Embed Size (px)
Citation preview

Renal Failure, 33(9): 878–884, (2011)Copyright © Informa Healthcare USA, Inc.ISSN 0886-022X print/1525-6049 onlineDOI: 10.3109/0886022X.2011.605978
CLINICAL STUDY
Impact of Nitric Oxide Synthase Glu298Asp Polymorphismon the Development of End-Stage Renal Disease in Type 2 DiabeticEgyptian Patients
Sahar Saad El-Din Bessa1 and Soha Mohamed Hamdy2
1Department of Internal Medicine, Faculty of Medicine, Tanta University, Tanta, Egypt; 2Department of Chemistry,Division of Biochemistry, Faculty of Science, Fayoum University, Al-Fayoum, Egypt
Abstract
Background: Nitric oxide is an important regulator of renal hemodynamics. This study aimed to investigate the role ofendothelial nitric oxide synthase (eNOS) gene polymorphism in type 2 diabetic patients with end-stage renal disease(ESRD) and to elucidate any alteration of nitric oxide synthase (NOS) activity caused by this polymorphism. Methods:The study included 80 patients with type 2 diabetes of >10 years duration (40 with diabetes-derived ESRD, 40 withoutnephropathy) and 20 healthy controls. Plasma nitrate/nitrite level, and serum NOS activity were measured and eNOSGlu298Asp genotypes were determined. Results: The frequency of Glu/Glu (GG) genotype in diabetics with ESRDwas lower than controls. However, the frequency of Asp/Asp (TT) genotype was increased in diabetics with ESRDas compared to those without nephropathy and controls. Diabetics with ESRD had significantly lower nitrate/nitritelevel and NOS activity than those without nephropathy. Diabetic patients with TT genotype are at a significant risk forESRD. Moreover, subjects carrying TT genotype had lower nitrate/nitrite level and NOS activity than those carryingGG genotype. In diabetics with ESRD, creatinine clearance was positively correlated with both nitrate/nitrite level andNOS activity. Conclusions: These results imply that TT genotype of eNOS may be associated with an increased riskof ESRD in Egyptian type 2 diabetics. It could represent a useful genetic marker to identify diabetics at high risk forthe development of ESRD. However, larger future prospective studies are required to confirm the role of eNOS genepolymorphism in the progression of diabetic nephropathy to ESRD.
Keywords: endothelial nitric oxide synthase, gene polymorphism, end-stage renal disease, type 2 diabetes
INTRODUCTION
Diabetic nephropathy (DN) is one of the most seriouscomplications of diabetes and the most common leadingcause of end-stage renal disease (ESRD). It is char-acterized pathophysiologically by an early phase withglomerular hypertrophy, hyperfiltration, and microal-buminuria that over the course of years leads to anadvanced phase with progressive glomerulosclerosis,proteinuria, and decline in renal function.1
The pathogenesis of DN is still a matter of debatealthough strong evidence suggests that it results froman interaction between susceptibility genes and the dia-betic milieu. Several studies have demonstrated thatDN occurs in familial clusters, suggesting that geneticfactors may contribute to its development in addition
Address correspondence to Sahar Saad El-Din Bessa, Department of Internal Medicine, Faculty of Medicine, Tanta University, Al-GeishStreet, Tanta, Al-Gharbia 31527, Egypt. Tel.: +202 040-3419831; Fax: +202 040-3419831; E-mail: [email protected]
Received 11 April 2011; Revised 12 July 2011; Accepted 12 July 2011
to poor glycemic control.2,3 However, the geneticbackground for the progression of DN to ESRD isstill unclear. A considerable body of evidence ascribesclinical manifestations of DN and their respectivepathophysiological mechanisms to a dysfunction in theendothelial nitric oxide synthase (eNOS)/nitric oxide(NO) system.4–7 Moreover, diabetic mice that lacksthe gene encoding eNOS, develops accelerated kidneydisease that resembles human DN.8,9
NO is derived from the enzymatic action, whichcatalyzes the conversion of L-arginine to NO, gener-ating L-citrulline as a by-product.10 The reaction ismediated by the enzyme nitric oxide synthase (NOS),of which three mammalian isoforms have been iso-lated: neuronal NOS (NOS1), inducible NOS (NOS2),
878
Ren
Fai
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Cas
e W
este
rn R
eser
ve U
nive
rsity
on
10/3
0/14
For
pers
onal
use
onl
y.

NOS Glu298Asp Polymorphism in Type 2 Diabetics with ESRD 879
and endothelial NOS (eNOS or NOS3).11 The effectsof NO are mediated by the activation of guanylatecyclase, resulting in increased levels of cyclic guanosinemonophosphate.
