Embed Size (px)
Citation preview

813
Language barriers may lead to poor quality of care for many reasons, including misdiagnosis, delays in care,
decreased patient engagement and empowerment, and mis-use of diagnostic testing.1–3 However, for many medical conditions, clinical decision making can be based to a large extent on the result of objective physical examination find-ings, laboratory testing, or diagnostic imaging. Therefore, patients who do not speak the same language as their care providers need not necessarily receive poorer care, because making a diagnosis or selecting a treatment option can be done effectively despite the communication barriers. For example, language proficiency does not impact outcomes for diabetes mellitus or myocardial infarction.4,5 However, acute stroke is different. Making a diagnosis often relies on elic-iting subjective patient symptoms, and treatment decisions, such as whether to administer thrombolysis, may hinge on definitively establishing the time since the onset of symp-toms. Therefore, language barriers between patients and their healthcare providers may influence care and outcomes for acute stroke. For example, in previous research, longer lengths of stay and inadequate anticoagulation for such patients have been found.6,7
The objective of this study was to determine the impact of language barriers on the quality of care and clinical outcomes for acute stroke. We hypothesized that patients with language barriers would have lower quality of care and worse outcomes than those without language barriers.
Materials and MethodsStudy Design and Data SourcesThis cohort study used clinical data from the Registry of the Canadian Stroke Network (RCSN, now known as the Ontario Stroke Registry) from July 2003 to March 2008 in Ontario, Canada’s most populous province. The RCSN was used to prospectively collect data on con-secutive patients with acute stroke or transient ischemic attack seen in emergency departments or hospitalized at 12 stroke centers in the province.8 Trained neurology research nurses collected data at each site using chart abstraction and care provider interview when needed. Detailed information was collected on patient demographics (includ-ing language preferences), presenting symptoms, risk factors, and other medical history, hospital care, interventions and complications, final disposition, discharge medications, and functional outcomes. Inter-rater reliability of chart abstraction for key variables was sub-stantial to almost perfect (κ=0.66–1.0).
To collect longitudinal follow-up data on patients after their initial stroke hospitalization, the Registry was then linked with
Background and Purpose—Language barriers may lead to poor quality of care, particularly for conditions like acute stroke for which diagnosis and treatment decision making rely on taking an accurate patient history. The purpose of this study was to determine the impact of patient language barriers on quality of stroke care and clinical outcomes.
Methods—This retrospective cohort study used data from the Registry of the Canadian Stroke Network. All Ontario patients who were admitted with acute stroke or transient ischemic attack between July 2003 and March 2008 were selected. Mortality, stroke outcomes, in-hospital complications, quality of care, and disposition were compared between those without (n=12 787) and with (n=1506) language barriers, which was defined based on the patient’s preferred language. Hierarchical multivariable regression models determined the effect of language barriers, independent of baseline covariates.
Results—Patients with language barriers had better 7-day mortality than those without (7.0% versus 9.2%; OR, 0.69; 95% CI, 0.57–0.82; P<0.001). However, they were more likely to be discharged with a moderate-to-severe neurological deficit (65.9% versus 51.5%; OR, 1.25; 95% CI, 1.15–1.35). In-hospital complication rates did not differ, and quality of care indicators generally favored patients with language barriers.
Conclusions—Patients who had language barriers had reduced mortality and better performance on some quality of care measures. These differences existed despite adjustment for many potential confounders, including ethnicity, prognostic factors, and stroke characteristics. (Stroke. 2015;46:813-818. DOI: 10.1161/STROKEAHA.114.007929.)
Key Words: communication barriers ◼ language ◼ mortality ◼ quality of health care
Impact of Language Barriers on Stroke Care and OutcomesBaiju R. Shah, MD, PhD; Nadia A. Khan, MD, MSc; Martin J. O’Donnell, MB, PhD;
Moira K. Kapral, MD, MSc
Received October 28, 2014; final revision received December 22, 2014; accepted January 6, 2015.From the Department of Medicine, University of Toronto, Ontario, Canada (B.R.S., M.K.K.); Institute for Clinical Evaluative Sciences, Toronto, Ontario,
Canada (B.R.S., M.K.K.); Department of Medicine, University of British Columbia, Vancouver, BC, Canada (N.A.K.); and Department of Medicine, National University of Ireland, Galway, Ireland (M.J.O.).
The online-only Data Supplement is available with this article at http://stroke.ahajournals.org/lookup/suppl/doi:10.1161/STROKEAHA. 114.007929/-/DC1.
Correspondence to Baiju R. Shah, MD, PhD, G106 – 2075 Bayview Ave, Toronto, Ontario M4N 3M5, Canada. E-mail [email protected]© 2015 American Heart Association, Inc.
