Embed Size (px)
Citation preview

Importance of Myocardial Infarct Artery Patency on the Prevalence of Ventricular Arrhythmia and
Late Potentials After Thrombolysis in Acute Myocardial Infarction
Frank V. Aguirre, MD, Morton J. Kern, MD, Judith Hsia, MD, Harvey Serota, MD, Denise Janosik, MD, Terry Greenwalt, BA,
Allan M. Ross, MD, and Bernard R. Chaitman, MD
Sustained infarct artery patency is an important determinant of survival in patients with acute myocardial infarction. We studied 61 patients with acute myocardial infarction who received intravenous recombinant tissue-type plasmino- gen activator, aspirin or heparin within 6 hours of symptom onset, to determine if infarct artery patency after intravenous thrombolytic therapy influences myocardial electrical stability as mea- sured by the prevalence of spontaneous ventricu- lar ectopy or late potential activity. Infarct artery patency was determined by angiographic evalua- tion 2.5 f 3 days after infarctlon. Forty-eight patients (79%) had a patent infarct-related ar- tery and 13 (21%) patients had an occluded ves- sel. The mean number of ventricular premature complexes (VPCs)/hour (p <O.Ol) and the preva- lence of late potentials (54 vs 19%; p <0.03) were significantly higher in patients with an oc- cluded versus patent-infarct related vessel. Al- though VPC frequency and late potentials were not influenced by the time to thrombolytic treat- ment, patients with a patent infarct-related ar- tery had a lower prevalence of late potentials re- gardless of whether treatment was initiated 52 hours (25% patent vs 50% occluded; p = not sig- nificant) or 2 to 6 hours (16% patent vs 55% oc- cluded; p >0.03) after symptom onset.
Thus, successful thrombolysis decreases the frequency of ventricular ectopic activity and late potentials in the early postinfarction phase. The reduction in both markers of electrical instability
From the Cardiology Division, St. Louis University Medical Center, St. Louis, Missouri; and the Cardiology Division, George Washington Uni- versity, Washington, DC. Manuscript received May 20, 1991; revised manuscript received and accepted July 9, 199 1.
Address for reprints: Frank V. Aguirre, MD, Cardiac Catheteriza- tion Laboratory, St. Louis University Medical Center, 3635 Vista Ave- nue at Grand Boulevard, St. Louis, Missouri 63 110.
may help explain why the prognosis after suc- cessful thrombolysis is improved after acute myocardial infarction.
(Am J Cardiol 1991;6&1410-1416)
T he benefit of thrombolytic therapy on both short- and long-term survival after acute myo- cardial infarction is well established.‘a2 The
mechanisms responsible for enhanced survival in pa- tients treated with thrombolytic therapy remain contro- versial, but may be related to properties other than preservation of left ventricular function alone.3 Recent studies have determined that early recanalization and sustained patency of the infarct-related vessel may en- hance survival in patients after myocardial infarction by contributing to improved ventricular remodeling and healing, establishing collateral blood flow to noninfarct myocardial segments and reducing electrical instabili- ty.3 The latter mechanism is particularly important since sudden death secondary to malignant ventricular arrhythmia may account for up to 40% of total mortali- ty in the first year after the index infarction.4,5
In the present study, we tested the hypothesis that patients with acute myocardial infarction treated within 6 hours of symptom onset with thrombolytic therapy who attain infarct artery patency have a more stable myocardial electrical substrate and reduced prevalence of ventricular arrhythmia and late potential activity in the early postinfarct phase. In addition, the relation be- tween the time from symptom onset to initiation of thrombolytic therapy and infarct artery patency was examined to determine their impact on myocardial electrical stability.
METHODS Patients: Data were obtained through a retrospec-
tive review of 6 1 patients who presented with 130 min- utes of chest pain, ST-segment elevation Ll mm in L2 contiguous leads and who received treatment within 6
1410 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 68 DECEMBER 1, 1991
hours of symptom onset with 100 or 150 mg of intrave- nous recombinant tissue-type plasminogen activator. Patients enrolled in either the Heparin Aspirin Reper- fusion Trial6 or the Thrombolysis In Myocardial In- farction-2B trial from St. Louis and George Washing- ton Universities who underwent all of the following pro- cedures were considered eligible for study entry: (1) a predischarge 24-hour ambulatory and signal-averaged electrocardiogram, and (b) a predischarge diagnostic cardiac catheterization. Patients with an intraventricu- lar conduction delay (QRS duration 20.11 ms), com- plete bundle branch block or those taking antiarrhyth- mic drugs before hospital discharge were excluded.
