-
Impact of Data Presentation on Physician Performance Utilizing
ArtificialIntelligence-Based Computer-Aided Diagnosis and
DecisionSupport Systems
L. Barinov1,2,3 & A. Jairaj1 & M. Becker3,4 & S
Seymour1 & E. Lee3,4 & A. Schram3,4 & E. Lane4 & A.
Goldszal3,4 & D. Quigley4 &L. Paster3,4
Published online: 15 October 2018# The Author(s) 2018
AbstractUltrasound (US) is a valuable imaging modality used to
detect primary breast malignancy. However, radiologists have a
limitedability to distinguish between benign and malignant lesions
on US, leading to false-positive and false-negative results,
whichlimit the positive predictive value of lesions sent for biopsy
(PPV3) and specificity. A recent study demonstrated that
incorpo-rating an AI-based decision support (DS) system into US
image analysis could help improve US diagnostic performance.
Whilethe DS system is promising, its efficacy in terms of its
impact also needs to be measured when integrated into existing
clinicalworkflows. The current study evaluates workflow schemas for
DS integration and its impact on diagnostic accuracy. The impacton
two different reading methodologies, sequential and independent,
was assessed. This study demonstrates significant
accuracydifferences between the two workflow schemas as measured by
area under the receiver operating curve (AUC), as well as
inter-operator variability differences as measured by Kendall’s
tau-b. This evaluation has practical implications on the
utilization ofsuch technologies in diagnostic environments as
compared to previous studies.
Keywords Breast cancer . Machine learning . Artificial
intelligence . Clinical workflow . Computer-aided diagnosis (CAD)
.
Decision support
Introduction
Excluding skin cancer, breast cancer has the highest
incidencerate and the second highest mortality rate in women [1].
Earlyand accurate diagnosis is a cornerstone strategy used
tominimizebreast malignancy, morbidity, and mortality. Imaging
plays acentral role in diagnosis; specifically, digital
mammography/tomosynthesis and ultrasound are the most frequently
usedscreening and diagnostic modalities. In current imaging
proto-cols, ultrasound (US) is a valuable tool for evaluating
breasttissue, achieving sensitivity comparable to digital
mammography(DM) and improved detection of invasive and
node-negative
breast cancers [2]. This improvement, however, comes at the
costof lower PPV3 and specificity [3]. In practice, the increased
false-positive rate manifests as an increase in benign
biopsies.
One avenue being explored to address these concerns is
theintroduction ofmachine learning-based artificial intelligence
(AI)systems. While these systems have been utilized in the past
formammography, their benefits have been recently called
intoquestion [4]. Additionally, rather than aiding in diagnosis,
thesesystems have traditionally been used as an aid for the
detection ofsuspicious areas [5–7]. This approach has been
replicated inautomated whole breast ultrasound (ABUS) but is only
clearedto target areas not known to have suspicious findings
[8].
More recently, tools have been developed to aid the
diagnosticperformance of radiologists, offering automated
assessments oflesion characteristics and risk. Initial iterations
have demonstrateda meaningful increase in sensitivity but a large
decrease in spec-ificity [4]. As machine learning techniques have
progressed overthe last 6 years, however, advances in performance
within thediagnostic ultrasound space have followed suit.
A recent study demonstrated that integration of US with anew
AI-based decision support (DS) system offers substantialimprovement
in both sensitivity and specificity. When tested
* L. [email protected]
1 Koios Medical, New York, NY, USA2 Princeton University,
Princeton, NJ, USA3 Rutgers University Robert Wood Johnson Medical
School, New
Brunswick, NJ, USA4 University Radiology Group, East Brunswick,
NJ, USA
Journal of Digital Imaging (2019)
32:408–416https://doi.org/10.1007/s10278-018-0132-5
http://crossmark.crossref.org/dialog/?doi=10.1007/s10278-018-0132-5&domain=pdfmailto:[email protected]
-
alone, the DS platform was shown to exceed radiologist
perfor-mance in US data analysis, showing a 34–55% potential
reduc-tion in benign biopsies and an increase in the positive
predictivevalue of lesions sent for biopsy (PPV3) of 7–20% [9].
