Embed Size (px)
Citation preview
European Journal of Neurology (1994), 1, 153-157
Impaired colou r discriminat ion in Huntington’s disease Th. Buttner, S. Schulz, W. Kuhn, A. Blumenschein and H. Przuntek
Department of Neurology, Ruhr- University Bochum, St. Jose f-Hospital, Bochum, Germany
Correspondence to: Th. Biittner, Department of Neurology, Ruhr-University Bochum, St. -Josef-Hospital, 0-4479 1 Bochum, GudrunstraBe 56, Germany
Colour discrimination and visual Contrast perception were investigated in 18 patients with Huntington’s disease (HD) and in 18 age- and sex-matched healthy volunteers using the Farnsworth-MunseU 100 Hue test (FM) and stationary contrast targets. The mean total error score (MTES) and the partial scores for the “red-green” and the Ublue-yeUoww axes in the FM of the patients with HD were significantly elevated as compared to controls (MTES in H D 113.0 2 90.8; MTES in controls: 19.2 2 8.8). The spatial contrast sensitivity in HD patients was normal. The colour perception dysfunction indicates that the visual system is affected in HD. The visual disorder may be related to an imbalance of certain neurotransmitters in the visual system of HD patients. Possible anatomical sites of the dysfunction responsible for colour discrimination abnormalities could be the retinal cone system and/or impaired parvocellular central visual pathways in HD.
Keywords: Chromatic vision - Colour discrimination - Contrast sensitivity - Huntington’s disease - Farnsworth-MunseU 100 Hue test
INTRODUCTION
Recently, an impairment of retinal increment thresholds for a blue test light during adaptation to a yellow back- ground was reported in Huntington’s disease (HD) (Pau- lus et ul., 1993). It was concluded that the visual system, especially retinal structures, is involved in the degenera- tive process of the disease. However, the performed col- our vision test which showed pathological results in HD patients is limited to a specific experimental visual con- dition, namely the presentation of a blue stimulus on a yellow background. It remains unclear whether a general defect of chromatic visual perception exists in HD. Fur- thermore, to our knowledge, achromatic contrast vision has never been evaluated in patients with HD. To firther elucidate visual disorders in HD we applied a different experimental procedure by studying colour discrimina- tion and spatial visual contrast sensitivity.
PATIENTS AND METHODS
The study comprised 18 patients with HD, 9 male and 9 female patients with a mean age of 41.1 2 11.5 years (range 24-68 years). The mean duration of the motor symptoms was 5.1 (23.9) years. The diagnosis was established by clinical symptoms, a positive family his- tory and genetic analysis in dl cases. Two individuals
0 1994 Rapid Communications of oxford Ltd
were clinically asymptomatic, but at risk according to family history and with a positive genetic testing. All patients except one were free of neuroleptic medication. One patient received tiapride. In this case the test was performed after a drug-free interval of 12 hours. Exclu- sion criteria were: manifest dementia as defined by the DSM-111-R (American Psychiatric Association, 1987); clinical, electrophysiological or neuroradiological evi- dence of additional CNS pathology exceeding HD; med- ication with digitalis, sedatives or anti-epileptic drugs; and visual disorders, especially distorted visual acuity, glaucoma, retinopathy or inherited dysfbction of chro- matic vision. All patients underwent a complete ophthal- mologic examination, including slit-lamp examination and determination of visual acuity. The visual acuity was better than 0.8 in all patients. Colour vision assessed by pseudo-isochromatic plates (Ishihara plates) was unaffec- ted in all patients.
