Embed Size (px)
Citation preview

Implications of English Proficiency on Immigrant Women’s Access to & Utilization of Health Services
Sepali Guruge1, Ryerson University Rachel Berman, Ryerson University Vappu Tyyskä, Ryerson University
Kenise Murphy Kilbride, Ryerson University Isaac Woungang, Ryerson University
Susanna Edwards, Ryerson University Laurie Clune, Ryerson University
KEYWORDS: IMMIGRANT WOMEN, LANGUAGE ACQUISITION,
SOCIAL DETERMINANTS OF HEALTH, HEALTH SERVICE UTILIZATION
Having the capacity to communicate in a common language is
centrally important when people access and utilize health, social, and settlement services. While a considerable portion of recent immigrant women to Canada speak English or French fluently, many others do not command either official language fluently enough to access and utilize available health care services. In this qualitative study, data were collected with service providers who work with newcomer women, with women who became fluent in English after arriving in Canada, and with women who do not currently speak English. We report on the challenges women face in acquiring proficiency in English and, through the use of a social determinants of health framework, on how limited language skills negatively influence the health of these immigrant women and their families. We also present a number of strategies that health professionals could use to better support women’s attempts to ensure their health and that of their families.
1 We thank the participants who found time in their busy lives to participate in this study. We are also grateful for the support we received from our community partner, COSTI Immigrant Services. The funding from Canadian Council on Learning; Ryerson University’s Research Assistant Program; and The Centre for Children, Youth and Families at Ryerson University, supported the project. Inquiries about this paper should be directed to Sepali Guruge, Daphne Cockwell School of Nursing, Ryerson University, 350 Victoria Street, Toronto, ON. M5B 2K3 (e-mail: [email protected])

Guruge et al.: ENGLISH PROFICIENCY & HEALTHCARE UTILIZATION 22
Over the last few decades, the movements of people from developing to developed countries have increased at an unprecedented rate. Since 1990, Canada has accepted approximately over 200,000 immigrants per year, just over half of whom are women (Citizenship and Immigration Canada [CIC], 2006). While a considerable number of recent immigrants speak English or French fluently, many others do not have fluency in either of these languages. Yet fluency in Canada’s primary languages shapes immigrants’ access to services. While interest is growing amongst researchers in how immigrants acquire English or French language fluency, further attention is required to how immigrant women, in particular, gain language fluency, the barriers to doing so, and the connection between these and their access to and use of health services in Canada. Based on the findings of our recent qualitative study conducted in Toronto, Ontario, in this paper we address the challenges immigrant women face in gaining English language proficiency in Canada; the impact of their proficiency, or lack thereof, on their health and access to and use of health services; and the strategies they use to overcome these challenges. These findings point to a number of policy changes, which we also discuss.
BACKGROUND Composition of Immigrant Women Coming to Canada
Much heterogeneity exists within the group of immigrant women coming to Canada based on country of origin, category of migration, length of stay in Canada, ethnocultural background, class, education, and knowledge of English or French. According to Citizenship and Immigration Canada (CIC), the composition of immigrants to Canada has shifted dramatically over the past 40 years from primarily European to ‘non-European’ countries of origin (CIC, 2004), and in the recent years, approximately 60% of recent immigrants come from Asia and the Middle East. Immigrants fall into several categories: economic/business class (56%); family class (29%); refugees (13%); and other, such as caregivers, retirees, (3%) (CIC, 2002). Recent immigrants are more likely to have a first language that is neither English nor French than those who immigrated to Canada 40 years ago, and women tend to be somewhat less likely than men to be able to carry on a conversation in English or French (CIC, 2004). Not only do some women not speak English upon arrival, but they are unable to speak English during subsequent enumerations. This can especially be the case for women who arrive as dependents, sponsored family members, or refugees. In 2004, for example, among those granted permanent residency in Canada, only 18% of principal applicants spoke neither English nor French, whereas 39% of family class immigrants, 50.5% of

Guruge et al.: ENGLISH PROFICIENCY & HEALTHCARE UTILIZATION 23
spouses and dependents, and 80.5% of refugees, most of whom were women, spoke neither English nor French (CIC, 2004). Language Instruction & Interpretation: The Canadian Context
CIC is responsible for the selection and settlement of immigrants; an aspect of the latter includes language instruction programs to newcomers. Related CIC programs have three main foci: language assessment, training, and delivery assistance (Ekos, 2004). Immigrants are assessed for their English proficiency through the Canadian Language Benchmarks framework, and are directed to an appropriate language training facility. The Canadian government spends approximately CDN$95 million a year on immigrant language training, and an estimated 50,000 individuals are enrolled in various language programs a year (CIC, 2006). Besides these government programs, approximately 600 private sector firms provide language industry services in Canada, with revenues in 2004 of over CDN$404 million (Statistics Canada, 2006). The language industry in Canada includes three sectors: instruction, translation, and interpretation. Of these, instruction brought in the highest revenues: CDN$193.2 million (48% of total) in 2004 (Statistics Canada, 2006). Interpretation services reported the lowest revenues: 2% of the total revenue (CDN $8.7 million) in 2004 (Statistics Canada). These figures indicate the general unavailability of interpretation services and highlight the expectation of and the need for newcomers to Canada to learn English or French quickly. Social Determinants of Health
Social determinants of health are the social and economic conditions that affect the health of individuals, their families, and communities (Raphael, 2004). Social determinants of health include (among others) income, social status, education, employment and working conditions, physical environment, gender, and health services (Health Canada, 2002). This perspective is also in line with the population health approach, which takes into account and acts upon the broad range of factors that influence health (World Health Organization [WHO], 1986). A key assumption in these approaches is that health promotion and disease prevention require healthy public policies both within and beyond the health sector (Kinnon, 1999). Along these lines, one of Health Canada’s policy interests includes a focus on the quality and accessibility of health care and services to immigrants by addressing the factors that affect access to and receipt of care – such as literacy and language (Kinnon, 1999).