While the system’s raw performance is promising, DS’spractical
efficacy and impact also need to be assessed whenintegrated into
existing real-world clinical workflows. Thisstudy investigates the
clinical impact of two different diagnos-tic workflows. Clinical
impact is evaluated as a function ofhow diagnostic support is
presented. Presentation can eitherbe sequential, where the
clinician has an initial opportunity toevaluate the case unaided
before receiving DS, or indepen-dent, where the case and decision
support are presented to-gether. Stand-alone clinician accuracy is
compared to that of aclinician utilizing DS, and the system’s
impact on intra-operator and inter-operator variability is
evaluated. The goalof this study is to evaluate workflow schemas
for DS integra-tion and their effects on diagnostic accuracy.
Methods
Data Collection
Using data acquired from the ACRIN 6666 trial [10], 500cases
were identified for inclusion. Lesion population statis-tics can be
seen in Fig. 1. The dataset was enriched for
malignancy, while all other statistics were chosen to
approxi-mate current population numbers per the Breast
CancerResearch Foundation (BCRF) [10]. All pathological groundtruth
for malignant lesions came from biopsy-proven patho-logical
follow-up, while for benign lesions, ground truth wasestablished
via biopsy or 1 year follow-up if the lesions wereBI-RADS 4 and
above or BI-RADS 3 and below, respectively.This dataset includes
images obtained using a diverse set ofUS equipment and a range of
high-frequency breast transduc-ers (Fig. 2). Overall, this
equipment and the lesion evaluatedin the dataset accurately
represent current clinical practice in-cluding inclusion of cases
from both academic and non-academic sites as well as dedicated
breast and non-dedicatedimaging centers [10].
Machine Learning
Utilizing original radiologist-designated regions of
interest(ROI), two orthogonal views of each lesion were used to
gen-erate a machine learning system-based score [9]. These ROIswere
selected by the radiologist who had originally read thecase
clinically. The score ranges from 0.0 to 1.0 and issubdivided into
four categories, each representing a clinicalcourse of action
(Table 1).
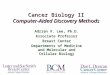
These scores were presented to all study readers in agraphical
form in the electronic Case Report Form (eCRF)(Fig. 3).
a b c
d e f
Fig. 1 Lesion population statistics. a Tumor size. b Tumor
grade. c Benign or malignant. dDCIS (non-invasive) vs invasive. e
Lymph node status. f BI-RADS designation for the three radiologists
tested
J Digit Imaging (2019) 32:408–416 409
-
Reader Characteristics and Training
ThreeAmericanBoard ofRadiology (ABR) certified
radiologists,training and experience summarized in Table 2,
evaluated the 500case dataset. Each radiologist was initially given
a 30-min trainingsession to understand the machine learning output,
stand-aloneperformance of the system, and the eCRF form. After
training,each radiologist demonstrated proper utilization of the
study plat-form by assessing 10 test cases proctored by the
training staff.
Each reader specializes in breast imaging and performs amix of
screening and diagnostic breast imaging across multi-ple
modalities.
Reader Workflow
Cases were presented to and scored by radiologists in a
singlesoftware environment that showed orthogonal images, ROIs,and
theDS output. The study platform then queried the radiologistto
input a Breast Imaging Reporting andData System (BI-RADS)score (the
current clinical systemused to evaluate lesion suspicion)and
likelihood of malignancy (LoM) as a percentage (Fig. 3).
Using this software, the readers reviewed ultrasound imagesusing
two separate workflows which are summarized in Fig. 4:
Sequential workflow
1. Readers reviewed the case without the DS output (con-trol
read)
Fig. 2 Ultrasound equipmentcharacteristics. a Manufacturer.
bTransducer frequency. Bn/a^refers to cases in which UStransducer
frequency was notrecorded
Table 1 Score ranges and their corresponding categorical
outputs.These ranges and categories are inherent to the system and
were notdesigned or altered for this study
Categorical output Score range
Benign [0, 0.25)Probably benign [0.25, 0.5)Suspicious [0.5,
0.75)Malignant [0.75 1.0]
410 J Digit Imaging (2019) 32:408–416
-
2. Readers scored the case via BI-RADS and LoM3. DS output was
presented to the readers4. Readers re-scored the case via BI-RADS
and LoM
Independent Workflow
This workflow was employed after a 4-week Bwashout^ peri-od that
followed the sequential workflow. After this washoutperiod, readers
where shown the images and the DS output,and they scored the case.