The colour discrimination was measured in a binocular fashion using the Farnsworth-Munsell 100 Hue test (Farnsworth, 1943). The examinations were performed in a noise-isolated darkened room. The coloured plates ofthe test were illuminated by a daylight Imp (BiolUX, osram, 6500 K). As recommended for patients With neurological disorders, no time limit was applied to the completion of the test. The total error score was deter-
European Journal of Neurology . Vol 1 . 1994 153
TH. BO-~TNER ET AL
mined by a method previously proposed (Vemest et al., 1982). To determine the existence of an axis, the error
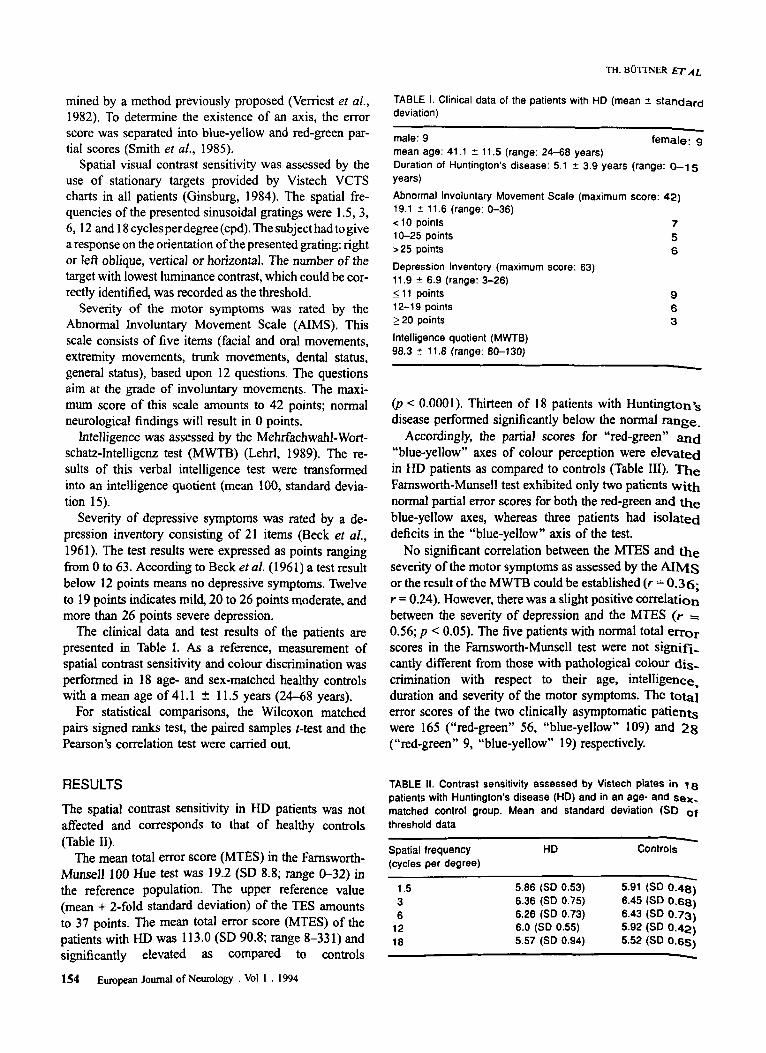
TABLE 1. Clinical data of the patients with HD (mean 2 standard deviation)
score was separated into blue-yellow and red-green par- tial scores (Smith er d, 1985).
Spatial visual contrast sensitivity was assessed by the use of stationary targets provided by Vistech VCTS charts in all patients (Ginsburg, 1984). The spatial fre- quencies of the presented sinusoidal gratings were 1.5,3, 6,12 and 18 cycles perdegree (cpd). The subject had to give a response on the orientation of the presented grating: right or left oblique, vertica) or horizontal. The number of the target with lowest luminance contrast, which could be cor- rectly identified, was recorded as the threshold.
Severity of the motor symptoms was rated by the Abnormal lnvoluntary Movement Scale (AIMS). This scale consists of five items (facial and oral movements, extremity movements, trunk movements, dental status, general status), based upon 12 questions. The questions aim at the grade of involuntary movements. The maxi- mum score of this scale amounts to 42 points; normal neurological findings will result in 0 points.
Intelligence was assessed by the Mehrfachwahl-Wort- schatz-Intelligenz test (MWTB) (Lehrl, 1989). The re- sults of this verbal intelligence test were transformed into an intelligence quotient (mean 100, standard devia- tion 15).
Severity of depressive symptoms was rated by a de- pression inventory consisting of 21 items (Beck et al., 1961). The test results were expressed as points ranging from 0 to 63. According to Beck er al. (1961) a test result below 12 points means no depressive symptoms. Twelve to 19 points indicates mild, 20 to 26 points moderate, and more than 26 points severe depression.
The clinical data and test results of the patients are presented in Table I. As a reference, measurement of spatial contrast sensitivity and colour discrimination was performed in 18 age- and sex-matched healthy controls with a mean age of 41.1 2 11.5 years (24-68 years).