Cardiac catheterization: Cardiac catheterization was performed 2.5 f 3 days (mean f standard devi- ation) after infarction. Significant coronary artery dis- ease was considered present if a narrowing of 260% of a major epicardial vessel was observed. Stenosis was determined by digital calipers in orthogonal views or by 2 independent experienced observers. Infarct artery pa- tency was defined by the coronary flow scoring system established in the Thrombolysis in Myocardial Infarc- tion trial.7 For the purposes of this study, flow grades of 0 to 1 were considered an “occluded” vessel and flow grades of 2 to 3 were considered a “patent” vessel.
Left ventricular ejection fraction was calculated from the 30’ right anterior oblique ventriculogram us- ing a standard area-length method. Regional wall mo- tion was subjectively classified as normal, hypokinetic, akinetic or dyskinetic.
Ambulatory electrocardiographic evaluation: Stan- dard 2-channel 24 hour clinical ambulatory electrocar- diograms were obtained at a mean of 8 f 4 days after infarction. The mean number of ventricular premature complexes (VPCs) per hour, ventricular couplets and episodes of ventricular tachycardia ( > 3 consecutive VPCs) were assessed.
Frequent ventricular ectopic activity was defined as a mean VPC count of 210 beats/hour. Complex ventricular ectopy was defined as the presence of ei- ther frequent ventricular ectopic activity or ventricular tachycardia, or both. All ambulatory electrocardio- graphic data were interpreted by physicians unaware of the angiographic findings.
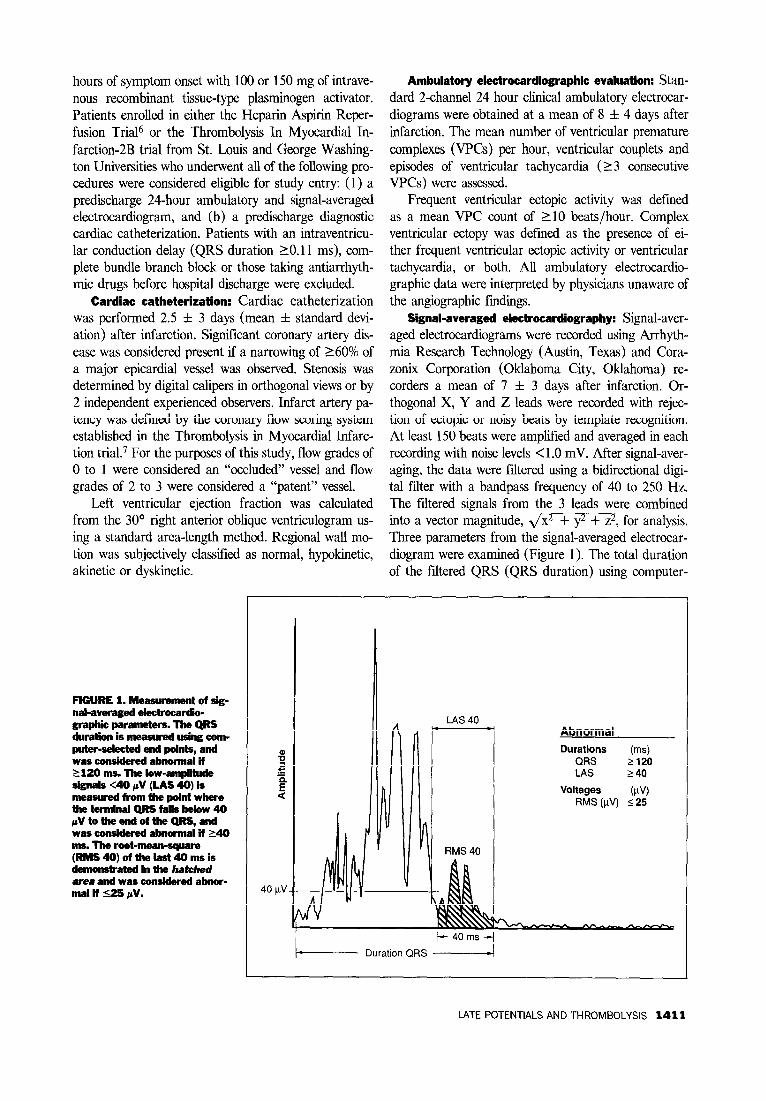
Signal-averaged electrocardiography: Signal-aver- aged electrocardiograms were recorded using Arrhyth- mia Research Technology (Austin, Texas) and Cora- zonix Corporation (Oklahoma City, Oklahoma) re- corders a mean of 7 f 3 days after infarction. Or- thogonal X, Y and Z leads were recorded with rejec- tion of ectopic or noisy beats by template recognition. At least 150 beats were amplified and averaged in each recording with noise levels <l.O mV. After signal-aver- aging, the data were filtered using a bidirectional digi- tal filter with a bandpass frequency of 40 to 250 Hz. The filtered signals from the 3 leads were combined into a vector magnitude, ,/x2 + y2 + z2, for analysis. Three parameters from the signal-averaged electrocar- diogram were examined (Figure 1). The total duration of the filtered QRS (QRS duration) using computer-
FIGURE 1. Measurement of sig- nal-averaged eiecmcardii- graphii parameters. The QRS duration is measured using com- puter-selacted end points, and was con&em! abmal if 2 120 ms. The low-ampiitde sifmals 40 UV (LAS 401 is &ad f&m ihe poiniwhere the terminal QRS falls below 40 jNtotheedoftheQRS,and wasconshkdabnomdif140 ms. The root-mean-square (RMS4O)ofthelast4Omsis demonstrated in the hatched area and was considered abnar- mal if 525 pv.
