Embed Size (px)
Citation preview

Implementation of ICH Q3D in Product
Development.
Presentation by Dr. Laurence. J. Harris (Lhasa
consortium member and Pfizer Colleague) at the
3rd Annual Impurities: Genotoxic and Beyond
Summit, 12 - 13 June 2019, Munich, Germany.

Outline
• ICH Q3D background knowledge.
• Implementation.
– tools developed to support implementation;
• flexible procedural guidance.
• risk assessment template.
• template for submission of the risk assessment summary.
• fit for purpose analytical methodology.
• Excipients.
• Using prior knowledge (data) to make the risk assessment process more efficient.
• Case histories.
– example risk assessments.
– control strategies.
• Conclusions / Learnings.

ICH Q3D background
• ICH Q3D is the “Guideline for Elemental Impurities”
• Applicable to new finished drug products (as defined in Q6A and Q6B) and new drug products containing existing drug substances.
• Does not apply to drug products used during clinical research stages of development.
– applicable to the commercial product. However, the principles can be usefully applied earlier in the development process.
• Because elemental impurities do not provide any therapeutic benefit to the patient, their levels in the drug product should be controlled.
• Approved guideline was published Dec 2014.
– 3yr implementation timeline for existing marketed products (Dec 2017).
– applicable to new drug products after ~18M (mid 2016).
– aligned Pharmacopoeial requirements established e.g. USP<232>.
• Useful resources;
– FDA “Guidance for Industry” 2018.
– ICH training modules (see next slide).
background

Elemental impurity PDEs background

Resources
ICH training materials
Training Module 0: Introduction
Training Module 1: Other Routes of Administration
Training Module 2: Justification for Elemental Impurity Levels Higher
than an Established PDE
Training Module 3: Acceptable Exposures for Elements without a PDE
Training Module 4: Large Volume Parenteral Products
Training Module 5: Risk Assessment and Control of Elemental
Impurities
Training Module 6: Control of Elemental Impurities
Training Module 7: Converting between PDEs and Concentration Limits
Training Module 8: Case studies
Training Module 9: Frequently Asked Questions
Overview article: A. Teasdale et. al, Pharmtech Europe, 2015(3), p12ff
background

Elements, limits and control options
• The guideline lists 24 elements that need to be considered in a drug
product focussed risk assessment (RA).
– elements are divided in different classifications based upon toxicity /
“abundance” - which also aids the RA process.
• Permitted Daily Exposures (PDEs) are established for each element
based on oral / parenteral / inhaled routes of administration.
• A control threshold (30% of the PDE) has been established to help
assess the significance of a measured or predicted daily intake of each
element.
– if the RA fails to establish that an EI is consistently < the control
threshold then controls should be established to ensure that the EI does
not exceed the PDE.
• Drug product manufacturer has a range of options available to
demonstrate risk of exceeding established limits is negligible.
background

Component approaches are generally preferred
7
Option 3
Finished Product Analysis; measure the
concentration of each element in the
finished drug product and compare to the
PDE
Option 2a
Common permitted concentration limits of
elements across all drug product components
for a drug product with a specified maximum
daily intake
Option 1
Common permitted concentration limits of
elements across all drug product components
for drug products with maximum daily intake
of <10 grams
Option 2b
Different permitted concentration limits of
elements in individual components of a drug
product with a specified maximum daily intake
background

The risk assessment
• The RA drives the decision to analyse components of the DP or the DP itself.
• Don’t test the drug product for all 24 EIs and then consider risks!
• A combination of risk analysis and available supportive data leads to a robust control strategy.
Water
Drug
Substance
Excipients
Manufacturing
Equipment Containers
Closures*
EI in DP
background
(Co, V <0.2% in 316L &
Ni ~ 11% in 316L)
*Jenke et al, PDA J Pharm Sci Technol Vol. 69(1), p 1-48
(2015) & PDA J Pharm Sci Technol Vol. 67(4), p 645-57
(2013)