For statistical comparisons, the Wilcoxon matched pairs signed ranks test, the paired samples t-test and the Pearson’s correlation test were carried out.
male: 9 female: 9 mean age: 41.1 2 11.5 (range: 24-68 years) Duration of Huntington’s disease: 5.1 t 3.9 years (range: 0-1 5 years)
Abnormal Involuntary Movement Scale (maximum score: 42) 19.1 2 11.6 (range: 0-36) < 10 points 7
5 10-25 points >25 points 6 Depression Inventory (maximum score: 63) 11.9 5 6.9 (range: 3-26) 5 1 1 points 9 12-19 points 6 220 points 3 Intelligence quotient ( M M B ) 98.3 2 11.8 (range: 80-130)
(p < 0.0001). Thirteen of 18 patients with Huntington*s disease performed significantly below the normal mge-
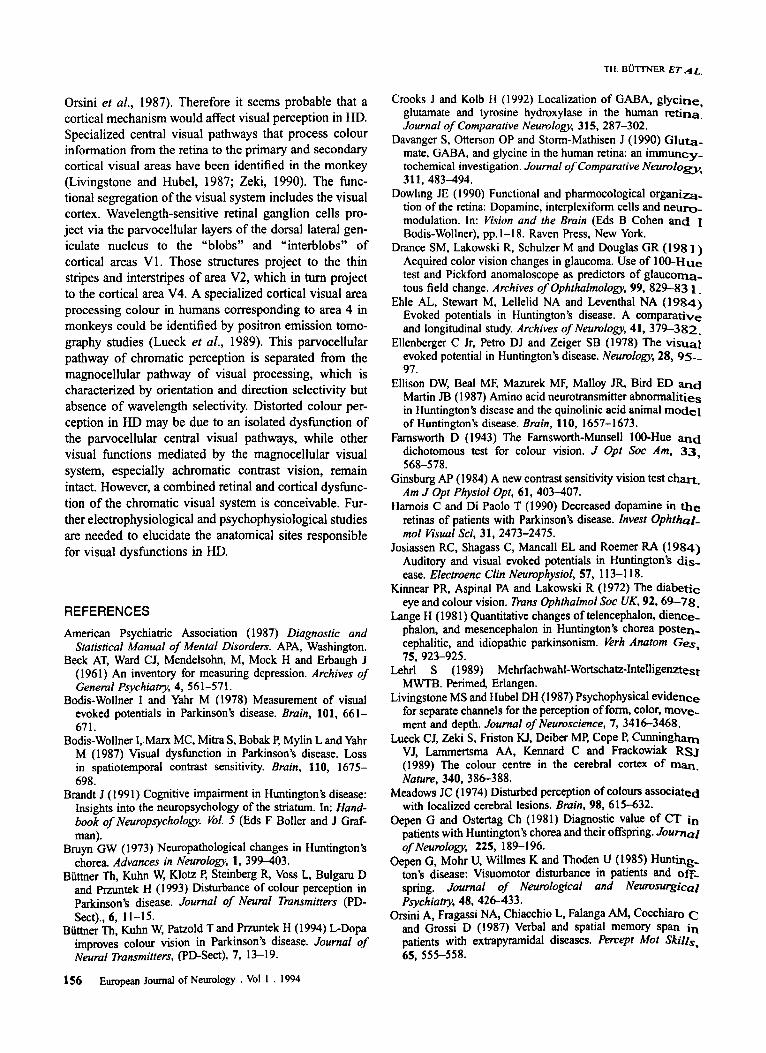
Accordingly, the partial scores for “red-green’’ a d “blue-yellow” axes of colour perception were elevated in HD patients as compared to controls (Table 111). The Famsworth-Munsell test exhibited only two patients with normal partial error scores for both the red-green and the blue-yellow axes, whereas three patients had isolated deficits in the “blue-yellow” axis of the test.
No significant correlation between the MTES and the severity of the motor symptoms as assessed by the AIMS or the result of the MWTB could be established (r = 0.36; r = 0.24). However, there was a slight positive correlation between the severity of depression and the MTES (r = 0.56; p < 0.05). The five patients with normal total error scores in the Famsworth-Munsell test were not signifi- cantly different fiom those with pathological colour dis- crimination with respect to their age, intelligence, duration and severity of the motor symptoms. The total error scores of the two clinically asymptomatic patients were 165 (“red-green’’ 56, “blue-yellow” 109) and 28 (“red-green” 9, “blue-yellow’’ 19) respectively.
