Embed Size (px)
Citation preview

AustralAs J Cardiac Thorac Surg 1993:2(2)
Impact Of Video Assisted Thoracoscopic Surgery On The Management Of Spontaneous Pneumothorax
Peter Clarke, FRACS
Thoracic Surgical Unit, Austin Hospital, Victoria, Australia
S pontaneous pneumothorax most commonly occurs when an apical bleb ruptures in a patient in their late
teens or young adulthood and is more commonly found amongst males than females. It is also common in the fifth and sixth decade of life when the underlying lesion is more likely to be a bulla. Blebs are covered with serosa and do not communicate with bronchi, whereas bullae are surrounded by lung tissue and are more likely to commu- nicate with a bronchus and thus be associated with a prolonged air leak.
In both instances the disease is more commonly found amongst smokers. After one episode of spon- taneous pneumothorax the likelihood of a recurrent episode is about 20%, but this markedly increases with each further occurrence.
The principles of management are as follows.
1. Keep the patient out of hospital if possible. 2. If admission is required, keep the admission as
short as possible.
3. Return the patient to full activity as soon as possible.
4. Prevent further recurrences.
The initial place of treatment is commonly the Emergency Department of a hospital. Admission used to be the rule. However, if the pneumothorax occupies less than 30% of the hemithorax and the patient is otherwise stable, it is now aspirated, and a chest x-ray examination is performed after 4 hours to make sure there is no recurrence. If the pneumothorax does recur or is greater than 30% at the time of admission, then a fine catheter (12 gauge) is inserted and placed on suction.
Once admitted, patients should be directly under the care of thoracic surgical units. It has been shown that their hospital stays are at least halved compared to those admitted to a medical unit. In addition, a benefit of admitting them initially to a surgical unit is that they have definitive treatment. Patients who present with a second episode, bilateral pneumothoraces or a tension pneumothorax should proceed directly to video assisted thoracoscopic surgery as should those patients who continue to have an air leak for more than 5 days after admission.
Thoracoscopy was introduced by Jacobaeus in 1910 1. He adapted a cystoscope for inspection of the pleural space in order to divide adhesions preventing a thera-
peutic pneumothorax for tuberculosis. The use of this technique for the management of spontaneous pneu- mothorax was suggested by Sattler in 1939 2, but the inability to deal with the underlying cysts limited its value. An open procedure with removal of the cyst and a pleurectomy became the management of choice. However patients who had open procedures generally remained in hospital for 5 to 8 days and required 2 to 3 weeks convalescence before returning to work. They were often discommoded by prolonged intercostal neu- ralgia which followed the necessity to spread the ribs.
During the past decade advances in microchip tech- nology have allowed for the miniaturisation of television cameras so that they could fit onto thoracoscopes. This development and the development of equipment which can be introduced through separate intercostal ports have lead to video assisted thoracoscopic surgery (VATS). Using VATS, a range of intrathoracic procedures can be performed without cutting muscles or spreading ribs.
The advantages of VATS are that it gives the operator a unparalleled view of the thorax with the ability to see and control bleeding. Patients have a shorter stay in hospital, a quicker convalescence and reduced postop- erative neuralgia. The disadvantages are the requirements for specialised equipment and training, and generally the operative times for any given procedure are longer.
During the past 16 months, 28 patients (5 females, 23 males, age range 16-74 years, mean age 27) have had 30 VATS procedures for spontaneous pneumothorax. One patient presented with bilateral pneumothoraces and had both sides treated during the same admission to hospital. Another patient with multiple cysts over the lung had a recurrence after VATS which was treated by an open procedure, only to have a further recurrence which was once again treated by VATS.