Guruge et al.: ENGLISH PROFICIENCY & HEALTHCARE UTILIZATION 24
Gender, Language Proficiency & Health Outcomes
Immigration and settlement can affect the health of people. Both international (Donovan et al., 1992; Stephen et al., 1994;) and Canadian (Chen, Ng, & Wilkins, 1996a, 1996b; Raphael, 2004) studies have shown that immigrants are in better health upon arrival than the native born, but that immigrants’ health deteriorates within the first 10 years of moving to countries such as the United States, Australia, and Canada. Women, in particular, are often disadvantaged by the gendered norms in social institutions and by the policies and practices that reinforce such norms, a consequence of which is difficulty maintaining or achieving good health (Public Health Agency of Canada, 2001). Some women, based on underprivileged social statuses (including economic, cultural, racialized, and immigration statuses), face more severe consequences. The Canadian Community Health Survey indicated that, compared to Canadian-born women, immigrant women who had been in Canada for less than 2 years were less likely to report poor health, whereas immigrant women who had been in Canada for at least 10 years were more likely to report poor health (Vissandjee et al., 2003). The contributing factors to this deterioration of health status include social isolation, changes in family roles and norms, language barriers, lack of information about resources, and unemployment (Fowler, 1998). The available research also suggests that immigrant women have lower rates of access to and utilization of health services – services that may maintain and/or promote health, prevent disease, and restore health and function as well as provide treatment (Health Canada, 2002). One of the key reasons for these lower rates among immigrant women is their limited fluency in English or French. Moreover, because women are important contributors to the health and well-being of their families, women’s language proficiency also has an impact on their families’ health. In summary, the link between women’s English or French language proficiency and their access to and use of health services (for themselves and their families) requires serious consideration.
METHODS Based on data from CIC’s Landing of Immigrants Data System and subsequent census data, we identified the four largest language groups in which women were not proficient in English at least 5 years after their arrival: Mandarin, Cantonese, Urdu, and Punjabi-speaking women. Immigrant women in these language groups became the target population for the study. A community advisory committee (CAC) composed of members who are active and knowledgeable in the field of immigration and settlement was set up to provide advice to the team in the areas of

Guruge et al.: ENGLISH PROFICIENCY & HEALTHCARE UTILIZATION 25
participant recruitment, feedback on interview protocols, and review of the final study report. Data generation for this qualitative study included three phases. The first involved four focus group discussions with 28 key informants (community leaders/stakeholders), who work with women in language instruction contexts and/or other social and settlement sectors, to learn about successful language instruction programs and strategies. The participants included settlement workers, English as a second language (ESL) teachers, and community counselors. Focus groups were hosted by the project’s community partner, COSTI Immigrant Services, at one of their downtown Toronto locations in order to ensure easier access for participants. Each session was facilitated by two co-investigators along with a research assistant (RA). The second phase involved in-depth individual interviews with 24 women who had overcome obstacles to acquiring proficiency in English. They were interviewed by one of the two co-investigators who conducted the interviews to learn about the women’s experiences and sources of their success. The initial group of interviewees was identified by service providers in Phase 1, and later interviewees were identified by previous participants in Phase 2. The interviewers noted that “proficiency” was higher among those identified by the service providers. English language proficiency was a subjective measure in this study, and reflected the women’s ability to function in English-language employment settings and dealings with mainstream institutions. In the third phase, four focus groups (one for each language group) were conducted with 30 women who were not fluent in English in order to understand the challenges they face in becoming fluent. Interviewees from the first and second phases helped recruit potential study participants for the third phase. One woman from each language group facilitated the focus group discussions. The four women facilitators (one for each language group) attended a 2-hour training session on focus group facilitation and protocol. The RA was present at the four focus group sessions to offer support and technical assistance to each of the facilitators. The individual interviews and focus groups were conducted using a set of semi-structured, open-ended questions that were developed based on a literature review, the data generated in each of the completed phases, and feedback from the CAC. All interviews and focus groups discussions were audio-taped and transcribed. The first-language focus groups from the third phase of the study were translated into English by the facilitators who conducted the groups. Data were analyzed using inductive thematic analysis (Bryman, 2001) by reading and coding transcripts sentence by sentence, and by searching for recurring themes in the data. The subcategories already developed were compared and contrasted to determine commonalities

Guruge et al.: ENGLISH PROFICIENCY & HEALTHCARE UTILIZATION 26
and variations, and to develop categories. Although our study did not directly address access to health services, it became apparent from the data that this key issue for these women required further exploration and, as we will demonstrate, the need for a policy shift. The key categories that emerged included the following: (a) challenges women face in learning English; (b) women’s resiliency in overcoming these challenges; and (c) the negative influence of the lack of English proficiency on the women’s access to and use of health services, both directly and indirectly, through other social determinants of health.
FINDINGS
Demographic Information about Study Participants
Table 1 presents a comparison of the women with English language fluency (individual interviews) and those without (focus groups). The 24 women in the former group ranged in age from their 20s to their 50s, and had been in Canada 3-13 years. Their level of education varied from high school to university degrees, with more achieving the latter among the Punjabi- and Urdu-speaking women.
Table I. Comparison1 of Individual Interviewees2 vs Women in Focus
Groups3 Cantonese Mandarin Urdu Punjabi
Indiv. F.G. Indiv. F.G. Indiv. F.G. Indiv. F.G. Age mid
30s upper 40s
early 40s
about 40
early 40s
30s early 40s
about 40
Educ. level prior to arrival
H.S. Dip.
Less than H.S.
College /Univ. Degree
H.S. Dip.
College /Univ. Degree
H.S. Dip.
College /Univ. Degree
H.S. Dip. plus
Length of time in Canada
6.6
15.0
5.6
1.5
6.6
3.5
6.4
5.5
Children: Pre-schoolers Modal Number None
3 3 1
04 2 0
0 1 2
1 1 0
2
3, 4 0
5 4 0
2 2, 4 1
3 3, 4 0
1 Based on averages of demographic data for participants. 2 Six women in each language group were interviewed individually in English for about an hour. 3 Focus groups had 8 members, except for the Punjabi group, which had 6 members. Each group was conducted in the participants’ first language. 4 Ages of children in Cantonese Focus Group ranged from 13 to 36.