The released NO mediates local vasodilatation andinhibits platelet aggregation, leukocyte adhesion, andvascular smooth muscle cell proliferation.12 In the kid-ney, NO is involved in the regulation of renal plasmaflow, glomerular filtration rate, sodium excretion, extra-cellular fluid volume, and the maintenance of renalstructural integrity.13–15 The important role of NOin the regulation of the hemodynamic and metabolicmilieu in the kidney suggests that an abnormal eNOSactivity due to a genetic mutation could be implicatedand may therefore aggravate renovascular injury in dia-betic patients.16 Recently, several polymorphisms havebeen identified in the eNOS gene, among which is onelocated in exon 7, a G894T substitution that resultsin glutamate to aspartate amino acid change at codon298. This polymorphism has been associated with coro-nary spasm,17 acute myocardial infarction,18 essentialhypertension,19 and carotid atherosclerosis.20 However,the potential link between eNOS gene variants and theprogression of DN has not yet been clarified and theavailable data have been controversial.21,22 Therefore,the aim of the present study was to investigate the roleof eNOS gene polymorphism in type 2 diabetic patientswith ESRD and to elucidate any alteration of NOSactivity caused by this polymorphism.
MATERIALS AND METHODS
SubjectsThis case–control study was conducted on 100 subjects.Eighty type 2 diabetic patients were randomly selectedfrom those attending the Internal Medicine DiabeticClinic and Nephrology Unit at Tanta University Hos-pital from October 2009 to September 2010. All hadbeen diagnosed as having type 2 diabetes (World HealthOrganization criteria) for more than 10 years. They wereclassified into two groups: group 1 included 40 diabeticpatients, 17 men and 23 women, without nephropathy(albuminuria <30 mg/24 h with normal renal function);their mean age (±SD) was 55.4 ± 8.8 years, while themean ± SD of the duration of diabetes was 15.3 ±3.7 years; and group 2 included 40 diabetic patients,21 men and 19 women, with diabetes-derived ESRDwho had persistent proteinuria and creatinine clearanceof <15 mL/min, being in need for hemodialysis (threetimes a week for 4 h). Their mean age (±SD) was58.8 ± 12.5 years, while the mean ± SD of diabetesduration was 19.4 ± 4.2 years. Patients with nondia-betic renal diseases were excluded from the study bycomplete urine analysis and medical records (micro-scopic or macroscopic hematuria, abnormal urinarysediment, urinary tract infection, and past history ofglomerulonephritis or nephro-ureterolithiasis). Patients
with microalbuminuria or intermittent proteinuria werealso excluded from the study.
Twenty healthy age- and sex-matched volunteers(10 men and 10 women) with a mean age (±SD) of54.1 ± 8.3 years, with no clinical signs of vascular orrenal disease and no family history of diabetes or renaldisease were recruited for participation as control sub-jects. They were selected from medical and paramedicalstaff and from blood donors in Tanta University Hos-pital. The study was approved by the scientific andethics committees of the Tanta University Hospital,Tanta University, Tanta, Egypt, and informed con-sent was obtained from all subjects prior to the startof this study. All cases included in this study weresubjected to careful history taking, complete clinicalexamination, biochemical investigations, and abdominalultrasonography.
Biochemical AssayAn early-morning urine sample was collected from eachsubject for complete urine analysis and detection ofmicroalbuminuria with a Micral test.23 A 24 h urinevolume was also collected for estimation of creatinineand quantitative assessment of albuminuria using animmunoturbidimetric assay.24 A fasting blood samplewas drawn aseptically from all subjects and a 2 hpostprandial blood sample was also collected for post-prandial blood glucose estimation. Fasting blood samplewas divided into three parts: one part was collectedinto EDTA tube for DNA isolation and estimation ofglycosylated hemoglobin percentage using a fast ion-exchange resin separation method,25 with kits suppliedby Stanbio Laboratory (Ambion, Austin, TX, USA).The second part was collected in a heparinized tube,centrifuged at 3000 × g for 10 min and the separatedplasma was used for determination of NO concentra-tion in the form of nitrate/nitrite products by modifiedmicroassay of Vodovotz.26 Briefly, nitrate in plasma wasreduced to nitrite by cadmium and assayed by Greissreaction. The third part was allowed to clot at roomtemperature for half an hour then centrifuged for at least10 min at 2000 × g and serum samples were used fordetermination of NOS activity spectrophotometricallyfrom the rapid and quantitative oxidation of oxyhe-moglobin to methemoglobin by NO,27 and for measure-ment of fasting blood glucose, blood urea, and serumcreatinine using commercial assay kits supplied by BiconCo. (Germany). The creatinine clearance was thencalculated.
Analysis of Glu298Asp Polymorphism of eNOS GeneGenomic DNA was extracted from whole blood samplesusing QIAamp DNA Mini Kit (Qiagen, Valencia, CA,USA) according to the manufacturer’s instructions. TheGlu298Asp polymorphism was a G >T substitutionat nucleotide position 894 in exon 7 that encodes forreplacement of glutamic acid by aspartic acid at residue
© 2011 Informa Healthcare USA, Inc.