Elements to be considered in the RA background

Implementation
• What are my deliverables?
1. a documented risk assessment that is held at the manufacturing
site and available for inspections.
2. summary of the risk assessment in the CTD.
3. controls established that are consistent with the RA & CTD
summary.
4. on-going re-evaluation of the RA if there are significant changes
throughout the product lifecycle.
implementation

Implementation of ICH Q3D in development;
Challenges
• Each project is very different!
– route of admin, dosing, speed of development, parallel formulations,
multiple different excipients, switching API route of synthesis etc.
• Pharmaceutical organizations are generally large and Global so
there are a lot of people to train!
• Guideline though fairly complex is clear.
• It is very new, so industry and regulators are all on a learning
curve.
– expect to have queries on your submissions.
• Drug products with routes of administration not covered by the
guideline e.g. topicals.
implementation

Implementation of ICH Q3D in development
• A successful implementation will benefit from;
– sponsors and change agents.
– procedural guidance and training.
– RA tools that drive a consistent approach.
– templates for generation of RA summaries required for the CTD.
– access to data that helps to reduce the testing burden.
– fit for purpose (generic) analytical methodology (ICP-MS).
implementation

Tools - flexible procedural guidance
• Internal guidance document based upon ICH Q3D.
– training delivered to analytical project leads.
– awareness training delivered to formulators, process chemists, regulatory strategists.
• If a project team follows the procedure they will meet all required deliverables.
• Flexibility around control options, but the “component approach” is encouraged / preferred.
• Q3D “lite” for early phase materials
– no RA mandated, any testing is focussed on gathering data for API (typically class 1, 2A and added catalysts), compendial excipients, fit for purpose analytical methods used.
• Q3D “compliance” expected for late phase projects
– targets established for API and DP when the RA shows they are necessary
– typically added catalysts are monitored via the specification, especially catalysts added at late stages of the route.
implementation

Tools - risk assessment template
• Excel based template has been developed.
– probably a very similar format & content across all companies!
• Project analyst inputs formulation details.
– excipients, mass of each individual component used, route of administration, daily intake etc.
• Project analyst selects elements that need to be considered.
• Based on the information provided above the Excel template calculates concentration limits for each element of concern.
– the excel gives the concentration limits for options 1, 2a and 3 for each EI.
• Any known elemental impurity data* for each component is then entered e.g. concentration of Pb in Magnesium Stearate is X ppm.
• Excel then converts that value (in ppm) to a daily intake (in micrograms/day) and compares to the PDE and 30% control threshold.
*data from testing or published literature
implementation

Tools - templated approach to submission of
the risk assessment summary
• Developing a template text for project teams is recommended to drive some level of consistency.
• A typical template text would include the following;
1. a statement that a risk assessment has been completed.
2. list all of the potential sources of EI considered.
3. discuss any potential EI risk originating from manufacturing equipment, utilities, container closure system.
4. test data on key batches of drug substance for any intentionally added elements (reagents / catalysts).
5. discuss whether excipient origin, any test data, database or literature data suggests any risk of EI contamination in the drug product.
6. a reference to any data used that isn’t generated in-house.
7. data generated by testing the drug product for any elements of concern (3 commercial lots or 6 pilot scale lots).
8. analytical technique used to generate any supportive or batch data.
9. statement about key validation criteria used e.g. linearity, accuracy, LOQ.
10. a summary table of key data and a clear statement of any controls required (engineering, specification etc.) for specific EIs.
implementation

Analytical methodology (ICP-MS)
• ICP-MS methodology has been extensively used within
industry.
– generic method has been established aligned with
USP<233>.
– acid digestion (in microwave) is preferred approach to
sample preparation.
– internal Standards with similar ionization potential have
been established for each Q3D element of concern.
– minimum of a 3 point calibration curve established.
– recovery established by use of spiked samples.
implementation

