Embed Size (px)
Citation preview

IMPACTS OF PHARMACIST’S ROLES ON REDUCING READMISSION RATE AND PROMOTING PATIENT SAFETY
IN PEDIATRIC CARDIAC PATIENTSManita Suriyarangsee
Monwarat Laohajeeraphan
Vimonkarn Sirisuksan
Pharmacy Department, Siriraj Hospital, Mahidol University, Thailand
Introduction
Objective To study the characteristics of drug-related problems (DRPs)
throughout discharge counseling and medication reconciliation process and its impacts on readmission rate and patient safety.
Long term treatment
Many drugs need to be taken around the clock several
times/day
Many cardiovascular
drugs are categorized as high
alert drugs
Prevention of medication errors which will result in harm to patients encourage patients & caregiver to
achieve the goal of treatment
Poor adherence
Pediatric cardiac patientsPediatric cardiac patients
Setting 14 beds pediatric cardiac ward in Siriraj Hospital that is the 2,300
beds tertiary-care teaching hospital of Mahidol University, Thailand.
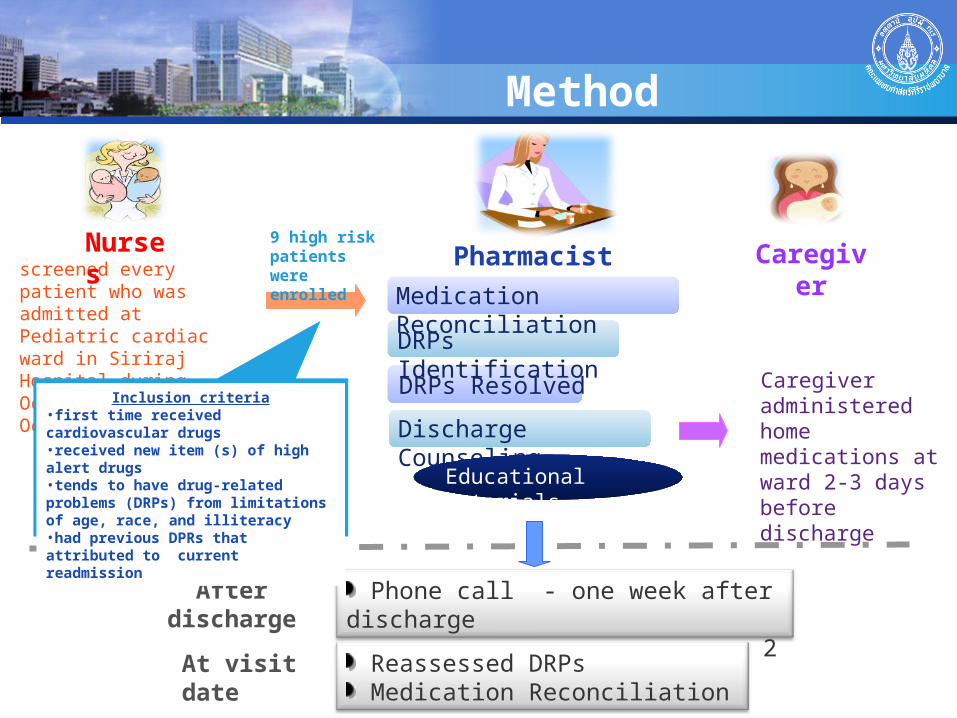
screened every patient who was admitted at Pediatric cardiac ward in Siriraj Hospital during October, 2009 to October, 2010
Method
Caregiver administered home medications at ward 2-3 days before discharge
Pharmacist Caregiver
After discharge
Nurses
Medication Reconciliation
DRPs Identification
DRPs Resolved
Discharge Counseling
Educational Materials
Phone call - one week after discharge - every 2 weeks or more
At visit date Reassessed DRPs Medication Reconciliation
9 high risk patients were enrolled
Inclusion criteria•first time received cardiovascular drugs•received new item (s) of high alert drugs•tends to have drug-related problems (DRPs) from limitations of age, race, and illiteracy •had previous DPRs that attributed to current readmission

