Embed Size (px)
Citation preview

Implementing Change
Session 4July 25, 2017

Today’s Presenters
Mary Andrawis-Refila, PharmD, MPHExecutive Director, Medication Safety and Quality Health Services Advisory Group (HSAG)
2
Kim Werkmeister, BA, RN, CPHQ, CPPSClinical Improvement EducatorHospital Quality Institute (HQI)
Session 4July 25, 2017
The HSAG HIIN ADE SPRINT
Aim:To reduce adverse drug events (ADEs) as measured by international normalized ratios (INRs) greater than 5, glucose less than 50, and naloxone for opioid reversal by 20 percent compared to a baseline year of 2015 by December 31, 2017, in all HSAG HIIN hospitals.
How will we accomplish this? By creating a community of medication safety leaders sprinting together toward a rapid, tangible reduction in specific ADEs over a short period of time by implementing small tests of change.
3

Report Out From Last Session
• Process for generating monthly ADE performance reports on the ADE measures
• Flowcharting your processes
4

Objectives
1. Review tools to perform a gap analysis of current processes and discuss action planning at the local level.
2. Examine techniques for readiness assessments/gap analyses and spread of interventions.
3. Distinguish between implementation and testing strategies.
4. Create a plan for updating run charts and spread of interventions.
5

How Do We Know if Our Processes Are Safe?
6
• Do we have enough data and are those data complete? How do we know?
• Are we looking at what matters?
• What tools are available to help?

Finding ADEs in Your Organization
“No wrong-door approach”• Trigger medications• Organizational gap analyses/self assessments• Leadership rounds• Pharmacy rounds• Data from event reports, pharmacy systems• Patient identified—what are they telling you?
7

Tools of the Trade: Gap Analysis
8

Gap Analysis Tools for Medication Safety
1. 2011 ISMP Medication Safety Self Assessment for Hospitalshttps://www.ismp.org/selfassessments/Hospital/2011/full.pdf
2. The IHI Trigger Tool for Measuring Adverse Drug Events www.IHI.org
3. Roadmap to a Medication Safety Programhttp://www.mnhospitals.org/Portals/0/Documents/ptsafety/ade/Medication-Safety-Roadmap.pdf
9

Self Assessment Tools for High-Alert Medications
1. Minnesota Hospital Association Anticoagulation Agent Adverse Drug Event Gap Analysishttp://www.mnhospitals.org/Portals/0/Documents/ptsafety/ade/Medication-Safety-Gap-Analysis-Anticoagulation-Agent.pdf
2. 2017 ISMP Medication Safety Self Assessment for Antithrombotic Therapyhttp://www.ismp.org/selfassessments/Antithrombotic/2017/2017_ISMP_Antithrombotic_Self_Assessment.pdf
10

Self Assessment Tools for High-Alert Medications (cont.)
3. Minnesota Hospital Association Opioid Agent Adverse Drug Event Gap Analysishttp://www.mnhospitals.org/Portals/0/Documents/ptsafety/ade/Medication-Safety-Gap-Analysis-Opioid.pdf
4. Pennsylvania Hospital Engagement Network: Organization Assessment of Safe Opioid Practiceshttp://patientsafety.pa.gov/pst/Documents/Opioids/organization.pdf
11

Self Assessment Tools for High-Alert Medications (cont.)
5. Pennsylvania Patient Safety Authority Opioid Knowledge Self Assessmenthttp://patientsafety.pa.gov/pst/Documents/Opioids/assessment.pdf
6. Minnesota Hospital Association Hypoglycemic Agent Adverse Drug Event Gap Analysishttp://www.mnhospitals.org/Portals/0/Documents/ptsafety/ade/Medication-Safety-Gap-Analysis-Hypoglycemic.pdf
12
Steps to Performing a Medication Safety Gap Analysis
• Identify best practice recommendations related to medication safety. – Field guides, national toolkits, patient safety
organizations
• Use a structured tool to compare the recommendations with your organizational practice.– Gap analysis tools and organizational self
assessments from patient safety organizations
13

Steps to Performing a Medication Safety Gap Analysis (cont.)
• Determine the differences between the organization’s practice versus the recommendations. – AHRQ1 Gap Analysis Tool
• Prioritize the gaps by calculating a risk priority number using a standard score. – FMEA2 Scoring System from VA Patient Safety or IHI3
• Determine implementation plans to improve safety with the support of organizational leadership.
141. Agency for Healthcare Research and Quality2. Failure Modes and Effects Analysis3. Institute for Healthcare Improvement

Will We Really Find Out Something We Don’t Already Know?
• A gap analysis requires input from the whole team, which means time and resources. Is it worth it? Don’t we already know our gaps?
• Pennsylvania Patient Safety Authority Opioid Knowledge Self Assessment
• Let’s try a few questions
15