Analytical methodology (ICP-MS)
• FDA Guidance for Industry;
– https://www.fda.gov/media/98847/download
implementation

Excipients – the greatest unknown?
• In 2014 there was very little data available and excipients were considered
to be a significant risk
excipients

Early example of data sharing for excipients*
• Literature (testing has already been done for you) = published
data.
– *Li et al., Journal of Pharmaceutical Sciences, Vol. 104, 4197 - 4206
(2015) - FDA/IPEC/Industry.
– 24 Elements, 205 excipient samples, > 4900 determinations.
– overall low EI levels. Some Pb, Cd, As in mined/marine derived
excipients.
• Data sharing (testing has already been done for you) = published
data.
– mutually beneficial for drug product manufacturers to analyse the EI
content of excipients and pool the data.
excipients
A proactive action from the pharma industry
Facilitate more scientifically driven elemental impurities risk
assessments under ICH Q3D, and reduce unnecessary testing
as part of the elemental impurities risk assessment efforts.
“A database of shared excipient elemental impurity determinations, with
equivalent provenance to published literature”
Elemental Impurities Data Sharing Initiative excipients

The growing consortium
The database and the consortium was established in 2016.

Elemental Impurities Data Sharing Initiative
Independent 3rd party to host and blind data.
- data on excipients NOT suppliers.
Quality is critical.
- standards (“acceptance criteria”) for method validation.
- active data management (outliers etc.)
Relevance.
- sufficient number of relevant excipients.
- data for relevant elements.
- multiple excipient samples, from a range of suppliers.
Data is accessible to industry and regulators
The database contains the results of 2304 analytical studies for 264
excipients.
excipients

Excipient relevance based on 2016 FDA
novel approved drugs list
22 Novel drugs approved in 2016
20 excipients used > once
90% (18 of these 20) have ≥ 3 studies in the database*
https://www.fda.gov/Drugs/DevelopmentApprovalProcess/DrugInnovation/ucm592464.htm
excipients
*value in 2019 is 100%

Excipient relevance based on 2018 FDA
novel approved drug list
49 novel drugs approved in 2018
42 excipients used > once
86% (36 of these 42) have ≥ 3 studies in the database
39 excipients (93%) used > once are covered in the
database
Notes;
1. A list of excipients used in 49 novel drugs was
generated using label information available
through Drugs@FDA service.
2. These comprised of 30 oral, 17 parenteral, 1
topical and 1 inhaled formulation.
3. Water for injection and tablet coatings were not
considered.
https://www.fda.gov/Drugs/DevelopmentApprovalProcess/DrugInnovation/ucm592464.htm
excipients

