Embed Size (px)
Citation preview

IMPACTE 2010 MKH Library Services | [email protected] | T: 01908 243077 2013-01-21
IMPACTE Groups
Improving Medical Practice by Assessing CurrenT Evidence
Summaries of Group Discussions
in
MK Primary Care
2010
Quality:MK project1: IMPACTE workstream2
Compiled by: Date
Primary Care / eLearning Librarian, MKH Library Services January 2013
1 Saffin, K. (2010) Quality:MK Engaging with quality in primary care: A qualitative evaluation study commissioned by Milton
Keynes Primary Care Trust. Final report. Oxford, SPH. 2 Glasziou, P. (2010) The impact of IMPACTE Groups: Use of EBM journal clubs in general practice.

Quality:MK
IMPACTE group Date Topic
Broughton 30/06/2010 Managing abnormal LFTs
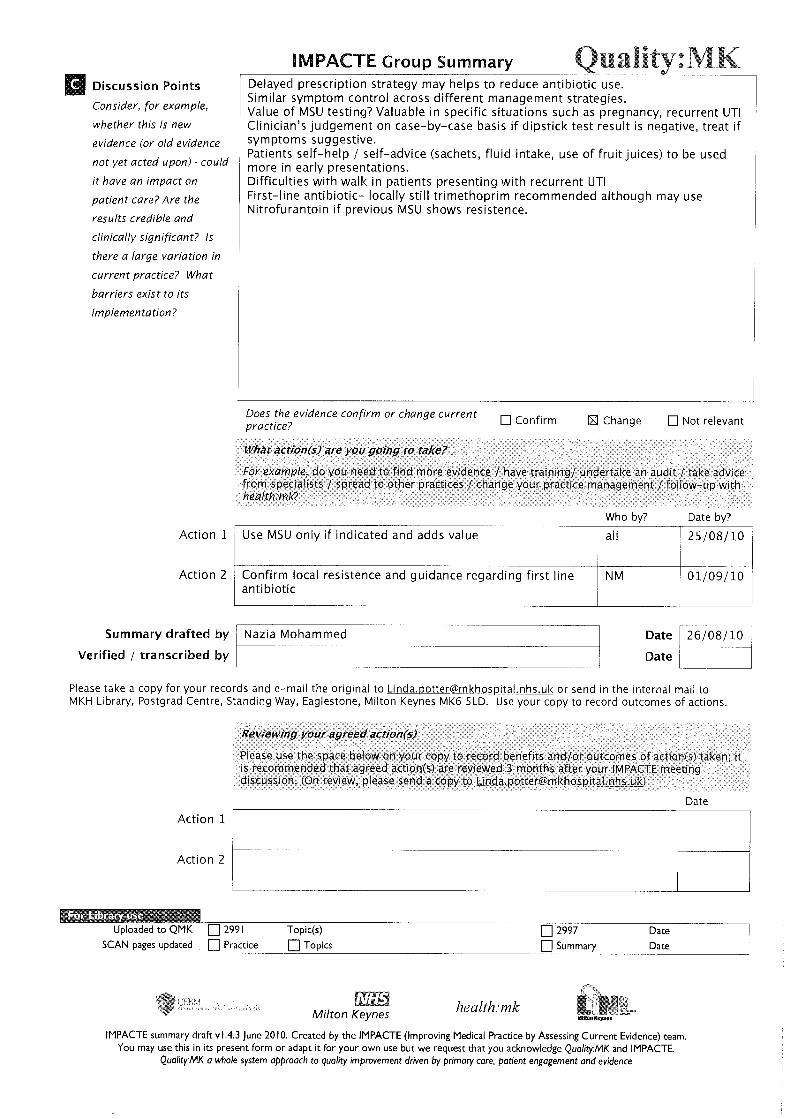
Broughton 25/08/2010 Management of UTI - symptom severity, duration and use of
antibiotics
Broughton 20/10/2010 GORD (gastric reflux / dyspepsia) and H pylori managemen
Broughton 20/10/2010 Hypertension in pregnancy
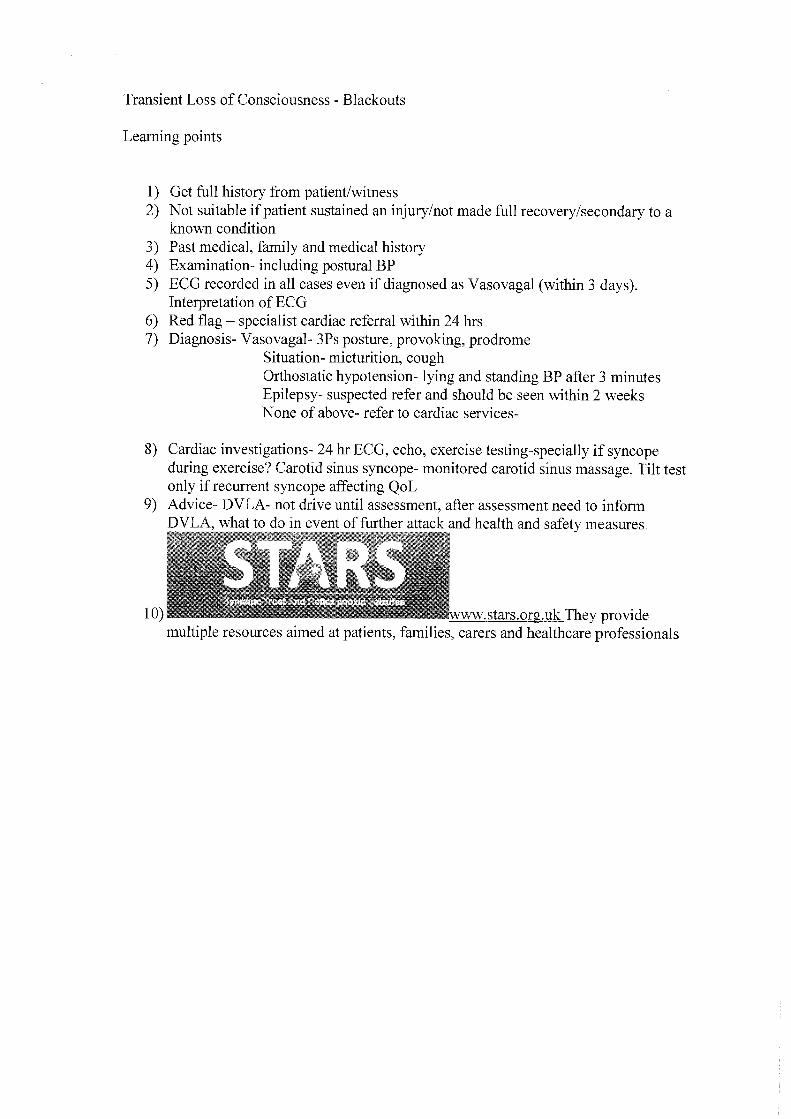
Broughton 20/10/2010 Transient loss of consciousness - blackouts
Broughton 20/10/2010 Heart failure
Broughton 24/11/2010 QRISK2 CVD risk assessment tool
CMK 26/03/2010 In patients with treated hypertension or recent TIA, what is
the relationship between various prognostic factors and risk of
CMK 04/06/2010 Vitamin D deficiency protocol
CMK 27/08/2010 Diagnosis of diabetes
CMK 27/08/2010 Audit report: Concomitant prescribing of triptans & SSRIs
CMK 27/08/2010 Audit report: Vitamin D deficiency
CMK 24/09/2010 GP consultations and self care for minor illness
CMK 29/10/2010 Pain referrals: clinical review - CMK Medical Centre audit
results
MK Village 28/05/2010 Review of NICE guidance on childhood UTI
MK Village 25/06/2010 Review of 2009 contraception guidelines
Parkside 02/02/2010 Management of dyspepsia; when to refer to endoscopy, when
to test for h pylori
Parkside 08/03/2010 What is the best way of managing UTI?
Parkside 30/03/2010 Psychotherapeutic tools to help adolescents in primary care
Parkside 04/05/2010 What are the risks & benefits of using quinine for muscle
cramps?
IMPACTE meetings 2010
IMPACTE 2010 MKH Library Services 2013-01-22