Educational MaterialsTo be used in poor adherence and low health literacy patients or caregivers
Poor adherence
Many items of home medication
Complicate administration time
Unable to read drug names in English
Unable to understand drug labels
Cannot read syringe scale
Home medication schedules indicate type, time and administration method in each home medication items.
In addition of cartoon sticker, they’ll be scaled the prescribed volume with red-line sticker
Red-line sticker
Cartoon sticker
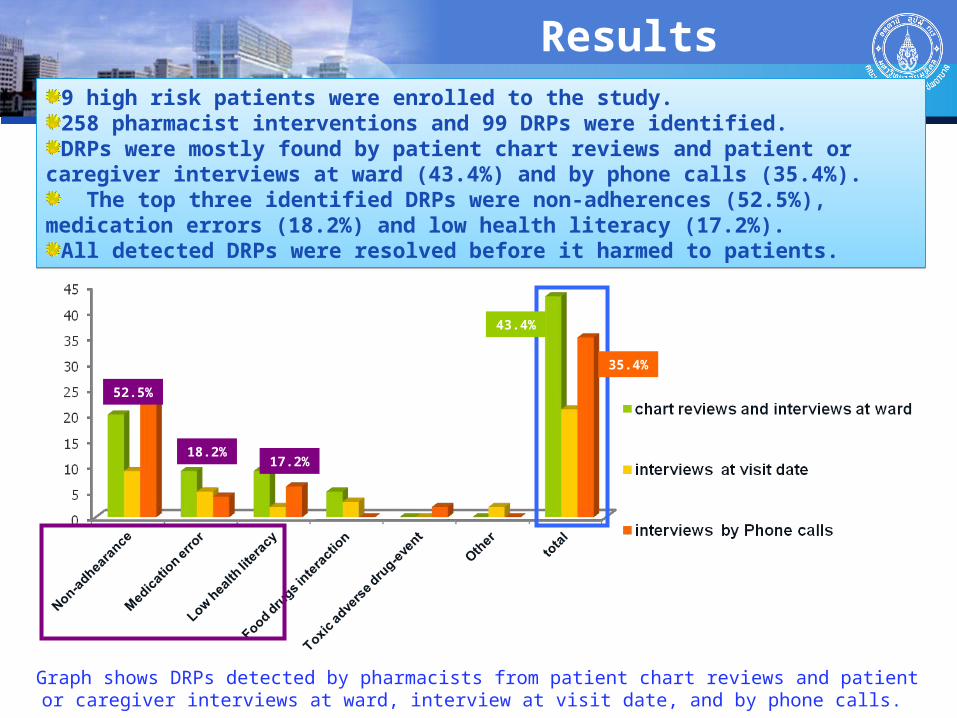
Results9 high risk patients were enrolled to the study.258 pharmacist interventions and 99 DRPs were identified.DRPs were mostly found by patient chart reviews and patient or caregiver interviews
at ward (43.4%) and by phone calls (35.4%). The top three identified DRPs were non-adherences (52.5%), medication errors
(18.2%) and low health literacy (17.2%).All detected DRPs were resolved before it harmed to patients.
9 high risk patients were enrolled to the study.258 pharmacist interventions and 99 DRPs were identified.DRPs were mostly found by patient chart reviews and patient or caregiver interviews
at ward (43.4%) and by phone calls (35.4%). The top three identified DRPs were non-adherences (52.5%), medication errors
(18.2%) and low health literacy (17.2%).All detected DRPs were resolved before it harmed to patients.
Graph shows DRPs detected by pharmacists from patient chart reviews and patient or caregiver interviews at ward, interview at visit date, and by phone calls.
43.4%
35.4%
52.5%
18.2%17.2%
Conclusion
• The pharmacist’s interventions could prevent DRPs that lead to readmission from non-adherences, medication errors and low health literacy.
• Early DRPs detection and resolving (by patient or caregiver interviews and phone calls) could generate more patient safety in vulnerable chronic disease patients.
What key lessons can we learn from your work?
“Drugs don’t work in patients who don’t take them1”, so it’s one of the pharmacist’s role to improve medication adherence in order to achieve treatment goals that lead to reduce readmission from poor adherence.
Continuous follow up with patients or caregivers by telephone after discharge will assure patient understanding on pharmacist’s counseling and DRPs will be promptly detected and resolved prior to causing any harms to patients.
Medication reconciliation is an important tool to reduce medication errors and ensure patient safety.
Patient’s participation in their therapeutic regimen is one of the success strategies for improving adherence.
1: C. Everett Koop, M.D.
Implementing policies and programs to improve the use of medicines
In short term Provide home medication schedule in every patient Medication reconciliation would be implemented to
promote patient safety. Provide discharge counseling by pharmacist in high risk
patients
In long term Establish pediatric cardiac care team which collaborate
with multidisciplinary experts to provide holistic care
Specific studies should be included in a future research agenda
Cost effectiveness studies of pharmacist interventions on reducing readmission rate and promoting patient safety
Pharmacist interventions on promoting patient safety in other chronic diseases

for your attention





























