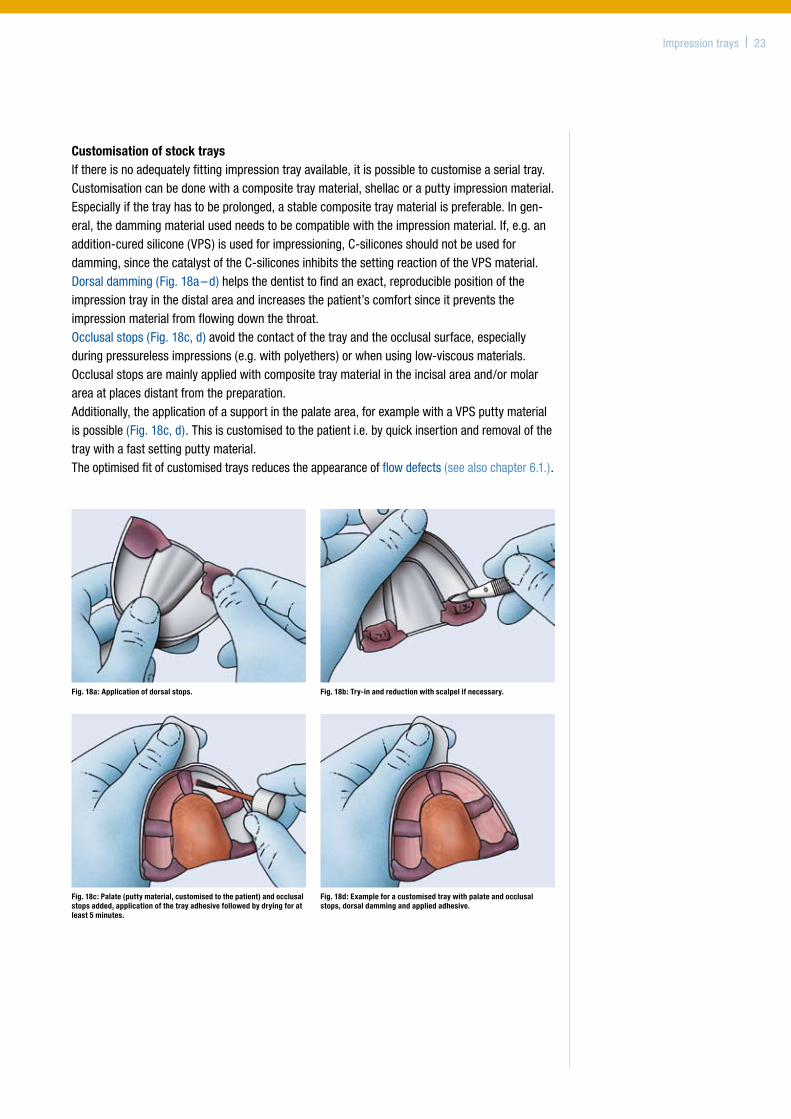
Customisation of stock traysIfthereisnoadequatelyfittingimpressiontrayavailable,itispossibletocustomiseaserialtray.Customisationcanbedonewithacompositetraymaterial,shellacoraputtyimpressionmaterial.Especiallyifthetrayhastobeprolonged,astablecompositetraymaterialispreferable.Ingen-eral,thedammingmaterialusedneedstobecompatiblewiththeimpressionmaterial.If,e.g.anaddition-curedsilicone(VPS)isusedforimpressioning,C-siliconesshouldnotbeusedfordamming,sincethecatalystoftheC-siliconesinhibitsthesettingreactionoftheVPSmaterial.Dorsaldamming(Fig.18a–d)helpsthedentisttofindanexact,reproduciblepositionoftheimpressiontrayinthedistalareaandincreasesthepatient’scomfortsinceitpreventstheimpressionmaterialfromflowingdownthethroat.Occlusalstops(Fig.18c,d)avoidthecontactofthetrayandtheocclusalsurface,especiallyduringpressurelessimpressions(e.g.withpolyethers)orwhenusinglow-viscousmaterials.Occlusalstopsaremainlyappliedwithcompositetraymaterialintheincisalareaand/ormolarareaatplacesdistantfromthepreparation.Additionally,theapplicationofasupportinthepalatearea,forexamplewithaVPSputtymaterialispossible(Fig.18c,d).Thisiscustomisedtothepatienti.e.byquickinsertionandremovalofthetraywithafastsettingputtymaterial.Theoptimisedfitofcustomisedtraysreducestheappearanceofflowdefects(seealsochapter6.1.).
Impressiontrays | 23
Fig. 18a: Application of dorsal stops. Fig. 18b: Try-in and reduction with scalpel if necessary.
Fig. 18c: Palate (putty material, customised to the patient) and occlusal stops added, application of the tray adhesive followed by drying for at least 5 minutes.
Fig. 18d: Example for a customised tray with palate and occlusal stops, dorsal damming and applied adhesive.
4.3.StocktrayswithoptimisedfitWhilechoosingatrayforimpressionsoftheupperjawisusuallyquiteeasy,youmightencounterproblemswithafully-toothedlowerjaw.Mostlowerjawserialtraysavailableinthedentalmarketareeitherwideenoughbutthendorsallytooshortor,iftheyarelongenough,theyaretoowide35;36.Thus,theuseofimpressiontrayswhichhavebeenespeciallydevelopedfortheimpres-sionoffully-toothedlowerjawsisadvantageous*.
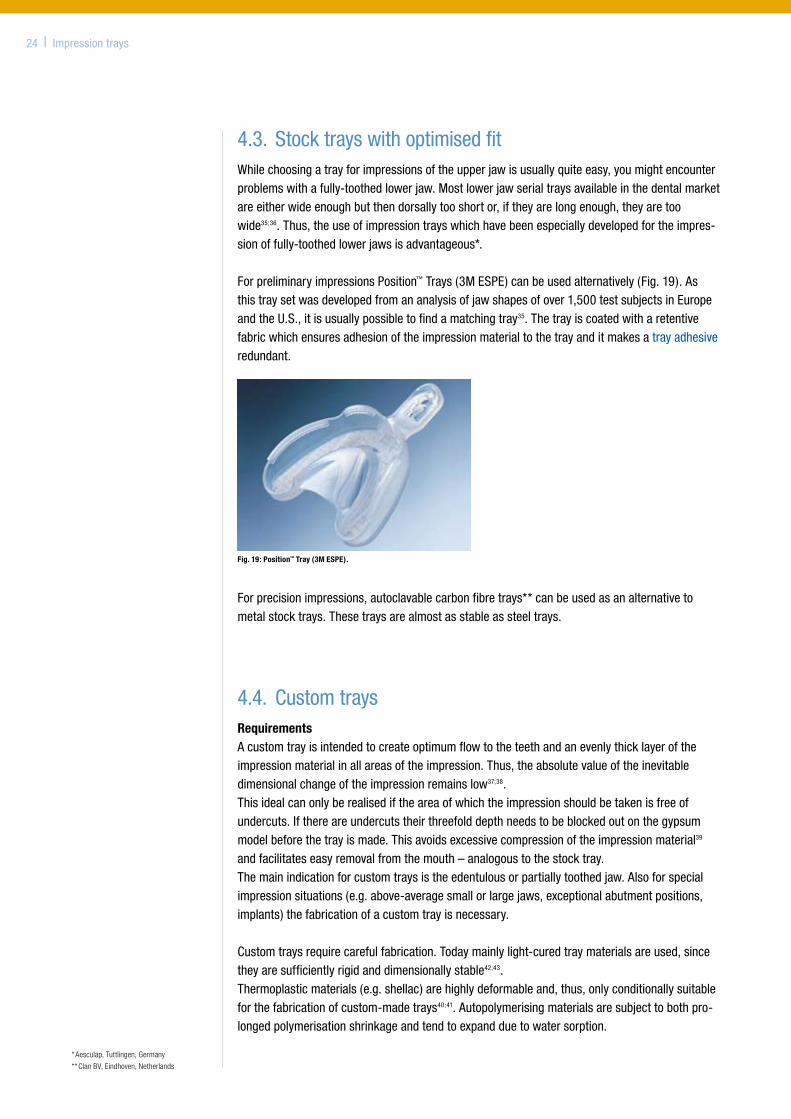
ForpreliminaryimpressionsPosition™Trays(3MESPE)canbeusedalternatively(Fig.19).Asthistraysetwasdevelopedfromananalysisofjawshapesofover1,500testsubjectsinEuropeandtheU.S.,itisusuallypossibletofindamatchingtray35.Thetrayiscoatedwitharetentivefabricwhichensuresadhesionoftheimpressionmaterialtothetrayanditmakesatrayadhesiveredundant.
Forprecisionimpressions,autoclavablecarbonfibretrays**canbeusedasanalternativetometalstocktrays.Thesetraysarealmostasstableassteeltrays.
4.4. CustomtraysRequirementsAcustomtrayisintendedtocreateoptimumflowtotheteethandanevenlythicklayeroftheimpressionmaterialinallareasoftheimpression.Thus,theabsolutevalueoftheinevitabledimensionalchangeoftheimpressionremainslow37;38.Thisidealcanonlyberealisediftheareaofwhichtheimpressionshouldbetakenisfreeofundercuts.Ifthereareundercutstheirthreefolddepthneedstobeblockedoutonthegypsummodelbeforethetrayismade.Thisavoidsexcessivecompressionoftheimpressionmaterial39andfacilitateseasyremovalfromthemouth–analogoustothestocktray.Themainindicationforcustomtraysistheedentulousorpartiallytoothedjaw.Alsoforspecialimpressionsituations(e.g.above-averagesmallorlargejaws,exceptionalabutmentpositions,implants)thefabricationofacustomtrayisnecessary.
Customtraysrequirecarefulfabrication.Todaymainlylight-curedtraymaterialsareused,sincetheyaresufficientlyrigidanddimensionallystable42;43.Thermoplasticmaterials(e.g.shellac)arehighlydeformableand,thus,onlyconditionallysuitableforthefabricationofcustom-madetrays40;41.Autopolymerisingmaterialsaresubjecttobothpro-longedpolymerisationshrinkageandtendtoexpandduetowatersorption.
24 | Impressiontrays
* Aesculap, Tuttlingen, Germany
** Clan BV, Eindhoven, Netherlands
Fig. 19: Position™ Tray (3M ESPE).
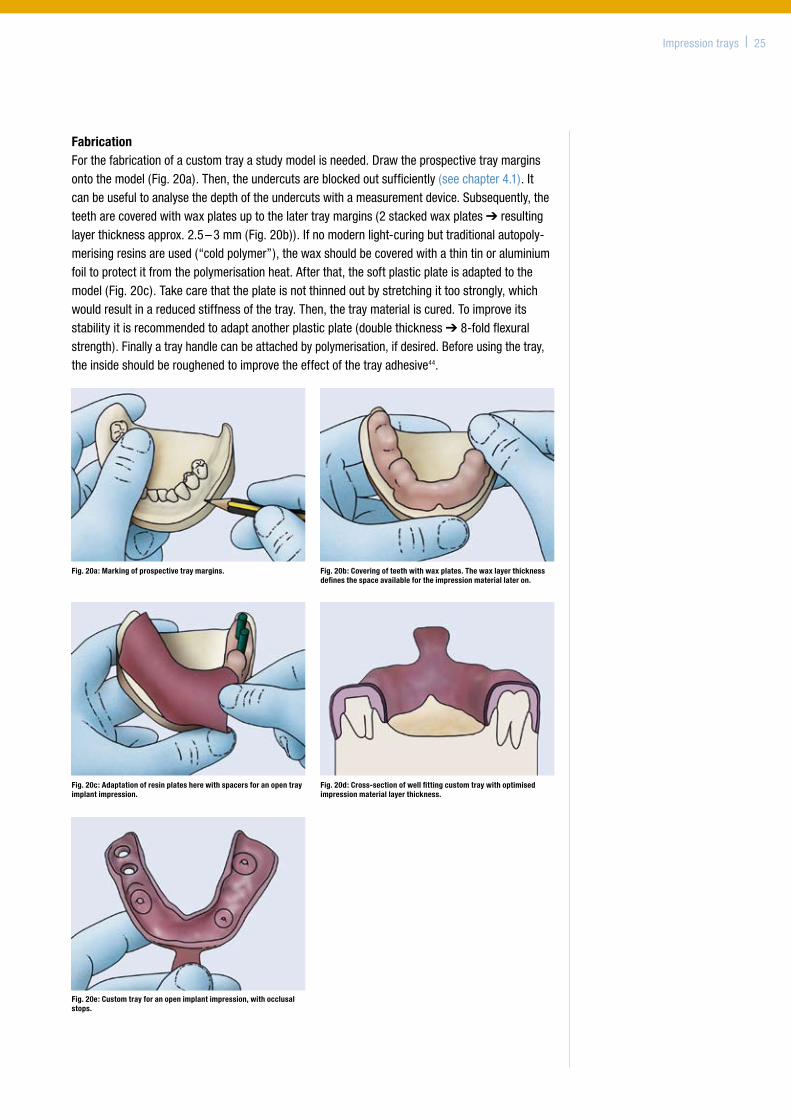
FabricationForthefabricationofacustomtrayastudymodelisneeded.Drawtheprospectivetraymarginsontothemodel(Fig.20a).Then,theundercutsareblockedoutsufficiently(seechapter4.1).Itcanbeusefultoanalysethedepthoftheundercutswithameasurementdevice.Subsequently,theteetharecoveredwithwaxplatesuptothelatertraymargins(2stackedwaxplates➔resultinglayerthicknessapprox.2.5–3mm(Fig.20b)).Ifnomodernlight-curingbuttraditionalautopoly-merisingresinsareused(“coldpolymer”),thewaxshouldbecoveredwithathintinoraluminiumfoiltoprotectitfromthepolymerisationheat.Afterthat,thesoftplasticplateisadaptedtothemodel(Fig.20c).Takecarethattheplateisnotthinnedoutbystretchingittoostrongly,whichwouldresultinareducedstiffnessofthetray.Then,thetraymaterialiscured.Toimproveitsstabilityitisrecommendedtoadaptanotherplasticplate(doublethickness➔8-foldflexuralstrength).Finallyatrayhandlecanbeattachedbypolymerisation,ifdesired.Beforeusingthetray,theinsideshouldberoughenedtoimprovetheeffectofthetrayadhesive44.
Impressiontrays | 25
Fig. 20a: Marking of prospective tray margins. Fig. 20b: Covering of teeth with wax plates. The wax layer thickness defines the space available for the impression material later on.
Fig. 20c: Adaptation of resin plates here with spacers for an open tray implant impression.
Fig. 20d: Cross-section of well fitting custom tray with optimised impression material layer thickness.
Fig. 20e: Custom tray for an open implant impression, with occlusal stops.