In the independent workflow, readerswere presented with 450 cases
in randomized order. Fiftycases were withheld and reserved as
control cases in order tomeasure intra-reader variability after the
4-week washout pe-riod. This workflow is summarized in the
following sequence:
Readers were presented with one of the following:
1. Control case read with no DS output (50 Total)
(a) Readers scored the case via BI-RADS and LoMOR
2. A case containing DS output (450 Total)
(b) Readers scored the case via BI-RADS and LoM
System Evaluation
Radiologists were presented with DS output that used theoriginal
ROIs selected during clinical evaluation of the cases.This choice
was made to enhance reader efficiency so that ahigh volume of cases
could be evaluated in a practical timeframe. However, while it is
felt that the ROI a radiologistchooses manually would be very
similar to the ROI used inthis study, it is possible that results
would be impacted thevariation caused by manually demarcated ROIs.
To evaluatethe system’s robustness to variation in the ROI
boundaries,two assessments were performed.
First, DS output’s robustness to ROI boundary variationwas
assessed by evaluating the 500 cases 20 times, randomlyvarying the
ROI boundary each time. Specifically, each cornerof the region was
shifted at random by up to 20% in eachdimension from the
predetermined optimal cropping. ROCcurves and the AUC distributions
were calculated.
Second, the boundaries between BI-RADS 3 ProbablyBenign (P) and
BI-RADS 4a Suspicious (S) represents themost clinically impactful
diagnostic decision point. It is
Fig. 3 Screen capture of the study platform. The left side shows
two orthogonal views with ROIs. On the right side is the DS output
and the radiologistcase assessment input (BI-RADS assessment and
likelihood of malignancy percentage)
Table 2 This table provides a summary of the three readers
involved inthis study
Radiologist ID Post-educational trainingexperience (years)
ABRcertified
Breast fellowshiptraining
1 20+ x x
2 10+ x x
3 5+ x
J Digit Imaging (2019) 32:408–416 411
-
critical to understand the effects of ROI variability on
classswitching across categories, and specifically the P-S
bound-ary. Since the system’s output is categorical, changes
acrossthis decision boundary have the potential to change
clinicalmanagement. The level of class switching due to ROI
sensi-tivity was evaluated by utilizing the 20 ROIs generated in
theprevious analysis and counting the number of times
categoryswitching is observed compared to the initial radiologist
sup-plied cropping.
Finally, in order to verify the relationship between the
sys-tem’s categorical output and BI-RADS, a sensitivity and
spec-ificity analysis was conducted. For each categorical group,
thesensitivity and specificity values were compared between
thesystem and each participating reader’s BI-RADS assessment.
Reader Evaluation
The area under the receiver operating curve (AUC) for
eachradiologist across each reading paradigm was calculated
andcompared to their control reads. The estimate of the change
inAUC as well as the 95% confidence intervals was made byusing the
Dorfman-Berbaum-Metz method of MRMC analy-sis using the Metz-ROC
LABMRMC software [11].
Intra- and inter-operator variability was assessed viaKendall’s
tau-b correlation coefficient [12]. This assessmentwas done in a
pairwise fashion across each pair of readersbefore and after being
provided with the decision supportoutput and across each reading
methodology.
Results
System Evaluation: Variability in ROI boundary producesno
significant change in either the shape of the ROC curveor the AUC
values (Fig. 5a). Similarly, the ROI analysisshows minimal class
switching between P-S/S-P categories,2.7 and 3.3%, respectively
(Fig. 5b). We further correlatethe results for each of the
categorical groups supplied by thesystem to the BI-RADS assessments
provided by the radi-ologist readers (Fig. 6).
Analysis of the operating points of the system appear to beas
good, or better, than the radiologists tested in this study(Fig.
6). This suggests that the performance of categoricaloutputs of the
system align to and exceed the performanceof the BI-RADS
assessments.
The reader evaluation analysis showed a system only AUC[95%
confidence interval (CI)] of 0.8648 [0.8345–0.8893].
Eachradiologist’s stand-alone performance is detailed in Table
3.
Similarly, the sequential and independent joint perfor-mance is
summarized in Table 4 and Fig. 7.
Intra-reader and inter-reader variability, as measured
byKendall’s tau-b, is summarized in Tables 5 and 6,
respectively.
Discussion
The current study confirms that this DS system performs
fa-vorably when compared with a radiologist’s performance,
Fig. 4 Schematic representation of the a sequential and b
independent reading paradigms. A combination approach seen in c was
utilized in this study
412 J Digit Imaging (2019) 32:408–416
-
confirming prior studies [9]. In addition, rather than
simplycomparing DS system performance to that of a radiologist,
itextends these prior results by assessing workflows that
morerealistically approximate clinical practice. Past studies
haveshown mixed evidence on the effect of the tested
readingmethodologies on overall reader performance, but none
haveconducted an investigation within the context of
diagnosticdecision support, and their effects remain unknown
[13].Our results show a sizeable variation in performance
obtaineddepending on which reading methodology was chosen(Table 4).