Guruge et al.: ENGLISH PROFICIENCY & HEALTHCARE UTILIZATION 27
Nearly all had at least one child. The 30 women who were not proficient in English ranged in age from their 20s to their 60s. They had been in Canada for 1-16 years, and all of them had children. Compared to their English-language proficient counterparts, more women in this group had no high school education. These women had arrived principally as dependents of economic migrants, as family-class sponsored immigrants, or as refugees. Challenges Women Face in Learning English
All interviewees in the three study phases spoke of immigrant women’s desire to become fluent in English. Participants’ accounts also indicated that immigrant women expected to gain two interrelated types of language skills: conversational and advanced English skills. All participants identified a strong need for women to acquire conversational skills to better manage their day-to-day lives in the new country, for example, to deal more efficiently with health issues or children’s school matters. Advanced-level English was seen as necessary for their success in obtaining a job at the level of their education and expertise. Related to the latter was an identified need for English instruction specific to a work category (e.g., teacher, engineer, etc.). Key challenges that women seemed to face in learning English were discussed in terms of finances, household work, family expectations, lack of information, and lack of childcare. Some of these challenges were captured in the following quotes: It is not that English is not important, but it cannot be their first priority. Refugees [often] have a financial responsibility. Even after 30 years, [some] cannot communicate in English. Because of the money they owed, they have to work to pay that back. (Key informant)
It’s really difficult for me to go for English classes. I have four children, parents-in-law, brother, and sister-in-law also to take care of. If I go to English classes my house is just a mess. Everyone looks at me in a mood. (Punjabi speaker)
When I came to Canada, I didn’t know that there is a facility to
learn English for free. By the time I came to know about LINC [Language Instruction for Newcomers to Canada], both my kids were toddlers; the LINC doesn’t provide childcare for young kids. When my kid started going to school, I went to LINC again…then they said that I have to pay, as LINC is for newcomers only! (Urdu speaker)
Another woman, a Punjabi speaker, spoke about the many hardships that she underwent since coming to Canada: a greatly lowered economic status, an absent husband who returned to the home country to tend their business, lack of childcare, a child bullied at school,

Guruge et al.: ENGLISH PROFICIENCY & HEALTHCARE UTILIZATION 28
experiences of racism, and coping with cultural taboos. Yet, after beginning language classes, which took her an hour and half to get to each way, she described how learning English has a myriad of benefits: “Learning English gives you self-respect, allows you to stand on your own, to visit MDs, provide response to teachers, and health care becomes more valuable.”
The previously noted challenges appear to be related to the women’s status in a gendered and racist society. However, other barriers women faced were related to the classes themselves: class location and scheduling, restrictive admission criteria to classes, types of instruction, and assessment and placement of students. Some of these barriers are reflected in the following:
I was assigned to Level 4. It was a teacher from Russia. I couldn’t understand what she said at all. I lost interest in learning. Later I was changed to Level 2; most of the participants there were retired seniors, most spoke Cantonese, and the teacher taught very, very slowly. I lost my interest again, then, I stopped and went to do labour work. (Mandarin speaker in focus group)
The community centre where I joined for classes had childcare but they are not offering it anymore. (Punjabi speaker) The learning is not from the beginning. When we came, we went to the class, others had already [done] quite a lot, we could only follow them, and we could hardly catch up with them (Mandarin speaker) Keep classes close to us. Keep kids in school. So we can leave them there and attend our classes. We don’t want our time wasted sitting. (Urdu speaker)
These comments point to a number of limitations in the way that
the language industry in Canada is set up and run. Overall, the challenges women faced in acquiring proficiency in English were complex but common across the three sets of data. However, family expectations appeared to be of greater concern for Urdu- and Punjabi-speaking women, while finances and “survival” appeared to be a greater challenge amongst Mandarin and Cantonese speakers. In addition, racism was identified as a barrier particularly by the key informants (Set 1) and by Urdu and Punjabi speakers (in Set 3).
Guruge et al.: ENGLISH PROFICIENCY & HEALTHCARE UTILIZATION 29
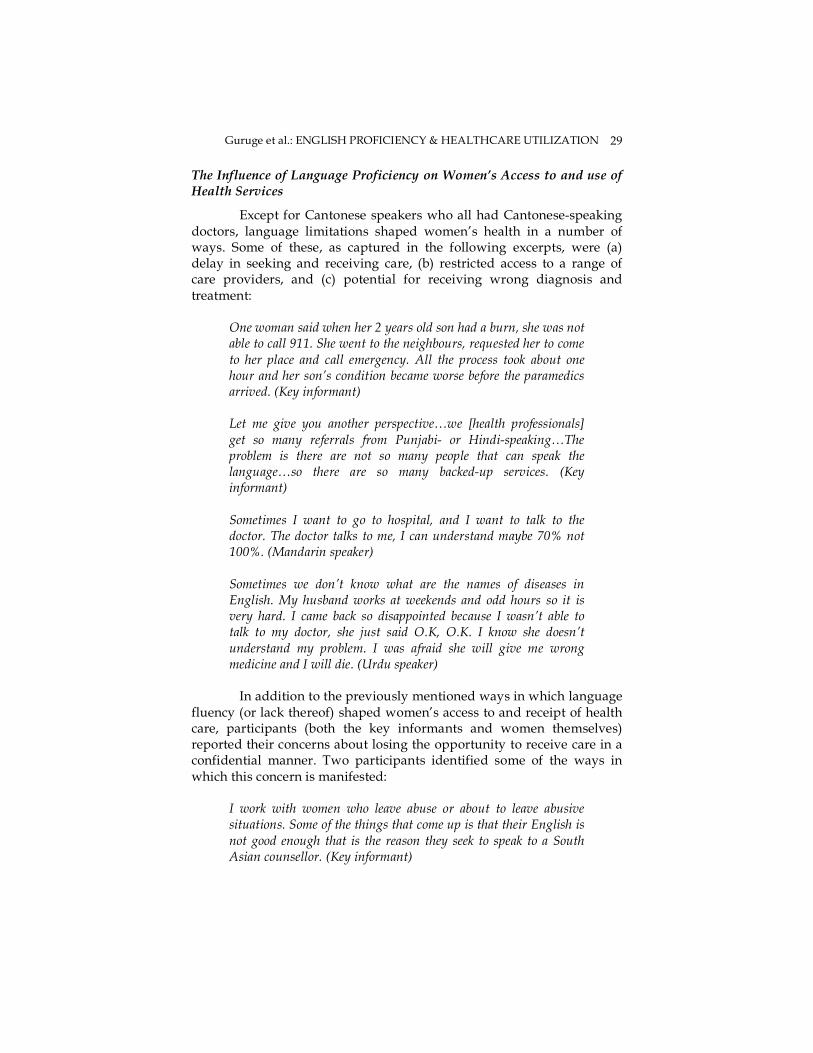
The Influence of Language Proficiency on Women’s Access to and use of Health Services
Except for Cantonese speakers who all had Cantonese-speaking doctors, language limitations shaped women’s health in a number of ways. Some of these, as captured in the following excerpts, were (a) delay in seeking and receiving care, (b) restricted access to a range of care providers, and (c) potential for receiving wrong diagnosis and treatment:
One woman said when her 2 years old son had a burn, she was not able to call 911. She went to the neighbours, requested her to come to her place and call emergency. All the process took about one hour and her son’s condition became worse before the paramedics arrived. (Key informant) Let me give you another perspective…we [health professionals] get so many referrals from Punjabi- or Hindi-speaking…The problem is there are not so many people that can speak the language…so there are so many backed-up services. (Key informant) Sometimes I want to go to hospital, and I want to talk to the doctor. The doctor talks to me, I can understand maybe 70% not 100%. (Mandarin speaker) Sometimes we don’t know what are the names of diseases in English. My husband works at weekends and odd hours so it is very hard. I came back so disappointed because I wasn’t able to talk to my doctor, she just said O.K, O.K. I know she doesn’t understand my problem. I was afraid she will give me wrong medicine and I will die. (Urdu speaker)
In addition to the previously mentioned ways in which language
fluency (or lack thereof) shaped women’s access to and receipt of health care, participants (both the key informants and women themselves) reported their concerns about losing the opportunity to receive care in a confidential manner. Two participants identified some of the ways in which this concern is manifested:
I work with women who leave abuse or about to leave abusive situations. Some of the things that come up is that their English is not good enough that is the reason they seek to speak to a South Asian counsellor. (Key informant)

