Embed Size (px)
Citation preview

Implementing change to improve performance !
UK role in research
Prof Adrian Banning
Consultant Cardiologist
Oxford

Prof Adrian Banning
MY CONFLICTS
OF INTEREST ARE
Unrestricted research grant –
Boston
Consulting - Abbott, Medtronic,
Boston

UK role in Research why bother? ( a personal view)
Improve patient care (!)
Keep our life interesting
– In the lab and out of the lab
Keep our staff engaged
Evolve our specialty

UK role in PCI research in 1997?

UK role in PCI research in 1997?
Lord Flashheart
“Im the man who has no
underwear. Ask me
why ?”

UK role in PCI research in 1997?
Lord Flashheart
“Im the man who has no
underwear. Ask me why ?”
“Because the pants haven't been built yet that'll take the job on!”

UK role in Research why bother?
Improve patient care (!)
Keep our life interesting
– In the lab and out of the lab
Keep our staff engaged
Evolve our specialty
Stop UK becoming a backwater
– DES price @ £300

Recruited 2000-2003 Published …. 2005

UK role in research
Developments in research infrastructure
– CCRN & CLRN
– BRC
– AHSC
Perspectives from industry
– Syntax , FAME, Excel, ABSORB II
– Apologies eg BBC- 1, Tryton, Cappella, DAPT etc
BCIS

NIHR

Biomedical Research Centres
2012 - 5 yr funding
– UCH,
– Maudsley, GOSH, Moorfields, Marsden
– Cambridge,
– Oxford,
– Imperial,
– Newcastle,
– Southampton,

Comprehensive research networks

CCRN : CLRN

CLRN: the portfolio

Other opportunities….
BCIS dataset NICOR
– Peter Ludman
HTA assessments
– Already funded….
UK TAVI trial
Revived

UK role in research “bridging the gap”
Lack of understanding of the clinical
challenges and motivations for research
Increased regulation and paperwork
Need for a process(es) to facilitate
participation

Academic Health Science Networks
Innovation Health & Wealth
(Dec 2011):
Described a need for “a more systematic
delivery mechanism for diffusion and
collaboration across the NHS by building
strong cross boundary networks”

Academic Health Science Networks
It recognised that innovation was important to meet the Nicholson Challenge, while maintaining quality of care and to address the need for the NHS and UK Life Sciences to contribute to the nation’s wealth
Recommended the introduction of AHSNs to “ align education, clinical research, informatics, training and healthcare delivery”
”

Academic Health Science Networks
Goal: “To improve patient and population health outcomes by
translating research into practice and developing and
implementing integrated health care systems”
This was a recognition that while AHSCs and BRCs had been
successful with early (t1 and t2) translation they had not had
much impact with later translation (t3 and t4)
AHSNs are to provide a population of 3 to 5m, which will allow
scalable embedding of early translation discoveries into
mainstream clinical practice

Academic Health Science Networks
1. 15 AHSNs to cover England
2. Expressions of Interest: submitted July 2012
3. Applications submitted: October 2012
4. Formal interviews: December 2012 to February 2013 (a development and assurance process)
5. Designation of all 15 planned by Q1 2013

Academic Health Science Networks
AHSNs are co-terminous with the 15 new NIHR clinical research networks They are to “act as a high value gateway for any NHS organisation needing support or help with innovation and provide industry with focused points of access to the NHS”
They will
support the Comply or Explain regime relating to NICE TAs
work with SMEs on medical technology projects
Drive innovation at pace and scale
Support and increase opportunities for patients to participate in research

That’s all well and good but what about industry?
What did the Romans ever do for us?

That’s all well and good but what about industry?
What did the Romans ever do for us?

What industry wants
Rapid processing of paperwork
Rapid recruitment
Quality data
High rates of follow up
Active participation
Development is expensive

What industry research can do for you
Directly compare your (our) practice with
the rest of the world

71% enrolled (N=3,075)
All Pts with de novo 3VD and/or LM disease (N=4,337)
Treatment preference (9.4%)
Referring MD or pts. refused informed consent (7.0%)
Inclusion/exclusion (4.7%)
Withdrew before consent (4.3%)
Other (1.8%)
Medical treatment (1.2%) TAXUS n=903
PCI n=198
CABG n=1077
CABG n=897
no f/u n=428
5yr f/u n=649
PCI all captured w/
follow up
CABG 2500
750 w/ f/u vs
Total enrollment N=3075
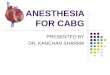
Stratification: LM and Diabetes
Two Registry Arms
Randomized Arms n=1800
Two Registry Arms N=1275
Randomized Arms N=1800
Heart Team (surgeon & interventionalist)
PCI n=198
CABG n=1077
Amenable for only one treatment approach
TAXUS*
n=903 CABG n=897
vs
Amenable for both treatment options
Stratification: LM and Diabetes
LM 33.7%
3VD 66.3%
LM 34.6%
3VD 65.4%
23 US Sites 62 EU Sites +
SYNTAX Trial Design
*TAXUS Express

Enrolling Centers in the UK
CABG Investigator PCI Investigator Site
Stephen Westaby Adrian Banning John Radcliffe Hospital
Geoff Berg Keith G. Oldroyd Western Infirmary
Steven A. Livesey Keith D. Dawkins Southampton University Hospital
Jatin B. Desai Martyn R. Thomas King's College Hospital London
Tomasz J. Spyt Anthony H. Gershlick Glenfield Hospital
Andrew Forsyth Adam de Belder Royal Sussex County Hospital
Graham Venn Simon Redwood St. Thomas & Guys
Patrick Magee Martin T. Rothman London Chest Hospital