The impact of the reading methodology on studyperformance has
practical workflow considerations. These re-sults suggest there may
a strong impact of confirmation bias ina sequential study design.
This can be clearly seen in Fig. 7bversus Fig. 7c, where the
deviation from the control assess-ment is significantly smaller in
the sequential read versus in-dependent read. This has practical
implications in the utiliza-tion of machine learning decision
support in breast ultrasounddiagnostics and likely beyond.
Furthermore, as would be expected by providing a supple-mental,
concurrent read that out-performs the original reader,overall
inter-operator variability decreased significantly.Surprisingly,
inter-operator variability decreased even beyondthat of the 4-week
washout intra-reader variability perTables 5 and 6. Due to the
study design, the effects of a ma-chine learning-based concurrent
read on intra-operator vari-ability were not evaluated, but with
the evidence presentedin this study, it would seem likely that a
proportional decreasein this metric could be expected.
Clinical Applications
When looking at practical clinical workflow applications,
theperformance results and study design have a number of
impli-cations on the application of AI software.
In clinical practice, the typical sequence of radiologyworkflow
is:
AUC
Coun
t
FPR ( 1 – Specificity)
TPR
a b
Fig. 5 Results of the system evaluation. a ROC curves and
corresponding AUCS assessing impact of ROI boundary variation. b
Assessment of classswitching due to ROI boundary variation
System
System
Fig. 6 Sensitivity and specificityof each reader’s
BI-RADSgrading is compared to that of thesystems
correspondingcategorical output
J Digit Imaging (2019) 32:408–416 413
-
1. Radiologist assesses mammographic images and
instructstechnologist to perform a complete
mammographicexamination
2. Radiologist decides if US is needed3. If so, the technologist
acquires images and presents to
radiologist4. Radiologist assesses images and the radiologist
may or
may not confirm the results with radiologist real
timescanning
5. Radiologist formulates diagnosis
In the sequential workflow, the radiologist would completeBstep
5^ then assess the DS output. In the independentworkflow, the DS
output would be presented to the radiologistduring Bstep 4,^ along
with the US images (e.g., along withthe other US Bdata^).
In clinical practice, if the radiologist has confidence in theDS
system, the independent workflow seems more likely toimpact
clinical management, e.g., the radiologist looks at allthe data
(demographic/clinical history, mammographic, US,DS output) and
forms a diagnosis (the ultimate goal).
Comparison to Other Systems
Prior research has explored the difference between sequentialand
independent study designs and their respective effects
onperformance [13–16]. These studies have suggested that
bothdesigns produce similar performance results within compara-tive
analyses. They then conclude that sequential designs arepreferable
due to lower time and resource requirements.
Interestingly, our results seem to suggest a more
significantdeviation between these two study designs.
The difference between our results and the results
discussedabove can perhaps be attributed to the following factors.
Thefirst consideration which must be made is that the
technologybeing tested and the underlying modality are both
different.Second, the task being performed by the decision support
sys-tem is all-together different from the CAD systems being
ex-amined in these studies. Most of the systems under study
arefocused on detection, while DS is focused on diagnosis.
In detection, a sequential read implies that the clinician
iden-tifies regions of interest, performs CAD, and then
potentiallyexamines additional regions, as suggested by the CAD
device.When performing an independent read, that clinician will
seeregions of interest as identified by CAD and may then
examineadditional regions based upon their own inspection. In both
cases,the clinician is combining their detection results with the
CAD’s,so it is reasonable that performance is similar between the
two.
In diagnosis, a sequential read implies that the clinicianwill
examine a nodule, arrive at a conclusion, and then re-ceive the
recommendation of the DS system. The recom-mendation will either
confirm their decision, alter their de-cision, or not be
considered. In an independent read, therecommendation is presented
at the outset, and is consid-ered as additional input data
alongside the image as theclinician makes a decision. In the
sequential case, sincethe clinician has already formed an opinion,
a dissentingrecommendation may meet with intransigence, and windup
suffering from confirmation bias.
