Embed Size (px)
Citation preview

NSAP CQI Webinar
Implementing Change: Tips for making change in the clinical
environment Robyn Wright
Quality & Risk Coordinator Banksia Palliative Care Service
24 April 2013

Aim:
Use a change management framework to explore
implementing an new assessment tool in to a
community palliative care service

Background Banksia Palliative Care Service (Banksia) was one of 20 palliative care services that participated in the NSAP
Collaborative Improvement Project – Assessment and Care Planning (CIP: A&CP)
Project Aims:
• All patients have an assessment that is patient centred and holistic
• All patients have a care plan that is holistic and current, that demonstrates patient involvement
Banksia Is a specialist community palliative care service providing home-based care to children and adults with a
progressive terminal illness in the local government areas of Banyule, Nillumbik and Whittlesea in Victoria.
Care is provided by an interdisciplinary team that consists of nursing, social workers/counsellors, spiritual
care worker, music and massage therapists and sessional palliative care physician. The model of care is
community based and recognises that the client is the centre of a broader social unit which may include the
family, friends and community.

Change management model
• John Kotter’s 8-step process of
successful change References: • Kotter, J. (2007). Leading change: why transformation efforts fail.
Harvard Business Review, Jan. 96-103. • Kotter, J., Rathgeber, H. (2006). Our Iceberg is melting: changing
and succeeding under any conditions. Macmillian: London.
8-step process Set the stage 1. Create a sense of urgency 2. Pull together the guiding team Decide what to do 3. Develop the change vision and strategy Make it happen 4. Communicate for understanding and buy-in 5. Empower others to act 6. Produce short-term wins 7. Don’t let up Make it stick 8. Create a new culture
Step 1: Create a sense of urgency • Help others to see the need for change and the importance of acting
immediately
• Communicate the need broadly and dramatically
Banksia • Long recognised need to review our care plan and client assessment pro forma
• Participation in the CIP:A&CP created need to for action – Accepted into the pilot program
– One of 20 agencies
– National program
– EO signed a commitment to do something, provide data, present our results
– Committed to the set timeframe May to Dec 2011
• Baseline data demonstrated the gaps in holistic assessment, in particular emotional, cultural and spiritual assessment

Step 1: Create a sense of urgency
Challenges • Can be difficult to achieve (failure in this step is high) • Tendency to shoot the bearer of bad news – particularly if
change is in response to poor performance • Not easy to drive people out of their comfort zone • Lack of patience…”enough with the preliminaries – let’s get
on with it” • Overwhelmed or paralyzed by the downside possibilities
– Staff become defensive
– Morale drops
– Events may spin out of control

Step 1: Create a sense of urgency When is the urgency rate high enough? • Rule of thumb: 75% of management/staff are convinced that the
status quo is unacceptable “Change begins well when a good leader sees the need for change”

Step 2: Pull together a guiding team • Leadership doesn’t rest with the Senior Manager,
Executive or Head of Unit • Successful change needs a powerful group guiding the
change – one with leadership skills, credibility (expertise, reputation), communications ability, authority, analytical skills, and a sense of urgency……’powerful guiding coalition’
Banksia • Working group – senior clinicians (nursing and
psychosocial team), Department Managers, Quality & Risk Coordinator and Executive Officer (Chair)

Step 2: Pull together a guiding team Challenges • The guiding team may have no history of working together • Important to develop a shared assessment of the problem and
opportunities • Need to create a minimum level of trust, communication and
teamwork • Managing changes in the guiding coalition “Efforts that don’t have a powerful enough guiding coalition can make apparent change for a while but sooner or later opposition
gathers itself together and stops the change.”