Quality:MK
IMPACTE group Date Topic
IMPACTE meetings 2010
Parkside 11/05/2010 Review of current guidance on the management of chest pain
Parkside 11/05/2010 Are we complying with best practice in the way we fit coils?
Parkside 18/05/2010 What is the current guidance for reducing the risk of venous
thromboembolism (VTE)?
Parkside 25/05/2010 What is the clinical significance of recent research on the
relationship between visit-to-visit variability of blood pressure
Parkside 15/06/2010 Review current NICE guidance on the management of LUTS in
men against current practice
Parkside 13/07/2010 Are we prescibing high levels of benzodiazepines and what
levels are harmful?
Parkside 13/07/2010 What is the latest guidance on bacterial meningitis?
Parkside 03/08/2010 Is it safe to manage alcohol detoxification in the community?
Parkside 09/11/2010 NICE guidelines on hypertension in pregnancy
Stony Stratford 16/06/2010 What is the evidence for the benefits & harms of long term
use of SSRIs and newer anti-depressants in adults with major
Stony Stratford 04/11/2010 Do ARBs affect cancer occurrence?
Wolverton 08/07/2010 Management of UTI
IMPACTE Central 09/02/2010 What has happened before a female patient comes to see their GP with suspected UTI?
IMPACTE Central 09/03/2010 Should we prescribe low dose aspirin to prevent CHD in patients with type 2 diabetes?
IMPACTE Central 13/04/2010 Is there an association between an educational program in mindful communication and primary care physician's burnout, empathy and attitude?
IMPACTE Central 01/06/2010 How accurate are diagnostic tests for identifying celiac disease
in adults presenting with abdominal symptoms in primary care
IMPACTE Central 13/07/2010 Doctors as patients
IMPACTE Central 12/10/2010 Does use of oral bisphosphonates increase the risk of cancer of oesophagus, stomach, and colorectum?
IMPACTE Central 09/11/2010 Effect of calcium supplements on risk of MI and cardiovascular
events
IMPACTE 2010 MKH Library Services 2013-01-22

















Quality:MK
Quality:MK a whole system approach to quality improvement driven by primary care, patient engagement and evidence
health:mk IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
IMPACTE Group summary
Practice/Group: CMK Medical Centre Date: 26 March 2010 Question/Topic :
In patients with treated hypertension or recent TIA, what is the relationship between various prognostic factors and risk of stroke?
Evidence used: i.e. References
Prognostic significance of visit-to-visit variability, maximum systolic blood pressure, and episodic hypertension (Rothwell, P M et al) The Lancet, Volume 375, Issue 9718, Pages 895 - 905, 13 March 2010
Type of evidence
1RCT, 2Systematic Review 3Qualitative Research 4Guideline Prognosis; review Prompts on how to appraise the different types of evidence, and space for comments are given on the back of this sheet.
What the evidence is about Population/Setting
Patients with a recent TIA; patients with treated hypertension. 4 studies were used – 1) UK-TIA randomised trial 1979-1985 [J Neurol Neurosurg Psychiatry 1991; 54: 1044-
54]; 1200mg vs 300mg aspirin vs placebo in 2435 patients with a recent TIA or ischaemic stroke; analysis of 2006 patients presenting with TIA only – 1438 men, mean age 60.3yrs, median time since TIA 23 days.
+ 3 other TIA and stroke cohorts 2) European Stroke Prevention Study (ESPS-1 [Lancet 1987; 330: 1351-54]; 2500
patients randomly assigned to dipyridamole plus 325mg aspirin vs placebo; analysis of placebo group only ? patients
3) Dutch TIA trial [N Engl J Med 1991; 325: 1261-66]; 3150 patients randomly assigned to 30mg aspirin vs 283mg aspirin; sub-group of 1473 patients randomly assigned to 50mg atenolol vs placebo
4) ASCOT-BPLA randomised control trial [Lancet 2005; 366: 895-906]; included 2011 patients with previous TIA or stroke; patients with hypertension, aged 40-79 yrs with 3 or more other vascular risk factors but no coronary heart disease randomly assigned to 2 antihypertensive regimes – amlodipine with perindopril as needed vs atenolol with bendroflumethiazide and potassium as needed
Intervention:
Comparison: (optional)
Outcome: Risk of stroke or other vascular event in relation to prognostic factors Prognostic factors: visit-to-visit variability in blood pressure, maximum systolic blood pressure, untreated episodic hypertension and residual variability
Is the evidence relevant to our practice? Is this a good source of evidence? Results, clinical bottom line: Is this new evidence ( or old evidence not yet acted upon) that could have an impact on patient care? Are the results credible and clinically significant? Is there a large variation in current practice? What barriers exist to its implementation? “More work is needed to identify measures that would combine the prognostic information associated with visit-to-visit variability in blood pressure with ease of use in routine clinical practice … “ (Rothwell p.904) No causal link between variability in blood pressure (or maximum SBP) and stroke – more research is needed using large-scale pooled analysis of multiple cohorts. See also ‘Rothwell, P.M. Effects of antihypertensive-drug class on interindividual varation in blood pressure and risk of stroke: a systematic review and meta-analysis. The Lancet, Volume 375, Issue 9718, Pages 906 - 915, 13 March 2010’

IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
Higher systolic reading is a predictor of stroke. Anti-hypertensive drug class-specific effects on risk of stroke; calcium-channel blockers seem to reduce risk to a greater extent? But, for now, need to continue to follow current guidelines. Discussion points How practically do you measure variability in blood pressure? Home monitoring vs clinic readings Instrumentation - mercury sphygmomanometer vs electronic readings. White coat syndrome. Choice of anti-hypertensive drug class. How are we going to follow up e.g. Do we need to find more evidence / have training/ undertake an audit / take advice from specialists / spread to other practices / change our practice management / follow-up with health:mkWhat action are we going to take Who by Date by
.Drafted by: Linda Potter Date: 06/04/10 verified by: Cheryl Manna Date: 06/04/10 Appraisal of different types of evidence
1RCT
Recruitment Were the subjects representative of the target population?
Allocation? Was the treatment allocation concealed before randomisation, were the groups comparable at the start?
Maintenance Follow up over 80%?
Measurements Were the outcomes measured with: Blinded subjects and assessors and/or Objective outcomes?
UK-TIA – 66% (1324) of patients reached visit 7 Blood pressure measurements in the 4 studies UK-TIA – sitting after rest, mercury sphygmomanometer, measured once at every 4mth follow-up visit (? yrs); variables were calculated from visits 1-7 (0-24mths) and from 1-10 (0-36mths) ESPS-1 – sitting after rest, mercury sphygmomanometer, mean of left and right arm, measured at follow-up visits every 3mths for 2 years Dutch TIA - sitting after rest, mercury sphygmomanometer, measured at follow-up visits every 4mths for a mean of 2 . 6 years ASCOT-BPLA – sitting after 5 min rest, validated semi-automated oscillometric device, measured at every visit (baseline 6 wks, 3 mths, 6mths and every 6mths thereafter). Participants at 4 centres had yrly 24-h ABPM with readings every 30 min. Mean time-weighted daytime (0900 – 2100h), night time (0100-0600h) and 24-h SBP and DBP were calculated.
Statistical Results: eg Risk Reduction (RR), Number Needed to Treat (NNT), Number Needed to Harm (NNH), Confidence Intervals (CI), P values
2Systematic review

IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
Question Does the research ask a clearly focussed question (PICO) and is it relevant?
Found all studies Did the search find all of the best evidence? (search strategy/publication bias
Appraisal/quality Have the studies been critically appraised
Synthesise Have the results been synthesised with appropriate summary tables and plots?
3Qualitative Research
Sampling strategy: Data collection methods : Data analysis methods: Relationship between the researcher and participant
:
4Guidelines Nationally recognised Guidelines e.g. NICE, SIGN, BTS are assumed to be based on high quality evidence and do not need to be appraised.

Quality:MK
Quality:MK a whole system approach to quality improvement driven by primary care, patient engagement and evidence
health:mk IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
IMPACTE Group summary
Practice/Group: CMK Medical Centre Date: 4 June 2010 Question/Topic :
Vitamin D deficiency protocol
Evidence used: i.e. References
Presentation by Dr Anne Jenkins, Consultant Rheumatology
Type of evidence
1RCT, 2Systematic Review 3Qualitative Research 4Guideline Prompts on how to appraise the different types of evidence, and space for comments are given on the back of this sheet.
What the evidence is about Population/Setting
Intervention:
Comparison: (optional)
Outcome:
Is the evidence relevant to our practice? Is this a good source of evidence? Results, clinical bottom line: Is this new evidence ( or old evidence not yet acted upon) that could have an impact on patient care? Are the results credible and clinically significant? Is there a large variation in current practice? What barriers exist to its implementation? Levels of deficiency / sufficiency in nmol/l Severe <25; Deficiency 25-50; Insufficiency 50-75; Replete 75-200; Toxicity >400 Issues in sourcing Vit D preparations – colecalciferol, ergocalciferol
Discussion points Risk factors for Vit D deficiency Assessing the patient Whether to assay & how many times Treatments during pregnancy & breastfeeding Sourcing unlicensed Vit D preparations How are we going to follow up e.g. Do we need to find more evidence / have training/ undertake an audit / take advice from specialists / spread to other practices / change our practice management / follow-up with health:mkWhat action are we going to take Who by Date by
Investigate sourcing Vit D preparations
SN
Search for more information on (a) the practicalities of treating Vit D deficiency in children and (b) Bristol & Birmingham protocols
LP
.Drafted by: L Potter Date:23/6/10 verified by: C Manna Date: 24/06/10

IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
Appraisal of different types of evidence
1RCT
Recruitment Were the subjects representative of the target population?
Allocation? Was the treatment allocation concealed before randomisation, were the groups comparable at the start?
Maintenance Follow up over 80%?
Measurements Were the outcomes measured with: Blinded subjects and assessors and/or Objective outcomes?
Statistical Results: eg Risk Reduction (RR), Number Needed to Treat (NNT), Number Needed to Harm (NNH), Confidence Intervals (CI), P values
2Systematic review
Question Does the research ask a clearly focussed question (PICO) and is it relevant?
Found all studies Did the search find all of the best evidence? (search strategy/publication bias
Appraisal/quality Have the studies been critically appraised
Synthesise Have the results been synthesised with appropriate summary tables and plots?
3Qualitative Research
Sampling strategy: Data collection methods : Data analysis methods: Relationship between the researcher and participant
:
4Guidelines Nationally recognised Guidelines e.g. NICE, SIGN, BTS are assumed to be based on high quality evidence and do not need to be appraised.