26 | Impressiontrays
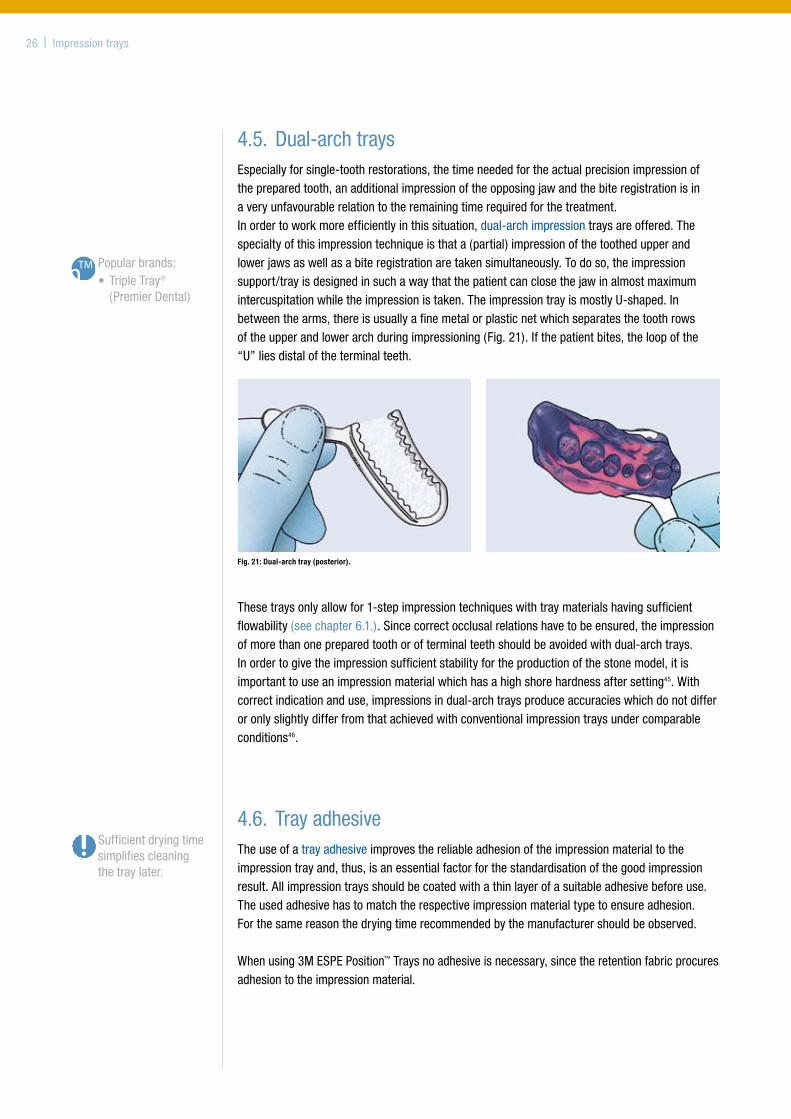
4.5.Dual-archtraysEspeciallyforsingle-toothrestorations,thetimeneededfortheactualprecisionimpressionofthepreparedtooth,anadditionalimpressionoftheopposingjawandthebiteregistrationisinaveryunfavourablerelationtotheremainingtimerequiredforthetreatment.Inordertoworkmoreefficientlyinthissituation,dual-archimpressiontraysareoffered.Thespecialtyofthisimpressiontechniqueisthata(partial)impressionofthetoothedupperandlowerjawsaswellasabiteregistrationaretakensimultaneously.Todoso,theimpressionsupport/trayisdesignedinsuchawaythatthepatientcanclosethejawinalmostmaximumintercuspitationwhiletheimpressionistaken.TheimpressiontrayismostlyU-shaped.Inbetweenthearms,thereisusuallyafinemetalorplasticnetwhichseparatesthetoothrowsoftheupperandlowerarchduringimpressioning(Fig.21).Ifthepatientbites,theloopofthe“U”liesdistaloftheterminalteeth.
Thesetraysonlyallowfor1-stepimpressiontechniqueswithtraymaterialshavingsufficientflowability(seechapter6.1.).Sincecorrectocclusalrelationshavetobeensured,theimpressionofmorethanonepreparedtoothorofterminalteethshouldbeavoidedwithdual-archtrays.Inordertogivetheimpressionsufficientstabilityfortheproductionofthestonemodel,itisimportanttouseanimpressionmaterialwhichhasahighshorehardnessaftersetting45.Withcorrectindicationanduse,impressionsindual-archtraysproduceaccuracieswhichdonotdifferoronlyslightlydifferfromthatachievedwithconventionalimpressiontraysundercomparableconditions46.
4.6. TrayadhesiveTheuseofatrayadhesiveimprovesthereliableadhesionoftheimpressionmaterialtotheimpressiontrayand,thus,isanessentialfactorforthestandardisationofthegoodimpressionresult.Allimpressiontraysshouldbecoatedwithathinlayerofasuitableadhesivebeforeuse.Theusedadhesivehastomatchtherespectiveimpressionmaterialtypetoensureadhesion.Forthesamereasonthedryingtimerecommendedbythemanufacturershouldbeobserved.
Whenusing3MESPEPosition™Traysnoadhesiveisnecessary,sincetheretentionfabricprocuresadhesiontotheimpressionmaterial.
Sufficientdryingtimesimplifiescleaningthetraylater.
Popularbrands:•TripleTray®
(PremierDental)
Fig. 21: Dual-arch tray (posterior).
Available3MESPEproducts:
• Impregum™FPoly-etherImpressionMaterial
•Permadyne™Poly-etherImpressionMaterial
•Ramitec™PolyetherBiteRegistrationMaterial
5. Mixing of impression materials (3MESPE)
Theimportanceofastandardisedworkflowhasbeendiscussedinchapters1.3.and1.4.Modernimpressionmaterialsarehigh-techproductswithasophisticatedchemistrywhichareproducedbythemanufacturerwithintighttolerancelimits.Allimpressionmaterialshavetobemixedfromatleasttwocomponents(usuallynamedbaseandcatalystpaste)beforeuse.Onlyahomogeneous,void-freemixingwithacorrectmixingratioofthecomponentsallowsaperfectprecisionimpressionwhichexploitsallqualitiesofmodernimpressionmaterials.
Themajorityofimpressionsworldwidearestillperformedwithhand-mixedmaterials,althoughautomixedsystemsbasedonhanddispenserswithdual-barrelcartridgeshavebeenavailablesince1983(Express™,3MESPE)andautomaticmixingsystemsforfoilbagssince1993(Pentamix™AutomaticMixingUnit,3MESPE).Meanwhileallcommonimpressionconsistencies,includingtheespeciallyhigh-viscousputtymaterialcanbemixedautomatically,homogeneouslyandvoid-free,usingthePentamix™System.
Today’smostcommonmixingproceduresare:
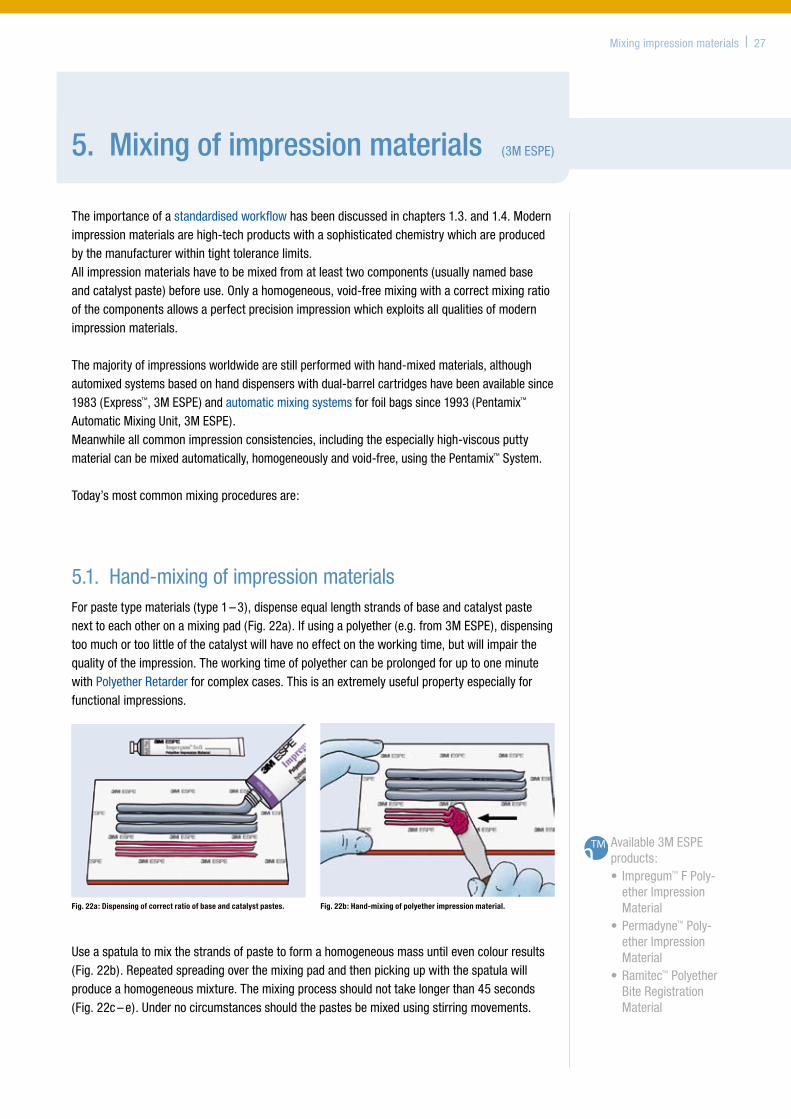
5.1. Hand-mixingofimpressionmaterialsForpastetypematerials(type1–3),dispenseequallengthstrandsofbaseandcatalystpastenexttoeachotheronamixingpad(Fig.22a).Ifusingapolyether(e.g.from3MESPE),dispensingtoomuchortoolittleofthecatalystwillhavenoeffectontheworkingtime,butwillimpairthequalityoftheimpression.TheworkingtimeofpolyethercanbeprolongedforuptooneminutewithPolyetherRetarderforcomplexcases.Thisisanextremelyusefulpropertyespeciallyforfunctionalimpressions.
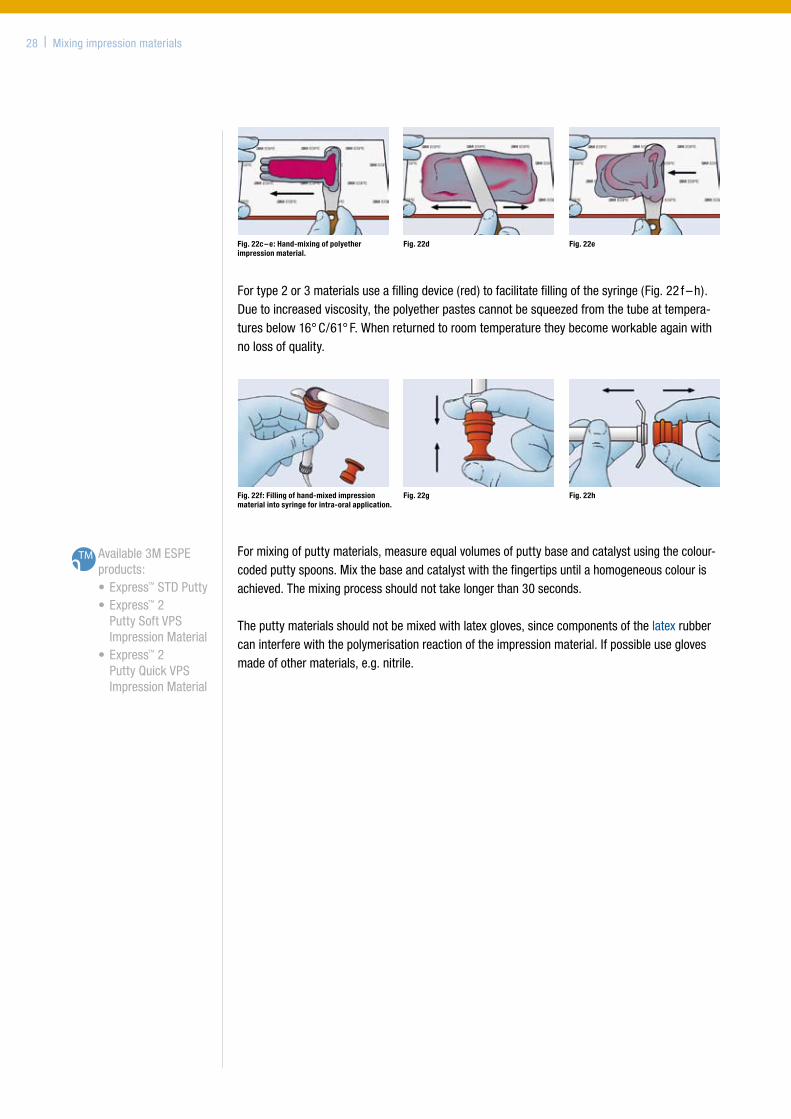
Useaspatulatomixthestrandsofpastetoformahomogeneousmassuntilevencolourresults(Fig.22b).Repeatedspreadingoverthemixingpadandthenpickingupwiththespatulawillproduceahomogeneousmixture.Themixingprocessshouldnottakelongerthan45seconds(Fig.22c–e).Undernocircumstancesshouldthepastesbemixedusingstirringmovements.
Fig. 22a: Dispensing of correct ratio of base and catalyst pastes. Fig. 22b: Hand-mixing of polyether impression material.
Mixingimpressionmaterials | 27
Available3MESPEproducts:
•Express™STDPutty •Express™2
PuttySoftVPSImpressionMaterial
•Express™2PuttyQuickVPSImpressionMaterial
Formixingofputtymaterials,measureequalvolumesofputtybaseandcatalystusingthecolour-codedputtyspoons.Mixthebaseandcatalystwiththefingertipsuntilahomogeneouscolourisachieved.Themixingprocessshouldnottakelongerthan30seconds.
Theputtymaterialsshouldnotbemixedwithlatexgloves,sincecomponentsofthelatexrubbercaninterferewiththepolymerisationreactionoftheimpressionmaterial.Ifpossibleuseglovesmadeofothermaterials,e.g.nitrile.
Fig. 22c – e: Hand-mixing of polyether impression material.
Fig. 22d Fig. 22e
Fortype2or3materialsuseafillingdevice(red)tofacilitatefillingofthesyringe(Fig.22f–h).Duetoincreasedviscosity,thepolyetherpastescannotbesqueezedfromthetubeattempera-turesbelow16°C/61°F.Whenreturnedtoroomtemperaturetheybecomeworkableagainwithnolossofquality.
28 | Mixingimpressionmaterials
Fig. 22f: Filling of hand-mixed impression material into syringe for intra-oral application.
Fig. 22g Fig. 22h
Mixingimpressionmaterials | 29
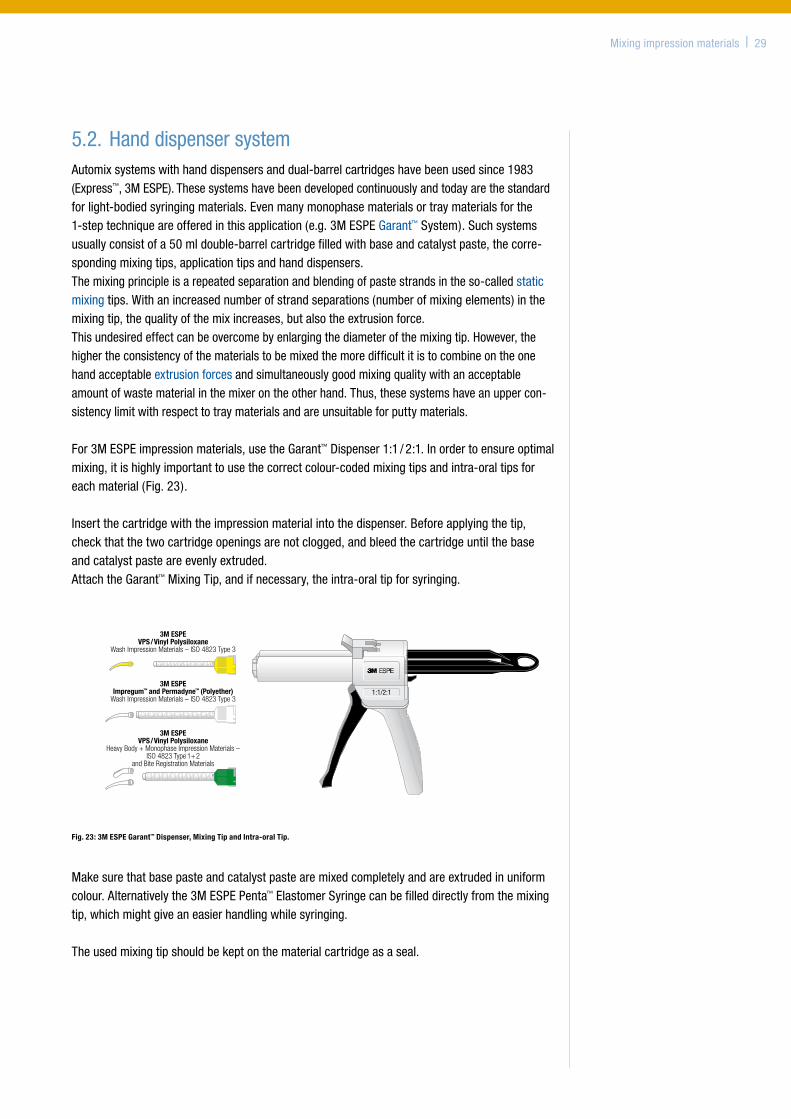
5.2.HanddispensersystemAutomixsystemswithhanddispensersanddual-barrelcartridgeshavebeenusedsince1983(Express™,3MESPE).Thesesystemshavebeendevelopedcontinuouslyandtodayarethestandardforlight-bodiedsyringingmaterials.Evenmanymonophasematerialsortraymaterialsforthe1-steptechniqueareofferedinthisapplication(e.g.3MESPEGarant™System).Suchsystemsusuallyconsistofa50mldouble-barrelcartridgefilledwithbaseandcatalystpaste,thecorre-spondingmixingtips,applicationtipsandhanddispensers.Themixingprincipleisarepeatedseparationandblendingofpastestrandsintheso-calledstaticmixingtips.Withanincreasednumberofstrandseparations(numberofmixingelements)inthemixingtip,thequalityofthemixincreases,butalsotheextrusionforce.Thisundesiredeffectcanbeovercomebyenlargingthediameterofthemixingtip.However,thehighertheconsistencyofthematerialstobemixedthemoredifficultitistocombineontheonehandacceptableextrusionforcesandsimultaneouslygoodmixingqualitywithanacceptableamountofwastematerialinthemixerontheotherhand.Thus,thesesystemshaveanuppercon-sistencylimitwithrespecttotraymaterialsandareunsuitableforputtymaterials.