Stroke is available at http://stroke.ahajournals.org DOI: 10.1161/STROKEAHA.114.007929
by guest on May 28, 2018
http://stroke.ahajournals.org/D
ownloaded from
by guest on M
ay 28, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on May 28, 2018
http://stroke.ahajournals.org/D
ownloaded from
by guest on M
ay 28, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on May 28, 2018
http://stroke.ahajournals.org/D
ownloaded from
by guest on M
ay 28, 2018http://stroke.ahajournals.org/
Dow
nloaded from
by guest on May 28, 2018
http://stroke.ahajournals.org/D
ownloaded from

814 Stroke March 2015
population-based healthcare administrative databases from the pub-licly funded health insurance program of the Ontario Ministry of Health and Long-Term Care, which provides coverage to all perma-nent residents of Ontario. These databases included the Registered Persons Database, which records demographic information includ-ing date of death for all residents; the Discharge Abstract Database, which records detailed diagnostic and procedural information for all hospital admissions; and the Ontario Health Insurance Plan’s Claims Database, which records all claims submitted by physicians for fee-for-service reimbursement. Individuals are linked between the Registry and all of these databases using a unique encrypted identi-fication number.
Patient Population and Exposure DefinitionAll patients aged ≥20 years who were admitted to a Registry-participating hospital with an ischemic stroke, hemorrhagic stroke, or transient ischemic attack between July 1, 2003 and March 31, 2008 were selected. Patients who had a subarachnoid hemorrhage were excluded. For patients with multiple strokes included in the Registry, only the first event was included. Patients with missing data on key baseline characteristics (language preferences, socioeco-nomic status, and level of consciousness at presentation) were also excluded. Language barriers were defined based on the patient’s pre-ferred language. Patients were considered to have no language bar-rier at most hospitals if their preferred language was English; at the Ottawa Hospital and the Sudbury Regional Hospital, which operate bilingually, patients whose preferred language was English or French were considered to have no language barrier. Patients who had other languages as their preferred language were considered to have a lan-guage barrier.
Outcome and Covariate DefinitionsThe primary outcome was early mortality (within 7 days) after stroke. Secondary outcomes were 30-day mortality, 1-year mortality, and (for patients who did not die in hospital) residual neurological deficit at discharge, measured as a modified Rankin scale between 3 (moder-ate disability) and 5 (severe disability).
To understand any potential observed differences in mortality, ad-ditional secondary clinical outcomes were evaluated: receipt of throm-bolytic therapy, time from hospital arrival to thrombolytic therapy (door-to-needle time), in-hospital complications (decubitis ulcer, fall with fracture, pneumonia, and thromboembolic complications), length of stay, and discharge disposition from hospital (discharge to home or to a rehabilitation hospital versus transfer to another acute care institu-tion or discharge to long-term care). Finally, a variety of quality of care indicators were studied, which were developed by a Canadian expert panel for inclusion in the Canadian Best Practice Recommendations for Stroke Care.9 These included brain imaging within 24 hours of hospital arrival; in-hospital assessment from an occupational thera-pist, physiotherapist, speech–language pathologist, social worker, and nutritionist; carotid imaging within 2 weeks of admission; and discharge prescriptions for aspirin or warfarin, antihypertensives, and statins. Detailed descriptions of each of these outcome variables and the eligible subset of the whole cohort in whom each was defined are described Table I in the online-only Data Supplement.
A variety of baseline characteristics were defined for each patient, including demographic, clinical, and stroke presentation factors. These are described in detail in Table II in the online-only Data Supplement.
Statistical AnalysisThe baseline characteristics were compared between patients with and without language barriers using χ2 tests for categorical variables and t tests for continuous variables. To determine the independent effect of language barriers on each of the primary and secondary out-comes, logistic regression models were built adjusting for age, sex, ethnicity, socioeconomic status, stroke type, level of consciousness on arrival, vascular risk factors, previous cardiovascular disease, pre-vious cancer, dementia or depression, Charlson comorbidity score,10
and the variables included in the PLAN-IT clinical prediction rule, a validated tool to identify patients at risk for poor stroke outcomes.11 Length of stay was modeled similarly using quantile regression. The independent effect of language barriers on the in-hospital quality of care indicators was determined using logistic regression models ad-justing for age, sex, ethnicity, socioeconomic status, stroke type, and level of consciousness on arrival only. Door-to-needle time was mod-eled similarly using quantile regression.
To explore in greater depth the factors that contribute to differences in the mortality outcomes between groups, we performed a series of logistic regression models: first unadjusted, and then sequentially adding the following covariates in a stepwise fashion: age and sex, then ethnicity and socioeconomic status, then stroke characteristics (stroke type and level of consciousness on arrival), then vascular risk factors and previous cardiovascular disease, then other comorbidities and PLAN-IT score, and then measures of aggressive versus support-ive care during the admission (admission to a dedicated stroke unit, admission to an intensive care unit, use of a nasogastric tube, use of a permanent feeding tube, consultation with a neurologist, and pal-liative care).