Ren
Fai
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Cas
e W
este
rn R
eser
ve U
nive
rsity
on
10/3
0/14
For
pers
onal
use
onl
y.

880 S.S. El-Din Bessa and S.M. Hamdy
Table 1. Clinical and biochemical characteristics of type 2 diabetic patients and controls.
ControlsDiabetics without
nephropathy Diabetics with ESRD
Number 20 40 40Age (years) 54.1 ± 8.3 55.4 ± 8.8 58.8 ± 12.5Sex (male/female) 10/10 17/23 21/19Duration of diabetes (years) – 15.3 ± 3.7 19.4 ± 4.2#
SBP (mmHg) 113.8 ± 7.3 117.2 ± 9.1 155.7 ± 5.5∗∗∗,#
DBP (mmHg) 75.2 ± 5.4 77.3 ± 5.2 94.8 ± 6.9∗∗∗,#
Fasting blood glucose (mg/dL) 77.6 ± 6.1 168.9 ± 8.2∗ 210.2 ± 10.5∗∗∗,#
Postprandial blood glucose (mg/dL) 109 ± 4.3 230.2 ± 11.2∗ 340.8 ± 13.6∗∗∗,#
HbA1c (%) 4.2 ± 0.3 6.6 ± 0.4∗ 10.4 ± 2.5∗∗∗,#
Total cholesterol (mg/dL) 153.3 ± 14.2 160.8 ± 15.1 194.4 ± 16.7∗∗∗,#
Triglyceride (mg/dL) 117.5 ± 10.8 125 ± 12.5∗∗ 170.5 ± 7.4∗∗∗,#
Urinary albumin (mg/24 h) 14.5 ± 5.1 16.2 ± 6.3 692 ± 110.7∗∗∗,#
Blood urea (mg/dL) 30.2 ± 6.4 32.6 ± 4.9 220 ± 30.8∗∗∗,#
Serum creatinine (mg/dL) 0.8 ± 0.2 0.9 ± 0.3 8.2 ± 1.2∗∗∗,#
Creatinine clearance (mL/min) 120 ± 6.8 118.3 ± 4.9 10.25 ± 2.7∗∗∗,#
Notes: Data are expressed as mean ± SD. ESRD, end-stage renal disease; SBP, systolic blood pressure; DBP,diastolic blood pressure; HbA1c, glycosylated hemoglobin.∗p < 0.001, ∗∗p < 0.05 diabetics without nephropathy versus controls. ∗∗∗p < 0.001 diabetics with ESRD versuscontrols. #p < 0.001 diabetics with ESRD versus diabetics without nephropathy.
298 in the mature eNOS protein. Genotyping of all par-ticipants was performed by polymerase chain reaction(PCR) amplification of exon 7 with the primers 5′-CATGAGGCTCAGCCCCAGAAC-3′ (sense) and 5′-AGTCAATCCCTTTGGTGCT- CAC-3′ (antisense)as described by Hingorani et al.28 Briefly, PCR ampli-fication was carried out using a thermal cycler (GeneAmp PCR system 9600, Perkin-Elmer, Norwalk, CT,USA) in a total volume of 25 µL containing 100 ngof genomic DNA, 10 mM Tris-HCl (pH 8.3), 50 mMKCl, 2.5 µL of thermophilic DNA polymerase buffer(supplied with Taq polymerase; Promega, Madison, WI,USA), 1.5 mM MgCl2, 200 µmol/L deoxynucleotidetriphosphates, 0.5 µmol/L each primer, and 1 U ofTaq polymerase. The PCR amplification consisted of 35cycles of denaturation at 94◦C for 1 min, annealing at61◦C for 1 min, extension at 72◦C for 1 min. Prede-naturation was at 94◦C for 5 min, and final extensionwas for 7 min. The PCR products were then digestedwith 1 U of MboI restriction endonuclease (MBI Fer-mentas, St. Leon-Rot., Germany) for 24 h at 37◦C andthen analyzed by 3% agarose gel electrophoresis, stainedwith ethidium bromide, and visualized under ultraviolettransillumination.
Statistical AnalysisResults were expressed as mean ± SD. Comparisonsbetween groups were made using Student’s t-test forcontinuous variables. The chi-square and Fisher’s exacttests were performed to compare genotype frequenciesbetween patients and controls. Odds ratios and 95%confidence intervals (CIs) were calculated as a mea-sure of the association between diabetes-derived ESRDand variable risk factors. A p-value less than 0.05 wasconsidered statistically significant.
