-
RESEARCH ARTICLE
Impact of Stewardship on Inhaled Nitric OxideUtilization in a
Neonatal ICUAmir Elmekkawi, MD,a Kiran More, MD,b Jennifer Shea,
RRT,a Christina Sperling, RRT,c Zelia Da Silva, RRT,a Michael
Finelli, RRT,a Asaph Rolnitsky, MD,d
Robert P. Jankov, MD, PhDa
A B S T R A C T OBJECTIVES: Inhaled nitric oxide (iNO) remains
the “gold standard” therapy for hypoxemicrespiratory failure in
newborns. Despite good quality evidence to guide iNO use in this
population,we observed considerable practice variation,
particularly in timing and rate of weaning. Topromote
evidence-based practice, we launched an iNO stewardship program in
April 2013. Ourobjective was to determine whether iNO stewardship
led to changes in iNO utilization and weaning.
METHODS: We conducted a quality improvement project in an
outborn quaternary NICU,targeting improved iNO guideline
compliance. We compared patterns of iNO utilization between2
cohorts: prestewardship (April 2011–March 2013; retrospective data
collection) andpoststewardship (April 2013–March 2015; prospective
data collection).
RESULTS: Eighty-seven neonates received 88 courses of iNO in the
2 years prestewardship, and64 neonates received 64 courses of iNO
in the 2 years poststewardship. There were no
significantdifferences (P . .05) in patient demographics, in the
proportion of patients receiving iNO“off-label,” in proportion
initiated at the referring hospital, or in outcomes (death or
extracorporealmembrane oxygenation). There were significant (P ,
.05) reductions in median total hours oniNO per patient (47 vs 20;
P , .001), in iNO hours per patient from maximum dose to
initialwean (28 vs 9; P , .01), and in hours from initial wean to
discontinuation (14 vs 8; P , .05).
CONCLUSIONS: The introduction of iNO stewardship was associated
with improved adherenceto evidence-based guidelines and an overall
reduction in total and per-patient iNO use.
aDivision of Neonatologyand cDepartment of
Critical Care, The Hospitalfor Sick Children, Toronto,Canada;
bDepartment of
Neonatology,Christchurch Women’sHospital, Christchurch,
New Zealand; anddDepartment of Newborn
and DevelopmentalPaediatrics, SunnybrookHealth Sciences
Centre,
Toronto, Canada
www.hospitalpediatrics.orgDOI:10.1542/hpeds.2016-0003Copyright ©
2016 by the American Academy of Pediatrics
Address correspondence to Robert P. Jankov, MD, PhD, Division of
Neonatology, The Hospital for Sick Children, 555 University
Ave,Toronto, Ontario, Canada M5G 1X8. E-mail:
[email protected]
HOSPITAL PEDIATRICS (ISSN Numbers: Print, 2154-1663; Online,
2154-1671).
FINANCIAL DISCLOSURE: The authors have indicated they have no
financial relationships relevant to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they
have no potential conflicts of interest to disclose.
Drs Elmekkawi and More codesigned the data collection
instrument, collected data, coordinated and supervised data
collection, andcodrafted the initial manuscript; Ms Shea collected
data and reviewed and revised the manuscript; Ms Sperling
codesigned the datacollection instrument and reviewed and revised
the manuscript; Ms Da Silva and Dr Rolnitsky reviewed and revised
the manuscript; MrFinelli codesigned the data collection
instrument, collected data, and reviewed and revised the
manuscript; Dr Jankov conceptualizedand designed the study,
codesigned the data collection instrument, analyzed data, and
codrafted the initial manuscript; and all authorsapproved the final
manuscript as submitted.
HOSPITAL PEDIATRICS Volume 6, Issue 10, October 2016 607
by guest on June 29, 2021www.aappublications.org/newsDownloaded
from
www.hospitalpediatrics.orghttp://dx.doi.org/10.1542/hpeds.2016-0003mailto:[email protected]
-
Persistent pulmonary hypertension ofthe newborn (PPHN) arises
either as aprimary condition or secondary torespiratory distress
syndrome, meconiumaspiration, sepsis, or birth asphyxia.1,2
PPHN is characterized by persistentlyraised pulmonary vascular
resistanceand arterial pressure, generally associatedwith
extrapulmonary right-to-left shuntingleading to hypoxemic
respiratory failure(HRF). Before the availability of inhalednitric
oxide (iNO), therapy was largelysupportive with extracorporeal
membraneoxygenation (ECMO) employed as a finalresort. Improved
oxygenation with iNOtreatment in cases of PPHN was firstreported in
1992,3,4 with subsequent largerandomized trials demonstrating
asignificant reduction in the need forECMO.5–7 Despite there being
no evidenceto suggest that iNO decreases mortality,length of
hospital stay or the incidence ofadverse neurodevelopmental
outcomesafter PPHN,8–13 iNO has greatly simplifiedthe management of
PPHN, with no evidenceof adverse effects, either in the short-
orlong-term.12
When inhaled, nitric oxide rapidly reachespulmonary vascular
smooth musclewhere it binds to soluble guanylate
cyclase,stimulating relaxation. Relative pulmonaryselectivity of
this effect is conferred bythe rapid reaction of NO with
oxyhemoglobinto produce methemoglobin. Toxicity ofNO may result
from direct inhibitoryeffects on platelet function, or via
itsproducts and reactive metabolites,including methemoglobin,
nitrogen dioxide,and peroxynitrite.14–20 At the dose rangeapplied
clinically (# 20 ppm), iNO rarelycauses clinically significant
bleeding, orleads to potentially toxic levels of
eithermethemoglobin or nitrogen dioxide. Norhas iNO been
demonstrated to increaseperoxynitrite formation in the lungs or
othertissues of human newborns.13 However, thepotential for such
effects and the fact thatiNO is an exceptionally
resource-intensivetherapy, argues for administering iNOjudiciously,
at the lowest effective doseand for the shortest time possible.