To search for multicollinearity between the predictor variables, we examined the variance inflation factors for all the covariates when included together in a multiple regression model, and confirmed that they were all <5.12
All of the above multivariable regression models were constructed as clustered data models, adjusting for hospital site to account for the clustered nature of the data. Analyses were conducted using SAS version 9.3 (Cary, NC). Clustered quantile regression analyses were conducted using the lqmm package in R version 3.1.0.
EthicsThe study was approved by the research ethics board of Sunnybrook Health Sciences Center, Toronto.
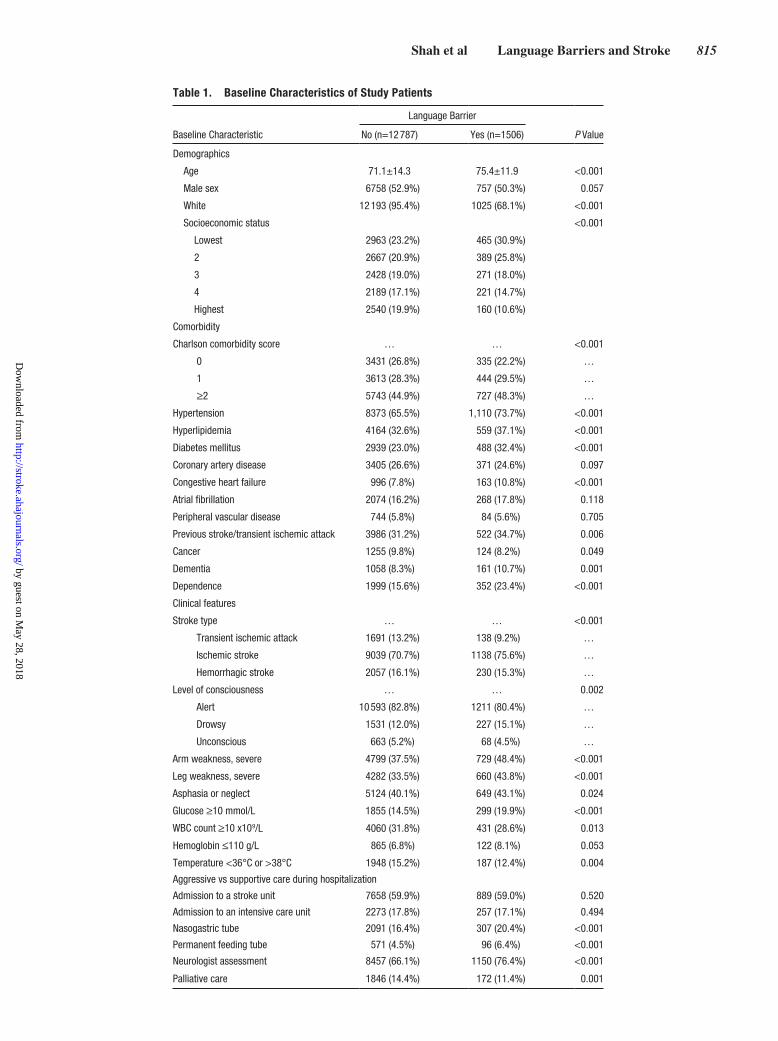
ResultsThere were 17 080 admissions for stroke to a participating hospital among adults during the 5 years of the study. Those with subarachnoid hemorrhage (n=1555) were excluded, and the second or subsequent admissions for individual patients (n=741) were also excluded. Finally, 491 patients were excluded because of missing data on key variables (language preference, socioeconomic status, or level of consciousness on admission). Thus, the final cohort included 14 293 patients, of whom 1506 (10.5%) had a language barrier. The baseline characteristics of the included patients are shown in Table 1. Patients with a language barrier were older, were less likely to be white, were poorer, and had greater comorbidity than patients without language barriers. They were also more likely to present with an ischemic stroke and were less likely to pres-ent with a transient ischemic attack.
The 7-day mortality rate was 7.0% among those with lan-guage barriers and 9.2% among those without (P=0.006). When adjusted for baseline demographic and clinical dif-ferences, patients with language barriers were less likely to have died within 7 days after their stroke (adjusted odds ratio 0.69, 95% confidence interval 0.57–0.82, P<0.001). Similar results were seen for 30-day and 1-year mortality although the adjusted odds ratios became increasingly closer to unity with longer time periods (Table 2). In contrast, patients with language barriers were more likely to be discharged from hos-pital with a moderate-to-severe residual neurological deficit (65.9% versus 51.5%, adjusted odds ratio 1.25; 95% confi-dence interval, 1.15–1.35; P<0.001).