Elemental impurities excipient database1. Identify all excipients in the drug product
2. Search the database for each excipient
3. Review and export relevant elemental impurity results
Retrieving data from the database is easy! risk assessment
It is easy to export all data required to assess excipient risk in a new
formulation in approximately 10 minutes.
Element
Cmax for
Excipient
1 (ppm)
Cmax for
Excipient
2 (ppm)
Cmax for
Excipient
3 (ppm)
Cmax for
Excipient
4 (ppm)
Cd
Pb
As
Hg
Co
V
Ni
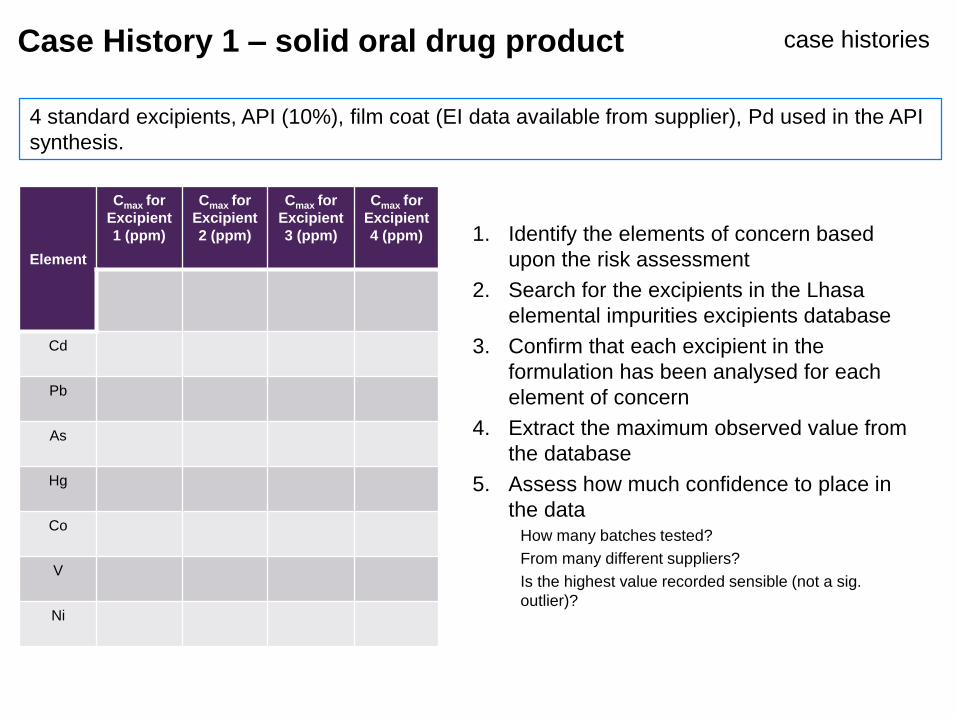
1. Identify the elements of concern based
upon the risk assessment
2. Search for the excipients in the Lhasa
elemental impurities excipients database
3. Confirm that each excipient in the
formulation has been analysed for each
element of concern
4. Extract the maximum observed value from
the database
5. Assess how much confidence to place in
the dataHow many batches tested?
From many different suppliers?
Is the highest value recorded sensible (not a sig.
outlier)?
Case History 1 – solid oral drug product case histories
4 standard excipients, API (10%), film coat (EI data available from supplier), Pd used in the API
synthesis.

Element
Cmax for
Excipient
1 (ppm)
Cmax for
Excipient
2 (ppm)
Cmax for
Excipient
3 (ppm)
Cmax for
Excipient
4 (ppm)
>76 lots
tested
4
suppliers
18 lots
tested
3
suppliers
9 lots
tested
3
suppliers
≥50 lots
tested
4
suppliers
Cd 0.2 0.2 0.2 0.2
Pb 0.2 0.27 0.2 0.2
As 1 1 0.2 1
Hg 0.9 0.2 0.2 0.9
Co 1.5 0.6 0.2 1.5
V 3 10 1 3
Ni 6 22 1 6
µg/day
from
Excipient
1
µg/day
from
Excipient
2
µg/day
from
Excipient
3
µg/day
from
Excipient
4
Calculation based on: 4 x 25mg tablets (approx. 1
g of drug product) and composition of each tablet.
0.115 0.057 0.006 0.002
6. Calculate the maximum Cd
contribution from excipient 1
convert micrograms per gram to grams
per day
7. Repeat for all excipients
8. Repeat for all elements of concern
case histories