Abnormal Durations
z”ss 5” Voltages (FV)
RMS (pV) $25
I------ Duration QRS 4
LATE POTENTIALS AND THROMBOLYSIS 1411
TABLE I Patient Characteristics According to Status of TABLE II Cardiac Catheterization Findings in Patients with Infarct-Related Artery Patent and Occluded Infarct Arteries
Infarct-Related Artery Infarct-Related Artery
Variable
Age (years)
Men/women
White/black
Prior myocardial infarction (%I
Congestive heart failure (%)
Infarct site (%)
Anterior
Inferior
Lateral
Symptom onset-throm- bolytic therapy (hours)
Patent (n = 48)
55 f 12
38110
4414
2 (4)
10 (21)
27 (56)
20 (42) 1 (2) 3*1
Occluded (n = 13)
58 f 9
914
1112
1 (8)
4 (31)
3 (23)
10 (77) 0 (0) 3&l
p Value
0.47
0.70
0.82
0.84
0.70
0.08
0.93
Patent Occluded (n = 48) (n = 13) - ~
Variable n (%I n (%I p Value
Time after MI to catheter- 2.6 + 2.6 2.3 2 3.2 0.73 ization (days)
Coronary angiography No. of coronary arteries 0.48
z 60% in diameter None 4 (8) 0 (0) One 25 (52) 5 (42) Two 11 (22) 5 (42) Three 8 (17) 3 (16)
% Residual stenosis 68 f 21 99 ‘- 0.3 0.0001 (mean)
Infarct-related artery Right coronary artery 19 (37) 10 (77) Left anterior descending 27 (56) 3 (23) 0.054
artery Left circumflex artery 2 (4) 0 (0)
Left ventriculography LV ejection fraction (%I 51 2 13 46 -1- 18 0.32 Segmental wall motion
Normal 2 (4) 0 (0) 0.86 Hypokinetic 15 (32) 4 (31) Akinetic 25 (53) 8 (62) Aneurysm 5 (10) 1 (8)
LV = left ventricular; MI = myocardial infarction.
selected end points was considered abnormal when the duration was 1120 ms. The duration of low-amplitude signals was measured from the point where the termi- nal QRS decreased to <40 mV to the end of the QRS, and was considered abnormal when the duration was 140 ms. The root-mean-square was considered abnor- mal when the value was 525 mV. Late potential activi- ty was considered present when 22 of these parameters were abnormal.
Statistical methods: Statistical analysis was per- formed using the student’s t test for continuous vari- ables, chi-square with Yates correction for categorical data and Wilcoxon signed-rank test for analysis of non- parametric parameters, where appropriate. Logistic re- gression analysis was performed with positive late po- tentials as the dependent variable and 5 clinical and angiographic variables: ( 1) Left ventricular ejection fraction, (2) site of infarction, (3) degree of residual coronary artery stenosis, (4) segmental wall motion analysis, and (5) infarct artery patency, were used as the independent variables. Data were expressed as mean f 1 standard deviation. A p value < 0.05 was considered significant. The effect of the timing of thrombolytic therapy as it relates to the prevalence of VPCs and abnormalities on signal-averaged electrocar- diography was evaluated by stratifying the patient pop- ulation by early (12 hours) and late (2 to 6 hours) presentation.
RESULTS Study group: The final study group consisted of 61
patients (mean age 56 f 12 years [range 25 to 741) of whom 77% were men. Mean time from symptom onset to initiation of intravenous thrombolytic therapy was 3.0 f 1.8 hours (range 0.4 to 6.0). The site of infarc- tion was anterior in 30 patients (49%), inferior in 30 patients (49%) and lateral in 1 patient (2%). Three pa-
1412 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 68
tients (5%) had a history of a prior myocardial in- farction.
Patent versus occluded infarct-related artery: At angiography, 48 (79%) patients had a patent infarct- related artery and 13 (21%) patients had an occluded vessel. There was no difference in baseline characteris- tics between the 2 groups (Table I).