RESULTS
The main clinical and biochemical characteristics of thesubjects enrolled in the study are given in Table 1. Therewere no significant differences between groups regard-ing age and gender. Diabetics with ESRD had signifi-cantly higher blood pressure, glycosylated hemoglobinpercentage, total cholesterol, and triglyceride levels(p < 0.001) and significantly longer diabetes duration(p < 0.001) than in those without nephropathy.
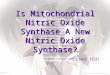
The representative result of agarose gel electrophore-sis of Glu298Asp polymorphism of the eNOS gene isshown in Figure 1. The 206 bp PCR product is cleavedinto 119 and 87 bp fragments in the presence of a T atnucleotide 894 (which corresponds to Asp298) but notin its absence.
Table 2 demonstrates that the frequency of Glu/Glu(GG) genotype (wild-type) in diabetics with ESRDwas 10/40 (25%) and was significantly lower than in
Figure 1. Representative agarose gel electrophoresis for the prod-ucts of enzymatic digestion of PCR amplified eNOS gene. M,DNA molecular marker. The GG genotype (wild-type) showed asingle band at 206 bp (base pair). The TT genotype (homozygousmutation) showed two bands at 119 and 87 bp. The GT geno-type (heterozygous mutation) showed three bands at 206, 119,and 87 bp.
Renal Failure
Ren
Fai
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Cas
e W
este
rn R
eser
ve U
nive
rsity
on
10/3
0/14
For
pers
onal
use
onl
y.

NOS Glu298Asp Polymorphism in Type 2 Diabetics with ESRD 881
Table 2. Distribution of endothelial nitric oxide synthase (eNOS) Glu298Asp genotypes amongdiabetic patients and controls.
Glu/Glu (GG)(wild-type)
Glu/Asp (GT)(heterozygous)
Asp/Asp (TT)(homozygous)
Controls n (%) 12/20 (60) 7/20 (35) 1/20 (5)Diabetics without nephropathyn (%) 17/40 (42.5) 19/40 (47.5) 4/40 (10)p-Value 0.201 0.357 0.509Diabetics with ESRDn (%) 10/40 (25) 18/40 (45) 12/40 (30)p-Value 0.008∗ 0.459 0.027∗p-Value∗∗ 0.098 0.823 0.025∗
Note: ∗significant, p-value versus controls, ∗∗p-value versus diabetics without nephropathy,p-values have been generated by chi-square and Fisher’s exact tests.
controls (12/20, 60%; p = 0.008); however, no signifi-cant difference was found between diabetics with ESRDand those without nephropathy (p = 0.098). In addi-tion, 18/40 (45%) of diabetics with ESRD had Glu/Asp(GT) genotype (heterozygous mutation), with no sta-tistically significant difference to controls (p = 0.459)or diabetics without nephropathy (p = 0.823). On theother hand, the frequency of Asp/Asp (TT) genotype(homozygous mutation) was significantly higher in dia-betics with ESRD (12/40, 30%) as compared to thosewithout nephropathy (4/40, 10%; p = 0.025) and con-trols (1/20, 5%; p = 0.027). Among diabetics withoutnephropathy, the frequency of eNOS genotypes (GG,GT, and TT) did not significantly differ from that ofcontrols.
Plasma nitrate/nitrite level and serum NOS activitywere significantly decreased in diabetics with ESRD ascompared to those without nephropathy and controls(p < 0.001); however, no significant differences werefound in nitrate/nitrite level and NOS activity betweendiabetics without nephropathy and controls, as shownin Figure 2. Furthermore, nitrate/nitrite level and NOSactivity were significantly lower in subjects with TTgenotype than in those with GG and GT genotypes(p < 0.001), as shown in Table 3. In diabetics withESRD, both nitrate/nitrite level and NOS activity werepositively correlated with creatinine clearance (r = 0.40,p < 0.01 and r = 0.49, p < 0.001, respectively), asshown in Figure 3.
In the present study, the association between eNOSGlu298Asp genotypes and ESRD in diabetic patientsis shown in Table 4. Using the GG genotype as thereference, the odds ratios were 1.61 (95% CI: 0.52–5.03) and 5.10 (95% CI: 1.09–25.80) for the GT andTT genotypes, respectively. Diabetic patients with TTgenotype are at a significant risk for ESRD.
DISCUSSION
Type 2 diabetes has reached epidemic proportions, andone of its ominous complications, DN, represents todaythe leading cause of ESRD. Despite more aggressivetreatment of diabetes, the incidence and prevalence
20
25
30
35
40
45
Diabetics withESRD
Diabetics withoutnephropathy
Plas
ma
nita
rte/
nitr
ite (
µmol
/L)
Controls
NS p < 0.001
(A)
30
45
60
75
90
105
120
Diabetics withESRD
Diabetics withoutnephropathy
Seru
m N
OS
activ
ity (
U/m
L)
Controls
NS p < 0.001
(B)
Figure 2. Plasma nitrate/nitrite level (A), and serum nitric oxidesynthase activity (B) in diabetic patients and controls.
rates of diabetes-derived ESRD continue to increaseworldwide.29
The pathogenesis of the development and progres-sion of DN is far from being clear at present. Becausethe susceptibility to diabetic vascular complicationsincluding nephropathy is genetically determined, it is
© 2011 Informa Healthcare USA, Inc.