Limitations
While the results suggest a strong performance benefit, thereare
several limitations to the study design that must be takeninto
consideration. The study only consisted of three (3)readers.
Although the readers had varying degrees of experi-ence within the
study, the study does not capture the fullbreadth of readers across
the broader population of radiolo-gists that read and interpret
breast ultrasound images. The
Table 3 Each reader’s performance was assessed prior to
beingpresented the system’s output. The results of their control
reads asmeasured via AUC is shown in this table
Radiologist ID AUC, 95% CI
1 0.7618 [0.7244–0.7934]
2 0.7543 [0.7197–0.7887]
3 0.7325 [0.6897–0.7689]
Table 4 In order to compare the two reading methodologies,
thereaders’ performance was assessed via AUC compared to
theircontrol reads summarized in Table 3. None of the readers
attained
statistical significance when utilizing sequential reads, while
allreaders were significantly better when utilizing an
independentreader strategy
Radiologist ID Sequential readAUC, 95% CI
P value CR vs SRtwo-tailed alpha = 0.05
Independent read AUC, 95% CI
P value CR vs IRtwo-tailed alpha = 0.05
1 0.7935 [0.7567–0.8229] 0.235 0.8213[0.7861–0.8516]
0.0285*
2 0.7674 [0.7327–0.8001] 0.601 0.8305[0.7982–0.8594]
0.00155*
3 0.7859 [0.7527–0.8174] 0.0532 0.7988[0.7632–0.8310]
0.0160*
*Significant
414 J Digit Imaging (2019) 32:408–416
-
number of cases (500) and enrichment within the study mayalso
limit its ability to represent the typical distribution ofcases
that a reader would expect to see in practice. The choiceof
distribution of the cases was an attempt to create a set thatwas
broadly representative of the greater populations of le-sions as a
whole but could also answer questions in a statisti-cally
meaningful way about events that have low populationincidence. This
further extends to the retrospective nature ofthe study design. In
clinical practice, additional factors impactclinical reasoning that
are not fully represented in the study,such as patient history,
prior studies, and patient preferencetowards clinical follow up.
While a prospective, randomized
control study would have addressed some of these concerns,
itwould come at the cost of study time and complexity.
This study did not compare intra-operator variability withand
without a decision support output as it would have requiredan
additional set of reads for each participant. Based on thecurrent
results, it would seem likely that the intra-operator var-iability
would decrease, but without study modification, theoccurrence and
extent of the variability is unknown.
The first reading session of this studywas not
counterbalanced,and all readers initially read sequential first and
independent sec-ond. Cases without a corresponding DS output were
randomlyintroduced in the independent session to break up the
readingschedule and allow for the evaluation of intra-operator
variability.The lack of counterbalancing between sequential and
independentreads may have introduced slight reader bias when
comparing thetwo paradigms.
Finally, the current study assesses the impact of DS on
USinterpretation in isolation, when in fact a complete breast
im-aging assessment incorporates demographic data, clinical
his-tory, and other imaging modalities such as mammography.New and
exciting avenues of inquiry are needed to more fullyevaluate the
role and utility of DS needs in this larger context.
Fig. 7 Comparative assessment of a control, b sequential, and c
independent reading workflows. Operating point specific improvement
for Independentvs control assessments were additionally measured
(D)
Table 5 To further characterize reader performance,
intra-readervariability was measured via Kendall’s tau-b
Radiologist ID Kendall’s tau-b for intra-readervariability
assessment.
1 0.597
2 0.595
3 0.529
J Digit Imaging (2019) 32:408–416 415
-
Conclusion
We have been able to demonstrate that reader workflow
cansignificantly affect clinical performance when
incorporatingAI-based decision support tools. This evaluation has
novelpractical implications on the utilization of such
technologiesin diagnostic environments as compared to previous
studieswhich have concluded an effective equivalence between
thesetwo reading paradigms. Independent reads (concurrent
reads)have shown dramatic shifts in reader performance and
inter-operator variability as compared to either control reads
orsequential reads. The evidence provided in this study can beused
to impact both study design when demonstrating efficacyof new
diagnostic decision support tools, as well as their im-plementation
in practical environments.
Acknowledgements We would like to thank Dr. Bruce
McClennan,William Hulbert, and Graham Anderson for all of the
discussion andinsight provided to make this work possible.