Despiteapproval being restricted to term andnear-term infants with
PPHN, use in pretermneonates with HRF21 and in neonates with
conditions other than HRF22–25 has beensteadily increasing,
despite authoritativerecommendations to the contrary.25–28 Atbest,
such practices have major economicconsequences; at worst, have the
potentialto cause harm. Lack of adherence toguidelines relating to
commencement andweaning of iNO therapy represents anotherpractice
with major economic and patientsafety implications29; however,
compliancewith guidelines relating to iNO use hasnot been
previously examined in the NICUsetting.
Stewardship programs are systematicinterventions aimed at
improving adherenceto protocols, promoting better practices,and/or
reducing costs. Stewardshipprograms to reduce antimicrobial use
arenow common30 and programs targetingblood products,31 pain, and
adverse druginteractions32 are also reported. Suchprograms have
been successful at reducingvariations in medical care that stem
fromhuman- and system-related causes.Motivated by a 65% increase in
utilization ofiNO in our institution from the beginning tothe end
of fiscal years 2009–2011, weaudited our iNO use across the
hospital andobserved significant variation in weaningpractices
leading to a longer duration of iNOtherapy than recommended by
institutionalguidelines. After consultation with keystakeholders
(physicians and respiratorytherapists), we instituted a
hospital-wideiNO stewardship program in an effort toreduce
unintended variations in practice.The objective of this study was
to determinewhether the introduction of stewardshipinfluenced iNO
utilization and weaningpractices in the NICU. Specifically,
wesought to determine whether stewardshipled to improved compliance
with our unit-specific weaning guideline, thus leading toreduced
hours of iNO per course oftreatment.
METHODSStudy Design
We performed a combined retrospectiveand prospective cohort
study using adeidentified data set. The Quality and RiskManagement
Department at The Hospital forSick Children approved this study as
aquality improvement project.
Population and Setting
The Hospital for Sick Children is a majorpediatric referral
center serving south-central Ontario, Canada, with 3 intensivecare
units (neonatal, pediatric, andcardiac). The NICU is a 34-bed
(average dailycensus 5 36) quaternary outborn unit with700 to 750
admissions annually within aregionalized tertiary and
quaternaryneonatal complex serving ∼80 000 deliveriesannually. All
neonates requiring, orpotentially requiring, tertiary-level
neonatalcare are retrieved by a dedicated transportteam consisting
primarily of nurses andrespiratory therapists, but also
physicians.Throughout the period of study, iNO wasinstituted only
on attending physician orderand commencement and weaning of iNOwere
conducted by respiratory therapistsunder the auspices of a
unit-specificguideline. Patients potentially requiringECMO were
transferred to the PICU. Thecurrent study included all
neonatesadmitted to our NICU from Apri1 1, 2011, toMarch 31, 2015,
who received iNO initiatedon transport or after admission to
theNICU. Infants with major congenital heartdisease were excluded.
The study periodwas divided into 2 epochs: a prestewardshipepoch
(April 1, 2011–March 31, 2013) anda poststewardship epoch (April
1,2013–March 31, 2015).
Data Extraction and Analysis
In the prestewardship epoch, weretrospectively identified all
patients whoreceived iNO by searching the medicationsand
respiratory support tables recorded inour electronic charting
software (CIMS,Allscripts Sunrise Clinical Care, Richmond,British
Columbia, Canada) for the term“nitric oxide.” Chart data collected
for eachpatient included sex, gestational age, andweight at
initiation of iNO, underlyingclinical problem leading to initiation
of iNO,place of initiation of iNO and outcomes,including the need
for ECMO or death.Deidentified data were entered into tablesthat
were subsequently queried for qualityimprovement purposes. The
total durationof iNO therapy was determined bysubtracting the age
(to the nearest hour)at which iNO was initiated from the age (tothe
nearest hour) at which iNO was
608 ELMEKKAWI et al
by guest on June 29, 2021www.aappublications.org/newsDownloaded
from
-
discontinued. The age (to the nearest hour)at which the patient
reached 5 ppm wasused to calculate hours for initial wean(from
maximum dose – 5 ppm) andhours for final wean (from 5 ppm
–discontinuation). Use of iNO wasconsidered off-label if
gestational age atinitiation was ,35 completed weeks,postnatal age
was .14 days, or if iNOwas used for conditions other than
HRF.Patients transferred from the NICU to thePICU for consideration
of ECMO or whodied in the NICU while on iNO wereexcluded from
analyses of iNO weaningtimes. In the poststewardship epoch,patients
commenced on iNO were identifiedand data (as above) were
recordedprospectively on a dedicated data form thatwas subsequently
transcribed into adeidentified table. Comparisons betweenepochs
were conducted by Student’s t test,Mann-Whitney U test or x2, as
appropriate,using Sigma Plot (version 12.5, SyStatSoftware, San
Jose, CA). A P value of , .05was considered statistically
significant.To demonstrate changes in the outcomesmeasure (iNO use)
and in process measures(compliance rate), process control
chartswere used. An X (individual) chart revealingmonthly iNO use
as continuous measureddata. For protocol compliance, a P chartwas
used for proportion of conformitiesin a changing sample size.