Cardiac catheterization variables (Table II): The 2 groups had similar cardiac catheterization characteris- tics. The occluded infarct vessel more often involved the right coronary artery (77%), whereas the left anterior descending artery was the culprit vessel in 56% of pa- tients with a patent infarct-related artery (p <0.05).
Ambulatory and signal-averaged electrocardio- graphic parameters (Table Ill): The mean number of VPCs per hour was significantly greater in patients with an occluded versus patent infarct-related artery. However, there was no difference in the prevalence of frequent or complex ventricular ectopic activity be- tween the 2 groups.
Patients with occluded arteries had significant- ly more abnormal signal-averaged electrocardiographic parameters compared with those with a patent vessel. Of the 13 patients with an occluded infarct artery, 7 (54%) had late potentials present compared with only 9 of 48 (19%) patients with a patent infarct artery (<0.03, Figure 2).
DECEMBER 1, 1991
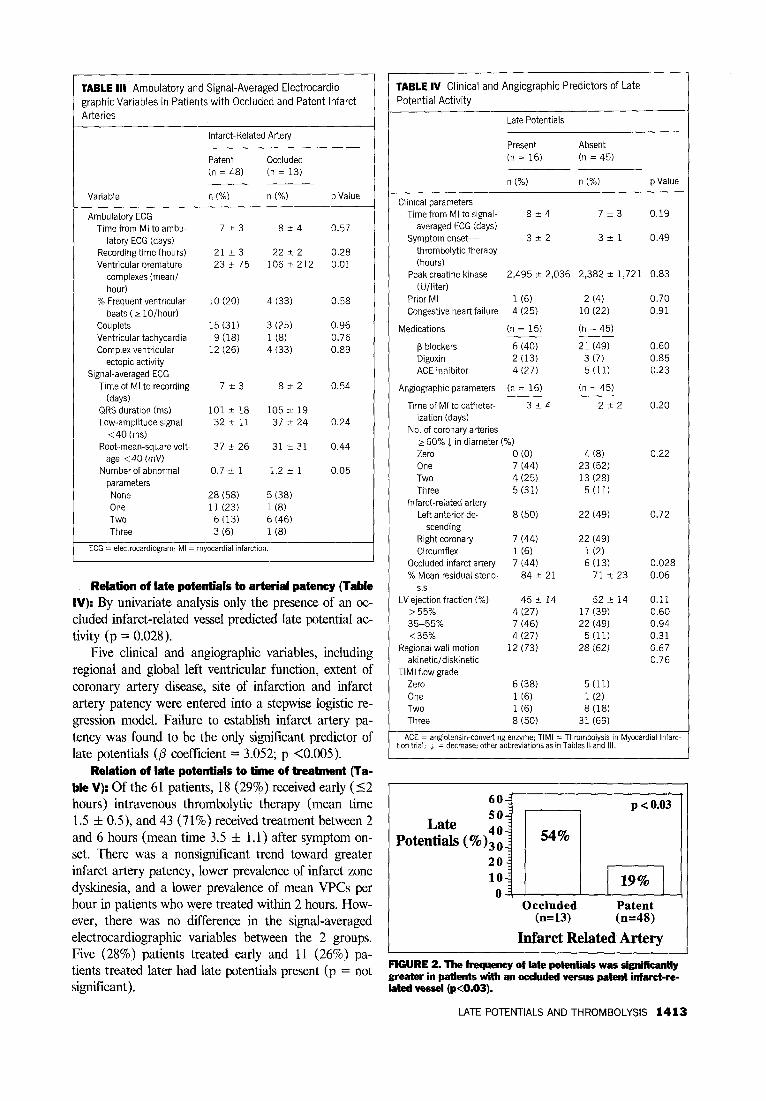
TABLE III Ambulatory and Signal-Averaged Electrocardio- graphicvariables in Patients with Occluded and Patent Infarct
Arteries
Infarct-Related Artery
Patent Occluded (n = 48) (n = 13) ___ -
Variable n (%) n (%) p Value
Ambulatory ECG Time from MI to ambu- 7,3 854 0.57
latory ECG (days) Recording time (hours) 21 * 3 22 2 2 0.28 Ventricular premature 23~75 106 + 212 0.01
complexes (mean/ hour)
% Frequent ventricular 10 (20) 4 (33) 0.58 beats (2 lo/hour)
Couplets 15 (31) 3 (25) 0.96 Ventricular tachycardia 9 (18) 1 (8) 0.76 Complex ventricular 12 (26) 4(33) 0.89
ectopic activity Signal-averaged ECG
Time of MI to recording 723 at2 0.54 (days)
QRS duration (ms) lOlk18 105 2 19 Low-amplitude signal 322 11 37 524 0.24
<40 (ms) Root-mean-square volt- 37k26 31231 0.44
age <40 (mV) Number of abnormal 0.7 ri: 1 1.2 2 1 0.05
parameters None 28(58) 5(38) One 11 (23) l(8) Two 6 (13) 6 (46) Three 3 (6) l(8)
ECG = electrocardiogram; MI = myocardial infarchon.