Open Access This article is distributed under the terms of the
CreativeCommons At t r ibut ion 4 .0 In te rna t ional License (h t
tp : / /creativecommons.org/licenses/by/4.0/), which permits
unrestricted use,distribution, and reproduction in any medium,
provided you give appro-priate credit to the original author(s) and
the source, provide a link to theCreative Commons license, and
indicate if changes were made.
References
1. Siegel RL, Miller KD, Jemal A: Cancer statistics, 2018. CA:
ACancer Journal for Clinicians 68:7–30, 2018.
https://doi.org/10.3322/caac.21442
2. Bae MS, HanW, Koo HR, Cho N, Chang JM, Yi A, Park I, Noh
D,Choi WS, Moon WK: Characteristics of breast cancers detected
byultrasound screening in women with negative mammograms.Cancer
Science 102:1862–1867, 2011.
https://doi.org/10.1111/j.1349-7006.2011.02034.x
3. Berg, Wendie A., Bandos, Andriy I., Mendelson, Ellen B.,
Lehrer,Daniel, Jong, Roberta A., Pisano, Etta D.; Ultrasound as the
prima-ry screening test for breast cancer: analysis from ACRIN
6666,JNCI: Journal of the National Cancer Institute, Volume 108,
Issue4, 1 April 2016, djv367,
https://doi.org/10.1093/jnci/djv367
4. Chabi M, Borget I, Ardiles R, Aboud G, Boussouar S, Vilar
VS,Dromain C, Balleyguier C: Evaluation of the accuracy of a
computer-aided diagnosis (CAD) system in breast ultrasound
according to theradiologist's experience. Academic radiology
19(3):311–319, 2012
5. Gur, D., Sumkin, J.H., Rockette, H.E., Ganott, M., Hakim,
C.,Hardesty, L., Poller, W.R., Shah, R., Wallace, L.; Changes in
breast
cancer detection and mammography recall rates after the
introduc-tion of a computer-aided detection system, JNCI: Journal
of theNational Cancer Institute, Volume 96, Issue 3, 4 February
2004,Pages 185–190, https://doi.org/10.1093/jnci/djh067.
6. Litjens G, Debats O, Barentsz J, Karssemeijer N, Huisman
H:Computer-aided detection of prostate cancer in MRI. in
IEEETransactions on Medical Imaging 33(5):1083–1092, 2014.
https://doi.org/10.1109/TMI.2014.2303821
http://ieeexplore.ieee.org/stamp/stamp.jsp?tp=&arnumber=6729091&isnumber=6803900
7. Van Ginneken B, Ter Haar Romeny BM, Viergever
MA:Computer-aided diagnosis in chest radiography: a survey. inIEEE
Transactions on Medical Imaging 20(12):1228–1241,
2001.https://doi.org/10.1109/42.974918
http://ieeexplore.ieee.org/stamp/stamp.jsp?tp=&arnumber=974918&isnumber=21028
8. FDA.gov. QVIEW Medical, Inc. Premarket approval for
QVCADsystem. Summary of safety and effectiveness. Approved:November
9, 2016.
https://www.accessdata.fda.gov/cdrh_docs/pdf15/P150043B.pdf
9. Barinov L, Jairaj A, Paster L, Hulbert W, Mammone R,
PodilchukC: Decision quality support in diagnostic breast
ultrasound throughartificial intelligence. IEEE Signal Processing
in Medicine andBiology Symposium (SPMB)., 2016.
https://doi.org/10.1109/spmb.2016.7846873
10. Data were obtained from the NCI-funded Breast
CancerSurveillance Consortium (HHSN261201100031C). Downloadedon
[2018, February 21] from the Breast Cancer SurveillanceConsortium
website, http://breastscreening.cancer.gov/.
11. Dorfman DD, Berbaum KS, Metz CE: Receiver operating
charac-teristic rating analysis: Generalization to the population
of readersand patients with the jackknife method. Investigative
Radiology.27:723–731, 1992
12. KendallM:Anewmeasure of rank correlation. Biometrika.
30(1–2):81–89, 1938.
https://doi.org/10.1093/biomet/30.1-2.81.JSTOR2332226
13. Schalekamp S, van Ginneken B, Schaefer-Prokop
CM,Karssemeijer N: Influence of study design in receiver
operatingcharacteristics studies: Sequential versus independent
reading.Journal of Medical Imaging. 1(1):015501, 2014.
https://doi.org/10.1117/1.JMI.1.1.015501
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4478981/.