Ren
Fai
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Cas
e W
este
rn R
eser
ve U
nive
rsity
on
10/3
0/14
For
pers
onal
use
onl
y.

882 S.S. El-Din Bessa and S.M. Hamdy
Table 3. Plasma nitrate/nitrite and serum NOS activity among the studied subjects according totheir eNOS genotypes.
Glu/Glu (GG)(wild-type)
Glu/Asp (GT)(heterozygous)
Asp/Asp (TT)(homozygous)
Number 39/100 44/100 17/100Plasma nitrate/nitrite (µmol/L) 40.6 ± 4.8 37.3 ± 5.4∗ 18.1 ± 3.6∗∗,∗∗∗Serum NOS activity (U/mL) 90.4 ± 5.8 86.8 ± 6.4∗ 54.2 ± 4.3∗∗,∗∗∗
Notes: Data are expressed as mean ± SD. NOS, nitric oxide synthase; eNOS, endothelial nitricoxide synthase.∗p < 0.01 GT genotype versus GG genotype, ∗∗p < 0.001 TT genotype versus GG genotype, ∗∗∗p< 0.001 TT genotype versus GT genotype.
12 15 18 21 24 27 30
5
10
15
20(A) (B)
r = 0.40p < 0.01
Cre
atin
ine
clea
ranc
e (m
L/m
in)
Plasma nitrate/ nitrite (µmol/L)
//
p < 0.001
30 45 60 75
4
8
12
16
20r = 0.49
Cre
atin
ine
clea
ranc
e (m
L/m
in)
Serum NOS activity (U/mL)
//
Figure 3. The positive correlation between creatinine clearance and plasma nitrate/nitrite level (A), and serum nitric oxide synthase activity(B) in diabetics with ESRD.
Table 4. Risk factors in diabetic patients with end-stage renal disease (ESRD).
Diabetics withoutnephropathy
Diabetics withESRD OR (95% CI)
Number 40 40eNOS Glu298AspWild-type (GG), n (%) 17 (42.5) 10 (25) 1.0 (Reference)Heterozygous (GT), n (%) 19 (47.5) 18 (45) 1.61 (0.52 − 5.03)Homozygous (TT), n (%) 4 (10) 12 (30) 5.10 (1.09 − 25.80)Hypertension, n (%) 15 (37.5) 28 (70) 3.89 (1.39 − 11.06)Hyperlipidemia, n (%) 19 (47.5) 30 (75) 3.32 (1.17 − 9.60)Smoking, n (%) 12 (30) 14 (35) 0.80 (0.28 − 2.25)
Note: eNOS, endothelial nitric oxide synthase; OR, odds ratio; CI, confidence interval.
reasonable to postulate that genetic polymorphism ofthe eNOS gene may contribute to the disease.30 How-ever, the contradictory findings by the multitude ofgenetic association studies reported by several investiga-tors, and the controversial role of the NO system in renalhemodynamic changes in diabetes render this subjectcomplex and puzzling.
This study has investigated the role of eNOS genepolymorphism in Egyptian type 2 diabetic patients withESRD and demonstrated that diabetic patients with TTgenotype are at a significant risk for ESRD. Moreover, itwas observed that 5% of control subjects had TT geno-type, and 60% of them had GG genotype and this isconsistent with the rates established among the Tunisianpopulation.31,32
These results are in agreement with the findingsof Neugebauer et al.21 and Shin Shin et al.,33 whoreported an association between the eNOS gene poly-morphism and the progression of DN in Japanese andKorean type 2 diabetic patients, respectively. Thesenotions were supported by recent reports.34,35 In stud-ies by Noiri et al.,36 and Thaha et al.,37 it is indicatedthat eNOS Glu298Asp polymorphism is the predis-posing factor in ESRD, especially DM-derived ESRD.Moreover, Zanchi et al.,38 and Mollsten et al.39 sug-gested an association between eNOS polymorphismand the risk of DN in patients with type 1 diabetes.Furthermore, the polymorphism in intron 4 of theeNOS gene may have influence on the progression ofrenal disease in both diabetic and nondiabetic ESRD
Renal Failure
Ren
Fai
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Cas
e W
este
rn R
eser
ve U
nive
rsity
on
10/3
0/14
For
pers
onal
use
onl
y.

NOS Glu298Asp Polymorphism in Type 2 Diabetics with ESRD 883
patients.40,41 Considering these observations, eNOSseems to be an attractive major candidate gene forprogression of DN to ESRD and warrants additionalstudies in other populations.