For3MESPEimpressionmaterials,usetheGarant™Dispenser1:1/2:1.Inordertoensureoptimalmixing,itishighlyimportanttousethecorrectcolour-codedmixingtipsandintra-oraltipsforeachmaterial(Fig.23).
Insertthecartridgewiththeimpressionmaterialintothedispenser.Beforeapplyingthetip,checkthatthetwocartridgeopeningsarenotclogged,andbleedthecartridgeuntilthebaseandcatalystpasteareevenlyextruded.AttachtheGarant™MixingTip,andifnecessary,theintra-oraltipforsyringing.
210 x 297 mm - Seite 1 - 163/0/571/51-54+F 11/07 - BLAU • GELB • GRÜN • SCHWARZ - 4-Farb-Satz nach Euroskala - 07-0435 (sr)
Dispenser 4:1/10:1
1:1/2:1
4:1/10:1
3M ESPEVPS/Vinyl Polysiloxane
Wash Impression Materials – ISO 4823 Type 3
3M ESPEImpregum™ and Permadyne™ (Polyether)
Wash Impression Materials – ISO 4823 Type 3
3M ESPEVPS/Vinyl Polysiloxane
Heavy Body + Monophase Impression Materials –ISO 4823 Type 1+2
and Bite Registration Materials
3M ESPEProtemp™ Temporization Material
4400
0727
808/
03 (N
ovem
ber 2
007)
Garant™
Dispenser 1:1/2:1
EPSE M3GA EPSE M3stcudorP latneDstcudorP latneD
D-82229 Seefeld - Germany St. Paul, MN 55144-1000
3M, ESPE, Garant, Impregum, Permadyne and Protemp are trademarks of 3M or 3M ESPE AG.© 3M 2007. All rights reserved.
Caution: U.S. Federal Law restricts this device to sale by or on the orderof a dental professional.
Fig. 23: 3M ESPE Garant™ Dispenser, Mixing Tip and Intra-oral Tip.
Makesurethatbasepasteandcatalystpastearemixedcompletelyandareextrudedinuniformcolour.Alternativelythe3MESPEPenta™ElastomerSyringecanbefilleddirectlyfromthemixingtip,whichmightgiveaneasierhandlingwhilesyringing.
Theusedmixingtipshouldbekeptonthematerialcartridgeasaseal.
5.3.AutomaticmixingsystemExactdispensingandthorough,homogeneousmixingofthematerialsarefundamentalrequire-mentsforsuccessfulprecisionimpressions.That’swhy3MESPEdevelopedthefully-automaticPentamix™AutomaticMixingUnitwhichenteredfull-scaleproductionattheendof1993.ThenamePentamixisderivedfromtheGreekwordforfive(penta),reflectingthemixratioofbasepastetocatalystpaste,namely5:1.Meanwhileinitsthirdgeneration,thissystemhashelpedtostandardiseclinicalworkflows,eliminatingthestrainanduncertaintyofhand-mixedmaterialsformanypractices.ThePentamix™3AutomaticMixingUnitdeliversacompletelyhomogeneousandvoid-freemixforhighlyaccurateimpressionsandperfectlyfittingrestorations.
Directfillingoftraysandsyringesfromtheautomaticmixingunitishygienic,andoverall,lesstimeisspentcleaninganddisinfectinggunsandcartridges.Theriskofcross-contaminationisreduced.
ClinicaltimingwiththePentamixmixingunitisreliableandreproducible.Twomainadvantagesofmachinemixingbecomeclearerthefasterthepastecanbeextruded:•Shortertrayfillingtimeleavesmoreworkingtimefortheactualimpression.•Shortertrayfillingtimegivesmoretimetotheassistantforchairsidehelp.
30 | Mixingimpressionmaterials
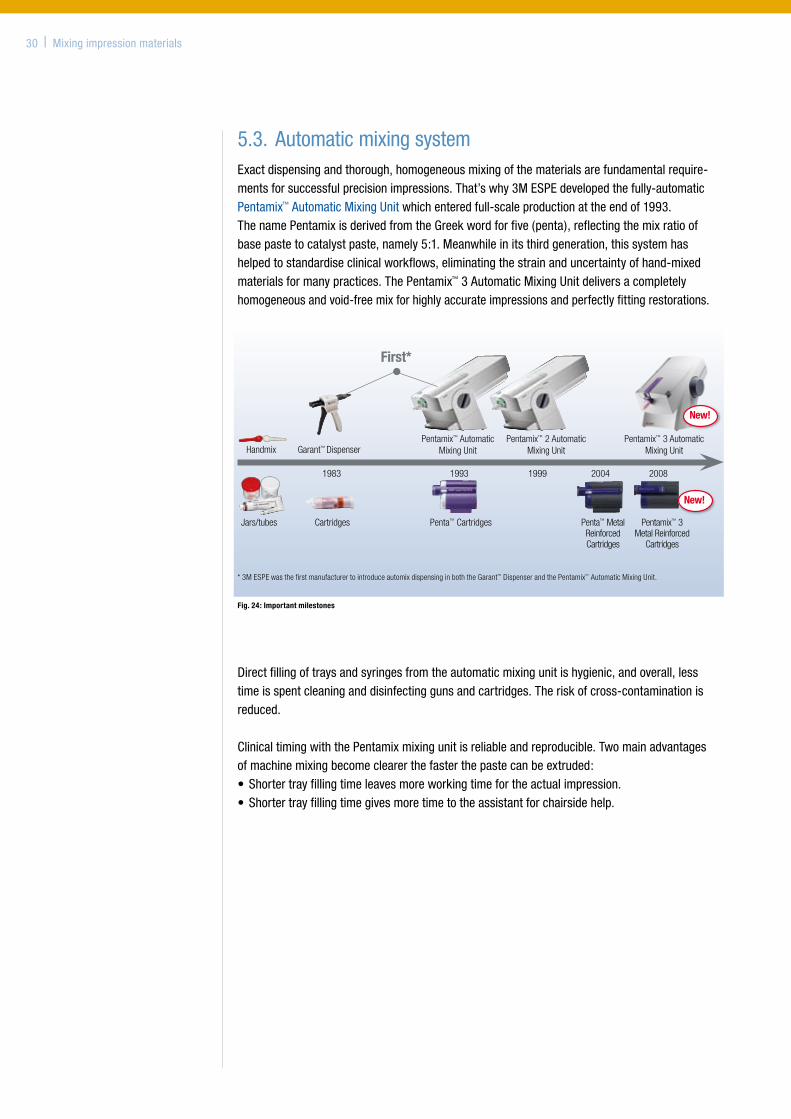
First*
1983 1993 1999 2004 2008
Jars/tubes Cartridges Penta™ Cartridges Pentamix™ 3 Metal Reinforced
Cartridges
Penta™ Metal Reinforced Cartridges
Handmix Garant™ DispenserPentamix™ Automatic
Mixing UnitPentamix™ 2 Automatic
Mixing UnitPentamix™ 3 Automatic
Mixing Unit
New!
New!
* 3M ESPE was the first manufacturer to introduce automix dispensing in both the Garant™ Dispenser and the Pentamix™ Automatic Mixing Unit.
Fig. 24: Important milestones
Mixing principleThePentamix™Systemisbasedondynamicmixing,i.e.themixingspiralinthemixingtipisdrivenbyaseparatemotorviaashaft.Therotationofthemixingspiralinconjunctionwiththeextrusiongeneratesaturbulentflowwithinthematerialwhichresultsincompletemixing.Incomparisontostaticmixingsystemsorhand-mixingthequalityofmixismuchmorehomo-geneous68,69.
Anotheradvantageofthedynamicmixingprincipleisthatitalsoallowshighlyviscousmaterialssuchastype0puttiestobemixedautomatically.
Pentamix™ System and componentsThecoreofthePentamixsystemisthePentamix™AutomaticMixingUnit,whichpermitsmorerelaxedandcost-effectivework.Overtime,systemcomponentswereimprovedtoenhancetherobustnessandreliabilityofthesystem.
Penta™ Mixing Tips – RedThePentaMixingTipenablesanefficientmixingprocessbyoptimisedinnergeometrywhichsignificantlyreducestheflowresistance.
PentaMatic™ AutoOpen System Foil BagsThePentafoilbagsrequirenoseparateactivationandarecolour-coded.APenta™AuthentificationLabelensuresgenuine3MESPEquality.
Penta™ CartridgesPentacartridgesarereinforcedwithsteelinnertubesandarelesssensitivetofatiguethantheoriginalplasticcartridges.
Mixingimpressionmaterials | 31
Fig 28: Pentamix™ 3 Automatic Mixing Unit.
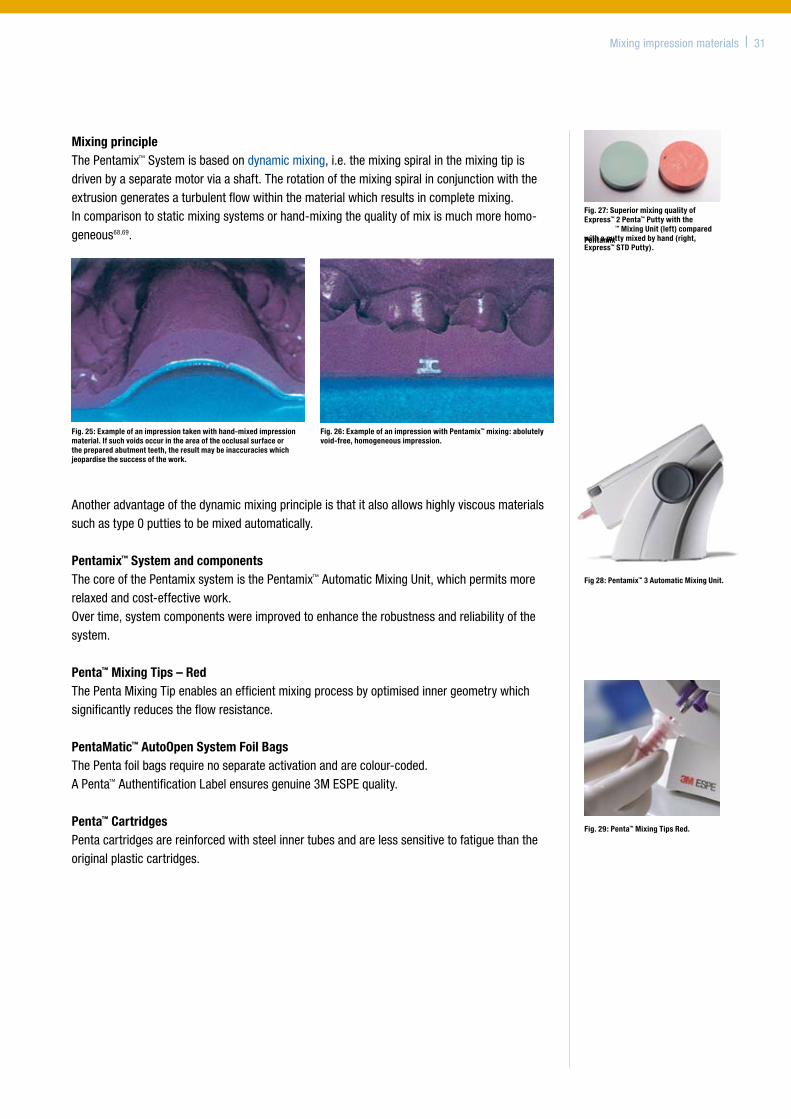
Fig. 25: Example of an impression taken with hand-mixed impression material. If such voids occur in the area of the occlusal surface or the prepared abutment teeth, the result may be inaccuracies which jeopardise the success of the work.
Fig. 26: Example of an impression with Pentamix™ mixing: abolutely void-free, homogeneous impression.
Fig. 27: Superior mixing quality of Express™ 2 Penta™ Putty with the Pentamix
™ Mixing Unit (left) compared with a putty mixed by hand (right, Express™ STD Putty).
Fig. 29: Penta™ Mixing Tips Red.
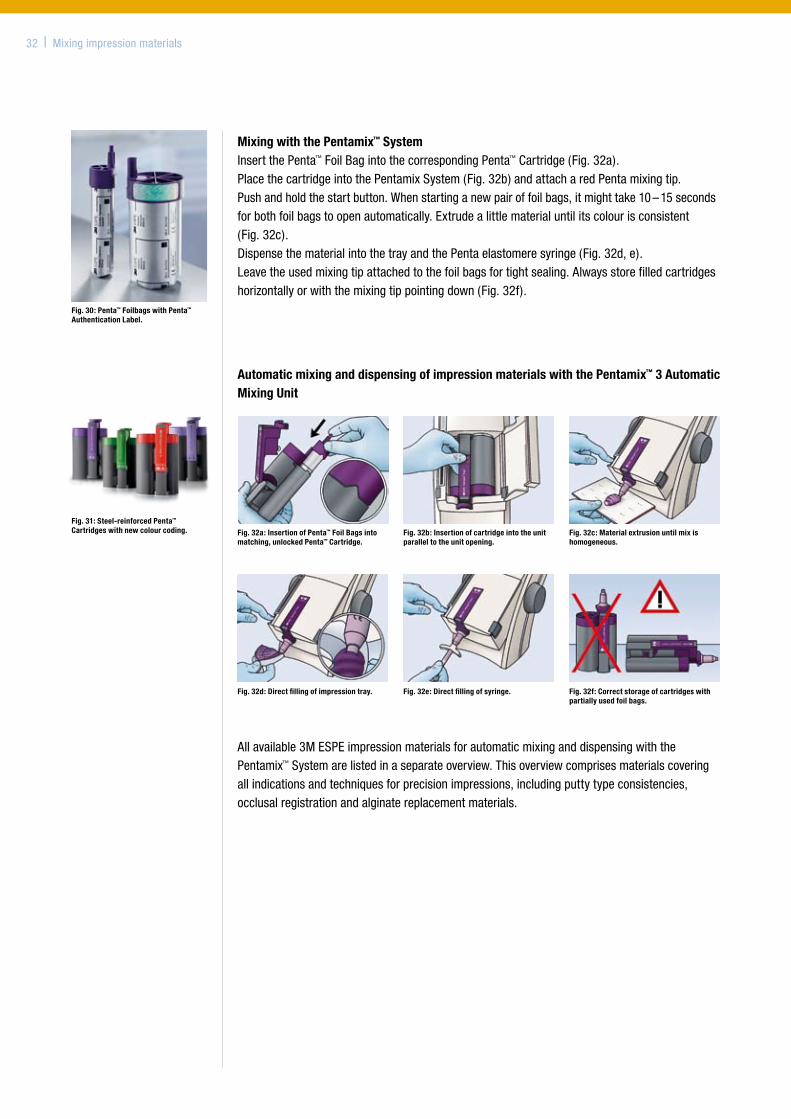
Mixing with the Pentamix™ System InsertthePenta™FoilBagintothecorrespondingPenta™Cartridge(Fig.32a).PlacethecartridgeintothePentamixSystem(Fig.32b)andattacharedPentamixingtip.Pushandholdthestartbutton.Whenstartinganewpairoffoilbags,itmighttake10–15secondsforbothfoilbagstoopenautomatically.Extrudealittlematerialuntilitscolourisconsistent(Fig.32c).DispensethematerialintothetrayandthePentaelastomeresyringe(Fig.32d,e).Leavetheusedmixingtipattachedtothefoilbagsfortightsealing.Alwaysstorefilledcartridgeshorizontallyorwiththemixingtippointingdown(Fig.32f).