Guruge et al.: ENGLISH PROFICIENCY & HEALTHCARE UTILIZATION 30
They would take a friend to interpret for them if they had to go to a hospital during emergency situations. Sometimes they asked their children to be their interpreters. (Mandarin speaker)
Even though Canada prides itself on having one of the best health
care systems in the world, not everyone in Canada benefits equally from it. From these excerpts, it is apparent that language barriers have a negative effect on immigrant women’s access to, use of, and receipt of quality care, thus preventing them from fully benefiting from the Canadian health care system. Language barriers were also perceived to restrict women’s ability to advocate for themselves and their family members when dealing with health care professionals, and to do so in a confidential manner. Some women spoke of relying on their children to act as translators with health care professionals, despite its inappropriateness in so many instances. For example, most Punjabi speakers and almost half of the Urdu speakers had daughters under 13 who engaged in translation/interpretation. This circumstance shaped what women could or were willing to discuss with their health care professionals in front of their children. This situation appears to leave women in abusive relationships particularly vulnerable. Influence of Language Proficiency on Women’s Health via Social Determinants of Health
Lack of fluency in English also affected women’s health indirectly via social determinants such as changes in social status inside and outside of the family, social isolation, employment and income, and stressful work conditions. The following quotes illustrate some of these factors:
[My daughter] says “communicate for you is so hard,” because sometimes she can’t use Chinese to express her thinking, so she can only use English and I can’t understand. At that time, I say, “I need your help, please repeat your question or the sentence slowly.” Maybe two times or three times, so, she say, “I’m so tired to talk to you.” (Mandarin speaker) I cannot read the information teachers sends home. I have to wait for my husband to explain it to me. Sometimes he is very tired or not in mood to read. I think our children will be left behind because they are not getting support and response from us. One day my son was telling about shoes that he needs outdoor and indoor shoes and I did not get the idea. I did not buy another pair of shoes for my son. After many days my son told me that his teacher does not allow him to play in the gym. I was surprised and