The mechanisms responsible for the associationbetween the eNOS polymorphism and the risk ofadvanced DN are not completely known at present.However, low NO levels caused by a defect in NO syn-thesis may play a role. In the rat model, decreased renalNO accelerates the progression of DN, presumablythrough mechanisms such as increased renal vasculartone and potentiation of angiotensin II effects.42
Interestingly, the eNOS gene is located on chro-mosome 7q3543 and the gene coding for aldosereductase44; a candidate gene for genetic susceptibilityto DN in type 1 diabetic patients45 has been locatedon the same chromosomal region. Therefore, it may bea candidate region for genetic susceptibility to diabeticmicrovascular complications. This highly speculativehypothesis needs to be clarified in future studies.
Although microalbuminuria is regarded as a risk fac-tor for DN, no association was found between the eNOSgene polymorphism and microalbuminuria in type 2diabetic patients.21 Therefore, it is postulated that thispolymorphism could be an aggravating factor ratherthan an initiating factor for DN.
Conversely, other studies have reported no asso-ciation between NOS gene polymorphisms andDN.22,46–48 Although these conflicting data may beconfusing, the data have to be reconciled with dif-ferences in patient populations, NOS isoforms, andstage of renal disease. Thus, more accurate informationis needed from systematic and large-scale studies toestablish causal links to pathogenesis.
In the current study, plasma NO level in theform of nitrate/nitrite was elevated in diabetics with-out nephropathy with no statistically significant differ-ence to controls. These results are consistent with thefindings of other previous studies.49,50 On the otherhand, plasma nitrate/nitrite level was significantly lowerin diabetics with ESRD as compared to those with-out nephropathy and controls, similar to the resultsobtained by Ahluwalia et al.35 Furthermore, plasmanitrate/nitrite level and serum NOS activity were signifi-cantly lower in subjects with TT genotype than in thosewith GG and GT genotypes, suggesting the hypothe-sis that the Glu298Asp polymorphism of eNOS gene isresponsible for the progression of DN to ESRD throughdecreased NO levels. These results are very interestingand could stimulate larger studies.
Some limitations of the present study should be dis-cussed. First, one must consider the possible effect ofmultiple comparisons on the significance level of thefindings. Second, the magnitude of the impact of the TTgenotype of eNOS on susceptibility to ESRD and thegeneralizability of our findings are uncertain since ourstudy was conducted in Egyptians with type 2 diabetes,so it is not clear whether our findings can be generalized
to other races or to patients with type 1 diabetes. Third,the participation of other genes, as well as environmen-tal factors must be considered in the development ofESRD in diabetics.
Although the literature continues to expand exponen-tially in the area of renal NO system and DN, severalquestions still remain unanswered. The challenge forfuture research will be to unravel the complex inter-action between hyperglycemia and NO pathway, whichmay lead to a better understanding of the pathogen-esis of diabetic kidney disease. The magnitude of theproblem of DN, particularly in the face of the globalepidemic of diabetes, warrants more concerned effortstoward seeking new potential strategies to prevent thedevelopment and therapeutic interventions to retard theprogression of this devastating disease.
In conclusion, these results imply that the TT geno-type of eNOS may be associated with an increased riskof ESRD in Egyptian type 2 diabetics. It could representa useful genetic marker to identify diabetics at high riskfor the development of ESRD and help to target preven-tive and therapeutic measures in susceptible individuals.However, larger future prospective studies are requiredto confirm the role of eNOS gene polymorphism inthe progression of DN to ESRD and to evaluate theinteractions between this genetic predisposition andenvironmental factors.
Declaration of interest: The authors report no con-flicts of interest. The authors alone are responsible forthe content and writing of the paper.
REFERENCES
[1] Schrijvers BF, De Vriese AS, Flyvbjerg A. From hyperglycemiato diabetic kidney disease: The role of metabolic, hemodynamic,intracellular factors and growth factors/cytokines. Endocr Rev.2004;25:971–1010.
[2] Seaquist ER, Goetz FC, Rich SS, Barbosa J. Familial clusteringof diabetic kidney disease: Evidence for genetic susceptibility todiabetic nephropathy. N Engl J Med. 1989;320:1161–1165.
[3] Agius E, Attard G, Shakespeare L, et al. Familial factorsin diabetic nephropathy: An offspring study. Diabet Med.2006;23:331–334.
[4] Craven PA, DeRubertis FR, Melhem M. Nitric oxide in diabeticnephropathy. Kidney Int. 1997;52(Suppl. 60):S46–S53.
[5] Prabhakar SS. Role of nitric oxide in diabetic nephropathy.Semin Nephrol. 2004;24:333–344.
[6] Sharma SP. Nitric oxide and the kidney. Indian J Nephrol.2004;14:77–84.
