Embed Size (px)
Citation preview

Implications for Peripheral Venous Access
Implications for Peripheral Venous Access
Gregory J. Schears, MD
Rochester, MN
The Science of Power Injection
Disclosures
Consultant & Participant
in Research for
Becton-Dickinson

Objectives• Review the pathophysiology of
extravasation induced tissue injury with an emphasis on contrast media
• Discuss the science of power injection and its impact on extravasation
• Provide new insights into the cause of extravasation and a technology that may help reduce this complication
IV InfusionComplications
Extravasation

DefinitionsExtravasation -
Is the inadvertent administration of a vesicant solution or medication into the surrounding tissues.
Vesicant –Is a solution or medication that causes the formation of blisters with subsequent sloughing of tissues occurring from tissue necrosis.
Infusion Nursing: An Evidence Based Approach, 3rd Edition, Saunders, Chapter V, 471-2, 2010
Access Related Cause
• A dislodged venous catheter or cannula
• Leaking of the medication or contrast media at injection site
• Rupture of the wall of the vessel
• Metal needles, large-gauge catheters
• Inadequate securement
• Undesirable site choice
Wilson, BG, Radiologic Tech, 2011; 83 (1): 63-77Sauerland, C, et.al., Oncology Nurs Forum, 33 (6) 2006, 1134-1141
Incidence-Extravasation
• Published reports from 0.01 to 6.5%
• For Contrast Media (CM) - 0.04 to 1.3%
• 39 Million Contrast enhanced CT-2007
• CM extravasations 15,600 – 507,000
Schulmeister, L, Seminars in Oncology Nursing, 2007; 23:184-190Sum, W, Ridley, LJ, Australasian Radiology, 2006; 50: 549-552 2007 CT Market Summary Report - March 2008", IMV Medical Information Division, Inc., pg. IV-57

Presentation
Wilson, BG, Radiologic Tech, 2011; 83 (1): 63-77
Presentation•Ranges from swelling and minor skin irritation and pain to severe skin and tissue necrosis, ulceration, vascular and nerve compromise to limb and life threatening compartment syndrome
•The severity of damage is directly related to the type, concentration and volume of the extravasated material
Infusion Nursing: An Evidence Based Approach, 3rd Edition, Saunders, Chapter V, 471-2, 2010

Vesicant Extravasation: Myths and Realities” by D.M. Boyle and C. Engelking, 1995, Oncology Nursing Forum, 22, p. 60.
VesicantsCause tissue injury when infused
outside the vascular space when:
• Direct or indirect toxicity (Chemo)
• ph < 5 or > 9 (Dopamine, Acyclovir)
• Osmolality > 600 mOsm / L (PPN, D25W)
Earhart, A, McMahan, P, JIN, 2011 345 (2) 97-105
VESICANTS
Sauerland, C, et.al., Oncology Nurs Forum, 33 (6) 2006, 1134-1141

VESICANTS
Sauerland, C, et.al., Oncology Nurs Forum, 33 (6) 2006, 1134-1141
Risk Factors• Device Related
– Metal needles, large gauge catheters
– Inadequate catheter securement
– Undesirable IV site location
• Agent Related– Vesicant
– Volume infiltrated
– Drug concentration
– Repeated use of same veinSauerland, C, et.al., Oncology Nurs Forum, 33 (6) 2006, 1134-1141
Risk Factors - continued
• Patient Related– Age (very young or old)
– Impaired communication
– Compromised circulation
– Altered sensory perception
– Fear, anxiety, cultural barriers, meds
• Clinician Related– Lack of knowledge
– Lack of IV skills
– Interruptions and distractionsSauerland, C, et.al., Oncology Nurs Forum, 33 (6) 2006, 1134-1141

Risk Factors - continued
• The Technique–Use of Power Injector
–Less optimal injection sites including lower limb and small distal veins
–Large volume of contrast
–High osmolar contrast medium
Bellin, MF, et.al., Eur Radiol, 2002; 12: 2807-2812
CompartmentSyndrome
Compartment Syndrome• Most feared physiology of extravasation
injury
• Most common severe injury associated with contrast media extravasation
• Occurs when swelling and increased pressure within a compartment compromise structures located within the compartment (blood vessels, nerves, muscles, and tendons)
Wilson, BG, Radiologic Tech, 2011; 83 (1): 63-77