32 | Mixingimpressionmaterials
Fig. 30: Penta™ Foilbags with Penta™ Authentication Label.
Fig. 31: Steel-reinforced Penta™ Cartridges with new colour coding.
Automatic mixing and dispensing of impression materials with the Pentamix™ 3 Automatic Mixing Unit
Allavailable3MESPEimpressionmaterialsforautomaticmixinganddispensingwiththePentamix™Systemarelistedinaseparateoverview. Thisoverviewcomprisesmaterialscoveringallindicationsandtechniquesforprecisionimpressions,includingputtytypeconsistencies,occlusalregistrationandalginatereplacementmaterials.
Fig. 32a: Insertion of Penta™ Foil Bags into matching, unlocked Penta™ Cartridge.
Fig. 32b: Insertion of cartridge into the unit parallel to the unit opening.
Fig. 32c: Material extrusion until mix is homogeneous.
Fig. 32d: Direct filling of impression tray. Fig. 32e: Direct filling of syringe. Fig. 32f: Correct storage of cartridges with partially used foil bags.
6. Impression techniques (B.Wöstmann)
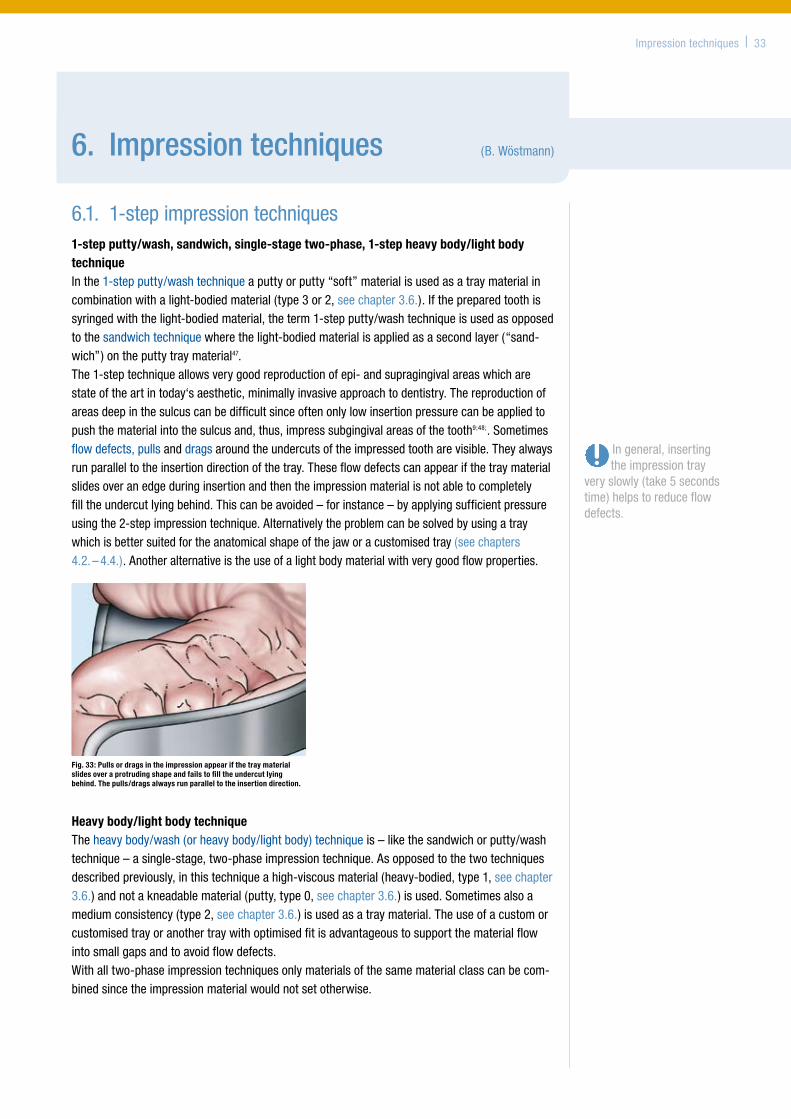
6.1. 1-stepimpressiontechniques1-step putty/wash, sandwich, single-stage two-phase, 1-step heavy body/light body techniqueInthe1-stepputty/washtechniqueaputtyorputty“soft”materialisusedasatraymaterialincombinationwithalight-bodiedmaterial(type3or2,seechapter3.6.).Ifthepreparedtoothissyringedwiththelight-bodiedmaterial,theterm1-stepputty/washtechniqueisusedasopposedtothesandwichtechniquewherethelight-bodiedmaterialisappliedasasecondlayer(“sand-wich”)ontheputtytraymaterial47.The1-steptechniqueallowsverygoodreproductionofepi-andsupragingivalareaswhicharestateoftheartintoday‘saesthetic,minimallyinvasiveapproachtodentistry.Thereproductionofareasdeepinthesulcuscanbedifficultsinceoftenonlylowinsertionpressurecanbeappliedtopushthematerialintothesulcusand,thus,impresssubgingivalareasofthetooth9;48;.Sometimesflowdefects,pullsanddragsaroundtheundercutsoftheimpressedtootharevisible.Theyalwaysrunparalleltotheinsertiondirectionofthetray.Theseflowdefectscanappearifthetraymaterialslidesoveranedgeduringinsertionandthentheimpressionmaterialisnotabletocompletelyfilltheundercutlyingbehind.Thiscanbeavoided–forinstance–byapplyingsufficientpressureusingthe2-stepimpressiontechnique.Alternativelytheproblemcanbesolvedbyusingatraywhichisbettersuitedfortheanatomicalshapeofthejaworacustomisedtray(seechapters4.2.–4.4.).Anotheralternativeistheuseofalightbodymaterialwithverygoodflowproperties.
Impressiontechniques | 33
Fig. 33: Pulls or drags in the impression appear if the tray material slides over a protruding shape and fails to fill the undercut lying behind. The pulls/drags always run parallel to the insertion direction.
Ingeneral,insertingtheimpressiontray
veryslowly(take5secondstime)helpstoreduceflowdefects.
Heavy body/light body techniqueTheheavybody/wash(orheavybody/lightbody)techniqueis–likethesandwichorputty/washtechnique–asingle-stage,two-phaseimpressiontechnique.Asopposedtothetwotechniquesdescribedpreviously,inthistechniqueahigh-viscousmaterial(heavy-bodied,type1,seechapter3.6.)andnotakneadablematerial(putty,type0,seechapter3.6.)isused.Sometimesalsoamediumconsistency(type2,seechapter3.6.)isusedasatraymaterial.Theuseofacustomorcustomisedtrayoranothertraywithoptimisedfitisadvantageoustosupportthematerialflowintosmallgapsandtoavoidflowdefects.Withalltwo-phaseimpressiontechniquesonlymaterialsofthesamematerialclasscanbecom-binedsincetheimpressionmaterialwouldnotsetotherwise.
Monophase techniqueInthemonophasetechnique,atype2(seechapter3.6.)materialconsistencyisusedasatraymaterialandforsyringingtheabutments.Sincestocktraysusuallycreatelesspressureuponinsertion,themonophasetechniqueisbestsuitedforusewithacustomisedtrayoranothertraywithoptimisedfitandanimpressionmaterialwithexcellentflowproperties.WithcustomtraysandanautomaticallymixedpolyetherorVPSmaterialextremelypreciseimpressionscanbeachieved25;49.
Hydrocolloid impressionAhydrocolloidimpressionisalsoa1-stepimpressionprocedure.Insteadofsiliconesorpoly-ethersareversiblethermoplastichydrocolloidisused.ThehydrocolloidtechniqueachievesresultswhicharecomparabletoVPSandpolyethermaterialswithregardtoaccuracy.However,itisnotthateasytoexactlyreproducesubgingivalareas50;51.Thisimpressiontechniqueinparticularshowstheimportanceofahighlystandardisedworkflowinthedentalpracticeforgoodandreproducibleresults.If,forexample,thematerialisonlyalittletoocold,itcannotbeapplied.Aslightlytoowarmmaterial,however,canbeperceivedbythepatientasratheruncomfortableorevencauseburns,whichalsoaffectsthequalityoftheimpression.
6.2.2-stepimpressiontechniques2-step putty/wash techniqueInthe2-stepputty/washtechniquewithsiliconesafirstimpressiontakenafterpreparationis“corrected“withamoreflowablematerial.Theinitialimpressionistakenwithaserialtrayandaputty(type0,seechapter3.6.)orheavybody(type1,seechapter3.6.)consistency.Thencarefulremovalofallundercutsandinterproximalseptaisessentialforthesuccessoftheimpression.Ifundercutsarenotremoved,displacementofthefirstimpressionmaterialwilloccurthroughthepressureoftheflowablematerialduringthesecondimpressionstepand,thus,errorsintheimpressionareinevitable.
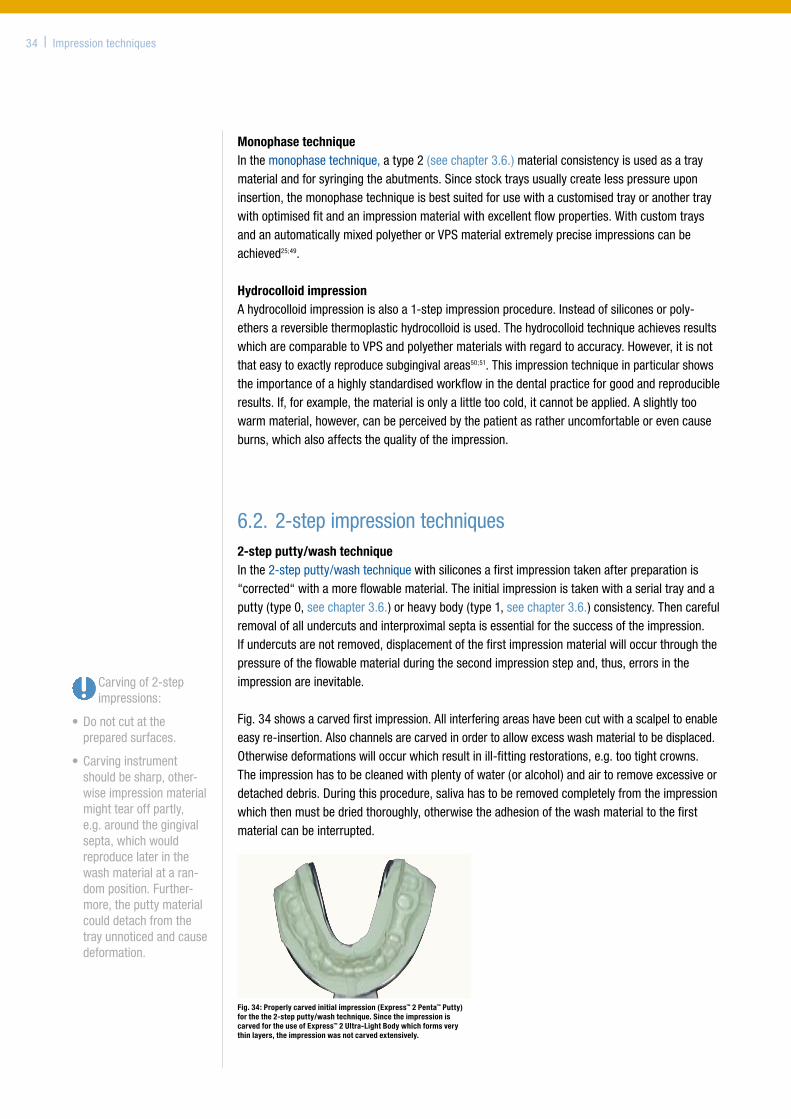
Fig.34showsacarvedfirstimpression.Allinterferingareashavebeencutwithascalpeltoenableeasyre-insertion.Alsochannelsarecarvedinordertoallowexcesswashmaterialtobedisplaced.Otherwisedeformationswilloccurwhichresultinill-fittingrestorations,e.g.tootightcrowns.Theimpressionhastobecleanedwithplentyofwater(oralcohol)andairtoremoveexcessiveordetacheddebris.Duringthisprocedure,salivahastoberemovedcompletelyfromtheimpressionwhichthenmustbedriedthoroughly,otherwisetheadhesionofthewashmaterialtothefirstmaterialcanbeinterrupted.
34 | Impressiontechniques
Fig. 34: Properly carved initial impression (Express™ 2 Penta™ Putty) for the the 2-step putty/wash technique. Since the impression is carved for the use of Express™ 2 Ultra-Light Body which forms very thin layers, the impression was not carved extensively.
Carvingof2-stepimpressions:
•Donotcutatthepreparedsurfaces.
•Carvinginstrumentshouldbesharp,other-wiseimpressionmaterialmighttearoffpartly,e.g.aroundthegingivalsepta,whichwouldreproducelaterinthewashmaterialataran-domposition.Further-more,theputtymaterialcoulddetachfromthetrayunnoticedandcausedeformation.
Eveniftheimpressionhasbeencarefullycarvedtheteetharereproducedslightlytoosmallduetothedistortionofthetraymaterial,whichcannotbecompletelyavoidedduetothematerials’inherentflexibility52–54.Thiscanbecompensatedforbythedentaltechnician,e.g.byapplyinganadditionallayerofspacer.
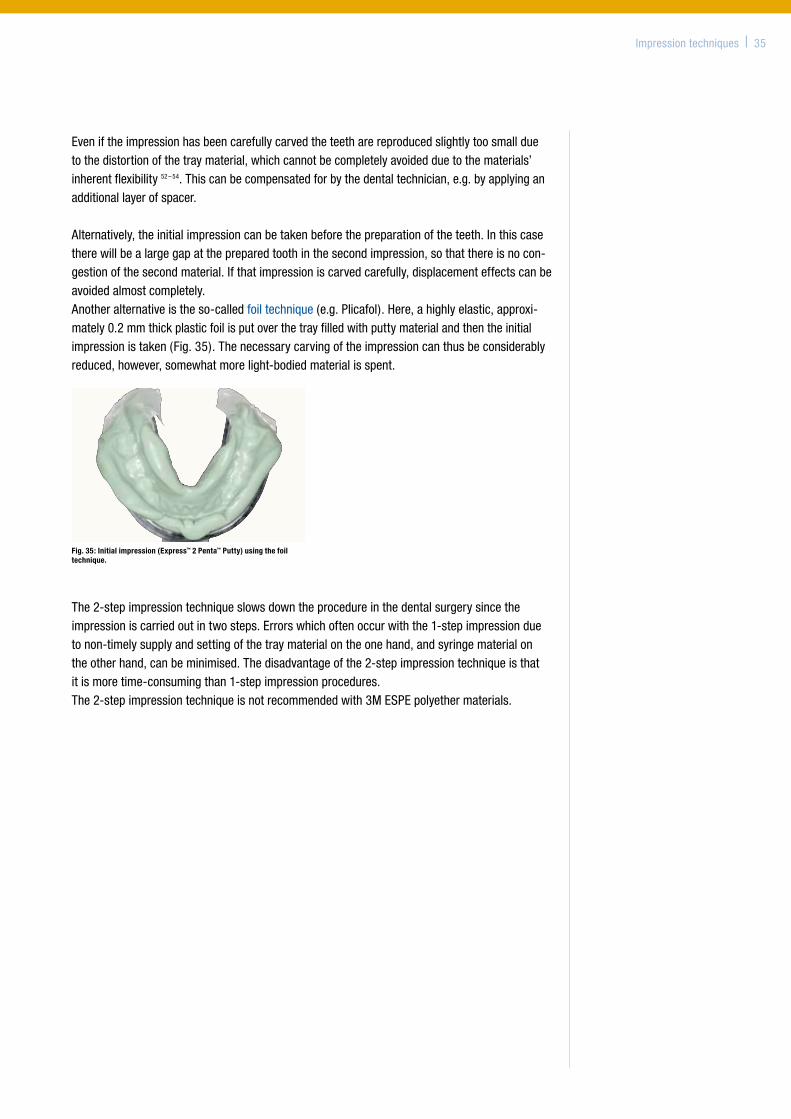
Alternatively,theinitialimpressioncanbetakenbeforethepreparationoftheteeth.Inthiscasetherewillbealargegapatthepreparedtoothinthesecondimpression,sothatthereisnocon-gestionofthesecondmaterial.Ifthatimpressioniscarvedcarefully,displacementeffectscanbeavoidedalmostcompletely.Anotheralternativeistheso-calledfoiltechnique(e.g.Plicafol).Here,ahighlyelastic,approxi-mately0.2mmthickplasticfoilisputoverthetrayfilledwithputtymaterialandthentheinitialimpressionistaken(Fig.35).Thenecessarycarvingoftheimpressioncanthusbeconsiderablyreduced,however,somewhatmorelight-bodiedmaterialisspent.