[7] Prabhakar SS. Pathogenic role of nitric oxide alterations indiabetic nephropathy. Curr Diab Rep. 2005;5:449–454.
[8] Zhao HJ, Wang S, Cheng H, et al. Endothelial nitric oxide syn-thase deficiency produces accelerated nephropathy in diabeticmice. J Am Soc Nephrol. 2006;17:2664–2669.
[9] Nakagawa T, Sato W, Glushakova O, et al. Diabetic endothelialnitric oxide synthase knockout mice develop advanced diabeticnephropathy. J Am Soc Nephrol. 2007;18:539–550.
[10] Moncada S, Higgs A. The L-arginine-nitric oxide pathway. NEngl J Med. 1993;329:2002–2012.
© 2011 Informa Healthcare USA, Inc.
Ren
Fai
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Cas
e W
este
rn R
eser
ve U
nive
rsity
on
10/3
0/14
For
pers
onal
use
onl
y.

884 S.S. El-Din Bessa and S.M. Hamdy
[11] Alderton WK, Cooper CE, Knowles RG. Nitric oxide synthases:Structure, function and inhibition. Biochem J. 2001;357:593–615.
[12] Schmidt HW, Walter U. NO at work. Cell. 1994;78:919–925.[13] Kone BC, Baylis C. Biosynthesis and homeostatic roles of nitric
oxide in the normal kidney. Am J Physiol. 1997;272:F561–F578.[14] Kone BC. Nitric oxide in renal health and disease. Am J Kidney
Dis. 1997;30:311–333.[15] Kone BC. Nitric oxide synthesis in the kidney: Isoforms, biosyn-
thesis and functions in health. Semin Nephrol. 2004;24:299–315.[16] Santilli F, Cipollone F, Mezzetti A, Chiarelli F. The role of nitric
oxide in the development of diabetic angiopathy. Horm MetabRes. 2004;36:319–335.
[17] Yoshimura M, Yasue H, Nakayama M, et al. A missense glu298-to-asp variant in the endothelial nitric oxide synthase gene isassociated with coronary spasm in the Japanese. Hum Genet.1998;103:65–69.
[18] Hibi K, Ishigami T, Tamura K, et al. Endothelial nitric oxidesynthase gene polymorphism and acute myocardial infarction.Hypertension. 1998;32:521–526.
[19] Miyamoto Y, Saito Y, Kajiyama N, et al. Endothelial nitric oxidesynthase gene is positively associated with essential hypertension.Hypertension. 1998;32:3–8.
[20] Lembo G, DeLuca N, Battagli C, et al. A common variantof endothelial nitric oxide synthase (Glu298Asp) is an inde-pendent risk factor for carotid atherosclerosis. Stroke. 2001;32:735–740.
[21] Neugebauer S, Baba T, Watanabe T. Association of the nitricoxide synthase gene polymorphism with an increased risk forprogression to diabetic nephropathy in type 2 diabetes. Diabetes.2000;49:500–503.
[22] Fujita H, Narita T, Meguro H, et al. Lack of association betweenan ecNOS gene polymorphism and diabetic nephropathy in type2 diabetic patients with proliferative diabetic retinopathy. HormMetab Res. 2000;32:80–83.
[23] Spooren PF, Lekker JF, Vermes I. Micral test a qualitativedipstick test for microalbuminuria. Diabetes Res Clin Pract.1992;18:83–87.
[24] Teppo AM. Immunoturbidimetry of albumin and immunoglob-ulin G in urine. Clin Chem. 1982;28:1359–1361.
[25] Maquart F, Giller P, Bernard J. Method for specially measur-ing of hemoglobin A1c with disposable commercial ion exchangecolumn. Clin Chim Acta. 1980;108:329.
[26] Vodovotz Y. Modified microassay for serum nitrite and nitrate.Biotechniques. 1996;20:390–394.
[27] Olken NM, Rusche KM, Richards MK, Marletta MA. Inac-tivation of macrophage nitric oxide synthase activity by N-methyl-L-arginine. Biochem Biophys Res Commun. 1991;177:828–833.
[28] Hingorani AD, Liang CF, Fatibene J, et al. A common variantof the endothelial nitric oxide synthase (Glu298Asp) is a majorrisk factor for coronary artery disease in the UK. Circulation.1999;100:1515–1520.
[29] Satko SG, Freedman BI, Moossavi S. Genetic factors in end-stage renal disease. Kidney Int. 2005;67(Suppl. 94):S46–S49.
[30] Freedman BI, Bostrom M, Daeihagh P, Bowden DW. Geneticfactors in diabetic nephropathy. Clin J Am Soc Nephrol.2007;2:1306–1316.