Compartment Syndrome
Wilson, BG, Radiologic Tech, 2011; 83 (1): 63-77
Compartment Syndrome
Wilson, BG, Radiologic Tech, 2011; 83 (1): 63-77
Compartment Syndrome
Wilson, BG, Radiologic Tech, 2011; 83 (1): 63-77

Belzunegui et al. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine 2011, 19:9
Belzunegui et al. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine 2011, 19:9

• Amaral J, Traubic J, BenDavid G, et al. Safety of Power Injector Use in Children as Measured by Incidence of Extravasation. AJR 2006; 187:580-583
• Bellin M, Jakobsen J, Tomassin I, et al. Contrast Medium Extravasation Injury: Guidelines for Prevention and Management. Eur Radiol, 2002;12:2807-2812
• Belzunegui T, Louis C, Torrededia L, et al. Extravasation of Radiographic Contrast Material and Compartment Syndrome in the Hand: a case report. Scand J Trauma, 2011;19(9):1-4
• Birnbaum B, Nelson R, Chezmar J, et al. Extravasation Detection Accessory: Clinical Evaluation in 500 Patients. Radiology 1999; 212:431-438
• Bui K, Horner J, Herts B, et al. Intravenous Iodinated Contrast Agents: Risks and Problematic Situations. Clev Clin J Med, 2007;74(5):361-367
• Cohan R, Ellis J, Garner W. Extravasation of Radiographic Contrast Material:Recognition, Prevention, and Treatment.
Conventional Contrast
• Iodine provides vascular imaging contrast
• Higher [iodine] yields better opacification
• Higher [iodine] increases risk of AE
• Most contrast agents now nonionic
• The osmolality of nonionic contrast agents relates to its extravasation toxicity
Osmolality is a measure of the number of particles dissolved in 1 kg of water (mOsm/L)
Costa, N, JIN 2004; 27(5):302-311
Earhart, A, McMahan, P, JIN, 2011 345 (2) 97-105

MRI• Gadolinium-based contrast used in MRIs
• Typically lower extravasation toxicity than conventional contrast
• Lower volumes typically used ~ 14 ml
• Often hand injected
• Agents have high osmolality which can cause tissue injury
Earhart, A, McMahan, P, JIN, 2011 345 (2) 97-105Runge, VM, et.al., Invest Radiol 2002;37:393–398
Runge, VM, et.al., Invest Radiol 2002;37:393–398
MRI
CONTRAST
Rickham, R, et.al. Onc Nursing Forum, 33 (6) 1143-50, 2006

Prevention• Knowledge of vesicant potential
• Reducing / awareness of known risks
• Fresh, optimally functioning catheter
• Monitoring the site during Power Injection
• Educated, aware patient
Prevention
• Impedance monitor which detects changes
• Four true positives, 484 true negatives
• Twelve false positives = 2.4%
• Technology is expensive
Birnbaum, BA, Radiology; 1999, 212:431-38
PowerInjection

Science of Power Injection
Science of Power Injection
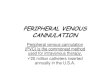
Infusion Induced Catheter Movement(IICM) is the movement of the catheter caused by the jet of fluid flowing from its distal end.
Science of Power Injection
10 ml Saline Pulsed 10 ml Saline Pushed

Science of Power Injection
Fluid Velocity & Thrust
Fluid Velocity = V = Q/A
Where:
Q = Flow rate
A = Cross-sectional area of lumen
DiffusicsOvineStudy

PurposeThis study will compared the
power injection induced angular deflection catheter motion of the BD Nexiva Diffusics 22 and 24ga product to 20, 22, and 24ga BD Insyte Autoguard
22 ga. BD Insyte Autoguard
22 ga. BD Nexiva Diffusics
Diffusics
Insyte

HypothesisThe additional catheter fenestrations
will reduce catheter motion in vivo compared to standard.
Reduction in catheter motion will help reduce catheter associated complications.
The additional catheter fenestrations will reduce catheter motion in vivo compared to standard.
Reduction in catheter motion will help reduce catheter associated complications.