Analysis ofstatistical process control charts was basedon the
Institute for Healthcare Improvementrules defining special cause
variations.33
Stewardship and GuidelineDevelopment Process
An iNO stewardship program was launchedat The Hospital for Sick
Children as ahospital-wide initiative on April 1, 2013,which
coincided with the release of arevised institutional guideline for
iNO use inthe NICU. The NICU guideline was revised aspart of a
process engaging key stakeholders(attending medical staff and
respiratorytherapists) that included presentation ofaudit data
highlighting practice variation induration on maximum dose of iNO
andweaning intervals, consultation to ensureuniversal buy-in to the
revised guideline anda description of monitoring and
prospectivedata collection as part of the stewardship
process. Substantive changes to the revisedguideline were few,
but included thefollowing: (1) consideration of iNO inpatients with
an oxygenation index of 15 to20 (the previous guideline
recommended$20), (2) recommendations to optimize pHand lung
recruitment before commencingiNO (not stated in the previous
guideline),(3) a recommendation to avoid any changesin therapy
while response to iNO was beingevaluated (not stated in the
previousguideline), (4) inclusion of an explicitstatement that iNO
should be discontinued ifno response is observed within 1 hour
(theprevious guideline simply stated that it ispossible to abruptly
discontinue iNO within1 hour of commencement), and (5) theprovision
of supplemental flow charts as avisual aid in guiding the initial
andsubsequent weans (not present in theprevious guideline; see Figs
1 and 2). Thestewardship process began when initiationof iNO
therapy, documented in thecomputerized chart, alerted the
primaryand supervising researchers, who with therespiratory
therapist/s, followed each caseuntil iNO therapy was discontinued.
Theresponsible respiratory therapist managedthe initiation and
weaning of iNO accordingto the guideline, in communication with
themedical team, and recorded the data. AlliNO-treated patients
were captured andfollowed during the poststewardship period.
The stewardship committee was led byrespiratory therapists and
includedphysician leads and clinical fellows from theNICU and the
PICU/Cardiac critical care unit.Over the 2-year period of study,
thecommittee met monthly to review iNO usagedata over the preceding
month. Respiratorytherapists collected data for each patient oniNO
at the bedside and total weekly hourswas crosschecked against
downloadedusage data from the iNO delivery devices. Allinstances of
iNO use over the precedingmonth were reviewed by the
committeechair, with a particular focus on theindications for use
of iNO and the durationof iNO therapy in each case. Compliant
usesof iNO were defined as dose and duration ofiNO therapy given in
accordance with theguideline, regardless of indication.Treatment
courses where initial dose iNOwas continued beyond 1 hour, despite
a lack
of response, or where weaning did notoccur within the
recommended time frame,despite meeting oxygenation criteria,
wereconsidered noncompliant. In cases wherethe indication for use
of iNO wasambiguous, or where therapy wasnoncompliant with the
guideline for reasonsthat were not clear at the time of themeeting,
a chart review was undertaken,which was followed if necessary by
adiscussion between the stewardshipphysician and the attending
physician. Newinformation derived from the chart reviewand
discussion was recorded in the patientdata sheet. All members of
the committeeregularly interacted with medical staff,trainees, and
respiratory therapists fromtheir respective intensive care units
toensure ongoing awareness of the guidelineand to review the
criteria forcommencement and weaning of iNO. Generaldata on trends
in iNO use were presented tothe attending staff every 6 months at
aminimum, which included discussions oncommon reasons for
noncompliance withthe guideline. The committee also followedtotal
hours of usage, targeting a yearlyhospital-wide reduction from an
average of11 938 hours annually in the 2 yearsprestewardship, to
7600 hours annually.Target hours were agreed upon with
allstakeholders at the beginning of theprocess.
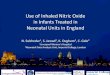
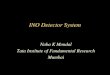
Flow charts summarizing the revisedguidelines are shown in Fig 1
(institution ofiNO) and Fig 2 (weaning and cessationof iNO).
Throughout the period of study(April 1, 2011–March 31, 2015),
theguidelines had not changed regardingindications for iNO therapy
(no gestationalage or postnatal age restriction wasspecified),
maximum dose, criteria forweaning, or weaning intervals. As shown
inFigs 1 and 2, the range for the duration ofiNO therapy in a
patient responding toiNO and persistently meeting criteria
forweaning is 6 hours for the initial wean(20–5 ppm) and 5 to 10
hours for weaningfrom 5 ppm to discontinuation (total timefrom
commencement is 11–16 hours).
RESULTS
Hospital-wide iNO use decreased from23 876 hours (n 5 212
courses of therapy)
HOSPITAL PEDIATRICS Volume 6, Issue 10, October 2016 609
by guest on June 29, 2021www.aappublications.org/newsDownloaded
from
-
in the 2 years prestewardship (April2011–March 2013) to 13 663
hours (n 5 209courses of therapy) in the 2 yearspoststewardship
(April 2013–March 2015).In the NICU, 89 infants received 90
coursesof iNO in the prestewardship epoch and65 infants received 65
courses of iNO inthe poststewardship epoch. Three patientswere
excluded due to a diagnosis of majorcongenital heart disease: 2 in
the pre- and1 in the poststewardship epoch. Amongthe 88 and 64
courses of treatment,
respectively, total hours of iNO use were5368 hours (23% of
hospital-wide hours)prestewardship and 2540 hours (19%
ofhospital-wide hours) poststewardship.There were no significant
differences inpatient characteristics between epochs(sex,
gestational age, weight, and age atinitiation; Table 1) or in
outcomes (need forECMO or death; Table 1). The percentage
ofpatients in whom iNO was initiated ontransport or received
off-label was alsosimilar between epochs (Table 1). Off-label
iNO use was, in the majority of cases, relatedto prematurity
(50% and 61% in pre- andpostepochs, respectively), postnatal age
(13%and 17%, respectively), both prematurity andpostnatal age (27%
and 17%, respectively),and indications other than HRF (10% and
5%,respectively). The most common reason forcommencing iNO other
than HRF was severepulmonary hypertension associated withright
ventricular dysfunction, diagnosed byechocardiography. The mean and
mediancompleted weeks’ gestational age among
FIGURE 1 Flowchart summarizing recommendations on initiation of
iNO, determination of response, safety monitoring, and initiation
of weaning.ABG, arterial blood gas; CXR, chest x-ray; FIO2,
fraction of inspired oxygen; Hgb, hemoglobin; MRP, most-responsible
physician; OI,oxygenation index; SpO2, pulse oxygen saturation.