The2-stepimpressiontechniqueslowsdowntheprocedureinthedentalsurgerysincetheimpressioniscarriedoutintwosteps.Errorswhichoftenoccurwiththe1-stepimpressionduetonon-timelysupplyandsettingofthetraymaterialontheonehand,andsyringematerialontheotherhand,canbeminimised.Thedisadvantageofthe2-stepimpressiontechniqueisthatitismoretime-consumingthan1-stepimpressionprocedures.The2-stepimpressiontechniqueisnotrecommendedwith3MESPEpolyethermaterials.
Impressiontechniques | 35
Fig. 35: Initial impression (Express™ 2 Penta™ Putty) using the foil technique.
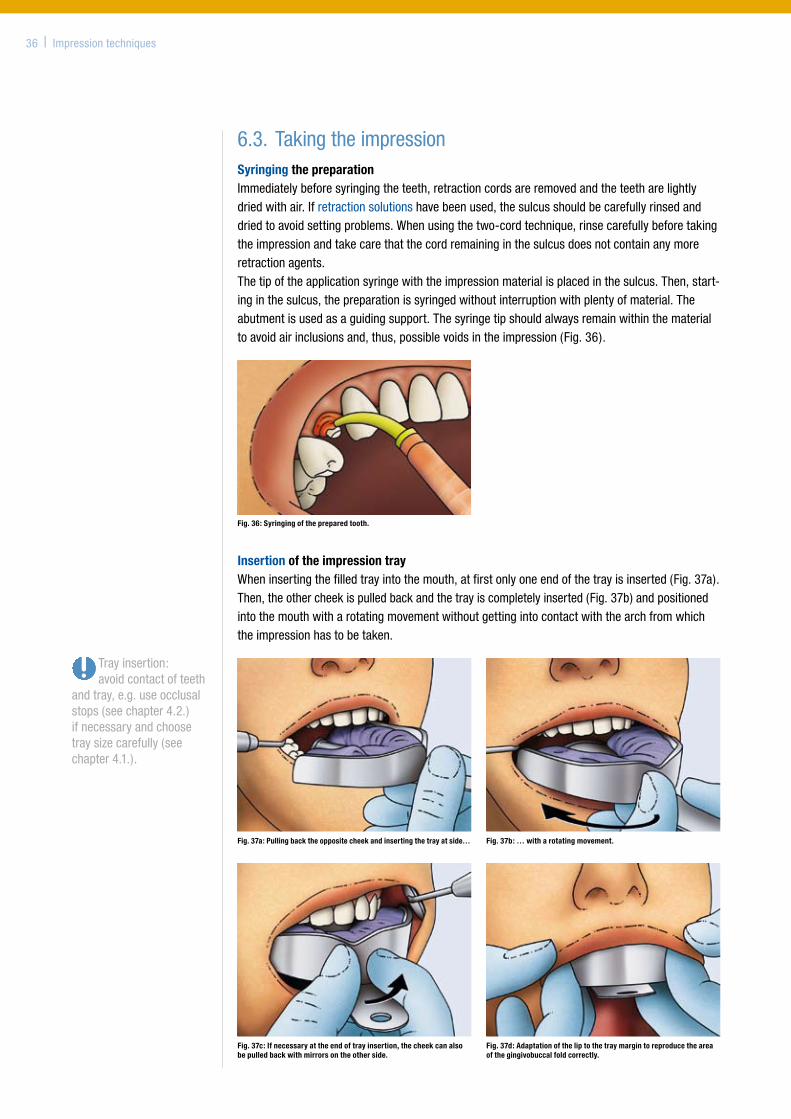
6.3.TakingtheimpressionSyringing the preparationImmediatelybeforesyringingtheteeth,retractioncordsareremovedandtheteetharelightlydriedwithair.Ifretractionsolutionshavebeenused,thesulcusshouldbecarefullyrinsedanddriedtoavoidsettingproblems.Whenusingthetwo-cordtechnique,rinsecarefullybeforetakingtheimpressionandtakecarethatthecordremaininginthesulcusdoesnotcontainanymoreretractionagents.Thetipoftheapplicationsyringewiththeimpressionmaterialisplacedinthesulcus.Then,start-inginthesulcus,thepreparationissyringedwithoutinterruptionwithplentyofmaterial.Theabutmentisusedasaguidingsupport.Thesyringetipshouldalwaysremainwithinthematerialtoavoidairinclusionsand,thus,possiblevoidsintheimpression(Fig.36).
Insertion of the impression trayWheninsertingthefilledtrayintothemouth,atfirstonlyoneendofthetrayisinserted(Fig.37a).Then,theothercheekispulledbackandthetrayiscompletelyinserted(Fig.37b)andpositionedintothemouthwitharotatingmovementwithoutgettingintocontactwiththearchfromwhichtheimpressionhastobetaken.
36 | Impressiontechniques
Fig. 37a: Pulling back the opposite cheek and inserting the tray at side… Fig. 37b: … with a rotating movement.
Fig. 37c: If necessary at the end of tray insertion, the cheek can also be pulled back with mirrors on the other side.
Fig. 37d: Adaptation of the lip to the tray margin to reproduce the area of the gingivobuccal fold correctly.
Fig. 36: Syringing of the prepared tooth.
Trayinsertion:avoidcontactofteeth
andtray,e.g.useocclusalstops(seechapter4.2.)ifnecessaryandchoosetraysizecarefully(seechapter4.1.).

Ifnecessary,thecheekcanalsobepulledbackwithmirrorsasshown(Fig.37c).Slowly,thetrayisadaptedinthedirectionofthepreparationandheldinthesamepositionwithoutpressurebythesamepersonuntilthematerialisset.
Setting process of the impression materialWhentakinganimpressionoftheupperjawyoucaneasilyfindsupportonthechinorcheekboneofthepatient(Fig.38).Thispreventsblurringoftheimpressionandthemovementsofthepatientcanbefollowed.Withimpressionsofthelowerjawitisrecommendedtosupportthetrayonthemandibula.Also,thepatientsshouldclosetheirmouthasmuchaspossibletoavoiddeformationofthemandibulaand,thus,errorsintheimpression.
Pleasenotethattheworkingtimestatedinthemanufacturers’instructionsforuse(accordingtoISO4823)mostlyrelatetoroomtemperature.Somemanufacturers(e.g.3MESPE)additionallylistaclinicallyrelevantworkingtime(e.g.atmouthtemperature),asduetothehighertempera-turesinsidethemouthofthepatientthematerialusedforsyringingthepreparedteethsetsfaster.Inanoptimisedworkflow,syringingtheteethandfillingthetrayshouldbecoordinatedsothatbothproceduresarefinishedsimultaneously.
Impressiontechniques | 37
Fig. 38: Extra-oral finger support on the zygomatic bone and intra-orally on both sides on the distal sections of the impression tray.
38 | Indications
7. Indications (B.Wöstmann)
Impressionsofunpreparedtoothstructuree.g.forastudymodelorthefabricationofanorthodonticsplintisnotsubjecttoasmanyconsiderationsasatrueprecisionimpressionforalaboratory-maderestoration.
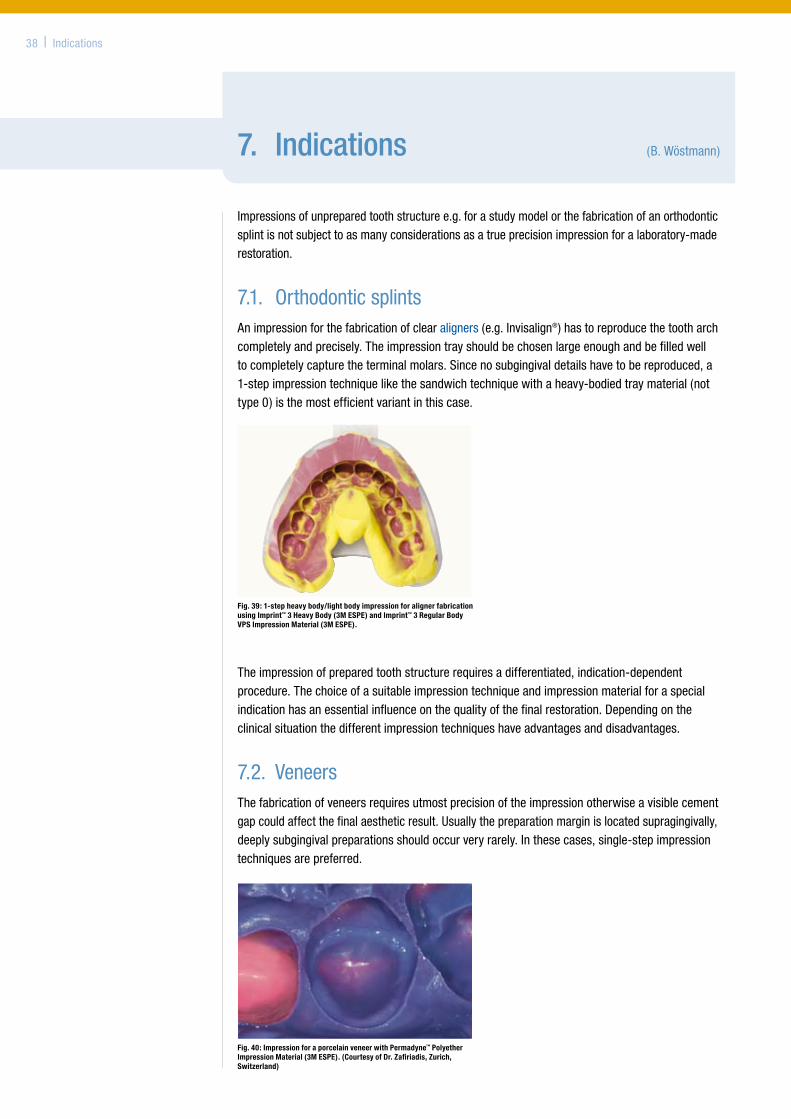
7.1. OrthodonticsplintsAnimpressionforthefabricationofclearaligners(e.g.Invisalign®)hastoreproducethetootharchcompletelyandprecisely.Theimpressiontrayshouldbechosenlargeenoughandbefilledwelltocompletelycapturetheterminalmolars.Sincenosubgingivaldetailshavetobereproduced,a1-stepimpressiontechniquelikethesandwichtechniquewithaheavy-bodiedtraymaterial(nottype0)isthemostefficientvariantinthiscase.
Theimpressionofpreparedtoothstructurerequiresadifferentiated,indication-dependentprocedure.Thechoiceofasuitableimpressiontechniqueandimpressionmaterialforaspecialindicationhasanessentialinfluenceonthequalityofthefinalrestoration.Dependingontheclinicalsituationthedifferentimpressiontechniqueshaveadvantagesanddisadvantages.
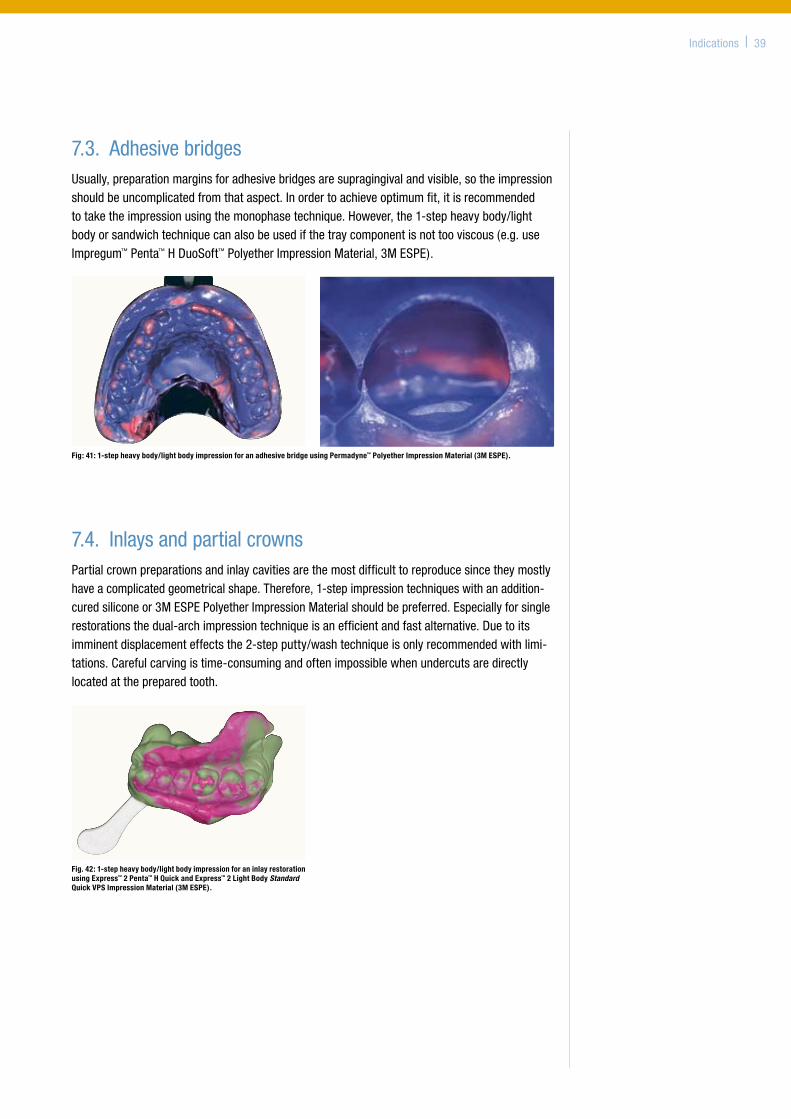
7.2. VeneersThefabricationofveneersrequiresutmostprecisionoftheimpressionotherwiseavisiblecementgapcouldaffectthefinalaestheticresult.Usuallythepreparationmarginislocatedsupragingivally,deeplysubgingivalpreparationsshouldoccurveryrarely.Inthesecases,single-stepimpressiontechniquesarepreferred.
Fig. 40: Impression for a porcelain veneer with Permadyne™ Polyether Impression Material (3M ESPE). (Courtesy of Dr. Zafiriadis, Zurich, Switzerland)
Fig. 39: 1-step heavy body/light body impression for aligner fabrication using Imprint™ 3 Heavy Body (3M ESPE) and Imprint™ 3 Regular Body VPS Impression Material (3M ESPE).