Methods• Sheep model used as a human replicate for
insertional forces and catheter performance
• IACUC approved protocol, PIVs inserted with sheep under general anesthesia
• Catheter motion monitored using IR suite fluoroscopy and video recorded
• Ten ~ 150lb fully grown adult sheep
• Insertion sites shaved and depilator applied
Methods• Front and back legs used equally
• IV insertion alternated between IAG and Diffusics
• IV placed, secured with transparent dressing and allowed to in-dwell 6 min before power injection
• Omnipaque 350 Contrast Media used at room temperature
• 24 ga injected at 3 or 4 ml/sec for 10 sec
• 22 ga injected at 4 or 6.5 ml/sec for 10 sec
Methods
• Each catheter only 2 injections, the second higher than the first
• Steel ball in field as measurement standard
• Camera at 90 degrees of injection
• A total of 480 power injections performed
• Data analyzed for catheter motion, backout and any adverse events

Methods
Steel Ball for StandardizedVessel Size MeasurementSteel Ball for StandardizedVessel Size Measurement
Methods
Results
6.45.64.84.03.22.41.60.8
50
40
30
20
10
0
Vessel Diameter, mm
Freq
uenc
y
1.76 3.93
3.930 0.9623 2381.76 0.6117 11
Mean StDev N
Included V essel Diameter, mmExcluded V ein Diameters, mm
V ariable
Normal Histogram of Vessel Diameter, mm

24 ga BD Insyte at 3 ml/sec
24 ga BD Diffusics at 3 ml/sec
22 ga BD Insyte at 6.5 ml/sec

22 ga BD Nexiva Diffusics at 6.5 ml/sec
24 ga BD Insyte at 3 ml/sec-Extrav
24 ga BD Insyte at 3 ml/sec-Extrav

24 ga BD Nexiva Diffusics at 3 ml/sec
22 ga BD Insyte 6.5 ml/sec, extrav
22 ga BD Nexiva Diffusics at 6.5 ml/sec

24 ga std 4 ml/sec, Int & Ext
22 ga std 6.5 ml/sec, Int & Ext
Flow Rate N N Mean 95% Conf. Median
Product Gauge (mL/s) Analysis Excluded Deflection IntervalDeflectio
n SD Min Max
Diffusics 22 4.0 29 1 1.87 (1.27, 2.46) 1.26 1.57 0.00 6.44
Diffusics 22 6.5 29 1 4.91 (3.58, 6.24) 4.85 3.49 0.00 11.31
Diffusics 24 3.0 78 2 3.03 (2.22, 3.84) 1.79 3.61 0.00 20.19
Diffusics 24 4.0 78 2 8.40 (5.23, 11.58) 5.08 14.09 0.00 115.64
IAG 20 6.5 30 0 5.86 (4.19, 7.54) 4.14 4.48 0.00 16.82
IAG 22 4.0 30 0 5.50 (4.05, 6.95) 5.63 3.88 0.00 12.67
Results

Predicted Percent of Back-outs vs. Deflection Angle
Percentage of Whip/Flip as a Function of Deflection Angle

Predicted % of Extravasation as a Function of Deflection Angle
Results
Flow Rate Percent 95% Upper
95% Upper
Comparisons (mL/s) Difference Bound Criteria < Criteria
Diffusics 24ga - IAG 22ga 4 mL/s 8.0% 58.8% 181.8% TRUE
Diffusics 22ga - IAG 20ga 6.5 mL/s -17.3% 32.4% 170.6% TRUE
ResultsFlow Rate Diffusics 24ga IAG 24ga
Event (mL/s) Yes No Percent Yes No Percent
Catheter Backout Observed 3 0 78 0.0% 2 69 2.8%
Catheter Backout Observed 4 0 78 0.0% 14 54 20.6%
Extravasation Observed 3 0 78 0.0% 3 68 4.2%
Extravasation Observed 4 4 74 5.1% 22 46 32.4%
Catheter Flip/Whip 3 0 78 0.0% 1 70 1.4%