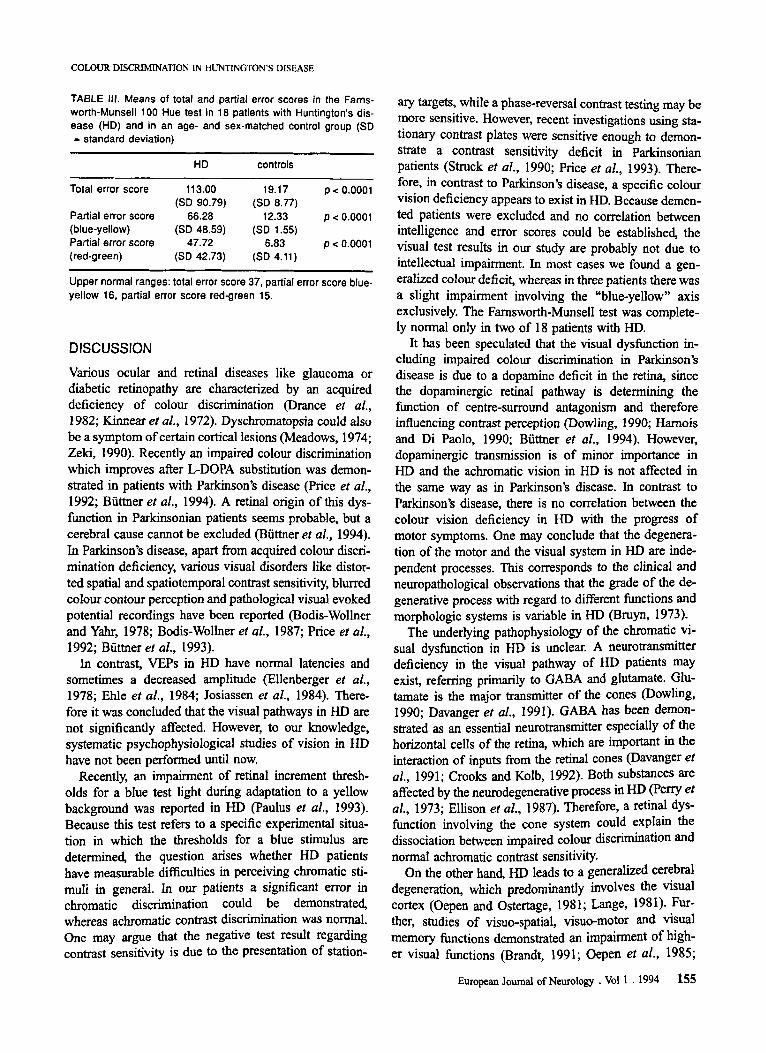
RESULTS The spatial contrast sensitivity in HD patients was not affected and corresponds to that of healthy controls
TABLE ti. Contrast sensitivity assessed by Vistech plates in 18 patients with Huntington’s disease (HD) and in an age- and sex- matched control group. Mean and standard deviation (SD of threshold data - Spatial frequency HD Controls (cycles per degree)
(Table 11). The mean total error score (MTES) in the Farnsworth-
Munsell 100 Hue test was 19.2 (SD 8.8; range 0-32) in the reference population. The upper reference value 1.5 5.86 (SD 0.53) 5.91 (SD 0.48)
(mean + 2-fold standard deviation) of the TES amounts 6.36 (SD 0.75) 6.45 (SD 0.68) 6 6.26 (SD 0.73) 6.43 (SD 0.73)
to 37 points. The mean total error score (MTES) of the 6.0 (SD 0.55) 5.92 (SD 0.42) patients with HD W ~ S 113.0 (SD 90.8; range 8-331) and 5.57 (SD 0.94) 5.52 (SD 0.65)
,2 18
significantly elevated as compared to controls - 154 European Journal of Neurology . VOI 1 . 1994
COLOUR DISCRIMINATION IN HUNTINGTON’S DISEASE
TABLE 111. Means of total and partial error scores in the Farns- worth-Munsell 100 Hue test in 18 patients with Huntington’s dis- ease (HD) and in an age- and sex-matched control group (SD = standard deviation)
~
HD controls
Total error score 11 3.00 19.17 p < 0.0001
Partial error score 66.28 12.33 p < 0.0001
Partial error score 47.72 6.83 p < 0.0001
(SD 90.79) (SD 8.77)
(blue-yellow) (SD 48.59) (SD 1.55)
(red-green) (SD 42.73) (SD 4.11)
Upper normal ranges: total error score 37, partial error score blue- yellow 16, partial error score red-green 15.