610 ELMEKKAWI et al
by guest on June 29, 2021www.aappublications.org/newsDownloaded
from
-
premature infants receiving off-label iNO was30 weeks (range
24–34 weeks) in bothepochs. No patients were treated
withalternative pulmonary vasodilators beforeiNO, none were exposed
to iNO atconcentrations higher than 20 ppm, andnone required
sildenafil or other pulmonaryvasodilators to facilitate weaning off
iNO.There was no significant change in mortalityor ECMO usage
between the groups.
Analyses of total iNO hours per patient, timeto initial wean,
and time from initial wean todiscontinuation between epochs are
shownin Table 2. Analyses of weaning times
included 75 (85%) patients from theprestewardship epoch and 49
(77%)patients from the poststewardship epoch. Ofthe 13 patients
excluded prestewardship,3 were transferred to the PICU
forconsideration of ECMO (2 received ECMO)and 10 died in the NICU
while on iNO. Of the15 patients excluded poststewardship,8 were
transferred to the PICU forconsideration of ECMO (5 received
ECMO)and 7 died in the NICU while on iNO. Themost common reason for
noncompliancewith the weaning guideline was
persistentechocardiographic evidence of severe
pulmonary hypertension with or withoutright ventricular
dysfunction. Comparingweaning times between epochs, weobserved a
significant reduction in totalhours on iNO per course of
treatmentpoststewardship, whether patients wereexcluded from
analyses. We also observed asignificant decrease in iNO hours
perpatient from maximum dose to initial wean(to 5 ppm) and in hours
from 5 ppm todiscontinuation of iNO in thepoststewardship epoch
(Table 2). As shownin Fig 3A, there was a persistent reductionof
iNO usage from 224 hours/month to
FIGURE 2 Flowchart summarizing weaning recommendations for iNO.
FIO2, fraction of inspired oxygen; SpO2, pulse oxygen
saturation.
HOSPITAL PEDIATRICS Volume 6, Issue 10, October 2016 611
by guest on June 29, 2021www.aappublications.org/newsDownloaded
from
-
106 hours/month between the pre- andpoststewardship eras. As
shown in Fig 3B,monthly percentage compliance with theguideline
increased from a mean of 3.2% ofiNO courses prestewardship to
25.8%poststewardship.
DISCUSSION
Despite there being high quality evidenceto inform use of iNO in
neonates, ourguideline was being frequently ignored.Concerns
surrounding the costly, andperhaps unnecessary, use of iNO led us
tore-examine our guideline and to developstrategies to improve
adherence. Ourfindings demonstrated that implementationof an iNO
stewardship program improvedadherence to guidelines, leading
tomeaningful reductions in total and per-patient hours of iNO use.
To our knowledge,the current study is the first to examineadherence
to evidence-based guidelines inthe context of iNO therapy in the
NICU andthe first to describe the impact of astewardship program on
utilizationpatterns of iNO. Major drivers of change in
iNO utilization likely included an enhancedawareness of the
guideline by front linestaff, increased vigilance by
respiratorytherapists regarding opportunities forweaning, the
observer (Hawthorne) effectand unmeasured cointerventions
(eg,arrival of new staff or discussion ofrational use of iNO at
conferences, etc),which modified physician behavior.
Clinical practice guidelines are widelyregarded as key to
reducing practice variationand improving the quality of care.29,33
However,to be effective, guidelines must be updatedregularly to
reflect current evidence or expertopinion, must be minimally
controversial toensure maximum buy-in, and must beimplemented in an
environment characterizedby sustained communication and
vigilance.The stewardship model has been usedsuccessfully in the
pediatric setting topromote safe and evidence-based use
ofantimicrobial agents.34 Key elements of ouriNO stewardship
program included anidentified staff physician and
trainee,widespread dissemination of evidence-based
practice guidelines that were approved by allmembers of the
medical and respiratorytherapy team, detailed prospective
datacollection, setting targets for total yearlyutilization,
regular reviews of iNO use by aninterprofessional stewardship
committee,discussion of specific cases with theattending physician,
and feedback on generaltrends in iNO use to NICU staff.
Our guidelines did not set limits ongestational age for
treatment with iNO.Despite this, our rate of off-label use
forprematurity was less than recentlypublished rates, which were as
high as50%.21 This disparity likely reflectedinherent differences
in our outbornpopulation, which is made uppredominantly of complex
term and near-term infants, rather than attitudesdiscouraging use
of iNO in the verypreterm. Indeed, the pathophysiology ofHRF in the
preterm may be identical to theterm infant with PPHN, making the
use ofiNO a logical and potentially usefulextension of therapy,
thoughresponsiveness may diminish withdecreasing gestational age.35
Similar toterm infants with PPHN, clinical trialsexamining effects
of iNO for HRF inpremature infants have confirmed short-term
improvements in oxygenation, but noreduction in mortality.36–40 In
the absence ofspecific evidence to guide iNO therapy inthis
population, our guidelines for startingdose and weaning of iNO were
the same,regardless of gestational age.