Step 3: Develop a change vision and strategy
• Develop a picture for the future that is easy to communicate with a clear compelling statement of where the change is leading
Banksia Project Plan This project will This project will not include • Develop an agreed client assessment
framework that is holistic and client centred
• Bereavement assessment
• Death Audit
• Intake/triage assessment
• Referral process
• Discharge Planning
• Family meetings
• Care Coordinator Role

Step 3: Develop a change vision and strategy
Challenges • Without a clear vision change can easily dissolve into
mess of incompatible activities • Staff become confused or alienated
“If you can’t communicate the vision to someone in five minutes or less and get a reaction that signifies both understanding and interest you’ve not completed this
phase in the change process”

Step 4: Communicate for understanding and buy-in
• Make sure as many others as possible understand and accept the vision and strategy
• Credible communication (lots and lots of it) using all existing communication channels to
broadcast the vision of the change
• We often signficantly under-communicate the vision for the change
Banksia
• CIP: A&CP Standing item on the monthly quality committee agenda
• Working group meetings were minuted (simple action style minutes)
• Storyboard to report progress (displayed in the clinical area) – captured the work of the working
group
• Working/draft protocols to support the implementation of the new tool and clarify our thinking
• Next time…..documented implementation and communication plan
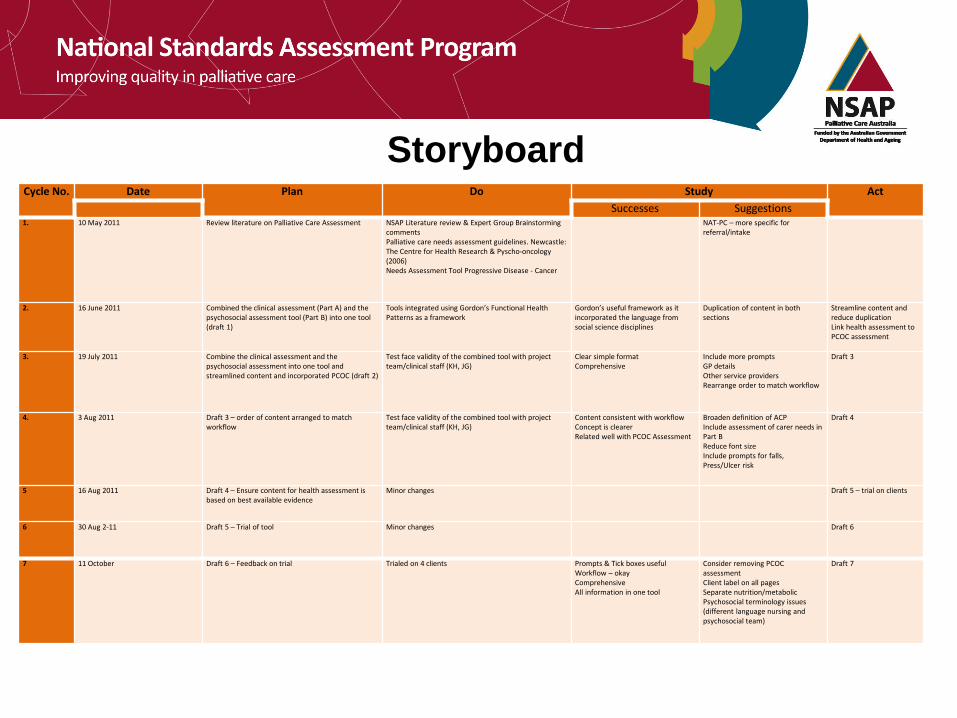
Storyboard Cycle No. Date Plan Do Study Act
Successes Suggestions 1.
10 May 2011 Review literature on Palliative Care Assessment NSAP Literature review & Expert Group Brainstorming comments Palliative care needs assessment guidelines. Newcastle: The Centre for Health Research & Pyscho-oncology (2006) Needs Assessment Tool Progressive Disease - Cancer
NAT-PC – more specific for referral/intake
2. 16 June 2011 Combined the clinical assessment (Part A) and the psychosocial assessment tool (Part B) into one tool (draft 1)
Tools integrated using Gordon’s Functional Health Patterns as a framework
Gordon’s useful framework as it incorporated the language from social science disciplines
Duplication of content in both sections
Streamline content and reduce duplication Link health assessment to PCOC assessment
3. 19 July 2011 Combine the clinical assessment and the psychosocial assessment into one tool and streamlined content and incorporated PCOC (draft 2)
Test face validity of the combined tool with project team/clinical staff (KH, JG)
Clear simple format Comprehensive
Include more prompts GP details Other service providers Rearrange order to match workflow
Draft 3
4. 3 Aug 2011 Draft 3 – order of content arranged to match workflow
Test face validity of the combined tool with project team/clinical staff (KH, JG)
Content consistent with workflow Concept is clearer Related well with PCOC Assessment
Broaden definition of ACP Include assessment of carer needs in Part B Reduce font size Include prompts for falls, Press/Ulcer risk
Draft 4
5
16 Aug 2011 Draft 4 – Ensure content for health assessment is based on best available evidence
Minor changes Draft 5 – trial on clients
6
30 Aug 2-11 Draft 5 – Trial of tool Minor changes Draft 6
7
11 October Draft 6 – Feedback on trial Trialed on 4 clients Prompts & Tick boxes useful Workflow – okay Comprehensive All information in one tool
Consider removing PCOC assessment Client label on all pages Separate nutrition/metabolic Psychosocial terminology issues (different language nursing and psychosocial team)
Draft 7
Step 5: Empower others to act
• Remove as many barriers as possible so that those who want to make the vision a reality can do so
Banksia • Force field analysis prior to implementation of the new
assessment tool – Driving forces – Restraining forces