Guruge et al.: ENGLISH PROFICIENCY & HEALTHCARE UTILIZATION 31
then I requested my husband to go to school and find out. I really felt sorry for my son and insufficient for myself when his teacher explained the idea to us. (Punjabi speaker) I had a lot of [experience] travelling before coming to Canada. Between 1995 and 1998, I [was staying] still in Canada. I [felt] like death…black… I don’t know English. So everyday when my husband go to work or when my son goes to school, at home, I am always crying. You know why? I feel very lonely. Nobody I can talk to. (Mandarin speaker) The way of the thinking is different and sometimes they say little to the parents, because they think you know you can’t speak English like me. I have this friend whose daughter meets her in the elevator and she doesn’t say hello to her mom. It is important for the women, the family members, to grow together. (Mandarin speaker)
One of the main concerns emerging out of the three data sets
referred to social isolation and resulting loneliness. Another was related to the changes in social status both within one’s own family and in the community or in society at large. Participants spoke about the difficulties they faced in communicating with their own children and their teachers, helping children with their homework, or shopping, and how these left participants feeling incompetent, and/or over-reliant on their children and/or husbands. These situations were perceived as creating stress and/or leading to depression. Racism also was raised as a major challenge facing the participants (especially those who spoke limited or no English). Workplace racism, in particular, was perceived by a number of participants to negatively affect their success in obtaining jobs, a fair wage, a fair appreciation of their work, and better work conditions, as the following excerpts demonstrate:
English-speaking workers in their factories make more money. Even the cleaner who spoke English had a higher income. [Mandarin and Cantonese speakers] used gestures to communicate with their supervisor. He would use a sample of clothing to show them what needed to be done. They work harder than the English-speaking colleagues... but their boss would say they did not work hard enough. On the other hand, the English-speaking sewing machine operators were praised for their productiveness even though they made fewer items of clothing. (Key informant).
Guruge et al.: ENGLISH PROFICIENCY & HEALTHCARE UTILIZATION 32
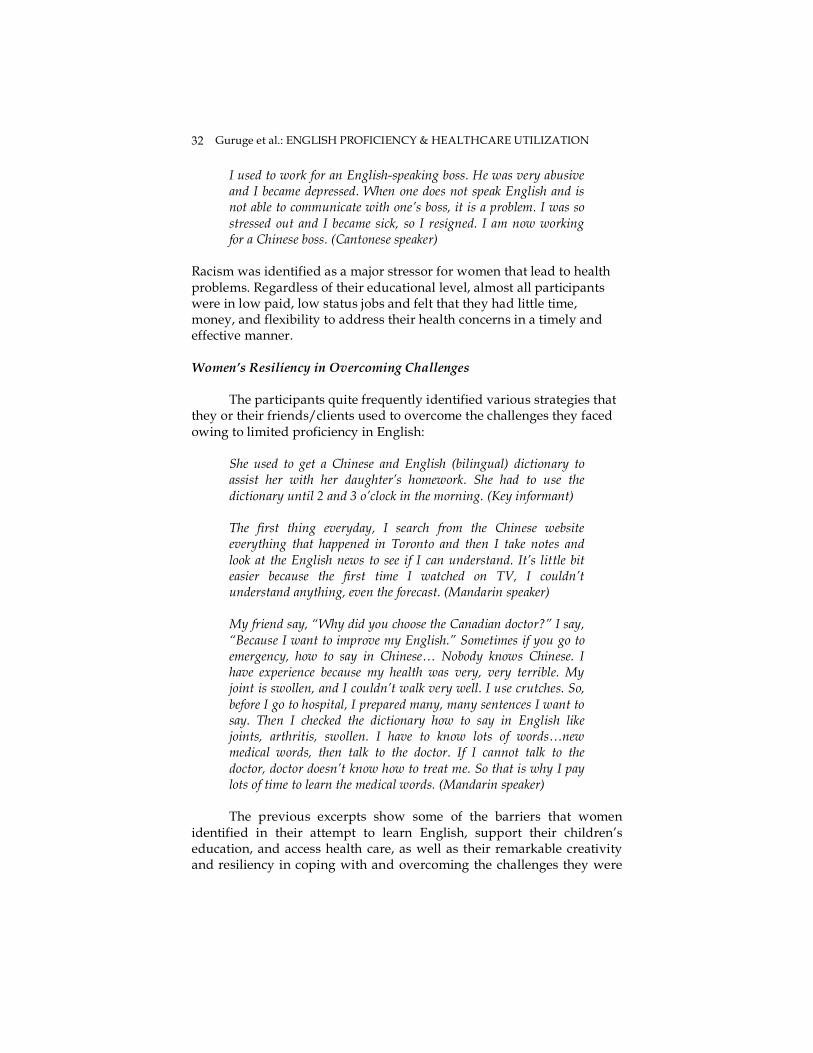
I used to work for an English-speaking boss. He was very abusive and I became depressed. When one does not speak English and is not able to communicate with one’s boss, it is a problem. I was so stressed out and I became sick, so I resigned. I am now working for a Chinese boss. (Cantonese speaker)
Racism was identified as a major stressor for women that lead to health problems. Regardless of their educational level, almost all participants were in low paid, low status jobs and felt that they had little time, money, and flexibility to address their health concerns in a timely and effective manner. Women’s Resiliency in Overcoming Challenges
The participants quite frequently identified various strategies that they or their friends/clients used to overcome the challenges they faced owing to limited proficiency in English:
She used to get a Chinese and English (bilingual) dictionary to assist her with her daughter’s homework. She had to use the dictionary until 2 and 3 o’clock in the morning. (Key informant) The first thing everyday, I search from the Chinese website everything that happened in Toronto and then I take notes and look at the English news to see if I can understand. It’s little bit easier because the first time I watched on TV, I couldn’t understand anything, even the forecast. (Mandarin speaker) My friend say, “Why did you choose the Canadian doctor?” I say, “Because I want to improve my English.” Sometimes if you go to emergency, how to say in Chinese… Nobody knows Chinese. I have experience because my health was very, very terrible. My joint is swollen, and I couldn’t walk very well. I use crutches. So, before I go to hospital, I prepared many, many sentences I want to say. Then I checked the dictionary how to say in English like joints, arthritis, swollen. I have to know lots of words…new medical words, then talk to the doctor. If I cannot talk to the doctor, doctor doesn’t know how to treat me. So that is why I pay lots of time to learn the medical words. (Mandarin speaker)
The previous excerpts show some of the barriers that women
identified in their attempt to learn English, support their children’s education, and access health care, as well as their remarkable creativity and resiliency in coping with and overcoming the challenges they were

Guruge et al.: ENGLISH PROFICIENCY & HEALTHCARE UTILIZATION 33
presented with in obtaining appropriate care. These individual solutions to systemic problems appear, however, to take their toll on the health of these women. Of particular note are psychological health problems that arise from isolation and stress.
DISCUSSION
In this study, the most commonly identified challenges to learning English were related to systemic issues, such as financial constraints, lack of information and lack of childcare, and to those pertaining to English instruction classes themselves, including assessment and placement of students, restrictive admission criteria, and lack of childcare available and/or associated with classes (or class location). Similar findings have been reported in the limited available literature that focuses specifically on immigrant women’s acquisition of English or on the obstacles in their way. Developing proficiency in English is a challenging endeavour (Duff, Wong, & Early, 2002; Springer & Kilbride, 2003), given the many barriers immigrant women face, including the high cost of housing in major cities; government’s deskilling of immigrant men, which results in women’s engaging in paid employment rather than pursuing language training; and difficulty finding affordable childcare (Alboim, Finnie, & Meng, 2005; Aydemir & Skuterud, 2005; Chiswick & Miller, 2005; Ho, 2006; Kahn & Watson, 2005; Man, 2004; Mojab, 1999;Warman & Worswick, 2004). The women’s accounts in our study demonstrate their resourcefulness and resiliency in dealing with and overcoming the challenges of learning a new language or navigating health, educational, and employment systems. At the same time, however, individual solutions can have negative consequences for both the women and their families (Yakushko & Chronister, 2005). For example, the current study findings indicate that women stayed up late, were stressed about learning medical terminology, and changed jobs to cope with workplace discrimination/racism, which were identified as leading to physical and mental health problems. Increasing evidence has linked racism to poorer mental and physical health (e.g., Karlsen & Nazroo, 2002; Krieger, 2003; Krieger & Williams, 2001; Moody-Ayers et al., 2005; Mustillo et al., 2004; Noh & Kasper, 2003; Williams, Neighbours & Jackson, 2003)
Our study findings show that limited language fluency, in general, negatively influenced women’s access to, use of, and receipt of quality care. In particular, the findings indicate that women experienced delay in receiving care, feared receiving the wrong diagnosis and treatment, and experienced difficulty advocating for themselves and their family members in a confidential manner. Other researchers in a wide range of health-related studies also have noted that limited or lack