A significant minority of our iNO-treatedinfants in both epochs
did not have HRF. Inmost cases, iNO was instituted based
onechocardiographic evidence of chronicpulmonary hypertension with
associatedright ventricular dysfunction. Most suchcases were
considered noncompliant inthe current study, due to avoidance
ofweaning until repeat evaluation byechocardiogram, which greatly
prolongediNO therapy. In patients with poorlyresponsive pulmonary
hypertensionand/or right ventricular dysfunction,prolonged
treatment with iNO may bejustified; however, use of iNO for
suchindications is difficult to incorporate intoweaning guidelines,
particularly in a
TABLE 1 Patient Demographics and Outcomes
Prestewardship Poststewardship P
Number of patients 87 64 NA
Sex F/M: 37/50 F/M: 31/33 .55
Gestational age in completed weeks at initiationof iNOa
38 (33–40) 38 (34–40) .88
Day of life at initiation of iNOa 2 (1–5) 2 (2–9) .083
Grams body weight at initiation of iNOa 3080 (1753–3675) 3020
(1931–3500) .75
Off-label use (%) 30 (34) 23 (36) .95
iNO initiated before admission (%) 32 (36) 29 (45) .35
ECMO (%) 2 (2) 5 (8) .11
Died (%) 23 (26) 14 (22) .52
NA, not applicable.a Data are presented as median (interquartile
range).
TABLE 2 iNO Utilization
Prestewardship Poststewardship P
Courses of iNO treatment given 88 64 NA
Total iNO hours 5368 2540 NA
Hours/course,a all patients 47 (23–66) 20 (13–46) ,.001
Hours/course,a with exclusionsb 49 (25–66) 22 (14–46) ,.001
Hours from maximum dose to 5 ppma,b 28 (12–51) 9 (5–26) ,.01
Hours from 5 ppm to discontinuationa,b 14 (7–24) 8 (6–15)
,.05
NA, not applicable.a Data are presented as median (interquartile
range).b Patients who died on iNO or were transferred to the PICU
for consideration of ECMO were excluded.
612 ELMEKKAWI et al
by guest on June 29, 2021www.aappublications.org/newsDownloaded
from
-
population in which iNO is usedpredominantly for oxygenation
failure. Ourcurrent approach to such cases is to use iNOas a bridge
to other therapies,41 if required,at the lowest dose at which a
response isobserved (generally 5 or 10 ppm), while
consulting with experts in themanagement of pulmonary
hypertension.
Improving Quality
This study evaluated a process that improvedcost-effectiveness
by reducing unnecessary
exposure to a medication, without evidence ofharm, thus
enhancing quality of health care.42
Limitations of the Study
Data from the prestewardship epoch wascollected retrospectively,
which has many
FIGURE 3 Statistical process control charts. A, X-chart
displaying hours of iNO use per month. The green line represents
the process mean. Thebroken red line represents the upper control
limit (3 SDs from the mean). B, P-chart revealing percentage of iNO
courses each monthgiven in compliance with the guideline. The blue
line and dots represent the compliance rate with the iNO guideline
(in percent) for eachmonth. The continuous green line represents
the compliance rate mean for each epoch. The pale red line
represents the upper controllimit (3 SDs from the mean).
HOSPITAL PEDIATRICS Volume 6, Issue 10, October 2016 613
by guest on June 29, 2021www.aappublications.org/newsDownloaded
from
-
inherent limitations. In particular, it wasfrequently
challenging or impossible todetermine the reasons behind patterns
ofiNO utilization that deviated greatly from ourguideline. We
observed no significantchange in proportion of infants dying
orreceiving ECMO between the pre- andpoststewardship eras,
suggesting a lack ofharm related to decreased iNO use.However, we
did not prospectively collectdata on other possible consequences
ofdecreased iNO utilization, including changesin patterns of muscle
relaxant, narcotic andsedative use, or on duration of
invasivemechanical ventilation or length of hospitalstay. This work
was conducted in a singlequaternary outborn NICU populated
byinfants across the gestational agespectrum, among which there
wassignificant complexity and heterogeneity;this has potential
implications forinterpretation of outcomes reflecting safety(use of
ECMO or death), at least in the short-term. Due to the
observational design of thisstudy, we cannot be certain that
thechanges in iNO utilization over time wereprimarily due to the
introduction ofstewardship, rather than a secular trend.A major
factor in favor of an importantimpact of stewardship on iNO
utilizationpatterns was that our guideline, and themethod by which
iNO was prescribed andmonitored, did not change
substantivelythroughout the period of study.
Generalizability and Spread
Our experience suggests that thestewardship model can be
implemented inany NICU. Toward this goal, national
Canadianguidelines guiding practice in neonates werecollaboratively
developed and promulgatedunder the auspices of the
CanadianAssociation of Pediatric Health Centres.43
A Canadian Association of Pediatric HealthCentres-sponsored
national iNO stewardshipnetwork is currently in the planning
phase.
CONCLUSIONS
Variation in the use of iNO leading tounnecessary prolongation
of therapy carriesa significant economic burden and haspotential to
cause harm. Implementation of astewardship program improved
adherenceto evidence-based guidelines, leading to
significant and important decreases in totaland per-patient iNO
use in our NICU. Weconclude that the stewardship model hasutility
in reducing practice variation in iNOuse in the NICU setting and
has the potentialto generate new knowledge that will informfuture
practice.
REFERENCES
1. Farrow KN, Fliman P, Steinhorn RH. Thediseases treated with
ECMO: focus onPPHN. Semin Perinatol. 2005;29(1):8–14
2. Steinhorn RH, Millard SL, Morin FC III.Persistent pulmonary
hypertension ofthe newborn. Role of nitric oxide andendothelin in
pathophysiology andtreatment. Clin Perinatol.
1995;22(2):405–428
3. Kinsella JP, Neish SR, Shaffer E, AbmanSH. Low-dose
inhalation nitric oxide inpersistent pulmonary hypertension ofthe
newborn. Lancet. 1992;340(8823):819–820
4. Roberts JD, Polaner DM, Lang P, ZapolWM. Inhaled nitric oxide
in persistentpulmonary hypertension of the newborn.Lancet.