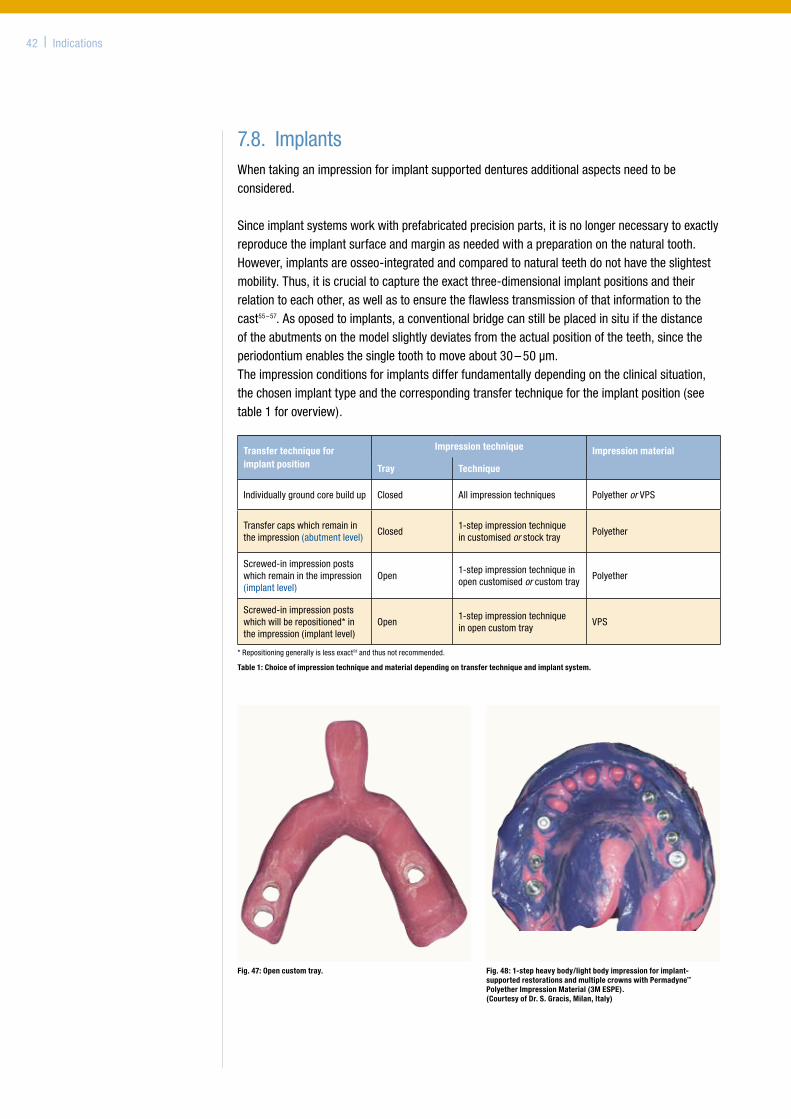
7.4. InlaysandpartialcrownsPartialcrownpreparationsandinlaycavitiesarethemostdifficulttoreproducesincetheymostlyhaveacomplicatedgeometricalshape.Therefore,1-stepimpressiontechniqueswithanaddition-curedsiliconeor3MESPEPolyetherImpressionMaterialshouldbepreferred.Especiallyforsinglerestorationsthedual-archimpressiontechniqueisanefficientandfastalternative.Duetoitsimminentdisplacementeffectsthe2-stepputty/washtechniqueisonlyrecommendedwithlimi-tations.Carefulcarvingistime-consumingandoftenimpossiblewhenundercutsaredirectlylocatedatthepreparedtooth.
Indications | 39
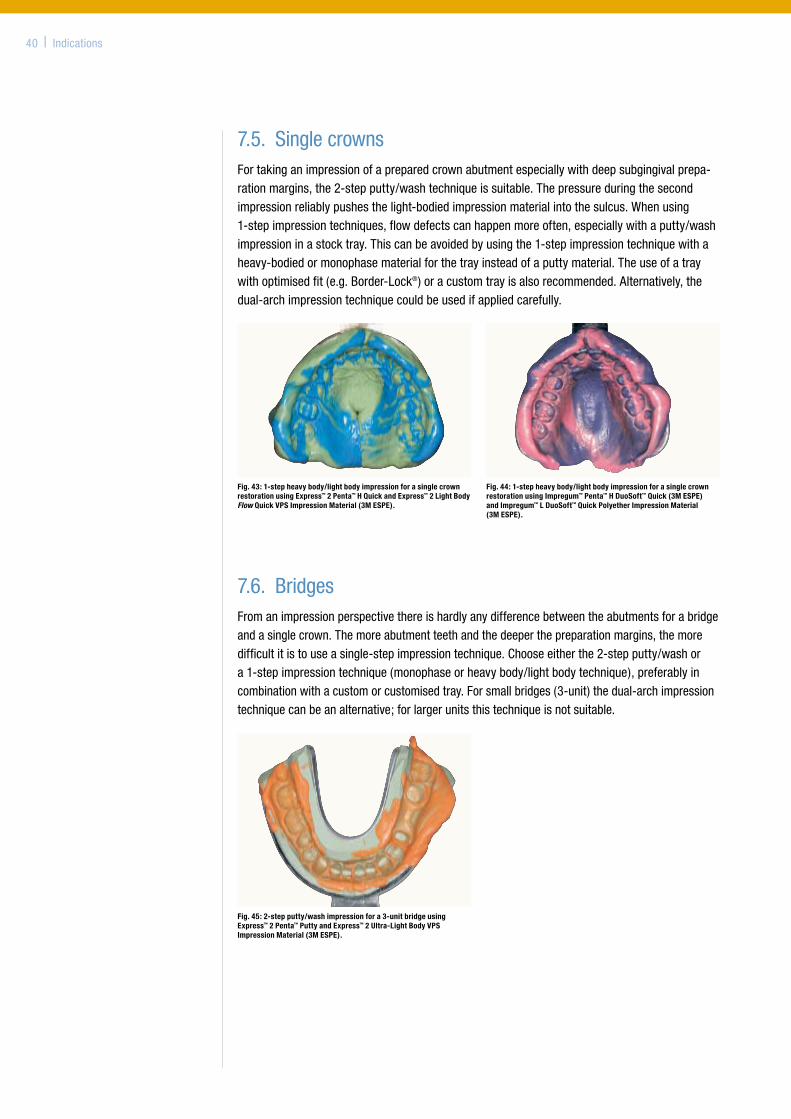
Fig: 41: 1-step heavy body/light body impression for an adhesive bridge using Permadyne™ Polyether Impression Material (3M ESPE).
Fig. 42: 1-step heavy body/light body impression for an inlay restoration using Express™ 2 Penta™ H Quick and Express™ 2 Light Body Standard Quick VPS Impression Material (3M ESPE).
7.3. AdhesivebridgesUsually,preparationmarginsforadhesivebridgesaresupragingivalandvisible,sotheimpressionshouldbeuncomplicatedfromthataspect.Inordertoachieveoptimumfit,itisrecommendedtotaketheimpressionusingthemonophasetechnique.However,the1-stepheavybody/lightbodyorsandwichtechniquecanalsobeusedifthetraycomponentisnottooviscous(e.g.useImpregum™Penta™HDuoSoft™PolyetherImpressionMaterial,3MESPE).
7.5. SinglecrownsFortakinganimpressionofapreparedcrownabutmentespeciallywithdeepsubgingivalprepa-rationmargins,the2-stepputty/washtechniqueissuitable.Thepressureduringthesecondimpressionreliablypushesthelight-bodiedimpressionmaterialintothesulcus.Whenusing1-stepimpressiontechniques,flowdefectscanhappenmoreoften,especiallywithaputty/washimpressioninastocktray.Thiscanbeavoidedbyusingthe1-stepimpressiontechniquewithaheavy-bodiedormonophasematerialforthetrayinsteadofaputtymaterial.Theuseofatraywithoptimisedfit(e.g.Border-Lock®)oracustomtrayisalsorecommended.Alternatively,thedual-archimpressiontechniquecouldbeusedifappliedcarefully.
7.6. BridgesFromanimpressionperspectivethereishardlyanydifferencebetweentheabutmentsforabridgeandasinglecrown.Themoreabutmentteethandthedeeperthepreparationmargins,themoredifficultitistouseasingle-stepimpressiontechnique.Chooseeitherthe2-stepputty/washora1-stepimpressiontechnique(monophaseorheavybody/lightbodytechnique),preferablyincombinationwithacustomorcustomisedtray.Forsmallbridges(3-unit)thedual-archimpressiontechniquecanbeanalternative;forlargerunitsthistechniqueisnotsuitable.
40 | Indications
Fig. 43: 1-step heavy body/light body impression for a single crown restoration using Express™ 2 Penta™ H Quick and Express™ 2 Light Body Flow Quick VPS Impression Material (3M ESPE).
Fig. 44: 1-step heavy body/light body impression for a single crown restoration using Impregum™ Penta™ H DuoSoft™ Quick (3M ESPE) and Impregum™ L DuoSoft™ Quick Polyether Impression Material (3M ESPE).
Fig. 45: 2-step putty/wash impression for a 3-unit bridge using Express™ 2 Penta™ Putty and Express™ 2 Ultra-Light Body VPS Impression Material (3M ESPE).

Indications | 41
Fig. 46: Monophase impression with fixed primary copings using Impregum™ Penta™ Polyether Impression Material (3M ESPE). (Courtesy of Dr. P. Chlum, Saalburg, Germany)
7.7. CombinationdenturesForthefabricationofcombinationdentures,twodifferentimpressionproblemshavetobesolved.Ontheonehand,abutmentteethhavetobereproducedand,ontheotherhand,mucogingivalareasandtheirrelationtotheteethhavetobereproduced.Forthereproductionoftheabutmentteeththesameguidelinesapplyasfortheimpressionofcrownsandbridges.Afterfabricationandseatingoftheprimarycopings,theimpressioniscarriedoutwithacustom-madetray.Here,theuseofpolyethermaterialsisadvantageous,sincetheyfavoursafefixationoftheprimarycopingsinthetotalimpressionduetotheirhighadhesion.Secondly,functionalmarginaladapta-tionispossiblesincethepatientcanmakefunctionalmovementsduringthesettingphaseoftheimpressionmaterial,and,thus,themobileareasofthemucosacanbereproducedintheirmaximumextension.(Ifapolyetherisusedforthefunctionalimpressionofatoothlessjaw,itcanbeadvantageoustousethePolyetherRetardertoprolongandadjusttheworkingtimeoptimallytotheclinicalrequire-ments).Alternatively,thesecondaryframecanbefabricatedontheprimarilyproducedstudymodelifitcontainsallthenecessaryinformation.
42 | Indications
Fig. 47: Open custom tray. Fig. 48: 1-step heavy body/light body impression for implant- supported restorations and multiple crowns with Permadyne™ Polyether Impression Material (3M ESPE). (Courtesy of Dr. S. Gracis, Milan, Italy)
Transfer technique for implant position
Impression technique Impression material
Tray Technique
Individuallygroundcorebuildup Closed Allimpressiontechniques PolyetherorVPS
Transfercapswhichremainintheimpression(abutmentlevel)
Closed1-stepimpressiontechniqueincustomisedorstocktray
Polyether
Screwed-inimpressionpostswhichremainintheimpression(implantlevel)
Open1-stepimpressiontechniqueinopencustomisedorcustomtray
Polyether
Screwed-inimpressionpostswhichwillberepositioned*intheimpression(implantlevel)
Open1-stepimpressiontechniqueinopencustomtray
VPS
*Repositioninggenerallyislessexact58andthusnotrecommended.
7.8. ImplantsWhentakinganimpressionforimplantsupporteddenturesadditionalaspectsneedtobeconsidered.
Sinceimplantsystemsworkwithprefabricatedprecisionparts,itisnolongernecessarytoexactlyreproducetheimplantsurfaceandmarginasneededwithapreparationonthenaturaltooth.However,implantsareosseo-integratedandcomparedtonaturalteethdonothavetheslightestmobility.Thus,itiscrucialtocapturetheexactthree-dimensionalimplantpositionsandtheirrelationtoeachother,aswellastoensuretheflawlesstransmissionofthatinformationtothecast55–57.Asoposedtoimplants,aconventionalbridgecanstillbeplacedinsituifthedistanceoftheabutmentsonthemodelslightlydeviatesfromtheactualpositionoftheteeth,sincetheperiodontiumenablesthesingletoothtomoveabout30–50µm.Theimpressionconditionsforimplantsdifferfundamentallydependingontheclinicalsituation,thechosenimplanttypeandthecorrespondingtransfertechniquefortheimplantposition(seetable1foroverview).
Table 1: Choice of impression technique and material depending on transfer technique and implant system.
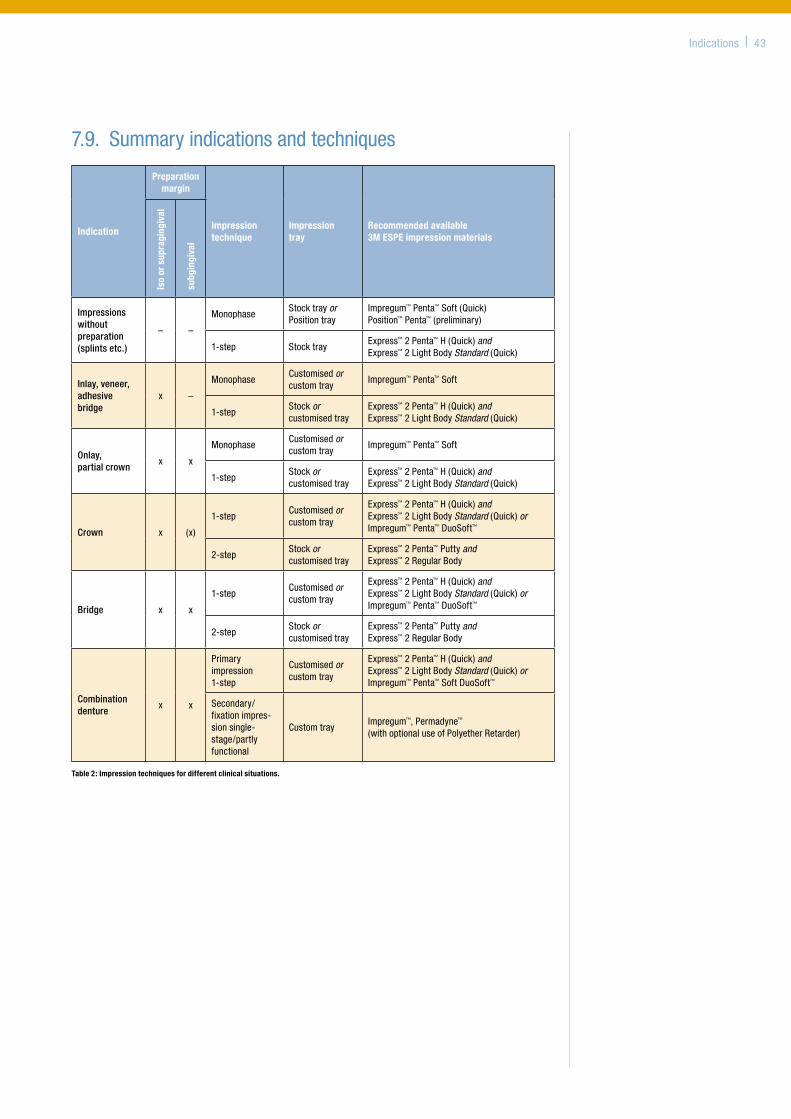
Indications| 43
7.9. Summaryindicationsandtechniques
Indication
Preparation margin
Impression technique
Impression tray
Recommended available 3M ESPE impression materials
Iso
or s
upra
ging
ival
subg
ingi
val
Impressions without preparation (splints etc.)
– –
MonophaseStocktrayorPositiontray
Impregum™Penta™Soft(Quick)Position™Penta™(preliminary)
1-step StocktrayExpress™2Penta™H(Quick)andExpress™2LightBodyStandard(Quick)
Inlay, veneer, adhesive bridge
x –
MonophaseCustomisedorcustomtray
Impregum™Penta™Soft
1-stepStockorcustomisedtray
Express™2Penta™H(Quick)andExpress™2LightBodyStandard(Quick)
Onlay, partial crown
x x
MonophaseCustomisedorcustomtray
Impregum™Penta™Soft
1-stepStockorcustomisedtray
Express™2Penta™H(Quick)and Express™2LightBodyStandard(Quick)
Crown x (x)
1-stepCustomisedorcustomtray
Express™2Penta™H(Quick)andExpress™2LightBodyStandard(Quick)orImpregum™Penta™DuoSoft™
2-stepStockorcustomisedtray
Express™2Penta™PuttyandExpress™2RegularBody
Bridge x x
1-stepCustomisedorcustomtray
Express™2Penta™H(Quick)andExpress™2LightBodyStandard(Quick)orImpregum™Penta™DuoSoft™
2-stepStockorcustomisedtray
Express™2Penta™PuttyandExpress™2RegularBody
Combination denture
x x
Primaryimpression1-step
Customisedorcustomtray
Express™2Penta™H(Quick)andExpress™2LightBodyStandard(Quick)orImpregum™Penta™SoftDuoSoft™
Secondary/fixationimpres-sionsingle-stage/partlyfunctional
CustomtrayImpregum™,Permadyne™(withoptionaluseofPolyetherRetarder)
Table 2: Impression techniques for different clinical situations.

Fig: 51: Impression material specimens contaminated with human saliva carry a multitude of potentially pathogenic microorganisms despite thorough rinsing with water.
Fig: 52: Impresept™ Immersion Disinfectant (3M ESPE) effectively kills microorganisms. After incubation on blood agar no colony-forming units can be detected.