Quality:MK
Quality:MK a whole system approach to quality improvement driven by primary care, patient engagement and evidence
health:mk IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
IMPACTE Group summary
Practice/Group: IMPACTE Central Date: 9 February 2010 Question/Topic :
What has happened before a female patient comes to see their GP with suspected UTI?
Evidence used: i.e. References
A journey from self care to GP care: a qualitative interview study of women presenting with symptoms of UTI Br Journal General Practice 2009; v59: 490-5
Type of evidence
1RCT, 2Systematic Review 3Qualitative Research X 4Guideline
What the evidence is about Population/Setting
Female patients in General Practices across 4 counties in Southern England Already enrolled on a GP UTI management trial
Intervention: Interviews of patients to determine what patients did about their UTI symptoms before they consulted their GP
Comparison: (optional)
Outcome:
Is the evidence relevant to our practice? Is this a good source of evidence? Yes this evidence is relevant in general practice especially for trainees. Results, clinical bottom line: Is this new evidence ( or old evidence not yet acted upon) that could have an impact on patient care? Are the results credible and clinically significant? Is there a large variation in current practice? What barriers exist to its implementation? This is not new evidence but it shows how different people manage their diseases and how different clinicians manage patients. The numbers were small but still there are lessons to learn to support understanding of the patient journey before a GP consultation 4 common triggers for seeking help were identified 1. Failure to alleviate symptoms through lay remedies ie self care 2. Patient perception of symptom type ,duration, or escalation. Eg some patients thought their symptoms were out of the ordinary or escalation of symptoms. 3. Impending normal functioning and fulfilment of social roles. E.g some couldn’t go to work or couldn’t look after their children. 4. Concerns that it might be a serious illness or become serious. E.g fear of cancer. Discussion points Triggers identified came as no surprise Small numbers make it difficult to extrapolate findings Highlights new ideas about which questions to ask when taking histories on patients with
symptoms of UTI and new approaches to formulating management plan Difficult to repeat in MK setting.

IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
Some missing data e.g how many people were recruited in the parent UTI management study How are we going to follow up e.g. Do we need to find more evidence / have training/ undertake an audit / take advice from specialists / spread to other practices / change our practice management / follow-up with health:mkWhat action are we going to take Who by Date by
To ask more questions about actions the patients took to alleviate symptoms prior to the consultation.
Individual
To formulate management plan based on the ideas brought up by the paper provided they are in line with current NICE guidelines.
Individual
.Drafted by: Gloria Mosha, ST3 Date: 16 Feb 2010 verified by:Anne Gray Date: 16 Feb 2010 3Qualitative Research
Sampling strategy: Data collection methods : Data analysis methods: Relationship between the researcher and participant
33 patients approached, 21 interviewed, 20 interviews used in analysis. Not randomly assigned across UTI management trial arms Total number of people in the UTI management study not given Semi structured interviews – no indication of number of interviewers (one or many?) Recorded Interviews of 1 hour duration held in patients home, Interview tapes were transcribed for analysis. Data was analysed thematically, using principles of analytic induction. Relationship between the researcher and the participant was not given in the paper.

Quality:MK
Quality:MK a whole system approach to quality improvement driven by primary care, patient engagement and evidence
health:mk IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
IMPACTE Group summary
Practice/Group: IMPACTE Central Date: 9 March 2010 Question/Topic :
Evidence used: i.e. References
Type of evidence
1RCT, 2Systematic Review 3Qualitative Research 4Guideline Prompts on how to appraise the different types of evidence, and space for comments are given on the back of this sheet.
What the evidence is about Population/Setting
Intervention:
Comparison: (optional)
Outcome:
Is the evidence relevant to our practice? Is this a good source of evidence? Results, clinical bottom line: Is this new evidence ( or old evidence not yet acted upon) that could have an impact on patient care? Are the results credible and clinically significant? Is there a large variation in current practice? What barriers exist to its implementation? Discussion points How are we going to follow up e.g. Do we need to find more evidence / have training/ undertake an audit / take advice from specialists / spread to other practices / change our practice management / follow-up with health:mkWhat action are we going to take Who by Date by
.Drafted by: Date: verified by: Date:

IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
Appraisal of different types of evidence
1RCT
Recruitment Were the subjects representative of the target population?
Allocation? Was the treatment allocation concealed before randomisation, were the groups comparable at the start?
Maintenance Follow up over 80%?
Measurements Were the outcomes measured with: Blinded subjects and assessors and/or Objective outcomes?
Statistical Results: eg Risk Reduction (RR), Number Needed to Treat (NNT), Number Needed to Harm (NNH), Confidence Intervals (CI), P values
2Systematic review
Question Does the research ask a clearly focussed question (PICO) and is it relevant?
Found all studies Did the search find all of the best evidence? (search strategy/publication bias
Appraisal/quality Have the studies been critically appraised
Synthesise Have the results been synthesised with appropriate summary tables and plots?
3Qualitative Research
Sampling strategy: Data collection methods : Data analysis methods: Relationship between the researcher and participant
:
4Guidelines Nationally recognised Guidelines e.g. NICE, SIGN, BTS are assumed to be based on high quality evidence and do not need to be appraised.

Quality:MK
Quality:MK a whole system approach to quality improvement driven by primary care, patient engagement and evidence
health:mk IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
IMPACTE Group summary
Practice/Group: IMPACTE Central Date: 13 April 2010 Question/Topic :
Association of an educational programme in mindful communication with burnout empathy and attitudes among primary care physicians. The objective was to determine whether an educational programme in mindfulness communication and self awareness is associated with improvement in primary care physicians’ well-being, psychological distress, burnout and capacity for relating to patients. To look at the relationship b/w educational programme in mindfulness communication and self awareness which is associated with improvement in well-being, psychological distress and burn out.
Evidence used: i.e. References
Krasner, M.S. et al (2009) Association of an Educational Program in Mindful Communication With Burnout, Empathy, and Attitudes Among Primary Care Physicians JAMA. 2009;302(12):1284-1293
Type of evidence
1RCT, 2Systematic Review 3Qualitative Research 4Guideline Qualitative research - Before and after study design Prompts on how to appraise the different types of evidence, and space for comments are given on the back of this sheet.
What the evidence is about Population/Setting
Before and after study of 70 primary care physicians (average 15yrs in practice) in Rochester New York on CME course on mindfulness. An 8 week intensive phase was followed by 10mth maintenance phase.
Intervention: Continuing medical education course; 8wk intensive phase (2.5hrs /wk and 7hr retreat) followed by a maintenance phase of 10 monthly 2.5hrs sessions.
Comparison: (optional)
Outcome: Main outcome measures were mindfulness, burnout, empathy psychosocial orientation personality and mood measured at 2, 12 and 15 months Mindfulness burnout personality mood empathy and psychosocial orientation measured at baseline 2, 12, 15 months
Is the evidence relevant to our practice? Is this a good source of evidence? Yes but not a good source of information Results, clinical bottom line: Is this new evidence ( or old evidence not yet acted upon) that could have an impact on patient care? Are the results credible and clinically significant? Is there a large variation in current practice? What barriers exist to its implementation? Over the course of programme and follow-up participants demonstrated improvements in mindfulness
Discussion points Definition of mindfulness : quality of being fully present and ability to pay full attention Use of CME course to test the hypothesis Characteristics of participants i.e. primary care physicians There is an overall improvement Before and after study designs limit inference about intervention effects Limitations of the study i.e. not a randomised control trial Participants were self-selected

IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
No long term follow up was offered Conducted in a single location thus limiting the generalizability How are we going to follow up e.g. Do we need to find more evidence / have training/ undertake an audit / take advice from specialists / spread to other practices / change our practice management / follow-up with health:mkWhat action are we going to take Who by Date by
A proposed approach to addressing loss of meaning and lack of control in work/ practice life is developing greater mindfulness
.Drafted by: S. Anjum Date:29/05/10 verified by: L Potter Date: 01/06/2010

IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
Appraisal of different types of evidence
1RCT
Recruitment Were the subjects representative of the target population?
Allocation? Was the treatment allocation concealed before randomisation, were the groups comparable at the start?
Maintenance Follow up over 80%?
Measurements Were the outcomes measured with: Blinded subjects and assessors and/or Objective outcomes?
Statistical Results: eg Risk Reduction (RR), Number Needed to Treat (NNT), Number Needed to Harm (NNH), Confidence Intervals (CI), P values
2Systematic review
Question Does the research ask a clearly focussed question (PICO) and is it relevant?
Found all studies Did the search find all of the best evidence? (search strategy/publication bias
Appraisal/quality Have the studies been critically appraised
Synthesise Have the results been synthesised with appropriate summary tables and plots?
3Qualitative Research
Sampling strategy: Data collection methods : Data analysis methods: Relationship between the researcher and participant
:
4Guidelines Nationally recognised Guidelines e.g. NICE, SIGN, BTS are assumed to be based on high quality evidence and do not need to be appraised.

IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
Supplementary Notes
13/04/2010 Association of an Educational Program in Mindful Communication With Burnout, Empathy, and Attitudes Among Primary Care Physicians JAMA. 2009;302(12):1284-1293
RECRUITMENT All primary care physicians in Greater Rochester, New York invited to participate; mailings, follow-up tel calls (METHODS)
871
Eligible for consideration as study participants (METHODS) 642 70 enrolled (RESULTS) 70 % of eligible population who consented and were included 11% MAINTENANCE Followed-up at 12 mths and 15 months Losses to follow-up at 12 months (survey 4) (RESULTS &
METHODS) 14 20%
Losses to follow-up at 15 months (survey 5) (RESULTS & METHODS)
19 27%
Losses to follow-up should be <20% MEASUREMENT Baer (2-factor) Mindfulness scale Table 4 Correlations are used to test if 2 variables are associated with each
other. Measuring the correlation will give an indication of how strong an association there is between 2 variables; in this study whether the measure of mindfulness [Baer mindfulness scale] was associated with measures of burnout, empathy, beliefs and mood states.
Generally a correlation coefficient will fall within the range of -1 to 1 Where there is perfect association, the values for the correlation are 1 (positive association) or -1 (negative association) When no association is present the correlation will be equal to 0
No clear consensus as to what is a high or low correlation but the following values have been proposed as indicators for interpretation:
Correlation Negative Positive Small -0.29 to -0.10 0.10 to 0.29 Medium -0.49 to -0.30 0.30 to 0.49 Large -1.00 to -0.50 0.50 to 1.00 CI - usually reported as 95% CI, which is the range of values within
which we can be 95% sure that the true value for the whole population lies.
CI for a difference between 2 means: If the interval includes [crosses] 0 (zero) then it is statistically insignificant

Quality:MK
Quality:MK a whole system approach to quality improvement driven by primary care, patient engagement and evidence
health:mk IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
IMPACTE Group summary
Practice/Group: IMPACTE Central Date: 13 July 2010 Question/Topic :
What happens when doctors are ill?
Evidence used: i.e. References
What happens when doctors are patients? Qualitative study of GPs Fox, F., Harris, M., Taylor, G., Rodham, K., Sutton, J., Robinson, B., Scott, J British Journal of General Practice, 2009;59:811-818
Type of evidence
1RCT, 2Systematic Review 3Qualitative Research 4Guideline Prompts on how to appraise the different types of evidence, and space for comments are given on the back of this sheet.
What the evidence is about Population/Setting
17 GPs (10 male, 7 female) from 2 PCTs in the west of England; median age 46
Intervention:
Comparison: (optional)
Outcome: What are GPs experiences of being a patient with significant illness (pyschiatric, physical, acute and chronic) and how does this affect their own subsequent practice?
Is the evidence relevant to our practice? Is this a good source of evidence? Results, clinical bottom line: Is this new evidence ( or old evidence not yet acted upon) that could have an impact on patient care? Are the results credible and clinically significant? Is there a large variation in current practice? What barriers exist to its implementation? There is more research going on. Discussion points GPs can become ill as well. Guidelines to be in place as to what steps to take when GPs are ill, as it is different from being a hospital doctor who becomes ill. Experiences of consultations with GP or other health professional as patient. How are we going to follow up e.g. Do we need to find more evidence / have training/ undertake an audit / take advice from specialists / spread to other practices / change our practice management / follow-up with health:mkWhat action are we going to take Who by Date by
Look after your own and your colleagues health. Talk to someone early, when feeling poorly to avoid burn out.
.Drafted by: S. Bhatti Date: 15/7/10 transcribed by: L. Potter Date: 06/08/10
X
X

IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
Appraisal of different types of evidence
1RCT
Recruitment Were the subjects representative of the target population?
Allocation? Was the treatment allocation concealed before randomisation, were the groups comparable at the start?
Maintenance Follow up over 80%?
Measurements Were the outcomes measured with: Blinded subjects and assessors and/or Objective outcomes?
Statistical Results: eg Risk Reduction (RR), Number Needed to Treat (NNT), Number Needed to Harm (NNH), Confidence Intervals (CI), P values
2Systematic review
Question Does the research ask a clearly focussed question (PICO) and is it relevant?
Found all studies Did the search find all of the best evidence? (search strategy/publication bias
Appraisal/quality Have the studies been critically appraised
Synthesise Have the results been synthesised with appropriate summary tables and plots?
3Qualitative Research
Sampling strategy: Data collection methods : Data analysis methods: Relationship between the researcher and participant
Phenomenological research Semi-structured interview guided by a schedule and all carried out by lead researcher; interviews audio-taped, transcribed verbatim and anonymised Lead researcher engaged in 'reflexive bracketing' Data analysis process described. Results discussed
4Guidelines Nationally recognised Guidelines e.g. NICE, SIGN, BTS are assumed to be based on high quality evidence and do not need to be appraised.









Quality:MK
Quality:MK a whole system approach to quality improvement driven by primary care, patient engagement and evidence
health:mk IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
IMPACTE Group summary
Practice/Group: Parkside Date: 2 February 2010 Question/Topic
Management of dyspepsia When to refer to endoscopy When to test for H. pylori
Evidence used: i.e. References
NICE Guideline CG17 (2004) Dyspepsia: Managing dyspepsia in adults in primary care. http://guidance.nice.org.uk/CG17 Map of Medicine – Dyspepsia pathway http://england.mapofmedicine.com
Type of evidence
1RCT, 2Systematic Review 3Qualitative Research 4Guideline X Prompts on how to appraise the different types of evidence, and space for comments are given on the back of this sheet.
What the evidence is about Population/Setting
Intervention:
Comparison: (optional)
Outcome:
Is the evidence relevant to our practice? X Is this a good source of evidence? X Results, clinical bottom line: Is this new evidence ( or old evidence not yet acted upon) that could have an impact on patient care? Are the results credible and clinically significant? Is there a large variation in current practice? What barriers exist to its implementation? Some uncertainties about when to test patients for helicobacter pylori and whether or not to arrange FBC on patients over 55 yrs. Evidence / guidelines are complicated and difficult to remember for everyday use.
Discussion points How are we going to follow up e.g. Do we need to find more evidence / have training/ undertake an audit / take advice from specialists / spread to other practices / change our practice management / follow-up with health:mkWhat action are we going to take Who by Date by
Develop flow chart
NS 02/03/10
Share with other clinicians in practice
NS 02/03/10
.Drafted by: Nicola Smith Date: transcribed by:Linda Potter Date:3 Feb 2010

IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
Appraisal of different types of evidence
1RCT
Recruitment Were the subjects representative of the target population?
Allocation? Was the treatment allocation concealed before randomisation, were the groups comparable at the start?
Maintenance Follow up over 80%?
Measurements Were the outcomes measured with: Blinded subjects and assessors and/or Objective outcomes?
Statistical Results: eg Risk Reduction (RR), Number Needed to Treat (NNT), Number Needed to Harm (NNH), Confidence Intervals (CI), P values
2Systematic review
Question Does the research ask a clearly focussed question (PICO) and is it relevant?
Found all studies Did the search find all of the best evidence? (search strategy/publication bias
Appraisal/quality Have the studies been critically appraised
Synthesise Have the results been synthesised with appropriate summary tables and plots?
3Qualitative Research
Sampling strategy: Data collection methods : Data analysis methods: Relationship between the researcher and participant
:
4Guidelines Nationally recognised Guidelines e.g. NICE, SIGN, BTS are assumed to be based on high quality evidence and do not need to be appraised.