Relation of late potentials to arterial patency (Table IV): By univariate analysis only the presence of an oc- cluded infarct-related vessel predicted late potential ac- tivity (p = 0.028).
Five clinical and angiographic variables, including regional and global left ventricular function, extent of coronary artery disease, site of infarction and infarct artery patency were entered into a stepwise logistic re- gression model. Failure to establish infarct artery pa- tency was found to be the only significant predictor of late potentials (@ coefficient = 3.052; p <O.OOS).
Relation of late potentials to time of treatment (la- ble V): Of the 61 patients, 18 (29%) received early (52 hours) intravenous thrombolytic therapy (mean time 1.5 f 0.5), and 43 (71%) received treatment between 2 and 6 hours (mean time 3.5 f 1 .l) after symptom on- set. There was a nonsignificant trend toward greater infarct artery patency, lower prevalence of infarct zone dyskinesia, and a lower prevalence of mean WCs per hour in patients who were treated within 2 hours. How- ever, there was no difference in the signal-averaged electrocardiographic variables between the 2 groups. Five (28%) patients treated early and 11 (26%) pa- tients treated later had late potentials present (p = not significant).
1
TABLE IV Clinical and Angiographic Predictors of Late
Potential Activity
Late Potentials
Present Absent (n = 16) (n = 45)
n (%) I- (%) p Value
1
Clinical parameters Time from Ml to signal- 824 7+3 0.19
averaged ECG (days) Symptom onset- 322 321 0.49
thrombolytic therapy (hours)
Peak creatine kinase 2,495 2 2,036 2,382 +- 1,721 0.83 (U/liter)
Prior MI l(6) Congestive heart failure 4 (25)
Medications (n = 15)
p blockers 6 (40) Digoxin 2 (13) ACE inhibitor 4 (27)
Angiographrc parameters (n = 16)
Time of Ml to catheter- 3-t-4 ization (days)
No. of coronary arteries 260% 1 in diameter (%I Zero 0 (0) One 7 (44) Two 4(25) Three 5 (31)
Infarct-related artery Left anterior de- a (50)
scending Right coronary 7 (44) Circumflex 1 (6)
Occluded infarct artery 7 (44) % Mean residual steno- 84+ 21
sis LV ejection fraction (%I 45 t 14
>55% 4 (27) 35-55% 7 (46) <35% 4(27)
Regional wall motion 12 (73) akineticidiskinetic
TIMI flow grade Zero 6 (38) One 1 (6) Two 1 (6) Three 8 (50)
2 (4) 10 (22)
(n = 45)
21 (49) 3 (7) 5 (11)
(n = 45)
222
0.70 0.91
0.60 0.85 0.23
0.20
4 (8) 23 (52) 13 (28)
5 (11)
0.22
22 (49) 0.72
22 (49) l(2) 6 (13)
71+ 23 0.028 0.06
52 5 14 17 (39) 22 (49)
5 (11) 28(62)
0.11 0.60 0.94 0.31 0.67 0.76
5 (11) l(2) 8 (18)
31 (69)
ACE = angiotensin-converting enzyme: TIMI = Thromboiyse in Myocardlal Infarc- ion trial; j. = decrease; otherabbreviatlons as in Tables II and III.
60-
Late 50
Potentials (%)zi 54%
20 10
0 ~ Occluded
(n=13)
p <0.03 (
JGJJ Patent (n=48)
Infarct Related Artery I FIGURE 2. The frequency of late potentials was significantly greater in patients with an occluded versus patent infarct-re- lated vessel (p<O.O3).
LATE POTENTIALS AND THROMBOLYSIS 1413

TABLE V Comparison of Early (5 2 hours) Versus Late ( > 2
hours) Initiation of Thromboly?ic Therapy on Catheterization,
Ambulatory and Signal-Averaged Electrocardiographic
Parameters
Symptom Onset to Initiation of Therapy
5 2 Hours > 2 Hours (n = 18) (n = 43)
Variable n (%) n (%I p Value
Mean time to thrombolytic 2*1 4Ll - therapy (hours)
Cardiac catheterization Infarct artery patency 16 (89) 32 (74) 0.36 Left ventricular ejection 482 16 50 rt 14 0.20
fraction (%) 535% 2 (11) 7 (16) 0.94
Dyskinetic infarct zone 1 (6) 5 (12) 0.80 Ambulatory electrocardio-
graphy Ventricular premature 4k6 64 +- 153 0.06
complexes (mean/hour) % Frequent ventricular 22 26 0.86
beats (> lO/hour) Complexventricular beats 28 26 0.96
(%I Signal-averaged electro-
cardiography QRS duration (ms) 101 2 18 102 2 19 0.87 Low-amplitude signal 30 + 14 35 2 15 0.26
<40 ms Root-mean-square voltage 39 2 26 35 + 27 0.58
140 mV Late potential present 5 (28) 11 (26) 0.89
Occluded Patent Occluded Patent -- -- (n = 2) (n = 16) (n = 11) (n = 32)
Late potentials based (%I 1 (50) 4 (25) 6 (55) 5 (16)*
*p <0.03.