8. Disinfection (B.Wöstmann)
Infectioncontrolisoneofthemostessentialtasksinthedentalpractice.Impressionsaremajorcarriersofbacteriaandvirusessincetheyarecontaminatedwithsalivaandoftenwithblood.Disinfectionensurestheinterruptionoftheinfectionchainbetweendentalpracticeandlaboratoryandprotectsthedentaltechnician.Soeachimpressionshouldbedisinfectedroutinelybeforeforwardingittothedentallabtopreventcontamination.
Impressionsshouldbedisinfectedassoonastheyareremovedfromthemouth.Eachdelaycancauseanincreaseinthenumberofmicroorganisms.Eachimpressionshouldbecarefullyrinsedunderrunningwaterbeforedisinfection,otherwisethebacteriaandviruseswhichshouldbedestroyedcanbeprotectedbysalivaorbloodproteinsandthedisinfectionsolutioncannotreliablydestroythegermsinthestatedimmersiontime.
Disinfectionaimsatreducingthenumberofgermsbyatleastafactorof105.Thus,inmostcasesspraydisinfectionisnotenoughascompletesurfacewettingcannotbeensured.Completeimmersionindisinfectantguaranteessufficientdisinfection59.Theimmersionbathshouldbeinasealablecontainertoavoidevaporationofthedisinfectionagentand,thus,enrichmentintheair.
Onlyusedisinfectantswhichhavebeenespeciallydevelopedandreleasedforimpressionmaterials(e.g.basedonaldehydeorperaceticacid:alcoholasdisinfectantisnotsufficientforsomegerms).Makesurethatthedisinfectantiscompatiblewiththeimpressionmaterialaswellaswiththestoneusedformodelfabrication60;61.Disinfectionsolutionsbasedonalcohol(insteadofwater)asasolventmaycauseswellingoftheimpressionsand,thus,ill-fittingrestorations.
Water-basedimpressionmaterialslikealginatesandhydrocolloidsarepronetoswellingandshouldthereforeremaininthedisinfectionbathforasshortatimeaspossible.Polyether,poly-sulfidesandsilicones,especiallyaddition-curedmaterialsarelesssensitive.Impresept™ImmersionDisinfectant(3MESPE)hasashortimmersiontimeandissuitableforallmaterials.Afterdisinfectiontheimpressionshouldberinsedagainunderrunningwateranddried.
Furthermore,pleasefollowtherecommendationsoftherespectiveassociationsforhygieneandoccupationalhealthandsafetyaswellasthemanufacturers’instructions62.
44 | Disinfection
Fig: 49: Immerse the impression trays completely. Action time 10 minutes (Impresept™, 3M ESPE).
Fig: 50: Let the impression drain in the basket after the immersion time and rinse with water. Exchange solution after one week.
Popularbrands:• Impresept™
(3MESPE)
9. Storage of the impression and transport to the dental lab (B.Wöstmann)
Onthewayfromthepracticetothedentallabtheimpressionisbestcarriedinacontainer,securelyfixedinfoam.Inappropriatetransportandstorageconditionscanleadtofurtherchangesindimension63,e.g.byoverheatingorabsorptionorreleaseofmoisture.Alginatesandhydrocolloidsshouldbecastimmediately(usuallyinthedentalpractice).Iftransportisinevitable,theimpressionshouldbestoredinhygrophororalternativelyinaresealableplasticbagtogetherwithamoist(notwet)papertowel.C-siliconeorpolysulfideimpressionsshouldbecastassoonaspossibleaswell,sincetheyarenotdimensionallystable.Polyetherimpressionsmustbesentseparatelyfromalginateimpressionsandshouldbetrans-portedandstoreddry,coldandprotectedfromdirectsunlight.Undertheseconditionstheycanbekeptforuptotwoweeks.VPSmaterialshavethemostfavourablematerialpropertiesforstorage.However,theyshouldalsobekeptandtransporteddryandnotaboveroomtemperature.Inanycasepleasefollowthemanufacturers’instructionsforuse.
Storage | 45
10. Fabrication of the stone model (B.Wöstmann)
Impressionsandmodelsarecloselyconnected.Basically,thesuccessfullyfabricatedmodelisthecompletionofthetreatmentstep“impression”.
10.1.StandardisationofthemodelfabricationEspeciallywhenusingVPSmaterials,thethermalcontractionofthematerialwhencoolingdownfrommouthtoroomtemperatureshouldnotbeunderestimated,sincetheextentofthiscontractioniscomparablyhigh64.Heatingtheimpressiontomouthtemperaturebeforepouring,however,isnotusefulsincethisprocessisneverreproducibleand,thus,cannotbestandardised.Forconse-quentstandardisationoftheprocessitismuchmorebenefitialtocompensateforthedimensionalerrorwithtargeteddentaltechnicalmethods.Thedentaltechnicianadjustsprocessesinresponsetoimpressionmaterial,trayandinformationreceivedfromthedentist(e.g.useofspacer,embed-dingmass,gypsumexpansion,controlofthemillingmachine,etc.)andcarriesoutcastingoftheimpressionunderconstantconditions(roomtemperature,watertemperatureetc.).
Resin-basedmodelmaterials,(e.g.epoxyresins)areusedlessfrequently.Someofthesematerialsarenotdirectlycompatiblewith3MESPEpolyetherimpressionmaterialsandcanonlybeusedwithaseparatorwhichcompletelysealsthesurface.Silverplatingof3MESPEpolyetherimpressionsinthegalvanisationbathispossible,butcopperplatingisnotpossibleforchemicalreasons.
10.2. ModelsystemsThesectionedmodelisstilloneofthemostusedmodelsystems.Inordertoworkonthemodelaremovalofthestonetissueisusuallynecessaryaroundthepreparationmargin.However,thesegypsumparts,oftenregardedassuperfluous,reproducethesofttissues.Inmostcasestheyfacilitateacorrectshapingofthecrown,sinceithastocorrectlyfittothepreparedtoothaswellasharmonisewiththeperiodontaltissue.Ifnecessary,aremovabletissue(gingivamask)hastobeprepared.Alternatively,modelsystemswithprefabricatedbasesorbasemouldscanbeused.
Theproblemwiththesesystemsis,however,thatthegypsumarchesexpandduringsettingand,thus,areputunderstressbeingfixedtothestablebase.Thesestressesarereleasedafterremovalfromthebaseplate,whichmightleadtodifficultiesincorrectlyrepositioningthetootharchlater.Theteethhavetobepinned,thensectionedintosmallsegmentseachofwhichcanberepositionedexactly.Still,highlyprecisemodelscanbefabricatedifthistechniqueisskilfullyused65–67.Modelsystemswithafinelydetailedbaseplateshouldbeavoidedsincecompleterepositioninginverticaldimensionissometimesdifficultorimpossible.
46 | Stonemodel
Fig: 53: Sectioned stone model.
10.3. TimingofthemodelfabricationCastBeforepouringthemastercasttheimpressionshouldbetrimmed.Theexcessimpressionmate-rialwhichdoesnotcontainanyinformationforthefabricationofthemastercastisremoved.Sinceeachimpressionisdeformeduponmouthremoval,theimpressionmaterialneedstimeforelasticrecoverybeforemodelfabrication.Usually,theminimumtimerequiredvariesbetween30minutesto2hours.All3MESPEpolyetherscanbecastafter30minutes.
Themanufacturers’instructionsmustalwaysbefollowed.EspeciallywithVPSimpressions,voidsinthestonemodelmaybearesultofcastingtooearly–reflectingacontinuingpolymerisationreactionduringwhichhydrogengasisreleased.Furthermore,thecastshouldberemovedfromthemouldonlyafterthetimestatedbythemanu-facturer.Carefulremovalofthearchisessential.Ifnecessary,itcanbecarefullyloosenedatthemarginwithaknife(thisiscomparabletobreakingthevacuumwhenlooseninganimpressioninthepatient’smouth,seechapter2.6.)thenremovetheimpressioninaflowingmovementtowardsthefrontteeth.Ifimpressionmaterialswithahighfinalhardnessareused,theimpressiontraycanberemovedfirst,ifpossible.Then,theflexibleimpressionmaterialcanbepulledoffthecastmucheasier.Alternatively,thetray(e.g.ofa3MESPEpolyetherimpression)canbewarmed,e.g.ontheradia-tor–butnotinahotwaterbath.Donotexceedamaximumtemperatureof40–45°C.Iftheimpressionneedstobecastasecondtime,itmustbegiventimetorecoverfromdeformationuponremovalofthefirstcast.
BaseThemodelbaseshouldbeofatypeIVorVstoneoraspecialbasestonewithalowexpansioncoefficienttokeepexpansionand,thus,errorsaslowaspossible.SuchspecialbasestoneshavealowerhardnessthantypeIVstone,buthavethesameorbetter(i.e.less)expansionbehaviour.TheusualtypeIIIstoneisobsolete.Itleadstoconsiderabledimensionalchangesofthemodel.Thehighlyexpandingstoneevenfurtherexpandsthefinishedtootharchfixedtoit.Themodelbaseisideallyimmediatelypreparedafterremovalofthecastarchorupto24hourslater.Ifthemodelbaseispreparedimmediatelythetootharchisnotsectionedimmediately,sincebaseandarchundergothesameexpansionbehaviour.Afterfabricationandfinalsettingofthemodelbase,thetootharchhastobetrimmedoffthebase.Otherwisethearchisunderstresswhichmightcausecracksandtears.Hardenedstoneishygroscopic.Ittakesupmoisturefromtheairandshouldbestoreddrytoavoidsurfaceanddimensionalchanges.
Stonemodel | 47
Fig: 54: Courtesy of J. H. Bellmann, MDT, Rastede, Germany.

11. Conclusion (B.Wöstmann)
Whatfurtherdevelopmentscanbeexpectedintheareaofimpressioning?High-techproceduresconnectedtoopticalimpressioningwillbeimprovedmoreandmore.This,however,doesnotsolvethebasicclinicalproblems.Allavailableimpressionmethodsallowonlyforthereproductionofaccessibleareas,irrespectiveoftheuseofanelastomericimpressionmaterialorascannerasreproductionmedia.
Accessible,visibleareascanbereproducedwithoutmanyproblems,andthesubsequentworkandmaterialflowissufficientlyexacttoachievegoodrestorations.Basically,today‘simpressionmaterialsandmethodsdeliverexcellentresults.Inordertotakeadvantageoftheirfullcapabilitiesitisessentialtorespecttheclinicalandprocess-relevant parametersdiscussedinthisdocument.Theyareoftenunderestimatedbutarethekeytoachievingresultscorrespondingtothehighlevelsofmaterialsciencebehindtodaysimpressionmaterials.
Followingastructuredprocedureduringimpressioninginconjunctionwithgoodcommunicationandcooperationwiththedentaltechnician(and,ofcourse,avoidingconsequentlyclinicalsourcesoferror)youcanproducerestorationswhichfullfilthehighestbiologicalaswellasaestheticrequirements.
48 | Conclusion
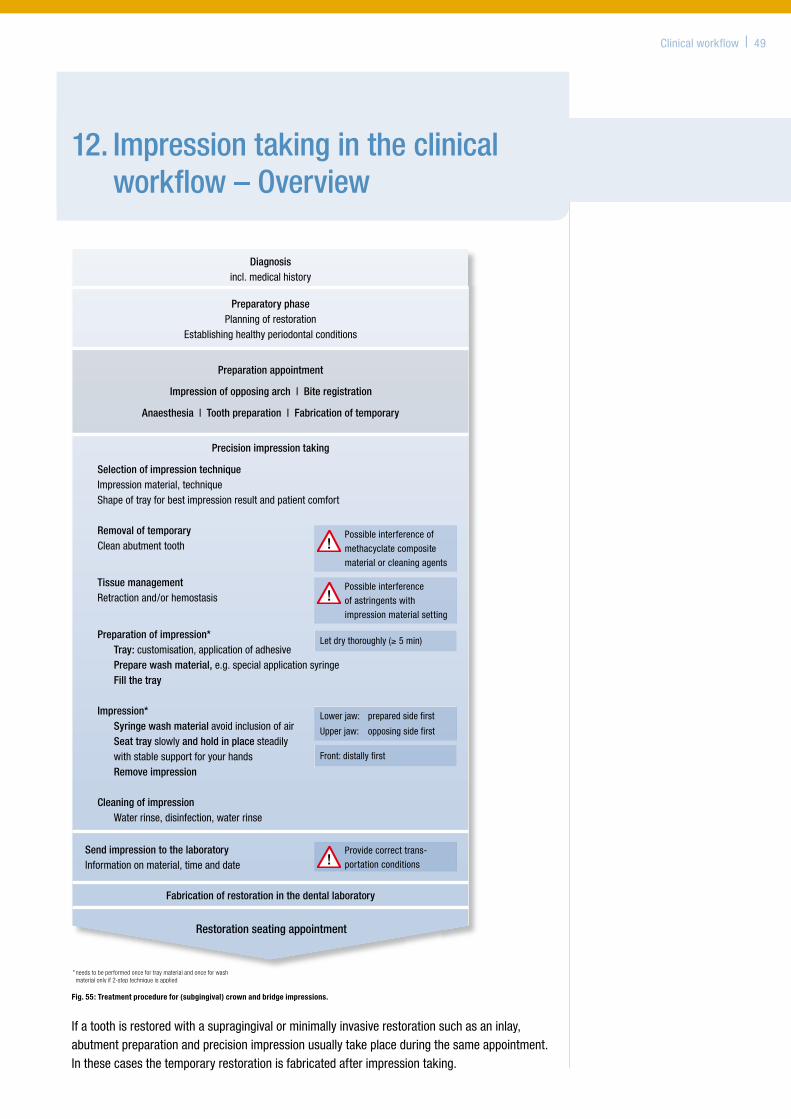
Clinicalworkflow | 49
12. Impression taking in the clinical workflow – Overview
Ifatoothisrestoredwithasupragingivalorminimallyinvasiverestorationsuchasaninlay,abutmentpreparationandprecisionimpressionusuallytakeplaceduringthesameappointment.Inthesecasesthetemporaryrestorationisfabricatedafterimpressiontaking.
Preparatory phasePlanning of restoration
Establishing healthy periodontal conditions
Preparation appointment
Impression of opposing arch | Bite registration
Anaesthesia | Tooth preparation | Fabrication of temporary
Precision impression taking
Selection of impression technique Impression material, technique Shape of tray for best impression result and patient comfort
Removal of temporaryClean abutment tooth
Tissue management Retraction and/or hemostasis
Preparation of impression* Tray: customisation, application of adhesive Prepare wash material, e.g. special application syringe Fill the tray
Impression* Syringe wash material avoid inclusion of air Seat tray slowly and hold in place steadily
with stable support for your hands Remove impression
Cleaning of impression Water rinse, disinfection, water rinse
Possible interference of
methacyclate composite
material or cleaning agents
Possible interference
of astringents with
impression material setting
Lower jaw: prepared side first
Upper jaw: opposing side first
Let dry thoroughly (≥ 5 min)
Front: distally first
Restoration seating appointment
Fabrication of restoration in the dental laboratory
* needs to be performed once for tray material and once for wash material only if 2-step technique is applied
Diagnosisincl. medical history
Send impression to the laboratoryInformation on material, time and date
Provide correct trans-
portation conditions
Fig. 55: Treatment procedure for (subgingival) crown and bridge impressions.
13. Literature
References
1. KnoernschildKL,CampbellSD.Periodontal tissue responses after insertion of artificial crowns and fixed partial dentures. JProsthetDent2000;84:492-498.
2. MüllerN,PröschelP.Kronenrand und parodontale Reaktion Ergebnisse einer histopathologischen Studie an 368 Sektionspräparaten. DtschZahnärztlZ1994;49:30-36.
3. TurnerCH.A retrospective study of the fit of jacket crowns placed around gold posts and cores, and the associated gingival health. JOralRehabil1982;9:427-434.
4. TjanAH,LiT,LoganGI,BaumL.Marginal accuracy of complete crowns made from alternative casting alloys. JProsthetDent1991;66:157-164.
5. TinschertJ,NattG,MautschW,SpiekermannH,AnusaviceKJ.Marginal fit of alumina- and zirconia-based fixed partial dentures produced by a CAD/CAM system. OperDent2001;26:367-374.
6. GelbardS,AoskarY,ZalkindM,SternN.Effect of impression materials and techniques on the marginal fit of metal castings. JProsthetDent1994;71:1-6.