Randomized Patient Enrollment
Rest of Sites N=1533
N=267
CABG n=132
PCI n=135
CABG n=765
PCI n=768

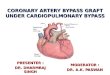
Patients Enrolled Per Site UK Subset
42 4 4
41 12 4
40 33 2
32 9 3
32 4 5
32 12 1
32 19 1
16 2
0 10 20 30 40 50 60 70 80
Total Patients Enrolled (N)
Banning/Westaby
Oldroyd/Berg
Dawkins/Livesey
Thomas/Desai
Gershlick/Spyt
DeBelder/Forsyth
Redwood/Venn
Rothman/Magee
Randomized
CABG Registry
PCI Registry

30
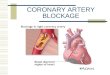
12 month MACCE CABG vs TAXUS
Size of circle adjusted for number of patients
CABG MACCE (%)
TA
XU
S S
tent
MA
CC
E (
%)
-5
5
15
25
35
45
55
65
75
85
95
105
-5 5 15 25 35 45 55 65 75 85 95 105
John Radcliffe Infirmary (UK)
CABG MACCE (%)
TA
XU
S S
tent
MA
CC
E (
%)
-5
5
15
25
35
45
55
65
75
85
95
105
-5 5 15 25 35 45 55 65 75 85 95 105
John Radcliffe Infirmary (UK)
CABG MACCE (%)
TA
XU
S S
tent
MA
CC
E (
%)
-5
5
15
25
35
45
55
65
75
85
95
105
-5 5 15 25 35 45 55 65 75 85 95 105
CABG MACCE (%)
TA
XU
S S
tent
MA
CC
E (
%)
-5
5
15
25
35
45
55
65
75
85
95
105
-5 5 15 25 35 45 55 65 75 85 95 105
John Radcliffe Infirmary (UK)

SYNTAX 5-year Outcomes • July 2012 • Slide 31
PCI MACCE (%)
CA
BG
MA
CC
E (
%)
Size of circle adjusted for number of patients
Individual Centers: MACCE to 5 Years for CABG & PCI
Oxford

Syntax trial…… K Dawkins
SYNTAX budget was $65M,
– and we shipped 60,000 stents

Ref. NEJM Vol 260, No 3, pp 213-224. Slides courtesy Nico H J Pijls.
Fractional Flow Reserve
versus
Angiography for
Multivessel
Evaluation
FRACTIONAL FLOW RESERVE
versus ANGIOGRAPHY
FOR GUIDING PCI IN PATIENTS WITH
MULTIVESSEL CORONARY ARTERY DISEASE

Ref. NEJM Vol 260, No 3, pp 213-224. Slides courtesy Nico H J Pijls.
Participating Centers USA (6)
Stanford University (William F. Fearon)
Northeast Cardiology, Bangor, Maine (Peter N. Ver Lee)
University of Louisville (Massoud Leesar)
St Louis University (Michael Lim)
University Hospital Virginia (Michael Ragosta) University of South Carolina (Eric Powers)
EUROPE (14)
King´s College Hospital, London) (Phil MacCarthy)
Cardiovascular Center Aalst (B. De Bruyne) Catharina Hospital Eindhoven (N.Pijls)
Rigshospitalet, Copenhagen (T.Engstrom)
Klinikum der Universitat Munchen(V.Klauss)
Aarhus University Hospital (Ole Frobert)
University Hospital Bergmannsheil
(Waldemar Bojara)
Sodersjukhhuset, Stockholm (I Herzfeld)
Helsingborgs Lasarett (F Schersten)
Klinikum Darmstadt (Gerald Werner)
Bristol Royal Infirmary (A.Baumbach) Staedt. Krankenhaus, Bogenhausen (G.Riess)
Glasgow Western Infirmary
(Keith Oldroyd)
Royal Victoria Hospital, Belfast (Ganesh Manoharan)


Americas Country Leaders Argentina - Jorge Belardi, Daniel Navia
Brazil – Alexandre Abizaid, Luiz Carlos Bento de Souza
Canada- Marc Ruel, Erick Schampaert
US – David Kandzari, John Puskas
EXCEL Leadership Team
Gregg W. Stone, MD Columbia University Medical
Center New York, NY USA
Patrick Serruys, MD
Erasmus Medical Center Rotterdam, The Netherlands
Joseph Sabik, MD Cleveland Clinic Main Campus
Cleveland, OH USA
A. Pieter Kappetein, MD Erasmus Medical Center
Rotterdam, The Netherlands
EU Country Leaders Poland – Pawel Buszman, Andrzej Bochenek
Spain – Manel Sabate, Jose Luis Pomar Switzerland – Stephan Windecker, Thierry Carrel The Netherlands – Patrick Serruys, AP Kappetein
UK – Tony Gershlick, David Hildick-Smith, David Taggart
EU Country Leaders Belgium – Bernard De Bruyne, Paul Sergeant France – Marie Claude Morice, Mauro Romano
Germany – Christian Hamm, J. Gummert Hungary – Béla Merkely, Laszlo Szekely Italy – Marco Valgimigli, Carol Savini,
Asia Pacific Country Leaders
Australia – Ian Meredith, Julian Smith Korea – Seung Jung Park, Jae Won Lee
EXCEL Principal Investigators

First randomised Excel case worldwide
Oxford Nov 2011
5stents 2 LCx, 2 LAD, 1 Left main

Excel recruitment Jan 2013

183/996 patients recruited in the UK
18% total

BCIS research group
New Research lead

Implementing change to improve performance ! We are in tough financial times
For a number of legitimate reasons (and
some others) changing our clinical practice
in the UK will be hard work
Contributing to “research” (at any level)
will help patients and
– might help keep you sane

Research can be….