14. Beiden SV, Wagner RF, Doi K, Nishikawa RM, Freedman
MB-L,Shih-Chung X, Xin-Wei: Independent versus sequential reading
inROC studies of computer-assist modalities. Academic
Radiology.9(9):1036–1043, 2002
https://www.sciencedirect.com/science/article/pii/S1076633203804798
15. Gallas BD, Chan H-P, D’Orsi CJ, Dodd LE, Giger ML, Gur
D,Krupinski EA, Metz CE, Myers KJ, Obuchowski NA, Sahiner
B,Toledano AY, Zuley ML: Evaluating imaging and
computer-aideddetection and diagnosis devices at the FDA. Academic
radiology.19(4):463–477, 2012.
https://doi.org/10.1016/j.acra.2011.12.016https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5557046/#R73.
16. Obuchowski NA,MezianeM, Dachman AH, Lieber ML,MazzonePJ:
What’s the control in studies measuring the effect of
computer-aided detection (CAD) on observer performance?
AcademicRadiology. 17:761–767, 2010
https://www.ncbi.nlm.nih.gov/pubmed/20457419
Table 6 Pairwise combinationsof variability were
measuredutilizing the sequential read (SR)methodology.
Interestingly, theindependent read (IR) variabilitywas lower than
intra-readervariability
Radiologist ID (KTBfor reading methods)
1 (control, SR, IR) 2 (control, SR,IR) 3 (control, SR,IR)
1 (control, SR,IR) (1, 1, 1) (0.5505, 0.6263*, 0.7231**)
(0.4944, 0.6640*, 0.7476**)
2 (control, SR,IR) – (1, 1, 1) (0.4229, 0.5641*, 0.6231**)
3 (control, SR,IR) – – (1, 1, 1)
*Significant with p < .01; **significant difference with p
< 1e−8
416 J Digit Imaging (2019) 32:408–416
https://doi.org/10.3322/caac.21442https://doi.org/10.3322/caac.21442https://doi.org/10.1111/j.1349-7006.2011.02034.xhttps://doi.org/10.1111/j.1349-7006.2011.02034.xhttps://doi.org/10.1093/jnci/djv367https://doi.org/10.1093/jnci/djh067https://doi.org/10.1109/TMI.2014.2303821https://doi.org/10.1109/TMI.2014.2303821http://ieeexplore.ieee.org/stamp/stamp.jsp?tp=&arnumber=6729091&isnumber=6803900http://ieeexplore.ieee.org/stamp/stamp.jsp?tp=&arnumber=6729091&isnumber=6803900https://doi.org/10.1109/42.974918http://ieeexplore.ieee.org/stamp/stamp.jsp?tp=&arnumber=974918&isnumber=21028http://ieeexplore.ieee.org/stamp/stamp.jsp?tp=&arnumber=974918&isnumber=21028https://www.accessdata.fda.gov/cdrh_docs/pdf15/P150043B.pdfhttps://www.accessdata.fda.gov/cdrh_docs/pdf15/P150043B.pdfhttps://doi.org/10.1109/spmb.2016.7846873https://doi.org/10.1109/spmb.2016.7846873http://breastscreening.cancer.gov/https://doi.org/10.1093/biomet/30.1-2.81.JSTOR2332226https://doi.org/10.1117/1.JMI.1.1.015501https://doi.org/10.1117/1.JMI.1.1.015501https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4478981/https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4478981/https://www.sciencedirect.com/science/article/pii/S1076633203804798https://www.sciencedirect.com/science/article/pii/S1076633203804798https://doi.org/10.1016/j.acra.2011.12.016https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5557046/#R73https://www.ncbi.nlm.nih.gov/pubmed/20457419https://www.ncbi.nlm.nih.gov/pubmed/20457419
Impact...AbstractIntroductionMethodsData CollectionMachine
LearningReader Characteristics and TrainingReader
WorkflowSequential workflowIndependent WorkflowSystem
EvaluationReader Evaluation
ResultsDiscussionClinical ApplicationsComparison to Other
SystemsLimitations
ConclusionReferences






![Artificial Intelligence for Mammography and Digital Breast ... · Automated analysis (ie, artificial intelligence [AI]) of mammograms and DBT images may address these needs. Computer-aided](https://img.pdfslide.us/doc/110x75/5f6c7222a90f5f482669f70a/artificial-intelligence-for-mammography-and-digital-breast-automated-analysis.jpg)




