by guest on May 28, 2018
http://stroke.ahajournals.org/D
ownloaded from
Shah et al Language Barriers and Stroke 815
Table 1. Baseline Characteristics of Study Patients
Baseline Characteristic
Language Barrier
P ValueNo (n=12 787) Yes (n=1506)
Demographics
Age 71.1±14.3 75.4±11.9 <0.001
Male sex 6758 (52.9%) 757 (50.3%) 0.057
White 12 193 (95.4%) 1025 (68.1%) <0.001
Socioeconomic status <0.001
Lowest 2963 (23.2%) 465 (30.9%)
2 2667 (20.9%) 389 (25.8%)
3 2428 (19.0%) 271 (18.0%)
4 2189 (17.1%) 221 (14.7%)
Highest 2540 (19.9%) 160 (10.6%)
Comorbidity
Charlson comorbidity score … … <0.001
0 3431 (26.8%) 335 (22.2%) …
1 3613 (28.3%) 444 (29.5%) …
≥2 5743 (44.9%) 727 (48.3%) …
Hypertension 8373 (65.5%) 1,110 (73.7%) <0.001
Hyperlipidemia 4164 (32.6%) 559 (37.1%) <0.001
Diabetes mellitus 2939 (23.0%) 488 (32.4%) <0.001
Coronary artery disease 3405 (26.6%) 371 (24.6%) 0.097
Congestive heart failure 996 (7.8%) 163 (10.8%) <0.001
Atrial fibrillation 2074 (16.2%) 268 (17.8%) 0.118
Peripheral vascular disease 744 (5.8%) 84 (5.6%) 0.705
Previous stroke/transient ischemic attack 3986 (31.2%) 522 (34.7%) 0.006
Cancer 1255 (9.8%) 124 (8.2%) 0.049
Dementia 1058 (8.3%) 161 (10.7%) 0.001
Dependence 1999 (15.6%) 352 (23.4%) <0.001
Clinical features
Stroke type … … <0.001
Transient ischemic attack 1691 (13.2%) 138 (9.2%) …
Ischemic stroke 9039 (70.7%) 1138 (75.6%) …
Hemorrhagic stroke 2057 (16.1%) 230 (15.3%) …
Level of consciousness … … 0.002
Alert 10 593 (82.8%) 1211 (80.4%) …
Drowsy 1531 (12.0%) 227 (15.1%) …
Unconscious 663 (5.2%) 68 (4.5%) …
Arm weakness, severe 4799 (37.5%) 729 (48.4%) <0.001
Leg weakness, severe 4282 (33.5%) 660 (43.8%) <0.001
Asphasia or neglect 5124 (40.1%) 649 (43.1%) 0.024
Glucose ≥10 mmol/L 1855 (14.5%) 299 (19.9%) <0.001
WBC count ≥10 x109/L 4060 (31.8%) 431 (28.6%) 0.013
Hemoglobin ≤110 g/L 865 (6.8%) 122 (8.1%) 0.053
Temperature <36°C or >38°C 1948 (15.2%) 187 (12.4%) 0.004
Aggressive vs supportive care during hospitalization
Admission to a stroke unit 7658 (59.9%) 889 (59.0%) 0.520
Admission to an intensive care unit 2273 (17.8%) 257 (17.1%) 0.494
Nasogastric tube 2091 (16.4%) 307 (20.4%) <0.001
Permanent feeding tube 571 (4.5%) 96 (6.4%) <0.001
Neurologist assessment 8457 (66.1%) 1150 (76.4%) <0.001
Palliative care 1846 (14.4%) 172 (11.4%) 0.001
by guest on May 28, 2018
http://stroke.ahajournals.org/D
ownloaded from

816 Stroke March 2015
In-hospital complications were rare, and not statistically significantly different between those with and without lan-guage barriers. However, those with language barriers had longer median lengths of stay (1.6 days longer; 95% CI, 0.6–2.7; P=0.002). Although the crude proportion of patients who received brain imaging within 24 hours of admission was similar in both groups, those with language barriers were more likely to receive such imaging once age, sex, ethnicity, and socioeconomic status were adjusted for (adjusted odds ratio 1.30; 95% CI, 1.01–1.66; P=0.036). Patients with lan-guage barriers were more likely to receive assessments from a variety of healthcare professionals during the hospitalization. Thrombolysis, carotid imaging, and discharge prescription rates did not differ between groups.
To explore the factors that contributed to the observed mor-tality difference, we performed a series of regression models for the primary outcome, adjusting for additional covariates (Figure). In the unadjusted model, language barriers were associated with reduced 7-day mortality (odds ratio 0.82; 95% CI, 0.70–0.97; P=0.023). However, with sequential adjust-ment for demographic factors, then adding stroke characteris-tics, and then adding comorbidities, the adjusted odds ratio for mortality moved increasingly away from the null. However,
adjustment for aggressive versus supportive care attenuated the mortality benefit for those with language barriers, with the 95% confidence interval nearly crossing unity. Similar results were seen for the 30-day and 1-year mortality outcomes (not shown).