Pennsylvania Opioid Knowledge Self-Assessment
• Assess practitioners’ knowledge of opioids• 11 multiple choice questions• Intended for ALL practitioners involved with
opioid use– Prescribers– Pharmacists– Nurses
16
Types of Questions
• Opioid-naïve vs. opioid-tolerant patients• Long-acting opioids• Equianalgesic dosing
– HYDROmorphone dosing vs. morphine dosing
• Patient-specific conditions requiring a lower starting dose of opioids
• Concomitant medications• Monitoring the effects of opioids
17
Polling Question 1
1. Patients who are considered opioid-tolerant are those who have been: a. Taking acetaminophen 300 mg with codeine 30 mg,
up to 5 doses a week b. Taking oxyCODONE 10 mg with acetaminophen
325 mg 4 times daily for 5 days c. Taking oxyCODONE 10 mg with acetaminophen
325 mg 4 times daily for 14 days d. Taking extended-release morphine 15 mg twice daily
for 1 week e. All of the above
18

Polling Question 2
2. The most important predictor of respiratory depression in patients receiving intravenous (IV) opioid analgesics in the hospital setting is: a. Respiratory rate b. Patient-reported pain intensity c. Sedation level d. Blood pressure e. All of the above
19

Polling Question 3
3. Which of the following statements about long-acting opioids is true? a. They are intended for use for pain on an as-needed
basis. b. They are indicated for pain in the immediate
postoperative period (12 to 24 hours following surgery). c. They are indicated for pain during the postoperative
period, if the pain is not expected to persist for an extended period of time.
d. They are only indicated if the patient is opioid tolerant and has already been receiving the drug prior to surgery.
e. All of the above
20

What Comes Next?
We’ve determined our gaps—now how do we choose strategies for improvement?
21
www.HSAGHIIN.orgTools and Resources
Adverse Drug Event Field Guide
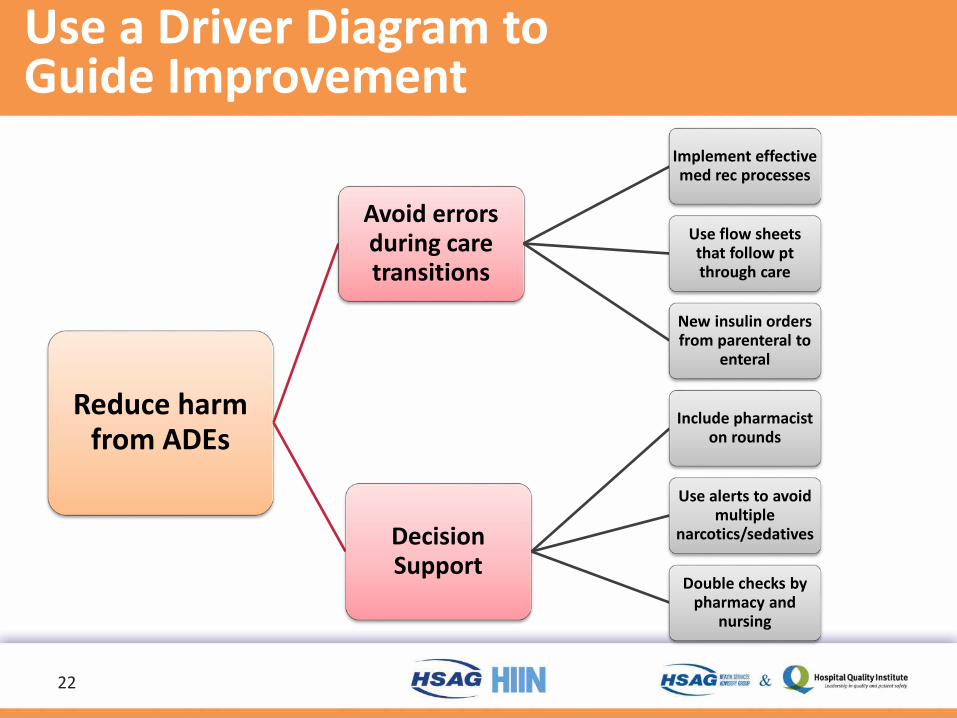
Use a Driver Diagram to Guide Improvement
22
Reduce harm from ADEs
Avoid errors during care transitions
Implement effective med rec processes
Use flow sheets that follow pt through care
New insulin orders from parenteral to
enteral
Decision Support
Include pharmacist on rounds
Use alerts to avoid multiple
narcotics/sedatives
Double checks by pharmacy and
nursing
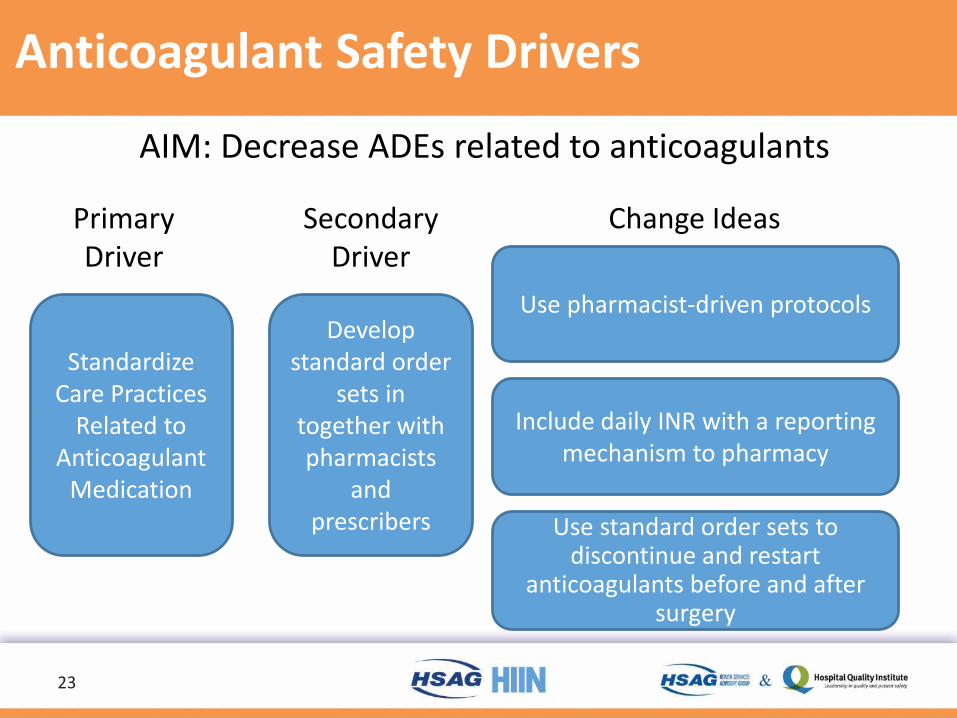
Anticoagulant Safety Drivers
23
AIM: Decrease ADEs related to anticoagulants
Change IdeasPrimaryDriver
Standardize Care Practices
Related to Anticoagulant
Medication
SecondaryDriver
Develop standard order
sets in together with pharmacists
and prescribers
Use pharmacist-driven protocols
Include daily INR with a reporting mechanism to pharmacy
Use standard order sets to discontinue and restart
anticoagulants before and after surgery