Guruge et al.: ENGLISH PROFICIENCY & HEALTHCARE UTILIZATION 34
of language fluency negatively affects immigrants’ access to health services. For example, limited proficiency was noted as presenting difficulty in receiving emergency care (Manson, 1998; Wen, Goel, & Williams, 1996) and preventative care (Grunfeld, 1997; Jacobs et al., 2005; Sent et al., 1998; Wen et al., 1996; Woloshin et al., 1997). Additional studies have also reported that language fluency has an impact on access and use of health care services for specific illnesses such as hypertension (Perez-Stable, Napoles-Springer, & Miramontes, 1997), diabetes (Tocher & Larsen, 1998), breast cancer (Stein & Fox, 1990), asthma (Patcher & Weller, 1993), and mental illness (Chen & Kazanjian, 2005; Globerman, 1998).
Empirical Canadian research is limited on the ways in which language proficiency negatively influences the access to health care services (Abraham & Rahman, 2008). In a review on the topic of language barriers in access to health care, Bowen (2001) indicated that language may be a more significant barrier than cultural beliefs and practices) to immigrants’ initial contact with health services, delay in seeking care, limited understanding of diagnoses, and follow-through with a ‘prescribed’ treatment plan. In a quantitative study on the prevalence of depressive symptoms among elderly Chinese immigrants in Canada, Lai (2004) also cited language barriers to their access to services. As indicated in the current study’s findings as well as those of the previous studies (such as Guruge, 2007; McDonald, 1999; Springer & Kilbride, 2003; Tyyskä, 2007), one of the most important areas in which the lack of language fluency affects immigrant women’s ability to seek services is violence against women, consequences of which are downplayed by the male-biased and male-dominant health care system. This situation is an indication of how racism and patriarchy in society are closely linked. In addition to the previously noted more apparent links between limited language skills and women’s health, the findings of our study also highlight the connection between language skills and women’s health via social determinants of health. More specifically, the findings demonstrate the ways in which limited language skills affected, among others, women’s access to social networks and support, quality of work conditions, employment and income, and social status, which are all social determinants of health. For example, Boyd (1990, 1999) noted language to be among the key labor market integration barriers for immigrant women in terms of their ability to obtain employment and achieve levels of learning according to their levels of education and prior work experience. Tastsoglou and Miedema (2005) also suggested that “language, and especially accent problems, continue to [have an impact on] most immigrant women after many years of residence, and affect in multiple, sometimes subtle and indirect ways, the quality of their

Guruge et al.: ENGLISH PROFICIENCY & HEALTHCARE UTILIZATION 35
working lives in Canada” (p, 213). How these social determinants of health affect immigrant women and men differently requires further exploration. IMPLICATIONS & NEW CONTRIBUTIONS TO THE LITERATURE
The findings of our study2 point to the need for systemic solutions to increase women’s access to and use of English language instruction classes. Some of the strategies that might address this concern include: 1) providing information in first languages about such classes at ports of entry to Canada; 2) improving outreach using local and community newspapers, word-of-mouth, in-person recruiting, public websites, flyers at libraries and community centers, community TV programs, cultural events, places of worship, parent-teacher meetings, and grocery stores; 3) increasing availability of English language classes; 4) removing admission criteria to classes (such as being a newcomer); 5) increasing availability of free daycare for women accessing language instruction classes; 6) holding classes at locations closer to schools or in schools, closer to daycare facilities, apartments, and community libraries, or on television; 7) providing financial incentives so that women do not have to choose between earning an income and attending language instruction classes (which in the long run is beneficial to all); 8) setting up flexible class hours based on catchment area; 9) offering both conversational and vocational language training; 10) linking language training to employment opportunities; and 11) systematically addressing workplace racism. As we have noted earlier, the language industry’s investment in interpretation and translation is limited. Given the importance of maintaining the good health of immigrants, it is crucial that much more emphasis be placed on hiring, training, and using professional interpreters across the board in the health care sector. It is equally important to ensure that health information is available orally and in written form in the clients’ first language. In addition, in order to improve care and services to women at the present time, we propose the following recommendations to health care professionals who work with immigrant women who might not be fluent in English: 1) assess women’s current English literacy level (given loss of language skills
2 Most of these findings have been stored as a database framework in a new automated developed system hosted at http://www.immigrantwomen.ca/. This Web portal, through its search functions and comments options, provides various types of information on the challenges addressed in this research. It potentially can be used as a supporting platform for other research on language acquisitions, either generated from our on-going analysis or initiated elsewhere, hence, contributing to improving the outreach.