DiscussionPatients with language barriers had an ≈30% reduced odds of death at 7 and 30 days, and a >20% reduced odds of death at 1 year, even after adjusting for baseline demographic and clinical differences between groups. This reduction in mor-tality risk was attenuated by differences between groups in the desire for aggressive versus supportive medical care, and previous studies have suggested that early stroke mortality is strongly sensitive to patient/family preferences for with-drawal of care.13 As further evidence of this preference for active treatment, patients with language barriers were more likely to be discharged with a residual neurological deficit, had longer lengths of stay, and were more likely to be dis-charged to home or to a rehabilitation hospital rather than to another acute care or a long-term care institution. Patients with language barriers also performed better on several in-hospital quality of care markers: they were more likely to
Table 2. Frequencies of Outcomes for Patients With and Without Language Barriers
Language Barrier
Outcome No Yes Adjusted Odds Ratio (95% CI) P Value
Mortality and stroke outcomes
7-day mortality 1171/12 787 (9.2%) 106/1506 (7.0%) 0.69 (0.57–0.82) <0.001
30-day mortality 2008/12 787 (15.7%) 220/1506 (14.6%) 0.71 (0.58–0.86) <0.001
1-yr mortality 3270/12 787 (25.6%) 403/1506 (26.8%) 0.79 (0.73–0.87) <0.001
Moderate-to-severe residual neurological deficit 5634/10 940 (51.5%) 858/1301 (65.9%) 1.25 (1.15–1.35) <0.001
In-hospital complications
Decubitis ulcer 124/12 787 (1.0%) 21/1506 (1.4%) 0.88 (0.60–1.29) 0.512
Fall with fracture 64/12 787 (0.5%) 8/1506 (0.5%) 0.79 (0.31–2.01) 0.620
Pneumonia 825/12 787 (6.5%) 139/1506 (9.2%) 1.18 (0.96–1.44) 0.124
Thromboembolic complications 190/12 787 (1.5%) 21/1506 (1.4%) 0.89 (0.50–1.56) 0.675
Disposition
Length of stay, days, median (IQR) 8 (4–15) 9 (5–20) 1.6 (0.6–2.7)* 0.002
Discharge to home or rehabilitation hospital 8617/10 940 (78.8%) 981/1301 (75.4%) 1.20 (1.00–1.44) 0.046
Quality of care
Received thrombolysis 900/1601 (56.2%) 93/160 (58.1%) 0.89 (0.67–1.18) 0.430
Door-to-needle time, minutes, median (IQR) 75 (58–99) 82 (61–105) 3.6 (-9.4–16.5)* 0.584
Brain imaging within 24 h 11 727/12 258 (95.7%) 1421/1480 (96.0%) 1.30 (1.01–1.66) 0.039
Occupational therapist assessment 9204/12 787 (72.0%) 1210/1506 (80.3%) 1.32 (1.17–1.48) <0.001
Physiotherapist assessment 9820/12 787 (76.8%) 1247/1506 (82.8%) 1.27 (1.09–1.49) 0.003
Speech–language pathologist assessment 6992/12 787 (54.7%) 988/1506 (65.6%) 1.26 (1.16–1.37) <0.001
Social worker assessment 6002/12 787 (46.9%) 884/1506 (58.7%) 1.26 (1.11–1.44) <0.001
Nutritionist assessment 4426/12 787 (34.6%) 633/1506 (42.0%) 1.28 (1.10–1.49) 0.002
Carotid imaging within 2 wk 3957/4742 (83.4%) 393/465 (84.5%) 1.07 (0.76–1.49) 0.704
Discharge prescription for aspirin or warfarin 9284/9577 (96.9%) 1119/1148 (97.5%) 1.17 (0.94–1.45) 0.156
Discharge prescription for antihypertensives 7434/9577 (77.6%) 938/1148 (81.7%) 1.03 (0.84–1.26) 0.771
Discharge prescription for statins 6434/9577 (67.2%) 817/1148 (71.2%) 1.17 (0.94–1.46) 0.167
*Absolute difference in the median value with 95% confidence intervals, adjusted for covariates and clustering.
by guest on May 28, 2018
http://stroke.ahajournals.org/D
ownloaded from

Shah et al Language Barriers and Stroke 817
receive timely brain imaging, and were more likely to receive assessments from paramedical personnel. In fact, these differ-ences in quality of care may have arisen because of language barriers: the healthcare team may have sought more intensive evaluation of patients with whom their communication was impeded. Alternatively, the longer lengths of stay for patients with language barriers may have provided more opportunities for paramedical assessments. Thrombolysis, carotid imaging, and appropriate discharge prescriptions were not associated with language barriers.