Quality:MK
Quality:MK a whole system approach to quality improvement driven by primary care, patient engagement and evidence
health:mk IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
IMPACTE Group summary
Practice/Group: Parkside Date: 8 March 2010 Question/Topic :
What is the best way of managing UTI?
Evidence used: i.e. References
Effectiveness of five different approaches in management of urinary tract infection: randomised controlled trial BMJ 2010;340:c199, doi: 10.1136/bmj.c199 (Published 5 February 2010)
Type of evidence
1RCT, X 2Systematic Review 3Qualitative Research 4Guideline Prompts on how to appraise the different types of evidence, and space for comments are given on the back of this sheet.
What the evidence is about Population/Setting
309 non-pregnant women in primary care aged 18-70 presenting with suspected urinary tract infection.
Intervention: 5 groups treated differently; empirical antibiotics; empirical delayed (by 48 hours) antibiotics; or targeted antibiotics based on a symptom score (two or more of urine cloudiness, urine smell, nocturia, or dysuria), a dipstick result (nitrite or both leucocytes and blood), or a positive result on midstream urine analysis
Comparison: (optional)
Outcome: Severity of symptoms (days 2-4) and duration and use of antibiotics
Is the evidence relevant to our practice? Is this a good source of evidence? Results, clinical bottom line: Is this new evidence ( or old evidence not yet acted upon) that could have an impact on patient care? Are the results credible and clinically significant? Is there a large variation in current practice? What barriers exist to its implementation? Best management plan is unclear. Discussion about value of sending mid stream urine (MSU) specimens to lab + delayed antibiotics. Plan - for uncomplicated UTIs – dipstick urine prescribe 3 day course of nitrofurantoin (based on local microbiology advice) Discussion points How are we going to follow up e.g. Do we need to find more evidence / have training/ undertake an audit / take advice from specialists / spread to other practices / change our practice management / follow-up with health:mkWhat action are we going to take Who by Date by
Audit MSUs before and after discussion
Jemma Mid April
.Transcribed by: Linda Potter Date: verified by: Date:

IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
Appraisal of different types of evidence
1RCT
Recruitment Were the subjects representative of the target population?
Allocation? Was the treatment allocation concealed before randomisation, were the groups comparable at the start?
Maintenance Follow up over 80%?
Measurements Were the outcomes measured with: Blinded subjects and assessors and/or Objective outcomes?
Yes Sealed in numbered envelopes Yes (research assistant was independent of the trial team and blinded to study group)
Statistical Results: eg Risk Reduction (RR), Number Needed to Treat (NNT), Number Needed to Harm (NNH), Confidence Intervals (CI), P values
2Systematic review
Question Does the research ask a clearly focussed question (PICO) and is it relevant?
Found all studies Did the search find all of the best evidence? (search strategy/publication bias
Appraisal/quality Have the studies been critically appraised
Synthesise Have the results been synthesised with appropriate summary tables and plots?
3Qualitative Research
Sampling strategy: Data collection methods : Data analysis methods: Relationship between the researcher and participant
:
4Guidelines Nationally recognised Guidelines e.g. NICE, SIGN, BTS are assumed to be based on high quality evidence and do not need to be appraised.

Quality:MK
Quality:MK a whole system approach to quality improvement driven by primary care, patient engagement and evidence
health:mk IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
IMPACTE Group summary
Practice/Group: Parkside Date: 30 March 2010 Question/Topic :
Psychotherapeutic tools to help adolescents in primary care
Evidence used: i.e. References
Expert opinion - Dr Mina Fazel, child psychiatrist and clinical lecturer in the Department of Psychiatry, University of Oxford. “Psychotherapeutic tools to help adolescents in primary care” - Psychiatry Study Day 2010 for GPs attended by GP
Type of evidence
1RCT, 2Systematic Review 3Qualitative Research 4Guideline Prompts on how to appraise the different types of evidence, and space for comments are given on the back of this sheet.
What the evidence is about Population/Setting
Intervention:
Comparison: (optional)
Outcome:
Is the evidence relevant to our practice? Is this a good source of evidence? Results, clinical bottom line: Is this new evidence ( or old evidence not yet acted upon) that could have an impact on patient care? Are the results credible and clinically significant? Is there a large variation in current practice? What barriers exist to its implementation? Strategies for helping adolescents with mental health problems
Sleep hygiene Problem solving Behavioural activation
How to help parents with a challenging child
Meet parents & help them to help the child together Solution focus – “miracle question” Information about local services Discussion points How are we going to follow up e.g. Do we need to find more evidence / have training/ undertake an audit / take advice from specialists / spread to other practices / change our practice management / follow-up with health:mkWhat action are we going to take Who by Date by
Buy books to patient library
RM 30/04/10
Use of power point info for patient information sheets
NS 30/04/10
.Drafted by: Nicola Smith Date: Transcribed by: Linda Potter Date: 19 April 2010
X X

IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
Appraisal of different types of evidence
1RCT
Recruitment Were the subjects representative of the target population?
Allocation? Was the treatment allocation concealed before randomisation, were the groups comparable at the start?
Maintenance Follow up over 80%?
Measurements Were the outcomes measured with: Blinded subjects and assessors and/or Objective outcomes?
Statistical Results: eg Risk Reduction (RR), Number Needed to Treat (NNT), Number Needed to Harm (NNH), Confidence Intervals (CI), P values
2Systematic review
Question Does the research ask a clearly focussed question (PICO) and is it relevant?
Found all studies Did the search find all of the best evidence? (search strategy/publication bias
Appraisal/quality Have the studies been critically appraised
Synthesise Have the results been synthesised with appropriate summary tables and plots?
3Qualitative Research
Sampling strategy: Data collection methods : Data analysis methods: Relationship between the researcher and participant
:
4Guidelines Nationally recognised Guidelines e.g. NICE, SIGN, BTS are assumed to be based on high quality evidence and do not need to be appraised.

Quality:MK
Quality:MK a whole system approach to quality improvement driven by primary care, patient engagement and evidence
health:mk IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
IMPACTE Group summary
Practice/Group: Parkside Date: 4 May 2010 Question/Topic :
What are the risks & benefits of using quinine for muscle cramps?
Evidence used: i.e. References
Katzberg HD, Khan AH, So YT (2010) Assessment: symptomatic treatment for muscle cramps (an evidence-based review): report of the therapeutics and technology assessment subcommittee of the American Academy of Neurology. Neurology. 2010 Feb 23;74(8):691-6. Review.
Type of evidence
1RCT, 2Systematic Review 3Qualitative Research 4Guideline Prompts on how to appraise the different types of evidence, and space for comments are given on the back of this sheet.
What the evidence is about Population/Setting
24 prospective controlled trials
Intervention:
Comparison: (optional)
Outcome:
Is the evidence relevant to our practice? Is this a good source of evidence? Results, clinical bottom line: Is this new evidence ( or old evidence not yet acted upon) that could have an impact on patient care? Are the results credible and clinically significant? Is there a large variation in current practice? What barriers exist to its implementation? Quinine effective for muscle cramps but risk of serious side effects is 2-4%. Use non-pharmacological methods first (Patient UK leg cramp leaflet) incl. slimline tonic; consider inv U+E, TFT, Ca++, LFT (?? magnesium) If quinine prescribed – use for 3 months then stop & see.
Discussion points How are we going to follow up e.g. Do we need to find more evidence / have training/ undertake an audit / take advice from specialists / spread to other practices / change our practice management / follow-up with health:mkWhat action are we going to take Who by Date by
Search for patients on quinine for more than 3 months
NS
.Drafted by: N. Smith Date: transcribed by: L Potter Date: 11 May 2010
X
yes yes

IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
Appraisal of different types of evidence
1RCT
Recruitment Were the subjects representative of the target population?
Allocation? Was the treatment allocation concealed before randomisation, were the groups comparable at the start?
Maintenance Follow up over 80%?
Measurements Were the outcomes measured with: Blinded subjects and assessors and/or Objective outcomes?
Statistical Results: eg Risk Reduction (RR), Number Needed to Treat (NNT), Number Needed to Harm (NNH), Confidence Intervals (CI), P values
2Systematic review
Question Does the research ask a clearly focussed question (PICO) and is it relevant?
Found all studies Did the search find all of the best evidence? (search strategy/publication bias
Appraisal/quality Have the studies been critically appraised
Synthesise Have the results been synthesised with appropriate summary tables and plots?
Yes + Yes
3Qualitative Research
Sampling strategy: Data collection methods : Data analysis methods: Relationship between the researcher and participant
:
4Guidelines Nationally recognised Guidelines e.g. NICE, SIGN, BTS are assumed to be based on high quality evidence and do not need to be appraised.