1992;340(8823):818–819
5. Neonatal Inhaled Nitric Oxide StudyGroup. Inhaled nitric
oxide in full-termand nearly full-term infants with
hypoxicrespiratory failure. N Engl J Med.1997;336(9):597–604
6. Roberts JD Jr, Fineman JR, Morin FC III,et al; The Inhaled
Nitric Oxide StudyGroup. Inhaled nitric oxide andpersistent
pulmonary hypertensionof the newborn. N Engl J Med.
1997;336(9):605–610
7. Clark RH, Kueser TJ, Walker MW, et al;Clinical Inhaled Nitric
Oxide ResearchGroup. Low-dose nitric oxide therapy forpersistent
pulmonary hypertension ofthe newborn. N Engl J Med.
2000;342(7):469–474
8. Day RW, Lynch JM, White KS, Ward RM.Acute response to inhaled
nitric oxide innewborns with respiratory failure andpulmonary
hypertension. Pediatrics.1996;98(4 pt 1):698–705
9. Inhaled nitric oxide in term and near-term infants:
neurodevelopmental
follow-up of the neonatal inhaled nitricoxide study group
(NINOS). J Pediatr.2000;136(5):611–617
10. Clark RH, Huckaby JL, Kueser TJ, et al;Clinical Inhaled
Nitric Oxide ResearchGroup. Low-dose nitric oxide therapy
forpersistent pulmonary hypertension:1-year follow-up. J Perinatol.
2003;23(4):300–303
11. Hintz SR, Van Meurs KP, Perritt R, PooleWK, Das A, Stevenson
DK, et al.Neurodevelopmental outcomes ofpremature infants with
severerespiratory failure enrolled in arandomized controlled trial
ofinhaled nitric oxide. J Pediatr. 2007;151(1):16–22
12. Konduri GG, Vohr B, Robertson C, et al;Neonatal Inhaled
Nitric Oxide StudyGroup. Early inhaled nitric oxide therapyfor term
and near-term newborn infantswith hypoxic respiratory
failure:neurodevelopmental follow-up. J
Pediatr.2007;150(3):235–240.e1
13. Finer NN, Barrington KJ. Nitric oxide forrespiratory failure
in infants born at ornear term. Cochrane Database Syst Rev.2006;
(4):CD000399
14. Weinberger B, Laskin DL, Heck DE, LaskinJD. The toxicology
of inhaled nitric oxide.Toxicol Sci. 2001;59(1):5–16
15. Cheung PY, Salas E, Etches PC,Phillipos E, Schulz R,
Radomski MW.Inhaled nitric oxide and inhibition ofplatelet
aggregation in critically illneonates. Lancet.
1998;351(9110):1181–1182
16. George TN, Johnson KJ, Bates JN, SegarJL. The effect of
inhaled nitric oxidetherapy on bleeding time and
plateletaggregation in neonates. J Pediatr. 1998;132(4):731–734
17. Souza JM, Peluffo G, Radi R. Proteintyrosine
nitration–functional alterationor just a biomarker? Free Radic
BiolMed. 2008;45(4):357–366
18. Zou M, Martin C, Ullrich V. Tyrosinenitration as a mechanism
of selectiveinactivation of prostacyclin synthase byperoxynitrite.
Biol Chem. 1997;378(7):707–713
614 ELMEKKAWI et al
by guest on June 29, 2021www.aappublications.org/newsDownloaded
from
-
19. Beckman JS, Koppenol WH. Nitric oxide,superoxide, and
peroxynitrite: the good,the bad, and ugly. Am J Physiol. 1996;271(5
pt 1):C1424–C1437
20. Beckman JS, Beckman TW, Chen J,Marshall PA, Freeman BA.
Apparenthydroxyl radical production byperoxynitrite: implications
forendothelial injury from nitric oxide andsuperoxide. Proc Natl
Acad Sci USA.1990;87(4):1620–1624
21. Ellsworth MA, Harris MN, Carey WA,Spitzer AR, Clark RH.
Off-label use ofinhaled nitric oxide after release of NIHconsensus
statement. Pediatrics. 2015;135(4):643–648
22. Van Meurs KP, Wright LL, Ehrenkranz RA,et al; Preemie
Inhaled Nitric Oxide Study.Inhaled nitric oxide for
prematureinfants with severe respiratory failure.N Engl J Med.
2005;353(1):13–22
23. Ballard RA, Truog WE, Cnaan A, et al; NOCLD Study Group.
Inhaled nitric oxide inpreterm infants undergoing
mechanicalventilation. N Engl J Med. 2006;355(4):343–353
24. Mercier JC, Hummler H, Durrmeyer X,et al; EUNO Study Group.
Inhaled nitricoxide for prevention of bronchopulmonarydysplasia in
premature babies (EUNO): arandomised controlled trial. Lancet.
2010;376(9738):346–354
25. Askie LM, Ballard RA, Cutter GR, et al;Meta-analysis of
Preterm Patients onInhaled Nitric Oxide Collaboration.Inhaled
nitric oxide in preterm infants:an individual-patient data
meta-analysisof randomized trials. Pediatrics.
2011;128(4):729–739
26. Cole FS, Alleyne C, Barks JD, et al. NIHConsensus
Development Conferencestatement: inhaled nitric-oxide therapyfor
premature infants. Pediatrics. 2011;127(2):363–369
27. Barrington KJ, Finer NN. Inhaled nitricoxide for respiratory
failure in preterminfants. Cochrane Database Syst Rev.2006;
(1):CD000509
28. Kumar P; Committee on Fetus andNewborn; American Academy
ofPediatrics. Use of inhaled nitric oxide inpreterm infants.