There has been little previous research examining the impact of language barriers on stroke care and outcomes. Differences in long-term (rather than in-hospital) mortal-ity and quality of care have not been studied previously. A Canadian study examining the impact of language pro-ficiency on lengths of hospital stay for various diagno-ses found the greatest difference for stroke: 14.9 days for patients proficient in English versus 26.1 days for those who were not.6 These observations are similar to those in our study, though greater in magnitude. An American study of an anticoagulation clinic found that Hispanic patients, but not Asian patients, who were English speaking spent more time in therapeutic range than those who were not.7 Other studies did not find differences in stroke care or out-comes based on language barriers, but they may have been underpowered.14,15
Our study has several strengths to highlight, including a rigorous ascertainment of stroke care and outcomes using uniform definitions and trained abstractors. Rich clinical data were collected, allowing for evaluation of many clinically important measures of quality, and for extensive adjustment for potential confounding factors. Furthermore, we were
able to link this rich clinical data with administrative data for long-term outcomes that, in the Canadian single-payer universal healthcare system, result in no loss to follow-up or missing data. In addition, the sample size in this study was markedly larger than virtually all previous studies, allowing greater power. However, there are some important limita-tions to note. Although we adjusted for a larger number of potential confounding variables in the analyses, as with any observational study, the associations that were found may be partially explained by residual confounding because of other unmeasured factors that differ between patients with and without language barriers. Second, notwithstanding the large number of participating hospitals, they remained pre-dominantly urban tertiary care centers, so the generalizabil-ity of the results to smaller or less well-resourced centers is uncertain. However, the participating hospitals may actually reflect the areas where most patients with language barri-ers live because few immigrants settle in rural areas. Third, a language preference other than English (or French at the two bilingual hospitals) does not necessarily mean a patient would have language barriers: they may have sufficient flu-ency to be able to communicate with their providers, they may have family members or professional translators avail-able to translate, or the healthcare providers may have been able to speak the patient’s language. However, many patients with even marginal English fluency may have self-reported an English language preference,16 which would bias the study toward the null.
Understanding the impact of language barriers on healthcare is important in many countries. For example, in Canada, the number of non-English–non-French speak-ers grew by >20% between 2001 and 2006, compared with
Figure. Odds ratios for language barriers on 7-day mortality, unadjusted and sequentially adjusted for increasing numbers of baseline covariates.
by guest on May 28, 2018
http://stroke.ahajournals.org/D
ownloaded from

818 Stroke March 2015
only 4% growth in the number of English speakers.17 The reasons why patients with language barriers have lower stroke mortality, even after adjusting for prognostic factors, comorbidity, and stroke characteristics, remain unclear, though their greater desire for aggressive intervention over supportive care likely plays a role. Rather than being related to language barriers per se, the desire for aggressive care is probably related more to ethnicity, religious background, or immigration status, and further research is required to char-acterize which patients share this preference for aggressive medical intervention, and to understand the sociocultural factors explaining it.
In conclusion, although we hypothesized that patients with language barriers would have had poor outcomes after acute stroke because of difficulties with communication with the healthcare team, in fact we found they had reduced mortal-ity, and better performance on some quality of care measures. These differences existed despite adjustment for many poten-tial confounders, including ethnicity, prognostic factors, and stroke characteristics. Greater understanding is needed of the mechanisms through which these patients achieved bet-ter stroke outcomes, and of the methods of translating these mechanisms to the remainder of the population.
AcknowledgmentsWe wish to thank Eriola Asllani, Maria Chiu, Jiming Fang, and Jeremiah Hwee for their assistance with the acquisition of data and the analyses.
Sources of FundingThe study was funded by the Canadian Institute for Health Research (CIHR), grant number MOP-102641. Dr Shah is supported by a new investigator award from the CIHR. Dr Kapral is supported by a career investigator award from the Heart and Stroke Foundation, Ontario Provincial Office. The Institute for Clinical Evaluative Sciences (ICES) is a nonprofit research institute funded by the Ontario Ministry of Health and Long-Term Care (MOHLTC). The Ontario Stroke Registry is funded by the Canadian Stroke Network and the MOHLTC. The opinions, results, and conclusions reported in these studies are those of the authors and are independent from the funding sources. No endorsement by the funders, ICES, or the MOHLTC is intended or should be inferred.
DisclosuresNone.
References 1. Flores G, Laws MB, Mayo SJ, Zuckerman B, Abreu M, Medina L, et al.
Errors in medical interpretation and their potential clinical consequences in pediatric encounters. Pediatrics. 2003;111:6–14.
2. Scheppers E, van Dongen E, Dekker J, Geertzen J, Dekker J. Potential barriers to the use of health services among ethnic minorities: a review. Fam Pract. 2006;23:325–348. doi: 10.1093/fampra/cmi113.
3. Flores G. The impact of medical interpreter services on the quality of health care: a systematic review. Med Care Res Rev. 2005;62:255–299. doi: 10.1177/1077558705275416.
4. Okrainec K, Booth GL, Hollands S, Bell CM. Impact of language bar-riers on complications and mortality among immigrants with diabetes: a population-based cohort study. Diabetes Care. 2015;38:189–196. doi: 10.2337/dc14-0801.
5. Grubbs V, Bibbins-Domingo K, Fernandez A, Chattopadhyay A, Bindman A. Acute myocardial infarction length of stay and hospital mortality are not associated with language preference. J Gen Intern Med 2008;23:190–194.