7. WöstmannB,KraftA,FergerP.Accuracy of impressions attainable in vivo. JDentRes1998;77:798.8. KernM,SchallerHG,StrubJR.Marginal Fit of Restaurations Before and After Cementation.
IntJProsthodont1993;6:585-591.9. WöstmannB,BlösserT,GouentenoudisM,BalkenholM,FergerP.Influence of margin design on the fit of
high-precious alloy restorations in patients. JDent2005;33:611-618.10. DiedrichP,ErpensteinH.Rasterelektronenmikroskopische Randspaltanalyse von in vivo eingegliederten
Stufenkronen und Inlays. SchweizMonatsschrZahnmed1985;95:575-586.11. WolfBH,WalterMH,BoeningKW,SchmidtAE.Margin quality of titanium and high-gold inlays and onlays – a
clinical study. DentMater1998;14:370-374.12. BoeningKW,WolfBH,SchmidtAE,KastnerK,WalterMH.Clinical fit of Procera AllCeram crowns.
JProsthetDent2000;84:419-424.13. MeinersH.Prophylaxe und Werkstoffkunde. ZahnärztlWelt1985;94:792-798.14. PospiechP,WildenhainM.Zur Frage der Mischbarkeit von Polyetherabformstoffen – ein Vergleich zwischen
Hand und dynamischer Mischung. DentalSpiegel1998.15. Wöstmann,B.Clinical parameters of impression techniques in dentistry.
ZStomatol93,531-532.1996.16. WöstmannB.Klinische Bestimmungsvariablen bei der Abformung präparierter Zähne.
ZStomatol1996;93:51-57.17. KernM,SchallerHG,StrubJR.Randschluß von Konuskronen vor und nach der Zementierung.
QuintessZahnärztlLit1994;45:37-48.18. KimotoK,TanakaK,ToyodaM,OchiaiKT.Indirect latex glove contamination and its inhibitory effect on
vinyl polysiloxane polymerization. JProsthetDent2005;93:433-438.19. RodriguesFilhoLE,MuenchA,FrancciC,LuebkeAK,TrainaAA.The influence of handling on the elasticity
of addition silicone putties. PesquiOdontolBras2003;17:254-260.20. ClancyJM,ScandrettFR,EttingerRL.Long-term dimensional stability of three current elastomers.
JOralRehabil1983;10:325-333.21. LinCC,DoneganSJ,DhuruVB.Accuracy of impression materials for complete-arch fixed partial dentures.
JProsthetDent1988;59:288-291.22. MeinersH,LehmannKM.Klinische Materialkunde für Zahnärzte. München–Wien:CarlHanser,1998.23. AnusaviceKJ.Phillips‘ Science of Dental Materials. 11ed.Philadelphia:W.B.Saunders,2003.24. EichnerK,KappertHF.Zahnärztliche Wertkstoffe und ihre Verarbeitung. 6ed.Heidelberg:Hüthig,1996.25. WöstmannB.Zum gegenwärtigen Stand der Abformung in der Zahnheilkunde. Berlin:Quintessenz,1998.26. WöstmannB.Accuracy of impressions obtained with the Pentamix automixing system.
JDentRes1997;76:139.27. GerrowJD,SchneiderRL.A comparison of the compatibility of elastomeric impression materials, type IV
dental stones, and liquid media. JProsthetDent1987;57:292-298.28. PowersJM,SakaguchiRL.Impression materials. Craig‘s restorative dental materials.
ElsevierMosby,2006:294-95.29. HembreeJH,Jr.,AndrewsJT.Accuracy of a polyether impression material.
ArkDentJ1976;47:10-11.30. SpranleyTJ,GettlemanL,ZimmermanKL.Acute tissue irritation of polysulfide rubber impression materials.
JDentRes1983;62:548-551.31. NayyarA,TomlinsCD,FairhurstCW,OkabeT.Comparison of some properties of polyether and polysulfide
materials. JProsthetDent1979;42:163-167.32. PetrieCS,WalkerMP,WilliamsK.A survey of U.S. prosthodontists and dental schools on the current materials
and methods for final impressions for complete denture prosthodontics. JProsthodont2005;14:253-262.
50 | Literature
33. KanehiraM,FingerWJ,EndoT.Volatilization of components from and water absorption of polyether impressions.JDent2006;34:134-138.
34. KandelmanD,MeyerJM,LamontagneP,NallyJN.Etudes comperative de 3 hydrocoillides irreversibles. SchweizMonatsschrZahnheilkd1978;88:134-152.
35. WöstmannB,LammertU,FP.Analysis of fit of stock trays for dentate jaws. JDentRes2002;81:A-60.
36. WöstmannB.Entwicklung neuer Abformlöffel für vollbezahnte Unterkiefer. DentMagazin1991;62-66.
37. BombergTJ,HatchRA,HoffmannWJ.Impression material thickness in stock and custom trays. JProsthetDent1985;54:170-173.
38. WirzJ.Materialien für individuelle Abformlöffel. DtschZahnärztlZ1982;92:207-211.39. MarxkorsR.Abformung bezahnter Kiefer mit individuellen Löffeln.
ZahnärztlWelt1978;87:682-684.40. ThongthammachatS,MooreBK,BarcoMT,HovijitraS,BrownDT,AndresCJ.Dimensional accuracy of dental
casts: influence of tray material, impression material, and time. JProsthodont2002;11:98-108.41. WirzJ,SchmidliF.Individuelle Abformlöffel. SchweizMonatsschrZahnmed1987;97:1417-142.42. MillsteinP,MayaA,SeguraC.Determining the accuracy of stock and custom tray impression/casts.
JOralRehabil1998;25:645-648.43. MartinezLJ,vonFraunhoferJA.The effects of custom tray material on the accuracy of master casts.
JProsthodont1998;7:106-110.44. AbdullahMA,TalicYF.The effect of custom tray material type and fabrication technique on tensile bond
strength of impression material adhesive systems. JOralRehabil2003;30:312-317.45. CeyhanJA,JohnsonGH,LepeX.The effect of tray selection, viscosity of impression material, and sequence
of pour on the accuracy of dies made from dual-arch impressions. JProsthetDent2003;90:143-149.46. CeyhanJA,JohnsonGH,LepeX,PhillipsKM.A clinical study comparing the three-dimensional accuracy
of a working die generated from two dual-arch trays and a complete-arch custom tray. JProsthetDent2003;90:228-234.
47. WirzJ,JägerK,SchmidtliF.Abformungen in der zahnärztlichen Praxis. Stuttgart:GustavFischer,1993.
48. KraftA,WöstmannB,FergerP.Marginal fit of crowns resulting from different impression materials and techniques. JDentRes2001;80:245.
49. WöstmannB,HöingM,FergerP.Vergleich von hand- und maschinengemischten Abformmassen (Pentamix-System). DtschZahnärztlZ1998;53:753-756.
50. NicholsC,WoelfelJB.Improving reversible hydrocolloid impressions of subgingival areas. JProsthetDent1987;57:11-14.
51. DeMourguesF,LloryH.Déflection et régéneration gingivale après électrotpmie. RevmenssuisseOdonto-stomat1979;89:1271-127.
52. OmarR,AbdullahMA,SherfudhinH.Influence on dimensional accuracy of volume of wash material intro-duced into pre-spaced putty/wash impressions. EurJProsthodontRestorDent2003;11:149-155.
53. LehmannKM,HartmannF.Untersuchungen zur Genauigkeit von Doppelabformungen. Quintessenz33,985–987.
54. LehmannKM,ZackeW.Untersuchungen zur okklusalen Schichtdicke des Korrekturmaterials bei der Korrekturabformung. DtschZahnärztlZ1983;38:220-222.
55. LorenzoniM,PertlC,PenknerK,PolanskyR,SedajB,WegscheiderWA.Comparison of the transfer precision of three different impression materials in combination with transfer caps for the Frialit-2 system. JOralRehabil2000;27:629-638.
56. KohaviD.A combined impression technique for a partial implant-supported fixed-detachable restoration. QuintessenceInt1997;28:177-181.
57. GiordanoR.Issues in handling impression materials. GenDent2000;48:646-648.58. WöstmannB,HassfurthU,BalkenholM,FergerP.Influence of Impression Technique and Material on the
Transfer Accuracy of the Implant Position onto the Working Cast. JDentRes2003;82:3060.59. BorneffM,BehnekeN,HartmetzG,SiebertG.Praxisnahe Untersuchung zur Desinfektion von Abformmateri-
alien auf der Basis eines standardisierten Modellversuches. DtschZahnärztlZ1983;38:234-237.60. HutchingsML,VandewalleKS,SchwartzRS,CharltonDG.Immersion disinfection of irreversible hydrocolloid
impressions in pH-adjusted sodium hypochlorite. Part 2: Effect on gypsum casts. IntJProsthodont1996;9:223-229.
61. AbdelazizKM,CombeEC,HodgesJS.The effect of disinfectants on the properties of dental gypsum, part 2: surface properties. JProsthodont2002;11:234-240.
Literature | 51

62. JaggerDC,VowlesRW,McNallyL,DavisF,O‘SullivanDJ.The effect of a range of disinfectants on the dimen-sional accuracy and stability of some impression materials.EurJProsthodontRestorDent2007;15:23-28.
63. WirzJ.Klinische Material- und Werkstoffkunde. Berlin:Quintessenz,1993.64. BrownD.An Update on Elastomeric Impression Materials. BrDentJ1981;150:35-40.65. AramouniP,MillsteinP.A comparison of the accuracy of two removable die systems with intact working casts.
IntJProsthodont1993;6:533-539.66. LehmannKM,WengelerU.Untersuchungen zur Genauigkeit verschiedener zahntechnischer Modellsysteme.
DentLabor1985;33:613-617.67. ReiberT,DertingerK.Zur Präzision von Präparationsmodellen nach der Sägeschnittmethode.
ZahnärztlPrax1988;39:257-263.68. GramannJ.andHartungM.:AADR2006Orlando,AbstractNo1297;„Mixing quality of static and dynamic
mixers for impression materials“ http://iadr.confex.com/iadr/2006Orld/techprogram/abstract_74418.htm.69. P.Pospiech,M.Wildenhain.Zur Frage der Anmischung von Polyetherabformstoffen – Ein Vergleich zwischen
Hand- und dynamischer Mischung. DentalSpiegel5/98.
70. MüllerN,PröschelP.Kronenrand und parodontale Reaktion. DtschZahnärztlZ1994;49:30-36.71. PadburyJrA,EberR,WangH-L.Interactions between the gingiva and the margin of restorations.
JClinPeriodontol2003;30:379–385.72. WöstmannB,HaderleinD,BalkenholM,FergerP.Influence of Different Retraction Techniques
on the Sulcus Exudate Flow. JDentRes2004;83:A-4087.
52 | Literature
14. Glossary
Glossary | 53
A
Abutmentlevel 42
Addition-curedsilicones(vinylpolysiloxanes) 14,17,23,44
Additionsilicones 15
Alginate 19,46
Alginatereplacement 19
Aligners 38
Anaesthesia 12
A-silicones 12,15
Automaticmixingsystems 9,19,20,27
B
Blurring 37
C
Communication 9
Condensationpolyether 15,18
D
Dorsaldamming 23
Doublecordretractiontechnique 11
Drags 33
Dual-archimpression 26,39,40
Dynamicmixing 31
E
Elasticrecovery 14,16,18,19,22,47
Epoxyresins 46
Extrusionforces 29
F
Flowdefects 23,33,40
Foiltechnique 35
Functionalimpression 27,41
G
Garant™ 29
H
Haemostatic 11
Heavybody 21,33,34
Heavybody/wash(orheavybody/lightbody)technique 33
Hydrogenperoxide 12
Hydrophilicity 14,15,17
Hydrophobic 14,15
Hydrophobicity 14
Hydrosylationreaction 15
I
Implantlevel 42
Infectioncontrol 44
Insertion 33,36
Intrinsichydrophilicity 15
Irreversiblehydrocolloids 19
L
Latex 28
Lightbody 21,33
M
Macromonomer 16,17
Mediumbody 21
Metalsalts 11,20
Methacrylatecomposite 12,20
Monophasetechnique 34
O
Occlusalstops 23,36
Oralhygiene 10,11
P
Pentamix™AutomaticMixingUnit 27,30,31,32
Periodontium 10,42,46
Permanentdeformation 13
Platinumcatalyst 15
PolyetherRetarder 27,41
Polysulfides 18
Pulls 33
Putty 20,21,22,23,27,28,33,34
R
Retractionsolutions/liquid 11,36
Reversiblehydrocolloids 14,15,18
S
Sandwichtechnique 33
Sectionedmodel 46
Settingprocess 11,12,37
Singlecordretractiontechnique 11
Smearlayer 20
Snapset 16,17
Standardisedworkflow 9,27,34
Staticmixing 29,31
Sulcusbleeding 10,12
Surfactants 14,15
Syringing 17,29,36
T
Temporaryrestorations 19,20,49
Tensilestrength 16
Tissuedisplacement 11
Toothaxes 13,22
Trayadhesive 24,25,26
U
Undercuts 22,25,33,34
V
Vasoconstrictor 11,12
VPS 12,15,16,20
1-stepputty/washtechnique 33
2-stepputty/washtechnique 34
54 | Overview
Indications•Crownandbridgeimpressions
•Inlayandonlayimpressions
15. Overview 3M ESPE impression materials
•Functionalimpressions
•Implantimpressions
Impregum™Penta™Soft/QuickPolyetherImpressionMaterial
Excellentfitduetofirst-classprecision.
Benefits•Precise and void-free impressionsthroughoutstandinginitialhydrophilicityinmoistenvironments
•First-rate detail reproductionthankstoexcellentflowproperties
•Constant flow behaviour throughout working period and less distortionsbyunique“snap-set”behaviour
•Quick material cuts working and setting timesbyatleast33%
•Fresh minty flavour and easier removabilityof“Soft”materials

Overview | 55
Indications
•Crownandbridgeimpressions
•Inlayandonlayimpressions
Indications•Preliminaryimpressions
•Provisionalcrownandbridgeimpressions
•Opposingdentitionimpressions
•Impressionsforbleachingtraysandmouthguards
•Studymodelimpressions
•Impressionsfororthodonticmodels
Position™Penta™/QuickVPSAlginateReplacement
Lesspreptime.Moreworkingtime.Astress-freealginatereplacement.
Express™2VPSImpressionMaterial
Outstandingbalanceofclinicallyrelevantpropertiesforuncompromisingimpressionaccuracy.
Benefits• Precise impressions throughhigheraccuracy
•Fast working and setting times atroomtemperature
•Less distortions thankstoelasticrecovery
•Easy and thorough disinfection becausematerialcanbecompletelysubmersedindisinfectantsolution
•Long-term storage ability duetohighdimensionalstability
•Suitable for multiple pouring plusnoneedofimmediatecasting
Benefits•Extraordinarily well balanced propertiescomparedtootherleadingVPSproducts
•Great detail reproduction throughsuperiorhydrophilicityandflowbehaviour
•Distortion-free removal from the mouth duetoexcellenttoughness
•Reduced chance of costly remakes duetoalmost100%recoveryfromdeformation
•Faster setting of wash materials without reduced working time throughthermallyactiveputtytechnology
Your notes


3M ESPE AGESPE Platz82229 Seefeld · GermanyE-Mail: [email protected]: www.3mespe.com
EUR 49.00 Recommended price.
3M, ESPE, DuoSoft, Express, Garant, Impregum, Impresept, Imprint, Lava, Palgat, Penta, PentaMatic, Pentamix, Permadyne, Position and Ramitec are trademarks of 3M or 3M ESPE AG.
Acculoid, Affinis, Alginot, Aquasil, Boder-Lock, CEREC, Expasyl, Hongum, Identic, Invisalign, Optosil, P2, Peridenta, Permalastic, Plicafol, Speedex, Triple Tray and Xantopren are not trademarks of 3M or 3M ESPE AG.
© 3M 2008. All rights reserved.
70200956095/01 (5.2008)










![ON THE TORTOISE SHELL artistic dossier · «Praveen’s nritta carries an ‘excellent’ tag - excellent adavus, excellent geometry, excellent agility and excellent timing […]](https://img.pdfslide.us/doc/110x75/5e89c65012d1fb001e665ec4/on-the-tortoise-shell-artistic-dossier-praveenas-nritta-carries-an-aexcellenta.jpg)


