[31] Kerkeni M, Addad F, Chauffert M, et al. Hyperhomocysteine-mia, endothelial nitric oxide synthase polymorphism, and risk ofcoronary artery disease. Clin Chem. 2006;52:53–58.
[32] Kerkeni M, Letaief A, Achour A, Miled A, Trivin F, MaaroufiK. Endothelial nitric oxide synthase, methylenetetrahydrofolatereductase polymorphisms, and cardiovascular complications in
Tunisian patients with nondiabetic renal disease. Clin Biochem.2009;42:958–964.
[33] Shin Shin Y, Baek SH, Chang KY, et al. Relations betweeneNOS Glu298Asp polymorphism and progression of diabeticnephropathy. Diabetes Res Clin Pract. 2004;65:257–265.
[34] Ezzidi I, Mtiraoui N, Mohamed MB, Mahjoub T, Kacem M,Almawi WY. Association of endothelial nitric oxide synthaseGlu298Asp, 4b/a, and -786T>C gene variants with diabeticnephropathy. J Diabetes Complications. 2008;22:331–338.
[35] Ahluwalia TS, Ahuja M, Rai TS, et al. Endothelial nitric oxidesynthase gene haplotypes and diabetic nephropathy among AsianIndians. Mol Cell Biochem. 2008;314:9–17.
[36] Noiri E, Satoh H, Taguchi J, et al. Association of eNOSGlu298Asp polymorphism with end-stage renal disease. Hyper-tension. 2002;40:535–540.
[37] Thaha M, Yogiantoro M, Tanimoto M, Gohda T, TominoY. Association of endothelial nitric oxide synthase Glu298Asppolymorphism with end-stage renal disease. Clin Nephrol.2008;70:144–154.
[38] Zanchi A, Moczulski DK, Hanna LS, Wantman M, Warram JH,Krolewski AS. Risk of advanced diabetic nephropathy in type 1diabetes is associated with endothelial nitric oxide synthase genepolymorphism. Kidney Int. 2000;57:405–413.
[39] Mollsten A, Lajer M, Jorsal A, Tarnow L. The endothelial nitricoxide synthase gene and risk of diabetic nephropathy and devel-opment of cardiovascular disease in type 1 diabetes. Mol GenetMetab. 2009;97:80–84.
[40] Buraczynska M, Ksiazek P, Zaluska W, Nowicka T, Ksiazek A.Endothelial nitric oxide synthase gene intron 4 polymorphismin patients with end-stage renal disease. Nephrol Dial Transplant.2004;19:2302–2306.
[41] Bellini MH, Figueira MN, Piccoli MF, et al. Association ofendothelial nitric oxide synthase gene intron 4 polymorphismwith end-stage renal disease. Nephrology. 2007;12:289–293.
[42] Shultz PJ, Schorer AE, Raij L. Effects of endothelium-derivedrelaxing factor and nitric oxide on rat mesangial cells. Am JPhysiol. 1990;258:F162–F167.
[43] Marsden PA, Heng HHQ, Scherer SW, et al. Structure andchromosomal localization of the human constitutive endothelialnitric oxide synthase gene. J Biol Chem. 1993;268:17478–17488.
[44] Graham A, Heath P, Morten JEN, Markham AF. The humanaldose reductase gene maps to region 7q35. Hum Genet.1991;86:509–514.
[45] Heesom AE, Hibberd ML, Millward A, Demaine AG. Poly-morphism in the 5-end of the aldose reductase gene is stronglyassociated with the development of diabetic nephropathy in type1 diabetes. Diabetes. 1997;46:287–291.
[46] Shimizu T, Onuma T, Kawamori R, Makita Y, Tomino Y.Endothelial nitric oxide synthase gene and the development ofdiabetic nephropathy. Diabetes Res Clin Pract. 2002;58:179–185.
[47] Rippin JD, Patel A, Belyaev ND, Gill GV, Barnett AH, BainSC. Nitric oxide synthase gene polymorphisms and diabeticnephropathy. Diabetologia. 2003;46:426–428.
[48] Liao L, Lim M, Chan S, Zhao J, Lee K. Nitric oxide synthasegene polymorphisms and nephropathy in Asians with type 2diabetes. J Diabetes Complications. 2006;20:371–375.
[49] Maejima K, Nakano S, Himeno M, et al. Increased basal levelsof plasma nitric oxide in type 2 diabetic subjects. Relation-ship to microvascular complications. J Diabetes Complications.2001;15:135–143.
[50] Apakkan Aksun S, Ozmen B, Ozmen D, et al. Serum and urinarynitric oxide in type 2 diabetes with or without microalbuminuria:Relation to glomerular hyperfiltration. J Diabetes Complications.2003;17:343 – 348.
Renal Failure
Ren
Fai
l Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Cas
e W
este
rn R
eser
ve U
nive
rsity
on
10/3
0/14
For
pers
onal
use
onl
y.