DISCUSSION Various ocular and retinal diseases like glaucoma or diabetic retinopathy are characterized by an acquired deficiency of colour discrimination (Drance et al., 1 982; Kinnear ef al., 1972). Dyschromatopsia could also be a symptom of certain cortical lesions (Meadows, 1974; Zeki, 1990). Recently an impaired colour discrimination which improves after L-DOPA substitution was demon- strated in patients with Parkinson’s disease (Price et al., 1992; Buttner et al., 1994). A retinal origin of this dys- function in Parkinsonian patients seems probable, but a cerebral cause cannot be excluded (Biittner ef al., 1994). In Parkinson’s disease, apart from acquired colour discri- mination deficiency, various visual disorders like distor- ted spatial and spatiotemporal contrast sensitivity, blurred colour contour perception and pathological visual evoked potential recordings have been reported (Bodis-Wollner and Yahr, 1978; Bodis-Wollner et al., 1987; Price et al., 1992; Btittner et al., 1993).
In contrast, VEPs in HD have normal latencies and sometimes a decreased amplitude (Ellenberger et al., 1978; Ehle et al., 1984; Josiassen et al., 1984). There- fore it was concluded that the visual pathways in HD are not significantly affected. However, to our knowledge, systematic psychophysiological studies of vision in HD have not been performed until now.
Recently, an impairment of retinal increment thresh- olds for a blue test light during adaptation to a yellow background was reported in HD (Paulus et al., 1993). Because this test refers to a specific experimental situa- tion in which the thresholds for a blue stimulus are determined, the question arises whether HD patients have measurable difficulties in perceiving chromatic Sti-
muli in general. our patients a significant error in chromatic discrimination could be demonstrated, whereas achromatic contrast discrimination was normal. one may argue that the negative test result regarding contrast sensitivity is due to the presentation of station-
arY targets, while a phase-reversal contrast testing may be more sensitive. However, recent investigations using ~ t a - tionW contrast Plates were sensitive enough to demon- strate a contrast sensitivity deficit in Parkinsonian Patients (Struck ef al., 1990; Price et al., 1993). There- fore, in contrast to Parkinson’s disease, a specific colour vision deficiency appears to exist in HD. Because demen- ted patients were excluded and no correlation between intelligence and error scores could be established, the visual test results in our study are probably not due to intellectual impairment. In most cases we found a gen- eralized colour deficit, whereas in three patients there was a slight impairment involving the “blue-yellow” axis exclusively. The Farnsworth-Munsell test was complete- ly normal only in two of 18 patients with HD.
It has been speculated that the visual dysfunction in- cluding impaired colour discrimination in Parkinson’s disease is due to a dopamine deficit in the retina, since the dopaminergic retinal pathway is determining the function of centre-surround antagonism and therefore influencing contrast perception (Dowling, 1 990; Hamois and Di Paolo, 1990; Biittner et al., 1994). However, dopaminergic transmission is of minor importance in HD and the achromatic vision in HD is not affected in the same way as in Parkinson’s disease. In contrast to Parkinson’s disease, there is no correlation between the colour vision deficiency in HD with the progress of motor symptoms. One may conclude that the degenera- tion of the motor and the visual system in HD are inde- pendent processes. This corresponds to the clinical and neuropathological observations that the grade of the de- generative process with regard to different functions and morphologic systems is variable in HD (Br~f l , 1973).
The underlying pathophysiology of the chromatic vi- sual dysfunction in HD is unclear. A neumtransmitter deficiency in the visual pathway of HD patients W Y exist, referring primarily to GABA and glutamate. Glu- tamate is the major transmitter of the cones @owling, 1990; Davanger et al., 1991). GABA has been demon- strated as an essential neurotransmitter especially of the horizontal cells of the retina, which are important in the interaction of inputs from the retinal cones (Davanger et al., 1991; Crooks and Kolb, 1992). Both substances are affected by the neurodegenerative process in HD (Pew et al., 1973; Ellison et al., 1987). Therefore, a r h ~ ~ l dYs- function involving the cone system could explain the dissociation between impaired CO~OUI discrimination and normal achromatic contrast sensitivity.