Element
Cmax for
Excipient
1 (ppm)
Cmax for
Excipient
2 (ppm)
Cmax for
Excipient
3 (ppm)
Cmax for
Excipient
4 (ppm)
µg/day
from
Excipient
1
µg/day
from
Excipient
2
µg/day
from
Excipient
3
µg/day
from
Excipient
4
µg/day
Film
coat*
Sum
µg/day
%
Oral
PDE
>76 lots
tested
4
suppliers
18 lots
tested
3
suppliers
9 lots
tested
3
suppliers
≥50 lots
tested
4
suppliers
Calculation based on: 4 x 25mg tablets (approx. 1 g of drug
product) and composition of each tablet.
*supplier data used
Cd 0.2 0.2 0.2 0.2 0.115 0.057 0.006 0.002 0.015 0.195 4 %
Pb 0.2 0.27 0.2 0.2 0.115 0.077 0.006 0.002 0.015 0.215 4 %
As 1 1 0.2 1 0.573 0.287 0.006 0.010 0.045 0.921 6 %
Hg 0.9 0.2 0.2 0.9 0.516 0.057 0.006 0.009 0.090 0.678 2 %
Co 1.5 0.6 0.2 1.5 0.860 0.172 0.006 0.015 0.150 1.203 2 %
V 3 10 1 3 1.720 2.867 0.030 0.030 0.300 4.947 5 %
Ni 6 22 1 6 3.440 6.307 0.030 0.060 0.600 10.44 5 %
9. For each element sum the individual contributions across all excipients
10. Compare to the PDE and 30% control threshold
case histories

Element
Cmax for
Excipient
1 (ppm)
Cmax for
Excipient
2 (ppm)
Cmax for
Excipient
3 (ppm)
Cmax for
Excipient
4 (ppm)
µg/day
from
Excipient
1
µg/day
from
Excipient
2
µg/day
from
Excipient
3
µg/day
from
Excipient
4
µg/day
Film
coat*
Sum %
Oral
PDE
>76 lots
tested
4
suppliers
18 lots
tested
3
suppliers
9 lots
tested
3
suppliers
≥50 lots
tested
4
suppliers
Calculation based on: 4 x 25mg tablets (approx. 1 g of drug
product) and composition of each tablet.
*supplier data used
Cd 0.2 0.2 0.2 0.2 0.115 0.057 0.006 0.002 0.015 0.195 4 %
Pb 0.2 0.27 0.2 0.2 0.115 0.077 0.006 0.002 0.015 0.215 4 %
As 1 1 0.2 1 0.573 0.287 0.006 0.010 0.045 0.921 6 %
Hg 0.9 0.2 0.2 0.9 0.516 0.057 0.006 0.009 0.090 0.678 2 %
Co 1.5 0.6 0.2 1.5 0.860 0.172 0.006 0.015 0.150 1.203 2 %
V 3 10 1 3 1.720 2.867 0.030 0.030 0.300 4.947 5 %
Ni 6 22 1 6 3.440 6.307 0.030 0.060 0.600 10.44 5 %
• 9 lots at commercial scale
• All class 1 and 2a elements < 30% of PDE
• Pd used in API synthesis routinely measured at <30% of control threshold in the API
• No specification based controls proposed in the CTD
case historiesTest data on the finished drug substance &
product was also generated

Case History 2 case histories
• Solid oral drug product, < 1g / day intake.
• API loading = 21%.
• The same 4 standard excipients.
– Data available from the Lhasa database for 96, 57, 18 & 9 batches of each excipient for class 1 and 2A elements.
• Film coat (EI data generated was in-house).
• No added catalysts used in the API synthesis.
• All elements of concern are an order of magnitude < 30% control threshold.
• Negligible risk.
– no specification controls required for any elements in either API or DP.
• >10 API lots tested by ICP-MS.
• 4 commercial process DP lots (for each tablet strength) tested by ICP-MS, data supports the conclusion
of the risk assessment.
• No regulatory queries received to date for this CTD submission relating to elemental impurities
• There are multiple similar examples from the past 3 years, with essentially the same
overall risk level.

Conclusions / learnings / outlook.
• Simplify the risk assessment as much as possible, be pragmatic and focussed.
• Supplement the risk assessment with as much data as possible.
– invest and develop ICP SMEs.
– use all available published data / databases.
• Expect questions on the content of your regulatory submissions.
– generally asking for more data and / or detail.
• A good risk assessment will tell a compelling story, the need for controls (or not) should be obvious.
• For solid oral DP using well precedented excipients at <10 gram daily intake then it is very common to not require any DP specification controls.
– it is possible to envisage much more extensive reliance on available data and much less reliance on testing.





