Pediatrics. 2014;133(1):164–170
29. Simsic JM, Harrison S, Evans L, McCleadR, Teske D; Institute
of HealthcareImprovement. Reducing variation in theuse of inhaled
nitric oxide. Pediatrics.2014;133(6). Available at:
www.pediatrics.org/cgi/content/full/133/6/e1753
30. Coulter S, Merollini K, Roberts JA, GravesN, Halton K. The
need for cost-effectiveness analyses of antimicrobialstewardship
programmes: A structuredreview. Int J Antimicrob Agents.
2015;46(2):140–149
31. Amerine LB, Chen SL, Daniels R, Key N,Eckel SF, Savage SW.
Impact of aninnovative blood factor stewardshipprogram on drug
expense and patientcare. Am J Health Syst Pharm.
2015;72(18):1579–1584
32. Ghafoor VL, Phelps P, Pastor J.Implementation of a pain
medicationstewardship program. Am J Health SystPharm.
2013;70(23):2070–2075
33. Benneyan JC, Lloyd RC, Plsek PE.Statistical process control
as a tool forresearch and healthcare improvement.Qual Saf Health
Care. 2003;12(6):458–464
34. Woolf SH. Practice guidelines: a newreality in medicine. I.
Recentdevelopments. Arch Intern Med. 1990;150(9):1811–1818
35. Di Pentima MC, Chan S. Impact ofantimicrobial stewardship
program onvancomycin use in a pediatric teachinghospital. Pediatr
Infect Dis J. 2010;29(8):707–711
36. Kumar VH, Hutchison AA,Lakshminrusimha S, Morin FC III,
WynnRJ, Ryan RM. Characteristics ofpulmonary hypertension in
pretermneonates. J Perinatol. 2007;27(4):214–219
37. Subhedar NV, Ryan SW, Shaw NJ. Openrandomised controlled
trial of inhalednitric oxide and early dexamethasone inhigh risk
preterm infants. Arch Dis ChildFetal Neonatal Ed.
1997;77(3):F185–F190
38. Kinsella JP, Walsh WF, Bose CL, et al.Inhaled nitric oxide
in prematureneonates with severe hypoxaemicrespiratory failure: a
randomisedcontrolled trial. Lancet. 1999;354(9184):1061–1065
39. Truffert P, Llado-Paris J, Mercier JC,Dehan M, Bréart G;
Franco-Belgian iNOStudy Group. Early inhaled nitric oxide
inmoderately hypoxemic preterm andterm newborns with RDS: the
RDSsubgroup analysis of the Franco-BelgianiNO Randomized Trial. Eur
J Pediatr.2003;162(9):646–647
40. Schreiber MD, Gin-Mestan K, Marks JD,Huo D, Lee G, Srisuparp
P. Inhaled nitricoxide in premature infants with therespiratory
distress syndrome. N Engl JMed. 2003;349(22):2099–2107
41. Kahveci H, Yilmaz O, Avsar UZ, et al. Oralsildenafil and
inhaled iloprost in thetreatment of pulmonary hypertension ofthe
newborn. Pediatr Pulmonol. 2014;49(12):1205–1213
42. Crossing the Quality Chasm. A NewHealth System for the 21st
Century.Washington, DC: National AcademyPress; 2001
43.
http://ken.caphc.org/xwiki/bin/view/PaediatricPracticeGuidelinesCollaborative/CAPHC1Guidelines1for1Inhaled1Nitric1Oxide1in1Neonates%3A11Dosing,1Administration1and1Weaning
HOSPITAL PEDIATRICS Volume 6, Issue 10, October 2016 615
by guest on June 29, 2021www.aappublications.org/newsDownloaded
from
http://www.pediatrics.org/cgi/content/full/133/6/e1753http://www.pediatrics.org/cgi/content/full/133/6/e1753http://ken.caphc.org/xwiki/bin/view/PaediatricPracticeGuidelinesCollaborative/CAPHC+Guidelines+for+Inhaled+Nitric+Oxide+in+Neonates%3A++Dosing,+Administration+and+Weaninghttp://ken.caphc.org/xwiki/bin/view/PaediatricPracticeGuidelinesCollaborative/CAPHC+Guidelines+for+Inhaled+Nitric+Oxide+in+Neonates%3A++Dosing,+Administration+and+Weaninghttp://ken.caphc.org/xwiki/bin/view/PaediatricPracticeGuidelinesCollaborative/CAPHC+Guidelines+for+Inhaled+Nitric+Oxide+in+Neonates%3A++Dosing,+Administration+and+Weaninghttp://ken.caphc.org/xwiki/bin/view/PaediatricPracticeGuidelinesCollaborative/CAPHC+Guidelines+for+Inhaled+Nitric+Oxide+in+Neonates%3A++Dosing,+Administration+and+Weaninghttp://ken.caphc.org/xwiki/bin/view/PaediatricPracticeGuidelinesCollaborative/CAPHC+Guidelines+for+Inhaled+Nitric+Oxide+in+Neonates%3A++Dosing,+Administration+and+Weaninghttp://ken.caphc.org/xwiki/bin/view/PaediatricPracticeGuidelinesCollaborative/CAPHC+Guidelines+for+Inhaled+Nitric+Oxide+in+Neonates%3A++Dosing,+Administration+and+Weaninghttp://ken.caphc.org/xwiki/bin/view/PaediatricPracticeGuidelinesCollaborative/CAPHC+Guidelines+for+Inhaled+Nitric+Oxide+in+Neonates%3A++Dosing,+Administration+and+Weaninghttp://ken.caphc.org/xwiki/bin/view/PaediatricPracticeGuidelinesCollaborative/CAPHC+Guidelines+for+Inhaled+Nitric+Oxide+in+Neonates%3A++Dosing,+Administration+and+Weaninghttp://ken.caphc.org/xwiki/bin/view/PaediatricPracticeGuidelinesCollaborative/CAPHC+Guidelines+for+Inhaled+Nitric+Oxide+in+Neonates%3A++Dosing,+Administration+and+Weaninghttp://ken.caphc.org/xwiki/bin/view/PaediatricPracticeGuidelinesCollaborative/CAPHC+Guidelines+for+Inhaled+Nitric+Oxide+in+Neonates%3A++Dosing,+Administration+and+Weaninghttp://ken.caphc.org/xwiki/bin/view/PaediatricPracticeGuidelinesCollaborative/CAPHC+Guidelines+for+Inhaled+Nitric+Oxide+in+Neonates%3A++Dosing,+Administration+and+Weaninghttp://ken.caphc.org/xwiki/bin/view/PaediatricPracticeGuidelinesCollaborative/CAPHC+Guidelines+for+Inhaled+Nitric+Oxide+in+Neonates%3A++Dosing,+Administration+and+Weaninghttp://ken.caphc.org/xwiki/bin/view/PaediatricPracticeGuidelinesCollaborative/CAPHC+Guidelines+for+Inhaled+Nitric+Oxide+in+Neonates%3A++Dosing,+Administration+and+Weaninghttp://ken.caphc.org/xwiki/bin/view/PaediatricPracticeGuidelinesCollaborative/CAPHC+Guidelines+for+Inhaled+Nitric+Oxide+in+Neonates%3A++Dosing,+Administration+and+Weaninghttp://ken.caphc.org/xwiki/bin/view/PaediatricPracticeGuidelinesCollaborative/CAPHC+Guidelines+for+Inhaled+Nitric+Oxide+in+Neonates%3A++Dosing,+Administration+and+Weaning
-
DOI: 10.1542/hpeds.2016-0003 originally published online
September 6, 2016; 2016;6;607Hospital Pediatrics
Michael Finelli, Asaph Rolnitsky and Robert P. JankovAmir
Elmekkawi, Kiran More, Jennifer Shea, Christina Sperling, Zelia Da
Silva,
Impact of Stewardship on Inhaled Nitric Oxide Utilization in a
Neonatal ICU
ServicesUpdated Information &
http://hosppeds.aappublications.org/content/6/10/607including
high resolution figures, can be found at:
Supplementary Material Supplementary material can be found
at:
Referenceshttp://hosppeds.aappublications.org/content/6/10/607#BIBLThis
article cites 37 articles, 10 of which you can access for free
at:
Subspecialty Collections
rovement_subhttp://www.hosppeds.aappublications.org/cgi/collection/quality_impQuality
Improvement_subhttp://www.hosppeds.aappublications.org/cgi/collection/neonatologyNeonatologyrn_infant_subhttp://www.hosppeds.aappublications.org/cgi/collection/fetus:newboFetus/Newborn
Infanton:practice_management_subhttp://www.hosppeds.aappublications.org/cgi/collection/administratiAdministration/Practice
Managementfollowing collection(s): This article, along with others
on similar topics, appears in the
Permissions & Licensing
mlhttp://www.hosppeds.aappublications.org/site/misc/Permissions.xhtin
its entirety can be found online at: Information about reproducing
this article in parts (figures, tables) or
Reprintshttp://www.hosppeds.aappublications.org/site/misc/reprints.xhtmlInformation
about ordering reprints can be found online:
by guest on June 29, 2021www.aappublications.org/newsDownloaded
from
http://http://hosppeds.aappublications.org/content/6/10/607http://hosppeds.aappublications.org/content/6/10/607#BIBLhttp://www.hosppeds.aappublications.org/cgi/collection/administration:practice_management_subhttp://www.hosppeds.aappublications.org/cgi/collection/administration:practice_management_subhttp://www.hosppeds.aappublications.org/cgi/collection/fetus:newborn_infant_subhttp://www.hosppeds.aappublications.org/cgi/collection/fetus:newborn_infant_subhttp://www.hosppeds.aappublications.org/cgi/collection/neonatology_subhttp://www.hosppeds.aappublications.org/cgi/collection/neonatology_subhttp://www.hosppeds.aappublications.org/cgi/collection/quality_improvement_subhttp://www.hosppeds.aappublications.org/cgi/collection/quality_improvement_subhttp://www.hosppeds.aappublications.org/site/misc/Permissions.xhtmlhttp://www.hosppeds.aappublications.org/site/misc/Permissions.xhtmlhttp://www.hosppeds.aappublications.org/site/misc/reprints.xhtml
-
DOI: 10.1542/hpeds.2016-0003 originally published online
September 6, 2016; 2016;6;607Hospital Pediatrics
Michael Finelli, Asaph Rolnitsky and Robert P. JankovAmir
Elmekkawi, Kiran More, Jennifer Shea, Christina Sperling, Zelia Da
Silva,
Impact of Stewardship on Inhaled Nitric Oxide Utilization in a
Neonatal ICU
http://hosppeds.aappublications.org/content/6/10/607located on
the World Wide Web at:
The online version of this article, along with updated
information and services, is
All rights reserved. Print ISSN: 1073-0397. Park Avenue, Itasca,
Illinois, 60143. Copyright © 2016 by the American Academy of
Pediatrics.Pediatrics is owned, published, and trademarked by the
American Academy of Pediatrics, 345 Hospital Pediatrics is an
official journal of the American Academy of Pediatrics.
Hospital
by guest on June 29, 2021www.aappublications.org/newsDownloaded
from
http://hosppeds.aappublications.org/content/6/10/607