Hypoglycemic Agent Safety Drivers
24
AIM: Decrease ADEs related to hypoglycemic agents
SecondaryDriver
Develop standard order
sets in together with pharmacists prescribers
and dietitians
PrimaryDriver
Standardize Care Practices
Related to Hypoglycemic
Medication
Change Ideas
Use basal bolus insulin correction
Discontinue the use of sliding scale insulin
Use standard order sets to respond to hypoglycemia that include assessment of insulin orders even after one epidose

Opioid Medication Safety Drivers
25
AIM: Decrease ADEs related to opioids
PrimaryDriver
Prevention of Failure to
Rescue
SecondaryDriver
Use standardized
approaches to safely manage opioid dosing
Change Ideas
Use pharmacy and/or CPOE alerts to avoid layering multiple
sedatives and opioids
Review unanticipated uses of reversal agents
Use standardized assessment tools to identify high risk patients
and sedation levels

Opioid Medication Safety Drivers
26
AIM: Decrease ADE Related to Opioids
PrimaryDriver
Prevention of Failure to
Rescue
SecondaryDriver
Use standardized
approaches to safely manage opioid dosing
Change Ideas
Use pharmacy and/or CPOE alerts to avoid layering multiple
sedatives and opioids
Review unanticipated uses of reversal agents
Use standardized assessment tools to identify high risk patients
and sedation levels

Change Idea
Use standardized assessment tools for opioid medication safety.
Step One: Pick an assessment tool to test.• Pasero Opioid-Induced Sedation Scale (POSS)• Richmond Agitation Sedation Scale (RASS)• Sedation Agitation Scale (SAS)
27
Change Idea (cont.)
Use standardized assessment tools for opioid medication safety.
Step Two: Find your champions and ask them to help you test.Step Three: Start small and then expand the use of the assessment tools more broadly, making changes along the way based on immediate feedback.
28

But How Will We Do That?
29
Aim
Measure
Small tests of change
PDSA—Test Your Change Idea
And then ask:Do weAdopt,Adapt,
orAbandon?
30
Discussion/QuestionsMary Andrawis-Refila, PharmD, MPH
Kim Werkmeister, BA, RN, CPHQ, [email protected]
31