Quality:MK
Quality:MK a whole system approach to quality improvement driven by primary care, patient engagement and evidence
health:mk IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
IMPACTE Group summary
Practice/Group: Parkside Date: 11 May 2010 Question/Topic :
Are we complying with best practice in the way we fit coils?
Evidence used: i.e. References
Faculty of Sexual and Reproductive Healthcare (FSRH) Guidance: Intrauterine contraception (Nov 2007) http://www.fsrh.org/admin/uploads/CEUGuidanceIntrauterineContraceptionNov07.pdf
Type of evidence
1RCT, 2Systematic Review 3Qualitative Research 4Guideline Prompts on how to appraise the different types of evidence, and space for comments are given on the back of this sheet.
What the evidence is about Population/Setting
Intervention:
Comparison: (optional)
Outcome:
Is the evidence relevant to our practice? Is this a good source of evidence? Results, clinical bottom line: Is this new evidence ( or old evidence not yet acted upon) that could have an impact on patient care? Are the results credible and clinically significant? Is there a large variation in current practice? What barriers exist to its implementation?
Discussion points Current practice consistent with best practice. Check pulse + BP prior to insertion. Change template How are we going to follow up e.g. Do we need to find more evidence / have training/ undertake an audit / take advice from specialists / spread to other practices / change our practice management / follow-up with health:mkWhat action are we going to take Who by Date by
Look out for new guidance (due out 2010)
MM
Change template
LH done
.Drafted by: N. Smith Date: transcribed by: L. Potter Date: 21/05/2010
X
X X

IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
Appraisal of different types of evidence
1RCT
Recruitment Were the subjects representative of the target population?
Allocation? Was the treatment allocation concealed before randomisation, were the groups comparable at the start?
Maintenance Follow up over 80%?
Measurements Were the outcomes measured with: Blinded subjects and assessors and/or Objective outcomes?
Statistical Results: eg Risk Reduction (RR), Number Needed to Treat (NNT), Number Needed to Harm (NNH), Confidence Intervals (CI), P values
2Systematic review
Question Does the research ask a clearly focussed question (PICO) and is it relevant?
Found all studies Did the search find all of the best evidence? (search strategy/publication bias
Appraisal/quality Have the studies been critically appraised
Synthesise Have the results been synthesised with appropriate summary tables and plots?
3Qualitative Research
Sampling strategy: Data collection methods : Data analysis methods: Relationship between the researcher and participant
:
4Guidelines Nationally recognised Guidelines e.g. NICE, SIGN, BTS are assumed to be based on high quality evidence and do not need to be appraised.

Quality:MK
Quality:MK a whole system approach to quality improvement driven by primary care, patient engagement and evidence
health:mk IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
IMPACTE Group summary
Practice/Group: Parkside Date: 11 May 2010 Question/Topic :
Review of current guidance on the management of chest pain
Evidence used: i.e. References
NICE CG94 (March 2010) Unstable angina and NSTEMI NICE CG95 (March 2010) Chest pain of recent onset
Type of evidence
1RCT, 2Systematic Review 3Qualitative Research 4Guideline Prompts on how to appraise the different types of evidence, and space for comments are given on the back of this sheet.
What the evidence is about Population/Setting
UK NICE Guidance
Intervention:
Comparison: (optional)
Outcome:
Is the evidence relevant to our practice? Is this a good source of evidence? Results, clinical bottom line: Is this new evidence ( or old evidence not yet acted upon) that could have an impact on patient care? Are the results credible and clinically significant? Is there a large variation in current practice? What barriers exist to its implementation? Diagnosis of stable angina is clinical (+1- CT) – consult risk chart Exercise ECGs have no place in diagnosing angina Query – Should clopidogrel be given with aspirin for patients presenting with ACS? O2 not to be given routinely Discussion points How are we going to follow up e.g. Do we need to find more evidence / have training/ undertake an audit / take advice from specialists / spread to other practices / change our practice management / follow-up with health:mkWhat action are we going to take Who by Date by
Discuss with cardiologist
Completed
Pulse oximeter for emergency use (+ paediatric probe)
.Drafted by: N Smith Date: transcribed by: L Potter Date: 21 May 2010
X
X X

IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
Appraisal of different types of evidence
1RCT
Recruitment Were the subjects representative of the target population?
Allocation? Was the treatment allocation concealed before randomisation, were the groups comparable at the start?
Maintenance Follow up over 80%?
Measurements Were the outcomes measured with: Blinded subjects and assessors and/or Objective outcomes?
Statistical Results: eg Risk Reduction (RR), Number Needed to Treat (NNT), Number Needed to Harm (NNH), Confidence Intervals (CI), P values
2Systematic review
Question Does the research ask a clearly focussed question (PICO) and is it relevant?
Found all studies Did the search find all of the best evidence? (search strategy/publication bias
Appraisal/quality Have the studies been critically appraised
Synthesise Have the results been synthesised with appropriate summary tables and plots?
3Qualitative Research
Sampling strategy: Data collection methods : Data analysis methods: Relationship between the researcher and participant
:
4Guidelines Nationally recognised Guidelines e.g. NICE, SIGN, BTS are assumed to be based on high quality evidence and do not need to be appraised.
Quality:MK
Quality:MK a whole system approach to quality improvement driven by primary care, patient engagement and evidence
health:mk IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
IMPACTE Group summary
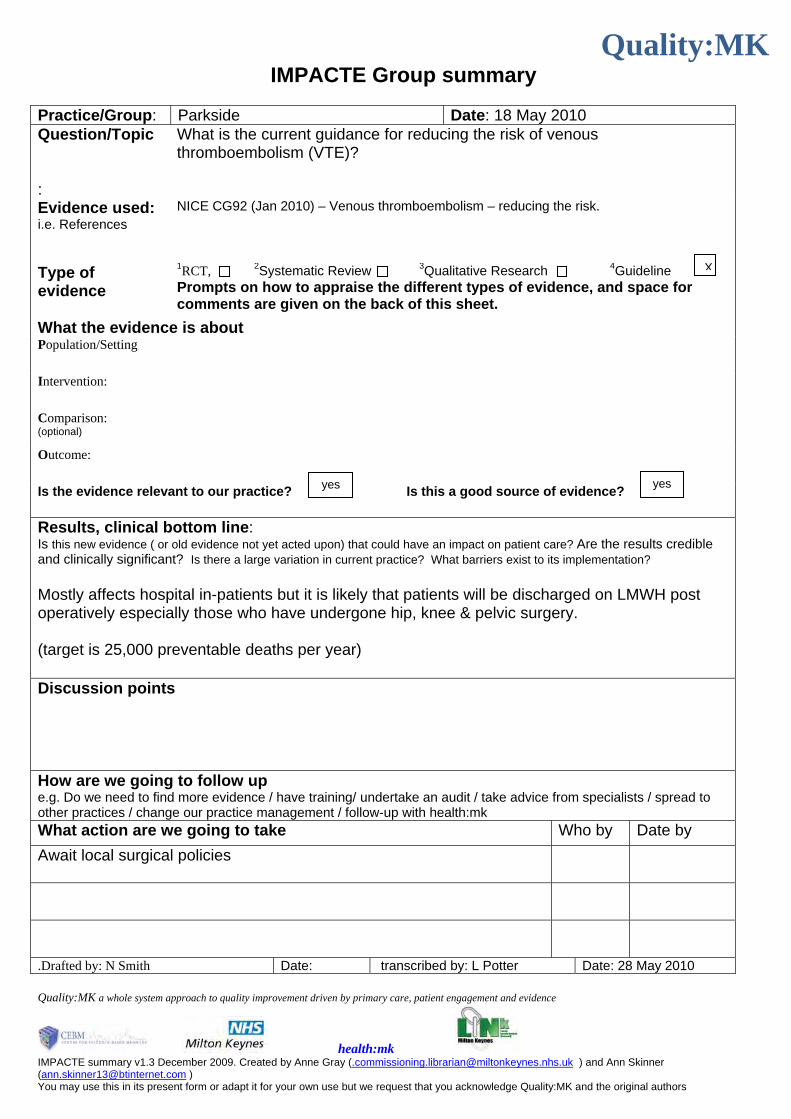
Practice/Group: Parkside Date: 18 May 2010 Question/Topic :
What is the current guidance for reducing the risk of venous thromboembolism (VTE)?
Evidence used: i.e. References
NICE CG92 (Jan 2010) – Venous thromboembolism – reducing the risk.
Type of evidence
1RCT, 2Systematic Review 3Qualitative Research 4Guideline Prompts on how to appraise the different types of evidence, and space for comments are given on the back of this sheet.
What the evidence is about Population/Setting
Intervention:
Comparison: (optional)
Outcome:
Is the evidence relevant to our practice? Is this a good source of evidence? Results, clinical bottom line: Is this new evidence ( or old evidence not yet acted upon) that could have an impact on patient care? Are the results credible and clinically significant? Is there a large variation in current practice? What barriers exist to its implementation? Mostly affects hospital in-patients but it is likely that patients will be discharged on LMWH post operatively especially those who have undergone hip, knee & pelvic surgery. (target is 25,000 preventable deaths per year) Discussion points How are we going to follow up e.g. Do we need to find more evidence / have training/ undertake an audit / take advice from specialists / spread to other practices / change our practice management / follow-up with health:mkWhat action are we going to take Who by Date by
Await local surgical policies
.Drafted by: N Smith Date: transcribed by: L Potter Date: 28 May 2010
X
yes yes

IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
Appraisal of different types of evidence
1RCT
Recruitment Were the subjects representative of the target population?
Allocation? Was the treatment allocation concealed before randomisation, were the groups comparable at the start?
Maintenance Follow up over 80%?
Measurements Were the outcomes measured with: Blinded subjects and assessors and/or Objective outcomes?
Statistical Results: eg Risk Reduction (RR), Number Needed to Treat (NNT), Number Needed to Harm (NNH), Confidence Intervals (CI), P values
2Systematic review
Question Does the research ask a clearly focussed question (PICO) and is it relevant?
Found all studies Did the search find all of the best evidence? (search strategy/publication bias
Appraisal/quality Have the studies been critically appraised
Synthesise Have the results been synthesised with appropriate summary tables and plots?
3Qualitative Research
Sampling strategy: Data collection methods : Data analysis methods: Relationship between the researcher and participant
:
4Guidelines Nationally recognised Guidelines e.g. NICE, SIGN, BTS are assumed to be based on high quality evidence and do not need to be appraised.