Patients with a patent infarct vessel had a lower prevalence of late potentials whether treated 12 or >2 hours after symptom onset (Table V). Of the 43 pa- tients treated 2 to 6 hours after symptom onset, 11 had an occluded infarct-related vessel, 6 (55%) of whom had late potentials present. In contrast, of the 32 pa- tients who had a patent infarct artery, only 5 (16%) had late potentials (p <0.03). A Similar but nonsignifi- cant trend was also noted in patients with a patent in- farct artery who were treated earlier (12 hours).
DISCUSSION Enhanced survival associated with intravenous
thrombolytic therapy for acute myocardial infarction has been demonstrated, and has mainly been attributed to preservation of left ventricular function.1>2 However, the mechanisms of improved survival appear to be mul- tifactorial, and may result from improved infarct artery patency and electrical stability.338,9 The results of this study support the concept that infarct artery patency after successful thrombolysis may enhance electrical stability as reflected by a reduction of both the preva- lence of VPCs and late potentials in patients with acute myocardial infarction.
Relation of ipfarct artery patency to myocardial electrical stabilitl: Frequent and complex ventricular ectopy have been recognized as significant and indepen- dent adverse prognostic factors in patients after myo- cardial infarction.4,5J0J l However, the influence of thrombolysis on ventricular ectopy after infarction re- mains poorly defined.
Theroux et all2 retrospectively analyzed the ambu- latory electrocardiographic data recordings in patients after infarction treated with either intravenous strep- tokinase or conventional therapy. Patients receiving thrombolytic therapy had a significantly lower preva- lence of ventricular ectopic activity than those treated conventionally. Similar findings were reported by Turi- to et a1,13 who also demonstrated a significantly lower prevalence of both VPCs (3.2 vs 6.4 VPCs/hour; p <0.05) and complex ventricular arrhythmia (p <O.Ol) in patients with a patent versus occluded infarct-related vessel. In the present study, infarct artery patency was also associated with a reduction in spontaneous ventric- ular ectopy, but only demonstrated a trend toward de- creased complex ventricular ectopy (Table III).
Late potential activity is also associated with an ad- verse prognosis when detected in the recovery phase of acute myocardial infarction.14-I6 Recent evidence sug- gests that thrombolytic therapy may enhance electrical stability and reduce the prevalence of late potentials in the postinfarct period. 17-19 In the study by Gang et al, l 7 signal-averaged electrocardiography performed within 48 hours of infarction revealed a significantly lower prevalence of late potentials in patients receiving recombinant tissue-type plasminogen activator than in those receiving conventional therapy (5 vs 23%; p <O.Ol ). Importantly, late potentials were present in only 14% compared with 33% of patients with a patent vs occluded infarct-related artery. Similar data have been reported by Vatterott et all8 and Zimmerman et a1.19
Although other investigators have not confirmed these lkdings,13,20 the use of different thrombolytic agents, differences in the timing of cardiac catheteriza- tion and the criteria used to define an abnormal signal- averaged electrocardiogram have been postulated as factors explaining these divergent results. Nonetheless, these data collectively indicate a lower prevalence of late potentials in patients following successful throm- bolysis.
Potential mechanisms relating infarct artery paten- cy to electrical stability in acute myocardial infarction: Recent experimental and clinical studies have shown that early reperfusion may improve infarct healing by altering myocardial cellular hemorrhage and edema formation, and by enhancing washout of toxic metabo- lites.21,22 In addition, successful thrombolysis has been associated with improved left ventricular remodeling23
1414 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 68 DECEMBER 1, 1991

and a decrease in left ventricular expansion and aneu- rysm formation. 24,25 These factors appear to lead to a more homogenous cellular infarct zone and may par- tially explain the resultant stability in the myocardial electrical substrate after successful thrombolytic reper- fusion.26
Ventricular ectopic activity, late potentials and time from symptom onset to treatment: The greatest mor- tality reduction after thrombolytic therapy is noted in those presenting within the first hour of symptom on- set.2 In the current study, early treatment did not result in a lower prevalence of ventricular ectopy or late po- tentials. However, infarct artery patency was an impor- tant determinant of late potential activity regardless of the timing of thrombolytic therapy (Table V). Al- though our data represent a small patient subset, the findings suggest an important role of infarct artery pa- tency in stabilizing the myocardial electrophysiologic substrate even when librinolytic therapy is not initiated early after symptom onset.