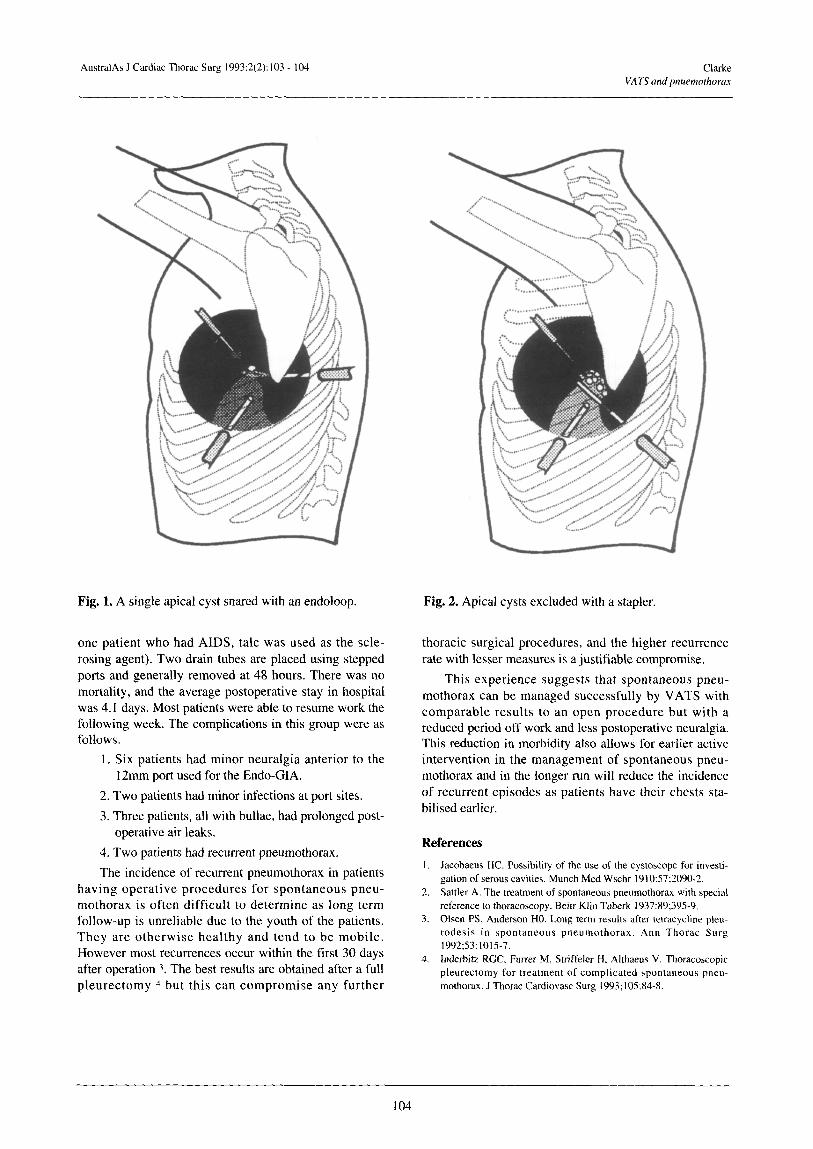
The VATS technique includes placement of a double-lumen tube with the patient in a lateral position and the scapula pulled upwards. Three ports are placed in an arch introducing the first port with a blunt trocar and placing the largest port anteriorly as this port is the one that is most likely to be associated with transient neu- ralgia. Simple cysts are ligated with an endoloop (Fig. 1) and more complex collections of cysts are excluded using an endo-GIA after removal of the knife (Fig. 2). A pleu- rodesis is effected by a combination of strip pleurectomy, diathermy and installation of alcohol-iodine solution. (In
103
AustralAs J Cardiac Thorac Surg 1993:2(2): 103 104 Clarke VATS and pnuemorhorax
Fig. 1. A single apical cyst snared with an endoloop. Fig. 2. Apical cysts excluded with a stapler.
one patient who had AIDS, talc was used as the scle- rosing agent). Two drain tubes are placed using stepped ports and generally removed at 48 hours. There was no mortality, and the average postoperative stay in hospital was 4.1 days. Most patients were able to resume work the following week. The complications in this group were as follows.
1. Six patients had minor neuralgia anterior to the I 2mm port used for the Endo-GIA.
2. Two patients had minor infections at port sites.
3. Three patients, all with bullae, had prolonged post- operative air leaks.
4. Two patients had recurrent pneumothorax.
The incidence of recurrent pneumothorax in patients having operative procedures for spontaneous pneu- mothorax is often difficult to determine as long term follow-up is unreliable due to the youth of the patients. They are otherwise healthy and tend to be mobile. However most recurrences occur within the first 30 days after operation 3. The best results are obtained after a full pleurectomy 4 but this can compromise any further
thoracic surgical procedures, and the higher recurrence rate with lesser measures is a justifiable compromise,
This experience suggests that spontaneous pneu- mothorax can be managed successfully by VATS with comparable results to an open procedure but with a reduced period off work and less postoperative neuralgia. This reduction in morbidity also allows for earlier active intervention in the management of spontaneous pneu- mothorax and in the longer run will reduce the incidence of recurrent episodes as patients have their chests sta- bilised earlier.
References I. Jacobaeus HC. Possibility of the use of the cystoscope for investi-
gation of serous cavities. Munch Med Wschr 1910:57;2090-2. 2. Sattler A. The treatment of spontaneous pneumothorax with special
reference to thoracoscopy. Beitr Klin Tuberk 1937:89;395-9. 3. Olsen PS. Anderson HO. Long term results after tetracycline pleu-
rodesis in spontaneous pneumothorax. Ann Thorac Surg 1992;53:1015-7.
4. Inderbitz RGC, Furrer M, Striffeler H, Althaeus V. Thoracoscopic pleurectomy for treatment of complicated spontaneous pneu- mothorax. J Thorac Cardiovasc Surg 1993;105:84-8.
104