Quality:MK
Quality:MK a whole system approach to quality improvement driven by primary care, patient engagement and evidence
health:mk IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
IMPACTE Group summary
Practice/Group: Parkside Date: 25 May 2010 Question/Topic :
What is the clinical significance of recent research on the relationship between visit-to-visit variability of blood pressure and risk of stroke?
Evidence used: i.e. References
Prognostic significance of visit-to-visit variability, maximum systolic blood pressure, and episodic hypertension (Rothwell, P M et al) The Lancet, Volume 375, Issue 9718, Pages 895 - 905, 13 March 2010
Type of evidence
1RCT, 2Systematic Review 3Qualitative Research 4Guideline Prognosis; review Prompts on how to appraise the different types of evidence, and space for comments are given on the back of this sheet.
What the evidence is about Population/Setting
Patients with a recent TIA; patients with treated hypertension. 4 studies were used – 1) UK-TIA randomised trial 1979-1985 [J Neurol Neurosurg Psychiatry 1991; 54: 1044-
54]; 1200mg vs 300mg aspirin vs placebo in 2435 patients with a recent TIA or ischaemic stroke; analysis of 2006 patients presenting with TIA only – 1438 men, mean age 60.3yrs, median time since TIA 23 days.
+ 3 other TIA and stroke cohorts 2) European Stroke Prevention Study (ESPS-1 [Lancet 1987; 330: 1351-54]; 2500
patients randomly assigned to dipyridamole plus 325mg aspirin vs placebo; analysis of placebo group only ? patients
3) Dutch TIA trial [N Engl J Med 1991; 325: 1261-66]; 3150 patients randomly assigned to 30mg aspirin vs 283mg aspirin; sub-group of 1473 patients randomly assigned to 50mg atenolol vs placebo
4) ASCOT-BPLA randomised control trial [Lancet 2005; 366: 895-906]; included 2011 patients with previous TIA or stroke; patients with hypertension, aged 40-79 yrs with 3 or more other vascular risk factors but no coronary heart disease randomly assigned to 2 antihypertensive regimes – amlodipine with perindopril as needed vs atenolol with bendroflumethiazide and potassium as needed
Intervention:
Comparison: (optional)
Outcome: Risk of stroke or other vascular event in relation to prognostic factors Prognostic factors: visit-to-visit variability in blood pressure, maximum systolic blood pressure, untreated episodic hypertension and residual variability
Is the evidence relevant to our practice? Is this a good source of evidence? Results, clinical bottom line: Is this new evidence ( or old evidence not yet acted upon) that could have an impact on patient care? Are the results credible and clinically significant? Is there a large variation in current practice? What barriers exist to its implementation? “More work is needed to identify measures that would combine the prognostic information associated with visit-to-visit variability in blood pressure with ease of use in routine clinical practice … “ (Rothwell p.904) No causal link between variability in blood pressure (or maximum SBP) and stroke – more research is needed using large-scale pooled analysis of multiple cohorts. See also ‘Rothwell, P.M. Effects of antihypertensive-drug class on interindividual varation in blood pressure and risk of stroke: a systematic review and meta-analysis. The Lancet, Volume 375, Issue 9718, Pages 906 - 915, 13 March 2010’

IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
Predictor – SBP where the range of visit-to-visit readings ≥ 50 mm Hg. Anti-hypertensive drug class-specific effects on risk of stroke; calcium-channel blockers seem to reduce risk to a greater extent? Discussion points Report from GP Update where this paper was discussed – wait for results of prospective BPLTTC trial. How to plot SBP readings to determine whether range of variability between systolics ≥ 50 mm Hg Frequency of blood pressure measurements (electronic home monitoring) – 2 times/day over 7 days (or 5 or 6 times/day over 10 days?) Postural hypo/ertension? No action at present – await outcome of BPLTTC trial How are we going to follow up e.g. Do we need to find more evidence / have training/ undertake an audit / take advice from specialists / spread to other practices / change our practice management / follow-up with health:mkWhat action are we going to take Who by Date by
Await outcome of BPLTTC trial
.Drafted by: Linda Potter Date: 28/05/10 verified by: Date: Appraisal of different types of evidence
1RCT
Recruitment Were the subjects representative of the target population?
Allocation? Was the treatment allocation concealed before randomisation, were the groups comparable at the start?
Maintenance Follow up over 80%?
Measurements Were the outcomes measured with: Blinded subjects and assessors and/or Objective outcomes?
UK-TIA – 66% (1324) of patients reached visit 7 Blood pressure measurements in the 4 studies UK-TIA – sitting after rest, mercury sphygmomanometer, measured once at every 4mth follow-up visit (? yrs); variables were calculated from visits 1-7 (0-24mths) and from 1-10 (0-36mths) ESPS-1 – sitting after rest, mercury sphygmomanometer, mean of left and right arm, measured at follow-up visits every 3mths for 2 years Dutch TIA - sitting after rest, mercury sphygmomanometer, measured at follow-up visits every 4mths for a mean of 2 . 6 years ASCOT-BPLA – sitting after 5 min rest, validated semi-automated oscillometric device, measured at every visit (baseline 6 wks, 3 mths, 6mths and every 6mths thereafter). Participants at 4 centres had yrly 24-h ABPM with readings every 30 min. Mean time-weighted daytime (0900 – 2100h), night time (0100-0600h) and 24-h SBP and DBP were calculated.

IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
Statistical Results: eg Risk Reduction (RR), Number Needed to Treat (NNT), Number Needed to Harm (NNH), Confidence Intervals (CI), P values
2Systematic review
Question Does the research ask a clearly focussed question (PICO) and is it relevant?
Found all studies Did the search find all of the best evidence? (search strategy/publication bias
Appraisal/quality Have the studies been critically appraised
Synthesise Have the results been synthesised with appropriate summary tables and plots?
3Qualitative Research
Sampling strategy: Data collection methods : Data analysis methods: Relationship between the researcher and participant
:
4Guidelines Nationally recognised Guidelines e.g. NICE, SIGN, BTS are assumed to be based on high quality evidence and do not need to be appraised.

Quality:MK
Quality:MK a whole system approach to quality improvement driven by primary care, patient engagement and evidence
health:mk IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
IMPACTE Group summary
Practice/Group: Parkside Medical Centre Date: 15 June 2010 Question/Topic :
Review current NICE guidance on the management of LUTS in men and to check that current practice is consistent
Evidence used: i.e. References
NICE CG97 (May 2010) Management of lower urinary tract symptoms in men
Type of evidence
1RCT, 2Systematic Review 3Qualitative Research 4Guideline Prompts on how to appraise the different types of evidence, and space for comments are given on the back of this sheet.
What the evidence is about Population/Setting
Intervention:
Comparison: (optional)
Outcome:
Is the evidence relevant to our practice? Is this a good source of evidence? Results, clinical bottom line: Is this new evidence ( or old evidence not yet acted upon) that could have an impact on patient care? Are the results credible and clinically significant? Is there a large variation in current practice? What barriers exist to its implementation? Confirms current practice
Discussion points No-one currently uses urinary frequency volume chart & we do not intend to Increase use of IPSS score at early stage in patient management Check PSA at earlier stage than advised by NICE as more convenient to do with early investigations
i.e. checking renal function + urinanalysis Discussion about appropriate medication & when to refer (i.e still symptomatic despite treatment)
How are we going to follow up e.g. Do we need to find more evidence / have training/ undertake an audit / take advice from specialists / spread to other practices / change our practice management / follow-up with health:mk What action are we going to take Who by Date by
LUTS management flowchart
NS 22/6/10
.Drafted by: N Smith Date: 15/6/10 transcribed by: L Potter Date: 24/6/10
x
x

IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
Appraisal of different types of evidence
1RCT
Recruitment Were the subjects representative of the target population?
Allocation? Was the treatment allocation concealed before randomisation, were the groups comparable at the start?
Maintenance Follow up over 80%?
Measurements Were the outcomes measured with: Blinded subjects and assessors and/or Objective outcomes?
Statistical Results: eg Risk Reduction (RR), Number Needed to Treat (NNT), Number Needed to Harm (NNH), Confidence Intervals (CI), P values
2Systematic review
Question Does the research ask a clearly focussed question (PICO) and is it relevant?
Found all studies Did the search find all of the best evidence? (search strategy/publication bias
Appraisal/quality Have the studies been critically appraised
Synthesise Have the results been synthesised with appropriate summary tables and plots?
3Qualitative Research
Sampling strategy: Data collection methods : Data analysis methods: Relationship between the researcher and participant
:
4Guidelines Nationally recognised Guidelines e.g. NICE, SIGN, BTS are assumed to be based on high quality evidence and do not need to be appraised.