Study limitations: Coronary angiography (2.5 f 3 days) and ambulatory signal-averaged electrocardio- graphic (mean 8 f 4 days) evaluations were not ob- tained at similar times. Although coronary reocclusion may have occurred between the time of angiography and noninvasive testing, the impact in the present study is expected to be small, since reocclusion after success- ful thrombolysis usually occurs early (24 to 48 hours) after initiation of therapy. 27 The greater frequency of late potentials in patients with an occluded infarct ar- tery may be related to the site of infarction (e.g., inferi- or location) in this group. Previous studies indicate that the signal-averaged electrocardiogram is abnormal in a higher proportion of patients with inferior than ante- rior myocardial infarction. 14,15 This may be due to a later depolarization of the inferoposterior segment of the left ventricle. However, in this study, infarct loca- tion was not a predictor of late potentials by multivar- iant analysis.
Conclusion: Thus, improved survival after successful thrombolytic reperfusion may be attributable, at least in part, to a more favorable arrhvthmic risk nrofile in
Because of the relatively small study size the favor- able trends in VPC reduction noted between groups precludes definite conclusions regarding prognostic im- portance. Also, the criteria for defining abnormal sig- nal-averaged electrocardiographic parameters are not firmly established. 28 The criteria used in the current study are based on known prognostic findings in pa- tients with sustained ventricular tachycardia at our in- stitution.29
RN, whose work contributed significantly to the suc- cess of these trials, and Marilyn J. Utt for superb secre- tarial assistance.
REFERENCES 1. AIMS Trial Study Group. Effect of intravenous APSAC on mortality after acute myocardial infarction: preliminary report of the placebo-controlled clinical trial. Lancet 1988;1:545-549. 2. Gruppo Italian0 Per Lo Studio Della Streptochinasi Nell’infarcto Miocardio (GISSI). Effectiveness of intravenous thrombolytic treatment in acute myocardial infarction. Lancer 1986;1:397-401. 3. Braunwald E. Myocardial reperfusion, limitation of infarct size, reduction of left ventricular dysfunction, and improved survival: should the paradigm be ex- panded? Circulation 1989;79:441-444. 4. Rosenthal ME, Oseran DS, Gang E, Peter T. Sudden cardiac death following acute myocardial infarction. Am Heart J 1985;4:865-876. 5. Bigger JT, Fleiss JL, Kleiger R, Miller VP, Rolnitzky LM. The Multicenter Postlnfarction Research Group. The relationship among ventricular arrhythmias, left ventricular dysfunction, and mortality in the 2 years after myocardial infarc- tion. Circulation 1984;69:250-258. 6. Hsia J, Hamilton WP, Kleiman N, Chaitman BR, Roberts R, Ross AM. A comparison between heparin and low-dose aspirin as adjunctive therapy with tissue plasminogen activator for acute myocardial infarction. N Engl J Med 1990;323:1433-1437. 7. The TIM1 Study Group. The Thrombolysis in Myocardial Infarction (TIMI) trial: phase I findings. N Engl J Med 1985;312:932-936. 8. Kennedy JW, Ritchie JL, Davis KG, Stadius ML, Maynard C, Fritz JK. The Western Washington randomized trial of intracoronary streptokinase in acute myocardial infarction: a 12 month follow-up report. N Engl J Med 1985;312: 1073-1078. 9. Dalen JE, Gore JM, Braunwald E, Borer J, Goldberg RJ, Passamani ER, Forman S, Knatterud G. The TIMI Investigators: six- and twelve-month follow- up of the phase I thrombolysis in myocardial infarction (TIMI) trial. Am J Cardiol 1988;62:179-185. 10. The Multicenter Postinfarction Research Group. Risk stratification and survival after myocardial infarction. N Engl J Med 1983;309:331-336. 11. Bigger JT Jr, Weld FM, Rolnitsky LM. Prevalence, characteristics and significance of ventricular tachycardia (3 or more complexes) detected with am- bulatory electrocardiographic recording in the late hospital phase of acute myo- cardial infarction. Am J Cardiol 1981;48:815-823. 12. Theroux P, Morissette D, Juneau M, de Guise P, Pelletier G, Waters DD. Infhrence of fibrinolysis and percutaneous transluminal coronary angioplasty on the frequency of ventricular premature complex. Am J Cardiol1989;63:797-801. 13. Turitto GA, Risa AL, Zanchi E, Prati PL. The signal-averaged electrocardio- gram and ventricular arrhythmias after thrombolysis for acute myocardial infarc- tion. J Am Coil Cardiol 1990;15:1270-76. 14. Kuchar DL, Tborburn CW, Sammel NL. Late potentials detected after myocardial infarction: natural history and prognostic significance. Circulation 1986;74:1280-1289. 1% Games JA, Winters SL, Martinson M, Machac J, Stewart D, Targonski A. The prognostic significance of quantitative signal-averaged variables relative to clinical variables, site of myocardial infarction, ejection fraction and ventricular premature beats: a prospective study. J Am Co2l Cardiol 1989;13:377-384, 16. Simson MB. Use of signals in the terminal QRS complex to identify patients with ventricular tachycardia after myocardial infarction. Circulation 1981;64: 235-242. 17. Gang ES, Lew AS, Hong M, Wang FZ, Siebert CA, Peter T. Decreased
330-337.