On the other hand, HD leads to a generalized Cerebral degeneration, which predominantly involves the Visual cortex (Oepen and Ostertage, 1981; Lange, 1981). Fur- ther, studies of visuo-spatial, visuo-motor and Visual memory functions demonstrated an impairment of high- er visual functions (Brandt, 1991; Oepen et al., 1985;
European Journal of Neurology . Vol 1 . 1994 155
Orsini et al., 1987). Therefore it seems probable that a cortical mechanism would affect visual perception in HD. Specialized central visual pathways that process colour information from the retina to the primary and secondary cortical visual areas have been identified in the monkey (Livingstone and Hubel, 1987; Zeki, 1990). The func- tional segregation of the visual system includes the visual cortex. Wavelength-sensitive retinal ganglion cells pro- ject via the parvocellular layers of the dorsal lateral gen- iculate nucleus to the “blobs” and “interblobs” of cortical areas V1. Those structures project to the thin stripes and interstripes of area V2, which in turn project to the cortical area V4. A specialized cortical visual area processing colour in humans corresponding to area 4 in monkeys could be identified by positron emission tomo- graphy studies (Lueck et al., 1989). This parvocellular pathway of chromatic perception is separated from the magnocellular pathway of visual processing, which is characterized by orientation and direction selectivity but absence of wavelength selectivity. Distorted colour per- ception in HD may be due to an isolated dysfunction of the parvocellular central visual pathways, while other visual functions mediated by the magnocellular visual system, especially achromatic contrast vision, remain intact. However, a combined retinal and cortical dysfunc- tion of the chromatic visual system is conceivable. Fur- ther electrophysiological and psychophysiological studies are needed to elucidate the anatomical sites responsible for visual dyshc t ions in HD.
REFERENCES American Psychiatric Association (1 987) Diagnostic and
Statistical Manual of Mental Disorders. APA, Washington. Beck AT, Ward CJ, Mendelsohn, M, Mock H and Erbaugh J
(1961) An inventory for measuring depression. Archives of General Psychiaw, 4,561-571.
Bodis-Wollner I and Yahr M (1978) Measurement of visual evoked potentials in Parkinson’s disease. Bmin, 101, 661- 671.
Bodis-Wollner I,.Marx MC, Mitra S, Bobak P, Mylin L and Yahr M (1987) Visual dysfunction in Parkinson’s disease. Loss in spatiotemporal contrast sensitivity. Brain, 110, 1675- 698.
Brandt J (1991) Cognitive impairment in Huntington’s disease: Insights into the neuropsychology of the striatum. In: Hand- book ojNeuropsychology. Val. 5 (Eds F Boller and J Graf- man).
BIUJTI GW (1 973) Neuropathological changes in Huntington’s chorea. Advances in Neurology, 1, 399403.
Burner Th, Kuhn W, Klotz P, Steinberg R, Voss L, Bulgam D a d m t e k H (1993) Disturbance of colour perception in Parkinson’s disease. Journal of Neural Tmnsmitters (PD- Sect)., 6, 11-15.
Burner Th, Kuhn W, Patzold T and Prmntek H (1 994) L-Dopa improves colour vision in Parkinson’s disease. Journal of Neural Tmnsmitters, (PD-Sect), 7, 13-19.
156 European Journal of Neurology . vol 1 . 1994
Crooks J and Kolb H (1992) Localization of GABA, glycine, glutamate and tyrosine hydroxylase in the human retina. Journal of Comparative Neurology, 3 15, 287-302.
Davanger S, Otterson OP and Storm-Mathisen J (1990) G l u u - mate, GABA, and glycine in the human retina: an immuncy- tochemical investigation. Journal of Comparative NeumIoe , 311, 483-494.
Dowling JE ( 1 990) Functional and pharmocological organim- tion of the retina: Dopamine, interplexiform cells and n e m - modulation. In: Vision and the Brain (Eds B Cohen and I Bodis-Wollner), pp. 1-1 8. Raven Press, New York.
Acquired color vision changes in glaucoma. Use of 1 0 0 - H ~ ~ test and Pickford anomaloscope as predictors of glaucoma- tous field change. Archives of Ophfhalmology, 99, 829-83 1.
Ehle AL, Stewart M, Lellelid NA and Leventhal NA (1984) Evoked potentials in Huntington’s disease. A comparative and longitudinal study. Archives of Neurology, 41, 379-382-
Ellenberger C Jr, Petro DJ and Zeiger SB (1978) The visual evoked potential in Huntington’s disease. Neurology, 28, 95- 97.