Results
ComparisonsPercent
Difference95% Upper
BoundAdjusted P-
Value
Diffusics 24ga 3ml/s vs IAG 24ga 3ml/s -67.3% -50.2% <0.0005
Diffusics 24ga 4ml/s vs IAG 24ga 4ml/s -72.5% -57.9% <0.0005
Diffusics 22ga 4ml/s vs IAG 22ga 4ml/s -48.7% -0.60% 0.05
CatheterSecurement
&Extravasation

Results• Using a transparent dressing for both
IAG and Diffusics catheter stabilization there were no episodes of catheter hubmovement in this acute model.
• A prior study with only tape in the same model securement demonstrated catheter hub movement.
Conclusions• Catheter movement without hub movement
was responsible for extravasation injury during power injection in the animal model
• IAG demonstrated IICM as has been seen before with PICCs under clinically relevant injection rates
• The angle of deflection predicted the likelihood of extravasation
• Transparent dressing was adequate securement to eliminate hub movement

Conclusions
• Diffusics catheters demonstrated non-inferior angular deflection even at one size below standard IAG catheters
• Diffusics catheters showed significantly less movement and were less likely to cause extravasation during power injection
• Diffusics may help reduce / prevent patient complications associated with power injection or even routine use.
References

• Amaral J, Traubic J, BenDavid G, et al. Safety of Power Injector Use in Children as Measured by Incidence of Extravasation. AJR2006; 187:580-583
• Bellin M, Jakobsen J, Tomassin I, et al. Contrast Medium Extravasation Injury: Guidelines for Prevention and Management. Eur Radiol, 2002;12:2807-2812
• Belloni B, Andres C. Extravasation of Peripherally Administered Parenteral Nutrition. N Engl J Med, 2011;364:10
• Belzunegui T, Louis C, Torrededia L, et al. Extravasation of Radiographic Contrast Material and Compartment Syndrome in the Hand: a case report. Scand J Trauma, 2011;19(9):1-4
• Birnbaum B, Nelson R, Chezmar J, et al. Extravasation Detection Accessory: Clinical Evaluation in 500 Patients. Radiology 1999; 212:431-438
• Bui K, Horner J, Herts B, et al. Intravenous Iodinated Contrast Agents: Risks and Problematic Situations. Clev Clin J Med, 2007;74(5):361-367
• Camp-Sorrell D. Developing Extravasation Protocols and Monitoring Outcomes. J Intraven Nurs, 1998;21(4):232-239
• Cohan R, Ellis J, Garner W. Extravasation of Radiographic Contrast Material:Recognition, Prevention, and Treatment. Radiology 1996; 200:593-604
• Costa N. Understanding Contrast Media. J Infus Nurs, 2004;27(5):302-312
• Earhart A, McMahon P. Vascular Access and Contrast Media. INS, 2011;34(2):97-105
• Namasivayam S, Kalra M, Torres W, et al. Adverse Reactions to Intravenous Iodinated Contrast Media: An Update. Curr Probl Diagn Radiol, 2006;July/Aug:164-169
• Runge V, Dickey K, Williams N, et al. Local Tissue Toxicity in Response to Extravascular Extravasaion of Magnetic Resonance Contrast Media. Investigative Radiology 2002;37(7):393-398
• Schulmeister L. Extravasation Management: Clinical Update. Semin Oncol Nurs, 2007;23:184-190
• Sinan T, Al-Khawari H, Chishti F, et al. Contrast Media Extravasation: Manual Versus Power Injector. Med Princ Pract, 2005;14:107-110
• Sum W, Ridley LJ. Recognition and Management of Contrast Media Extravasation. Australasian Radiology, 2006;50:549-552
• Wickham R, Engelking C, Sauerland C, et al. Vesicant Extravasation Prat I: Mechanisms, Pathogenesis, and Nursing Care to Reduce Risk. ONF, 2006;33(6):1134-1141
• Wickham R, Engelking C, Sauerland C, et al. Vesicant Extravasation Prat II: Evidence-Based Management and Continuing Controversies. ONF, 2006;33(6):1143-1150