6. John-Baptiste A, Naglie G, Tomlinson G, Alibhai SM, Etchells E, Cheung A, et al. The effect of English language proficiency on length of stay and in-hospital mortality. J Gen Intern Med. 2004;19:221–228.
7. Bhandari VK, Wang F, Bindman AB, Schillinger D. Quality of antico-agulation control: do race and language matter? J Health Care Poor Underserved. 2008;19:41–55. doi: 10.1353/hpu.2008.0002.
8. The Ontario Stroke Registry Web site. 2013. https://osr.ices.on.ca. Accessed October 15, 2014.
9. Lindsay MP, Gubitz G, Bayley M, Phillips S, eds. Canadian Best Practice Recommendations for Stroke Car. 4th ed. Ottawa: Canadian Stroke Network; 2013.
10. Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45:613–619.
11. O’Donnell MJ, Fang J, D’Uva C, Saposnik G, Gould L, McGrath E, et al; Investigators of the Registry of the Canadian Stroke Network. The PLAN score: a bedside prediction rule for death and severe disability following acute ischemic stroke. Arch Intern Med. 2012;172:1548–1556. doi: 10.1001/2013.jamainternmed.30.
12. Craney TA, Surles JG. Model-dependent variance inflation factor cutoff values. Qual Eng 2002;14:391–403.
13. Kelly AG, Hoskins KD, Holloway RG. Early stroke mortality, patient preferences, and the withdrawal of care bias. Neurology. 2012;79:941–944. doi: 10.1212/WNL.0b013e318266fc40.
14. Shen Q, Cordato DJ, Chan DK, Kokkinos J. Comparison of stroke risk factors and outcomes in patients with English-speaking back-ground versus non-English-speaking background. Neuroepidemiology. 2005;24:79–86. doi: 10.1159/000081054.
15. Smith MA, Lisabeth LD, Bonikowski F, Morgenstern LB. The role of ethnicity, sex, and language on delay to hospital arrival for acute ischemic stroke. Stroke. 2010;41:905–909. doi: 10.1161/STROKEAHA.110.578112.
16. Ayers JW. Measuring English proficiency and language preference: are self-reports valid? Am J Public Health. 2010;100:1364–1366.
17. Statistics Canada. Language Highlight Tables, 2006 Census. Ottawa: Statistics Canada; 2007. Report No.: 97-555-XWE2006002.
by guest on May 28, 2018
http://stroke.ahajournals.org/D
ownloaded from

Baiju R. Shah, Nadia A. Khan, Martin J. O'Donnell and Moira K. KapralImpact of Language Barriers on Stroke Care and Outcomes
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 2015 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke doi: 10.1161/STROKEAHA.114.007929
2015;46:813-818; originally published online February 5, 2015;Stroke.
http://stroke.ahajournals.org/content/46/3/813World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org/content/suppl/2015/02/05/STROKEAHA.114.007929.DC1Data Supplement (unedited) at:
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in the
Request Permissions in the middle column of the Web page under Services. Further information about thisOnce the online version of the published article for which permission is being requested is located, click
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Strokein Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on May 28, 2018
http://stroke.ahajournals.org/D
ownloaded from

SUPPLEMENTAL MATERIAL
The impact of language barriers on stroke care and outcomes

SUPPLEMENTAL TABLE I
Definitions for outcome variables.
Outcome Definition Data source Population where measured
MORTALITY AND STROKE OUTCOMES 7 day mortality Death within 7 days of stroke
onset RPDB All patients
30 day mortality Death within 30 days of stroke onset
RPDB All patients
1 year mortality Death within 365 days of stroke onset
RPDB All patients
Moderate to severe residual neurological deficit
Modified Rankin Score 3 to 5 RCSN All patients discharged alive from hospital
IN HOSPITAL COMPLICATIONS Decubitis ulcer Decubitis ulcer in hospital and
within 30 days of stroke onset RCSN All patients
Fall with fracture Fall with fracture in hospital and within 30 days of stroke onset
RCSN All patients
Pneumonia Pneumonia in hospital and within 30 days of stroke onset
RCSN All patients
Thromboembolic complications
Deep vein thrombosis or pulmonary embolism in hospital and within 30 days of stroke onset
RCSN All patients
DISPOSITION Length of stay Days from hospital admission
to discharge RCSN All patients
Discharge to home or rehabilitation hospital
Patient was discharged from hospital to their home or to a rehabilitation hospital (vs. to another acute care institution, a long-term care facility, or a nursing home)
RCSN All patients discharged alive from hospital
QUALITY OF CARE Received thrombolysis Received thrombolysis
treatment for acute stroke RCSN All patients with ischemic
stroke who arrived to hospital within 2.5 hours of stroke onset and who had no contraindications to thrombolysis (age ≥80 years, major CT changes, comfort measures only, decreased level of consciousness, PTT >40 s, INR >1.4, platelets <100 x103/mL, blood pressure >185/100 mmHg, glucose <3 or >22 mmol/L, rapidly improving