Step 5: Empower others to act Driving Forces Restraining forces
Comprehensive health assessment
• Combines physical and psychosocial
• Holistic not just medically focused
Consistent with National Palliative Care Standards
Clinical Tool
• Consistency in approach to assessment
• Less subjective
• Facilitates collection of client data
• Can be scanned into Bankpall (Electronic Client Record)
Good foundation to establish a client centred care plan
• Comprehensive assessment – comprehensive care plan
• Prompts to promote follow up actions
Workforce driven
Opportunity to be part of National project with collective goals of being holistic and client centred
More paperwork/forms (need to be a trade off)
Terminology
• New
• Confronting
Difficulty containing
• the assessment interview
• emotions solicited by the interview questions
Need to complete the assessment may be a barrier to a good discussion
7 pages/too busy
Time
Variation in skill set /confidence in assessment
How much detail is required in first visit if the admission is urgent?

Step 5: Empower others to act
Challenges
• No organisation has the momentum, power or
time to get rid of all the obstacles – focus on the
big one

Step 6: Produce short-term wins • Real change takes time – at risk of losing momentum
• Create some visible, unambiguous successes as soon as possible
Banksia • Celebrated minor breakthroughs
– Acknowledgement of the different worldview that each discipline holds
– Agreed framework
– Establishing a common language
– Initial response for clinical staff was very positive
• Look for small successes that may come in the form of words instead of deeds

Step 7: Don’t let up • Press harder and faster after the first successes until the change has sunk into
the organisational culture – the new approach is fragile and subject to regression
• Tackle the broader problems (structures and systems) that are consistent with the new process
Banksia • Implemented the tool in March 2012 – reviewed in 3 months
• May audit for completeness demonstrated that further work required in psycho-social
assessment and a review of workpractices in undertaking an initial assessment.
• In the process of introducing a validated assessment tool for anxiety & depression (HAD)
• On the back of this health assessment we have modified our interdisciplinary care plan. It
was the logical follow on from the changed assessment framework.
Step 8: Create a new culture • Hold onto the new ways of behaving, and make sure that they
succeed, until they become strong enough to replace old traditions
Banksia • Demonstrate that the new approach will improve performance
– Documentation audits - completion of a comprehensive client-centred assessment (physical, social, cultural, spiritual and emotional)
– Increase referrals to the psychosocial team – More comprehensive assessments of pain on admission (Victorian
PCCN clinical pain indicators)

Questions?