Guruge et al.: ENGLISH PROFICIENCY & HEALTHCARE UTILIZATION 36
when not regularly in use) and provide appropriate delivery of information; 2) offer programs/services during evenings, nights, and weekends so that women will not have to take time off from work or classes to attend; 3) address the family financial situation when deciding on care and treatment options, and link women to resources; and 4) understand the influence of social determinants of health on immigrant women’s health, and work in collaboration with multiple stakeholders in health, social, and settlement sectors to incorporate such an understanding into practice. Lastly, we propose that addressing barriers to language learning must incorporate a coordinated approach by municipal, provincial, and federal governments. Study Strengths
This study incorporated the voices of women currently experiencing barriers to acquiring proficiency in English, as well as those of women who had overcome such challenges. By speaking with women about their individual situations, we were able to gain a micro-level perspective and to give voice to their concerns. This approach to our study also provided a window into the resourcefulness and resiliency of these newcomer women. Talking with community leaders and service providers who work with large numbers of immigrant women and come up against restrictive policies and bureaucracies in the context of language learning and settlement helped in understanding relevant macro-level issues. To our knowledge, no other Canadian study has explored the topic of challenges to acquiring English by using this approach. Study Limitations
Recruitment of all three sets of study participants involved convenience and snowball sampling strategies, which might have restricted our sample representation.
CONCLUSIONS The ability to communicate fluently in English affected women’s health both directly and indirectly via social determinants of health (such as social isolation, income, social status, employment and work conditions, and racism). The challenges to becoming proficient in English were largely related to systemic barriers that the women faced in the post-migration and settlement context. These barriers must be addressed in order to improve immigrant women’s and their families’ health.

Guruge et al.: ENGLISH PROFICIENCY & HEALTHCARE UTILIZATION 37
REFERENCES
Abraham, D. & Rahman, S. (2008). The community interpreter: A critical link between clients and service providers. In S. Guruge & E. Collins (Eds.), Working with immigrant women: Issues and strategies for mental health professionals (pp.103-117). Toronto: Centre for Addiction and Mental Health.
Alboim, N., Finnie, R. & Meng, R. (2005). The discounting of immigrants’ skills in Canada: Evidence and policy recommendations. Choices, 11(2), 25.
Aydemir, A. & Skuterud, M. (2005). Explaining the deteriorating entry earnings among Canada’s immigrant cohorts, 1966-2000. Canadian Journal of Economics, 38, 641-671.
Bowen, S. (2001). Language Barriers in Access to Health Care. Ottawa: Health Canada. Retrieved from: http://www.hc-sc.gc.ca/hcs-sss/pubs/index_e.html (last visited Jan. 25, 2008)
Boyd, M. (1999). Integrating gender, language and visible minority groups. In S. Halli & L. Driedger (Eds). Immigrant Canada: Demographic, Economic & Social Challenges. (pp. 282-306). Toronto: University of Toronto Press.
Boyd, M. (1990). Immigrant women: Language, socioeconomic inequalities and policy issues. In S. Halli, F. Trovato & L. Driedger (Eds), Ethnic Demography: Canadian Immigrant, Racial & Cultural Variations (pp. 275-296). Ottawa: Carleton University Press.
Bryman, A. (2001). Social Research Methods. New York: Oxford University Press.
Chen, A. W. & Kazanjian, A. (2005). Rate of mental health service utilization by Chinese immigrants in British Columbia. Canadian Journal of Public Health, 96(1), 49-51.
Chen, J., Ng. E. & Wilkins, R. (1996a). The health of Canada’s immigrants in 1994-1995. Health Reports, 7(4), 33-45.
Chen, J., Ng. E. & Wilkins, R. (1996b). Health expectancy by immigrant status. Health Reports, 8(3), 29-37.
Chiswick, B. & Miller, P. (2005). Linguistic distance: A qualitative measure of the distance between English and other languages. Journal of Multilingual and Multicultural Development, 26(1), 1-11.
Citizenship and Immigration Canada (2006). Retrieved from: http://www.integration-net.cic.gc.ca/inet/English/n-info-n/index.htm#i1 (last visited July 31, 2006)
Citizenship & Immigration Canada. (2002). Facts & Figures 2002: Immigration Overview. Ottawa: Minister of Public Works & Government Services Canada.

Guruge et al.: ENGLISH PROFICIENCY & HEALTHCARE UTILIZATION 38
Citizenship & Immigration Canada. (2004). Facts & Figures 2004: Immigration Overview # 28. Ottawa: Minister of Public Works & Government Services Canada.
Donovan, J., d'Espaignet, E., Metron, C., & Van Ommeren, M. (Eds.). (1992). Immigrants in Australia: A Health Profile (Ethnic Health Series No. 1). Canberra: Australian Institute of Health and Welfare.
Duff, P., Wong, P. & Early, M. (2002). Learning language for work and life: The linguistic socialization of immigrant Canadians seeking careers in healthcare. Modern Language Journal, 86, 397-422.
Ekos Research. (2004). Evaluation of the Language Instruction for Newcomers to Canada (LINC) Program. Ottawa: Citizenship and Immigration Canada.
Fowler, N. (1998). Providing primary health care to immigrants & refugees: The North Hamilton experience. Canadian Medical Association Journal, 159, 388-91.
Globerman, S. (1998). Immigration and health care utilization patterns in Canada: Final report. Research on Immigration & Integration in the Metropolis (Working Group Paper Series No.8, pp. 98-108). Vancouver: Vancouver Centre for Excellence.
Grunfeld, E. (1997). Cervical cancer: Screening hard to reach groups. Canadian Medical Association Journal, 157, 543-545.
Guruge S. (2007). The Influence of Gender, Racial, Social, and Economic Inequalities on the Production of & Responses to Intimate Partner Violence in the Post-migration Context. Unpublished doctoral dissertation, University of Toronto, Toronto.
Health Canada. (2002). Population Health. Retrieved from: http://www.phac-aspc.gc.ca/ph-sp/phdd/
Ho, C. (2006). Migration as feminisation? Chinese women’s experiences of work and family in Australia. Journal of Ethnic & Migration Studies, 32, 497-514.
Jacobs, E. A., Karavolos, K., Rathouz, P. J., Ferris, T. G. & Powell, L. H. (2005). Limited English proficiency and breast and cervical cancer screening in a multiethnic population. American Journal of Public Health, 95, 1410-1416.
Kahn, S. & Watson, J. (2005). The Canadian immigration experiences of Pakistani women: Dreams confront reality. Counselling Psychology Quarterly, 18, 307-317.
Karlsen, S. & Nazroo, J. (2002). Relation between racial discrimination, social class, and health among ethnic minority groups. American Journal of Public Health, 92, 624–631.
Kinnon, D. (1999). Canadian Research on Immigration & Health: An Overview. Retrieved from: http://www.hc-sc.gc.ca/iacb-dgiac/nhrdp/metropolis/
Guruge et al.: ENGLISH PROFICIENCY & HEALTHCARE UTILIZATION 39
Krieger, N. (2003). Does racism harm health? Did child abuse exist before 1962? On explicit questions, critical science, and current controversies: An ecosocial perspective. American Journal of Public Health, 93(2): 194-199.
Krieger, N. & Williams, D. R. (2001). Changing to the 2000 Standard Million: Are declining racial/ethnic and socioeconomic inequalities in health real progress or statistical illusion? American Journal of Public Health, 91, 1209-1213.
Lai, D. (2004). Health status of older Chinese in Canada: Findings from the SF-36 Health Survey. Canadian Journal of Public Health, 95, 193-200.
Man, G. (2004). Gender, work and migration: Deskilling Chinese immigrant women in Canada. Women’s Studies International Forum, 2, 135-148.
Manson, A. (1998). Language concordance as a determinant of patient compliance and emergency room use in patients with asthma. Medical Care, 26, 1119-1128.
McDonald, S. (1999). Not in the numbers: Domestic violence and immigrant women. Canadian Women’s Studies, 19,163-167.
Mojab, S. (1999). De-skilling immigrant women. Canadian Women’s Studies, 19, 110-113.
Moody-Ayers, S.Y., Stewart, A. L., Covinsky, K. E. & Inouye, S. K. (2005). Prevalence and correlates of perceived societal racism in older African-American adults with type 2 diabetes mellitus. Journal of the American Geriatrics Society, 53(12), 2202-8.
Mustillo, S., Krieger, N., Gunderson, E. P., Sidney, S., McCreath, H. & Kiefe, C. I. (2004). Self-reported experiences of racial discrimination and black-white differences in preterm and low-birthweight deliveries: The CARDIA Study. American Journal of Public Health, 94, 2125-2131.
Noh, S. & Kaspar, V. (2003). Perceived discrimination and depression: Moderating effects of coping, acculturation, and ethnic support. American Journal of Public Health, 93(2): 232-238.
Patcher, L. M., & Weller, S. C. (1993). Acculturation and compliance with medical therapy. Journal of Developmental and Behavioural Pediatrics, 14, 163-167.
Perez-Stable, E. J., Napoles-Springer, A. N. & Miramontes, J. M. (1997). The effects of ethnicity and language on medical outcomes of patients with hypertension or diabetes. Medical Care, 35, 1212-1219.
Public Health Agency of Canada. (2001). Towards a common understanding: Clarifying the core concepts of population health. Retrieved from: http://www.phac-aspc.gc.ca/ph-sp/docs/common-commune/appendix_d-end.php