symptoms, recent bleeding, trauma or surgery; seizures at onset)
Door to needle time Minutes from hospital arrival to administration of thrombolysis
RCSN All patients with ischemic stroke who arrived to hospital within 2.5 hours of stroke onset and who had no contraindications to thrombolysis (as above)
Brain imaging within 24 hours
First brain imaging within 24 hours of stroke onset
RCSN All patients
Occupational therapist assessment
Assessed by an occupational therapist while in hospital
RCSN All patients
Physiotherapist assessment
Assessed by a physiotherapist while in hospital
RCSN All patients
Speech-language pathologist assessment
Assessed by a speech-language pathologist while in hospital
RCSN All patients
Social worker assessment Assessed by a social worker while in hospital
RCSN All patients
Nutritionist assessment Assessed by a nutritionist while in hospital
RCSN All patients
Carotid imaging within 2 weeks
Completed while in hospital or booked as an outpatient, any of the following: carotid Doppler; or carotid catheter, MR or CT angiogram
RCSN All patients with TIA or ischemic stroke, excluding those with posterior circulation territory, with a history of cancer or dementia, in palliative care or a nursing home, or with disabling or fatal stroke
Discharge prescription for aspirin or warfarin
Prescribed aspirin or warfarin at discharge, or aspiring and warfarin both contraindicated
RCSN All patients with TIA or ischemic stroke
Discharge prescription for antihypertensives
Prescribed a antihypertensive medication at discharge
RCSN All patients with TIA or ischemic stroke
Discharge prescription for statins
Prescribed a statin at discharge
RCSN All patients with TIA or ischemic stroke
INR = international normalized ratio; PTT = partial thromboplastin time; RCSN = Registry of the Canadian
Stroke Network; RPDB = Registered Persons Database; TIA = transient ischemic attacks.

SUPPLEMENTAL TABLE II
Definitions for baseline characteristics.
Outcome Definition Data source DEMOGRAPHICS Age As of admission date RPDB Sex RPDB Ethnicity Categorized as Caucasian or other RCSN Socioeconomic status Average neighborhood household income,
determined using patient’s home postal code, divided into quintiles
RPDB and 2006 Canadian Census
COMORBIDITY Charlson comorbidity score Based on history recorded during the index
hospitalization, and diagnoses coded for any other hospitalizations up to 1 year previously
RCSN and DAD
Hypertension History of hypertension noted at hospitalization RCSN Hyperlipidemia History of hyperlipidemia noted at hospitalization RCSN Diabetes History of diabetes noted at hospitalization RCSN Coronary artery disease History of angina, myocardial infarction or coronary
revascularization noted at hospitalization RCSN
Congestive heart failure History of congestive heart failure or pulmonary edema noted at hospitalization
RCSN
Atrial fibrillation History of atrial fibrillation or flutter noted at hospitalization
RCSN
Peripheral vascular disease History of peripheral vascular disease noted at hospitalization
RCSN
Previous stroke / TIA History of previous stroke or TIA noted at hospitalization
RCSN
Cancer History of cancer noted at hospitalization RCSN Dementia History of dementia noted at hospitalization RCSN Dependence History of dependence for some/all activities of daily
living noted at hospitalization RCSN
CLINICAL FEATURES Stroke type Final diagnosis, categorized as TIA, ischemic stroke
or hemorrhagic stroke RCSN
Level of consciousness Level of consciousness on arrival to hospital, categorized as alert, drowsy or unconscious
RCSN
Arm weakness, severe Significant or total proximal arm weakness on arrival to hospital
RCSN
Leg weakness, severe Significant or total proximal leg weakness on arrival to hospital
RCSN
Asphasia or neglect Receptive aphasia, expressive aphasia, neglect or inattention on arrival to hospital
RCSN
Glucose ≥10 mmol/L Initial laboratory testing on arrival to hospital RCSN WBC count ≥10 x109/L Initial laboratory testing on arrival to hospital RCSN Hemoglobin ≤110 g/L Initial laboratory testing on arrival to hospital RCSN Temperature <36°C or >38°C Initial vital signs on arrival to hospital RCSN AGGRESSIVE VS SUPPORTIVE CARE DURING HOSPITALIZATION Admission to a stroke unit Any part of the hospitalization on a dedicated stroke
unit RCSN
Admission to an intensive care unit
Any part of the hospitalization in an intensive care unit
RCSN

Nasogastric tube Inserted or used during the hospitalization RCSN Permanent feeding tube Inserted or used during the hospitalization RCSN Neurologist assessment Assessed by a neurologist while in hospital RCSN and OHIP Palliative care Palliative care during the hospitalization RCSN
DAD = Discharge Abstracts Database; OHIP = Ontario Health Insurance Plan’s claim database; RCSN =
Registry of the Canadian Stroke Network; RPDB = Registered Persons Database; TIA = transient
ischemic attacks.