Quality:MK
Quality:MK a whole system approach to quality improvement driven by primary care, patient engagement and evidence
health:mk IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
IMPACTE Group summary
Practice/Group: Stony Medical Centre Date: 16 June 2010 Question/Topic :
What is the evidence for the benefits & harms of long term use of SSRIs and newer anti-depressants in adults with major depression?
Evidence used: i.e. References
Reid, S. & Barbui, C. Long term treatment of depression with selective serotonin reuptake inhibitors and newer antidepressants BMJ 2010, 3 April, Vol 340, 752-756
Type of evidence
1RCT, 2Systematic Review 3Qualitative Research 4Guideline Prompts on how to appraise the different types of evidence, and space for comments are given on the back of this sheet.
What the evidence is about Population/Setting
Severe spectrum of depression disorder.
Intervention: Antidepressant
Comparison: (optional)
Placebo
Outcome: Risk of relapse
Is the evidence relevant to our practice? Is this a good source of evidence? Results, clinical bottom line: Is this new evidence ( or old evidence not yet acted upon) that could have an impact on patient care? Are the results credible and clinically significant? Is there a large variation in current practice? What barriers exist to its implementation? Continuation of SSRI – agree continue for 12 months not 6 then review. Age – SSRIs associated with increased suicidal behaviours in under 25s Consider side effects – particularly GI effects & hyponatraemia in the over 80s.
Discussion points How long to continue SSRI? When to get advice from secondary care specialists Local services related to Mental Health Services & access to services How are we going to follow up e.g. Do we need to find more evidence / have training/ undertake an audit / take advice from specialists / spread to other practices / change our practice management / follow-up with health:mk What action are we going to take Who by Date by
.Drafted by: L Potter Date: 24/6/10 verified by: Date:
X
X

IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
Appraisal of different types of evidence
1RCT
Recruitment Were the subjects representative of the target population?
Allocation? Was the treatment allocation concealed before randomisation, were the groups comparable at the start?
Maintenance Follow up over 80%?
Measurements Were the outcomes measured with: Blinded subjects and assessors and/or Objective outcomes?
Statistical Results: eg Risk Reduction (RR), Number Needed to Treat (NNT), Number Needed to Harm (NNH), Confidence Intervals (CI), P values
2Systematic review
Question Does the research ask a clearly focussed question (PICO) and is it relevant?
Found all studies Did the search find all of the best evidence? (search strategy/publication bias
Appraisal/quality Have the studies been critically appraised
Synthesise Have the results been synthesised with appropriate summary tables and plots?
Review included 31 randomised trials (mainly discontinuation studies; most secondary care). NNT = 4 Need to look at risk factors ! Discontinuation can mimic symptoms of depression ? Was discontinuation tapered or abrupt (need to look at individual studies) most secondary care relative short follow-up of treatment; need longer longitudinal data
3Qualitative Research
Sampling strategy: Data collection methods : Data analysis methods: Relationship between the researcher and participant
:
4Guidelines Nationally recognised Guidelines e.g. NICE, SIGN, BTS are assumed to be based on high quality evidence and do not need to be appraised.

Quality:MK
Quality:MK a whole system approach to quality improvement driven by primary care, patient engagement and evidence
health:mk IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
Supplementary sheet 16/06/2010 Reid, S & Barbui, C. Long term treatment of depression with selective
serotonin reuptake inhibitors and newer antidepressants BMJ 2010, 3 April, Vol 340, 752-756
A What is the intervention (dose & frequency)? SSRIs B What is the intervention for? whether
continuing treatment with antidepressants reduces the risk of relapse
6mths 12mths 18mths 24mths 36mths
C What is the successful outcome (when, over what time did it occur)? Reduced risk of relapse
D How many had the intervention? 2527 442 1604 117 190 174 E How many had successful outcome with the intervention? 2044 377 1330 98 136 122 F Express as a percentage (100 x E/D) 81% 85% 83% 84% 72% 70% G What is the control or comparator? placebo H How many people had the control? 1883 296 1122 123 166 176 I How many had successful outcome with the control? 1073 187 707 64 65 50 J Express as a percentage (100 x I/H) 57% 63% 63% 52% 39% 28% ARR = F-J (ie absolute benefit of SSRIs is a 24% reduction in risk of
relapse)The absolute risk reduction (ARR) is the difference between the event rate in the experimental group and the event rate in the control group.
A low ARR indicates that there is a little difference in the frequency of the outcome between the control and new treatment groups.
24% 22% 20% 32% 32% 42%

IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
NNT = 1/ARRNo. of patients who need to receive the new treatment to prevent one
adverse event occurring.
4.2 4.5 5.0 3.2 3.1 2.4
RR = (100 - F) 0.19 0.15 0.17 0.16 0.28 0.30 (100 - J) 0.43 0.37 0.37 0.48 0.61 0.72 (100 - F)/(100 - J) (ie relative risk of relapse in patients receiving SSRIs
compared to placebo)0.44 0.40 0.46 0.34 0.47 0.42
44% 40% 46% 34% 47% 42% RRR 1-RR 0.56 0.60 0.54 0.66 0.53 0.58 56% 60% 54% 66% 53% 58%





Quality:MK
Quality:MK a whole system approach to quality improvement driven by primary care, patient engagement and evidence
health:mk IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
IMPACTE Group summary
Practice/Group: Wolverton Health Centre Date: 8 July 2010 Question/Topic :
Management of UTI – symptom severity, duration and use of antibiotics
Evidence used: i.e. References
Little, P. et al. Effectiveness of five different approaches in management of urinary tract infection: randomised controlled trial BMJ 2010, 3 April, Vol 340, 199
Type of evidence
1RCT, 2Systematic Review 3Qualitative Research 4Guideline Prompts on how to appraise the different types of evidence, and space for comments are given on the back of this sheet.
What the evidence is about Population/Setting
Non-pregnant women aged 18-70
Intervention: 1. empirical (immediate) antibiotics 2. empirical delayed (48hrs) antibiotics 3. targeted antibiotics based on a symptom score 4. targeted antibiotics based on a dipstick result 5. targeted antibiotics based on a positive result on midstream urine analysis
Comparison: (optional)
Outcome: Symptom severity (days 2-4) and duration, and use of antibiotics
Is the evidence relevant to our practice? Is this a good source of evidence? Results, clinical bottom line: Is this new evidence ( or old evidence not yet acted upon) that could have an impact on patient care? Are the results credible and clinically significant? Is there a large variation in current practice? What barriers exist to its implementation? Dipstick testing with targeted antibiotic use & delayed prescription or empirical delayed prescription helps to reduce antibiotic use. Similar symptom control across different management strategies. Confirms current practice. Discussion points Value of MSU testing? Clinician’s judgement on case-by-case basis if dipstick test result is negative. Severity of symptoms – if mild, no harm in waiting [negative dipstick test] / delayed prescription. Patients self-help / self-advice (sachets, fluid intake, use of fruit juices) Patients presenting with recurrent UTI First-line antibiotic? How are we going to follow up e.g. Do we need to find more evidence / have training/ undertake an audit / take advice from specialists / spread to other practices / change our practice management / follow-up with health:mk What action are we going to take Who by Date by
.Drafted by: L. Potter Date:9/7/10 verified by: S Raju Date: 10/07/10
X
X

IMPACTE summary v1.3 December 2009. Created by Anne Gray ([email protected] ) and Ann Skinner ([email protected] ) You may use this in its present form or adapt it for your own use but we request that you acknowledge Quality:MK and the original authors
Appraisal of different types of evidence
1RCT
Recruitment Were the subjects representative of the target population?
Allocation? Was the treatment allocation concealed before randomisation, were the groups comparable at the start?
Maintenance Follow up over 80%?
Measurements Were the outcomes measured with: Blinded subjects and assessors and/or Objective outcomes?
Statistical Results: eg Risk Reduction (RR), Number Needed to Treat (NNT), Number Needed to Harm (NNH), Confidence Intervals (CI), P values
2Systematic review
Question Does the research ask a clearly focussed question (PICO) and is it relevant?
Found all studies Did the search find all of the best evidence? (search strategy/publication bias
Appraisal/quality Have the studies been critically appraised
Synthesise Have the results been synthesised with appropriate summary tables and plots?
3Qualitative Research
Sampling strategy: Data collection methods : Data analysis methods: Relationship between the researcher and participant
:
4Guidelines Nationally recognised Guidelines e.g. NICE, SIGN, BTS are assumed to be based on high quality evidence and do not need to be appraised.





