Ellison DW, Beal MF, Mazurek MF, Malloy JR, Bird ED and Martin JB (1987) Amino acid neurotransmitter abnormalities in Huntington’s disease and the quinolinic acid animal model of Huntington’s disease. Brain, 110, 1657-1673.
Famsworth D (1943) The Famsworth-Munsell 100-Hue and dichotomous test for colour vision. J Opt SOC Am, 33,
Ginsburg AP (1984) A new contrast sensitivity vision test chart. Am J Opt Physiol Opt, 61, 403-407.
Hamois C and Di Paolo T (1 990) Decreased dopamine in the retinas of patients with Parkinson’s disease. Invest Ophthal- mol Visual Sci, 31, 2473-2475.
Josiassen RC, Shagass C, Mancall EL and Roemer RA (1984) Auditory and visual evoked potentials in Huntington’s dis- ease. Electmenc Clin Neurophysiol, 57, 1 13-1 18.
Kinnear PR, Aspinal PA and Lakowski R (1972) The diabetic eye and colour vision. Tmns Ophthalmol Soc UK, 92,6%78.
Lange H (1981) Quantitative changes of telencephalon, dience- phalon, and mesencephalon in Huntington’s chorea posten- cephalitic, and idiopathic parkinsonism. Yerh Anatom G e ,
Lehrl S (1 989) Mehrfachwahl-Wortschatz-Intelligemst MWTB. Perimed, Erlangen.
Livingstone MS and Hubel DH (1987) Psychophysical evidence for separate channels for the perception of form, color, move- ment and depth. Journal of Neuroscience, 7, 34163468.
Lueck CJ, Zeki S, Friston KJ, Deiber MP, Cope P, Cunningham VJ, Lammertsma AA, Kennard C and Frackowiak R S j (1989) The colour centre in the cerebral cortex of m a . Nature, 340,386388.
Meadows JC (1 974) Disturbed perception of colours associated with localized cerebral lesions. Bmin, 98, 615-632.
Oepen G and Ostertag Ch (1981) Diagnostic value of CT in patients with Huntington’s chorea and their offspring. Journal
Oepen G, Mohr U, Willmes K and Thoden U (1985) Hunting- ton’s disease: Visuomotor disturbance in patients and off- spring. Journal of Neurological and Neurosurgical Psychiahy, 48, 426-433.
Orsini A, Fragassi NA, Chiacchio L, Falanga AM, Cocchiaro c and Grossi D (1987) Verbal and spatial memory span in patients with extrapyramidal diseases. Percepf Mot Ski&,
Drance SM, Lakowski R, Schulzer M and Douglas GR (198 1
568-578.
75,923-925.
of Neurology, 225, 189-196.
65, 555-558.

COLOUR DISCRlMINATION IN HUNTINGTON’S DISEASE
Paulus W, Schwarz G, Werner A, Lange H, Bayer A, Hofschus- ter M, Miiller N and Zrenner E (1 993) Impairment of retinal increment thresholds in Huntington’s disease. Annals of Neu- rology, 34, 574-518.
Perry TL, Hansen S and Kloster M (1973) Huntington’s chorea: deficiency of gamma-aminobutytnc acid in brain. New Eng- land Journal of Medicine, 288, 337-342.
Price MJ, Feldman RG, Adelberg D and Kayne H (1992) Abnormalities in color vision and contrast sensitivity in Parkinson’s disease. Ne~rology, 42, 887-890.
Smith VC, Pokorny J and Pass AS (1985) Color-axis determi- nation on the Famsworth-Munsell 100-Hue test. American Journal of Ophthalmology, 100, 176-82.
Struck LK, Rodnitzky RL and Dobson JK (1990) Circadian fluctuations of contrast sensitivity in Parkinson’s disease. Neudogy, 40,467470.
Verriest G, van Laethem J and Uvijls A (1982) A new assess- ment of the normal ranges of the Farnsworth-Munsell 100- Hue test scores. American Journal of Ophthalmology, 93, 635-642.
Zeki S (1990) A century of cerebral achromatopsia. Brnin, 113, 1721-1 777.
(Received 8 June 1994; accepted as revised 9 September 1994)
European Journal of Nembgy , Vol 1 . 1994 157





