incidence of ventricular late potentials after successful thrombolytic therapy for acute myocardial infarction. N Engl J Med 1989;321:712-716.
19. Zimmermann M, Adamec R, Ciaroni S, Malbois F, Tieche R. Reduction in
18. Vatterott PJ, Hammill SC, Bailey KR, Wiltgen CM, Gersh BJ. Late poten- tials on signal-averaged electrocardiograms and patency of the infarct-related
the frequency of ventricular late potentials after acute myocardial infarction by
artery in survivors of acute myocardial infarction. J Am Coil Cardiol 1991~17:
early thrombolytic therapy. Am J Cardiol 1991;67:697-703. & I I
the recovery phase of acute myocardial infarction. 20. Goedel-Meinen L, Hofmann M, Schmidt G, Jahns G, Klein G, Baedeker W, Bliimer H. The influence of fibrinolvtic theraov using streotokinase on the fre-
Acknowbdgment: We would like to thank Theresa quency and pattern of ventricular late potentials. ImHombach V, Hilger HH,
Thornton, RN, Martha Majors, RN, and Gail Cavallo, Kennedy HL, cds. Electrocardiography and Cardiac Drug Therapy. Dordrecht, the Netherlands: Kluwer, 1989;167-171.
LATE POTENTIALS AND THROMBOLYSIS 1415

21. Schaper J, Schaper W. Reperfusion of ischemic myocardium: ultrastructural and histochemical aspects. J Am CON Cardiol 1983;1:1037-1046. 22. Fishbein MC, Y-Rit J, Lando U, Kanmatsuse K, Mercier JC, Ganz W. The relationship of vascular injury and myocardial hemorrhage to necrosis after reper- fusion. Circulation 1980;62: 1274- 1279. 23. Bonaduce D, Petretta M, Villari B, Breglio R, Conforti G, Montemurro MV, Lanzillo T, Morgan0 G. Effects of late administration of tissue-type plasminogen activator on left ventricular remodeling and function after myocardial infarction. J Am CON Cardiol 1990;16:1561-1568. 24. Hochman SJ, Choo H. Limitation of myocardial infarct expansion by reper- fusion independent of myocardial salvage. Circulation 1987;75:299-306. 25. Jeremy RW, Hackworthy RA, Bautovich G, Hutton BF, Harris PH. Infarct artery perfusion and changes in left ventricular volume in the month after acute myocardial infarction. J Am Coil Cardiol 1987;9:989-995. 26. Gang ES, Bigger JT, Livelli FD Jr. A model of chronic ischemic arrhythmias: the relation between electrically inducible ventricular tachycardia, ventricular
fibrillation threshold and myocardial infarct size. Am J Cardiol198 1;50:469-477. 27. Ohman EM, Califf RM, Top01 EJ, Candela RJ, Abbottsmith CW, Ellis SG, Sigmon KN, Kereiakes DJ, George BS, Stack RS, and the TAMI Study Group. Consequences of reocclusion after successful reperfusion therapy in acute myocar- dial infarction. Circulation 1990;82:781-791. 28. Breithardt G, Cain ME, El-Sherif N, Flowers NC, Hombach V, Janse M, Simson MB, Steinbeck G. Standards for analysis of ventricular late potentials using high-resolution or signal-averaged electrocardiography: a statement by a task force committee of the European Society of Cardiology, the American Heart Association, and the American College of Cardiology. J Am Coil Cardiol 1991;17:999-1006. 29. Buckingham TA, Ghosh S, Homan SM, Theasen CC, Redd RM, Stevens LL, Chaitman BR, Kennedy HL. Independent value of signal-averaged electrccardi- ography and left ventricular function in identifying patients with sustained ven- tricular tachycardia with coronary artery disease. Am J Cardiol 198759: 568-572.
1416 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 68 DECEMBER 1, 1991





