Guruge et al.: ENGLISH PROFICIENCY & HEALTHCARE UTILIZATION 40
Raphael, D. (2004). Social Determinants of Health: Canadian Perspectives. Toronto: Canadian Scholars’ Press.
Sent, L., Ballem, P., Paluck, E., Yalland, L. & Vogel, A. M. (1998). The Asian women’s health clinic: Addressing cultural barriers to preventive care. Canadian Medical Association Journal, 159, 350-354.
Springer, J. & Kilbride, K. (2003). Forging Links, Building Social Capital: Responding to Migration as a Factor in Emergency Shelter Use (Report to the City of Toronto). Toronto: City of Toronto.
Statistics Canada. (2006). Survey of language industry companies in Canada: Translation, interpretation & language training. Ottawa: Industry Canada. Retrieved from: http://www.ic.gc.ca/eic/site/lain-inla.nsf/eng/h_qs00040.html
Stein, J. A. & Fox, S. A. (1990). Language preference as an indicator of mammography use among Hispanic women. Journal of the National Cancer Institute, 82, 1715-1716.
Stephen, E. H., Foote, K., Hendershot, G. E. & Schoenborn, C. A. (1994). Health of the foreign-born population. Advance Data from Vital and Health Statistics, 241, 1-10.
Tastsoglou, E. & Miedema, B. (2005). Working much harder and always having to prove yourself: Immigrant women’s labour force experiences in the Canadian Maritimes. In M.T. Segal & V. Demos (Eds). Special edition on Gender Realities: Local and Global, Advances in Gender Research, 9, 201-233.
Tocher, T. M., & Larsen, E. (1998). Quality of diabetes care for non-English speaking patients: A comparative study. Western Journal of Medicine, 168, 504-511.
Tyyskä, V. 2007. Immigrant families in sociology. In J. Lansford, K. Dieter-Deckard & M. C. Bornstein (Eds.). Immigrant Families in Contemporary Society (pp. 83-99). New York: Guilford Press.
Vissandjee, B., Desmeules, M., Cao, Z., Abdool, S. & Kazanjian, A. (2003). Integrating ethnicity & migration as determinants of Canadian women’s health. In M. Desmeules, D. Stewart, A. Kazanjian, H. Maclean, J. Payne & B. Vissandjée (Eds.). Women's Health Surveillance Report: A Multidimensional Look at the Health of Canadian Women. Ottawa: Canadian Institute for Health Information.
Warman, C. & Worswick, C. (2004). Immigrant earnings performance in Canadian cities: 1981 through 2001. Canadian Journal of Urban Research, 13(1), 62-84.
Wen, S. W., Goel., V. & Williams, J. I. (1996). Utilization of health care services by immigrants and other ethnic/cultural groups in Ontario. Ethnicity & Health, 1(1), 99-109.
Williams, R., Neighbours, H. & Jackson, J. (2003). Racial/Ethnic discrimination and health: Findings from community studies. American Journal of Public Health, 93 (2), 37-48.
Guruge et al.: ENGLISH PROFICIENCY & HEALTHCARE UTILIZATION 41
World Health Organization, Health and Welfare Canada, Canadian Public Health Association. (1986). Ottawa Charter for Health Promotion. Ottawa: Canadian Public Health Association.
Woloshin, S., Schwartz, L. M., Katz, S. J. & Welch, H. G. (1997). Is language a barrier to the use of preventive services? Journal of General Internal Medicine, 12, 472-477.
Yakushko, O. & Chronister, K. (2005). Immigrant women and counseling: The invisible others. Journal of Counseling & Development, 83, 292-298.