Embed Size (px)
Citation preview
Listen to this manuscript’s
audio summary by
JACC Editor-in-Chief
Dr. Valentin Fuster.
J O U R N A L O F T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y V O L . 6 8 , N O . 1 6 , 2 0 1 6
ª 2 0 1 6 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O UN DA T I O N
P U B L I S H E D B Y E L S E V I E R
I S S N 0 7 3 5 - 1 0 9 7 / $ 3 6 . 0 0
h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j a c c . 2 0 1 6 . 0 7 . 7 5 6
Impact of Ischemic Heart Failure Etiologyon Cardiac Recovery DuringMechanical Unloading
James Wever-Pinzon, MD,a Craig H. Selzman, MD,a,b Greg Stoddard, MPH, MBA,a Omar Wever-Pinzon, MD,aAnna Catino, MD,a Abdallah G. Kfoury, MD,a Nikolaos A. Diakos, MD,a,b Bruce B. Reid, MD,a Stephen McKellar, MD,a,b
Michael Bonios, MD, PHD,a Antigone Koliopoulou, MD,a Deborah Budge, MD,b Aaron Kelkhoff, MD,a
Josef Stehlik, MD,a James C. Fang, MD,a Stavros G. Drakos, MD, PHDa,b
ABSTRACT
Fro
Int
Ut
cov
Dr
Tra
an
Ne
fro
oth
Ma
BACKGROUND Small-scale studies focused mainly on nonischemic cardiomyopathy (NICM) have shown that a subset
of left ventricular assist device (LVAD) patients can achieve significant improvement of their native heart function,
but the impact of ischemic cardiomyopathy (ICM) has not been specifically investigated. Many patients with acute
myocardial infarction are discharged from their index hospitalization without heart failure (HF), only to return much later
with overt HF syndrome, mainly caused by chronic remodeling of the noninfarcted region of the myocardium.
OBJECTIVES This study sought to prospectively investigate the effect of ICM HF etiology on LVAD-associated
improvement of cardiac structure and function using NICM as control.
METHODS Consecutive patients (n ¼ 154) with documented chronic and dilated cardiomyopathy (ICM, n ¼ 61; NICM,
n ¼ 93) requiring durable support with continuous-flow LVAD were prospectively evaluated with serial echocardiograms
and right heart catheterizations.
RESULTS In patients supported with LVAD for at least 6 months, we found that 5% of subjects with ICM and 21% of
subjects with NICM achieved left ventricular ejection fraction $40% (p ¼ 0.034). LV end-diastolic and end-systolic
volumes and diastolic function were significantly and similarly improved in patients with ICM and NICM.
CONCLUSIONS LVAD-associated unloading for 6 months resulted in a substantial improvement in myocardial
structure, and systolic and diastolic function in 1 in 20 ICM and 1 in 5 NICM patients. These specific incidence and
timeline findings may provide guidance in clinical practice and research design for sequencing and prioritizing
advanced HF and heart transplantation therapeutic options in patients with ICM and NICM. (J Am Coll Cardiol
2016;68:1741–52) © 2016 by the American College of Cardiology Foundation.
L eft ventricular assist devices (LVADs) areincreasingly used in the management ofpatients with advanced heart failure (HF)
nonresponsive to traditional therapeutic modalities,
m the aUtah Transplantation Affiliated Hospitals Cardiac Transplant Pr
ermountain Medical Center, Veterans Affairs Salt Lake City Health Care
ah Molecular Medicine Program, Salt Lake City, Utah. This work was fun
ery Grant (15CVGPSD27690000, to Dr. Drakos), the Doris Duke Foundat
. Drakos), National Institutes of Health National Center for Research Re
nslational Sciences (UL1-RR025764 and C06-RR11234 to Drs. Drakos and K
dMedical Foundation (00571, to Drs. Drakos and Kfoury), and the American
twork - Clinical Project 1 (to Dr. Drakos). Dr. Stehlik has received research s
mSt. JudeMedical andHeartware. Dr. Drakos has received research suppor
er authors have reported that they have no relationships relevant to the c
nuscript received April 12, 2016; revised manuscript received July 7, 2016
as a bridge to transplant or as permanent therapy(1). LVADs improve symptoms, exercise tolerance,quality of life, and survival in this population.Furthermore, the intriguing observation that some
ogram, University of Utah Health Sciences Center,
System, Salt Lake City, Utah; and the bUniversity of
ded by the American Heart Association CVGPS Dis-
ion Clinical Scientist Development Grant (7/2013, to
sources grant that supports the Center for Clinical
foury), Deseret Foundation/Intermountain Research
Heart Association HF Strategically Focused Research
upport from St. Jude Medical; and speaker honoraria
t fromAbiomed; and is a consultant for Heartware. All
ontents of this paper to disclose.
, accepted July 12, 2016.

ABBR EV I A T I ON S
AND ACRONYMS
CI = confidence interval
HF = heart failure
ICM = ischemic cardiomyopathy
LV = left ventricle
LVAD = left ventricular
assist device
LVEDD = left ventricular
end-diastolic diameter
LVEF = left ventricular ejection
fraction
MI = myocardial infarction
NICM = nonischemic
cardiomyopathy
Wever-Pinzon et al. J A C C V O L . 6 8 , N O . 1 6 , 2 0 1 6
HF Etiology and LVAD-Induced Myocardial Recovery O C T O B E R 1 8 , 2 0 1 6 : 1 7 4 1 – 5 2
1742
patients with advanced chronic HF undergo-ing LVAD support can experience reverseremodeling and significant improvement ofmyocardial function suggests that LVAD-associated mechanical unloading of thefailing heart may be a plausible therapeuticstrategy aimed at myocardial recovery anddevice removal, avoiding the need for hearttransplantation (2–6).
The availability of myocardial tissuecollected at the time of LVAD implantationand explantation has allowed characteriza-tion of individuals who experienced signifi-cant recovery of myocardial function duringmechanical unloading. The genetic, molecu-lar, cellular, and structural bases of this ob-
served phenomenon are now being unveiled (7–10).However, the optimal approach to prospectivelyidentify patients who would benefit from electiveLVAD insertion as a bridge to recovery remains un-known. The impact of the etiology of HF on the po-tential for myocardial recovery is not wellunderstood. The field has primarily focused on pa-tients with nonischemic cardiomyopathy (NICM),reasoning that patients with chronic ischemic car-diomyopathy (ICM) would have experienced irre-versible scarring following myocardial infarction (MI)that would hamper their chances for recovery. How-ever, a large number of patients with acute MI, evensome with large anterior wall MI, are discharged fromtheir index hospitalization without HF symptoms toreturn later with overt HF syndrome, mainly causedby chronic remodeling of the noninfarcted regions ofthe myocardium (11,12).
SEE PAGE 1753
A few studies suggested a low incidence ofmyocardial recovery in ICM (13,14), but lack a pre-specified protocol to monitor for structural andfunctional changes serially. We aimed to prospec-tively evaluate the effect of mechanical unloading onmyocardial structure and function in a large cohort ofpatients with chronic end-stage cardiomyopathysupported with continuous-flow LVADs, and to assessthe effects and natural history of mechanicalunloading on patients with ICM in relation to patientswith NICM using a serial and systematic approach.
METHODS
STUDY POPULATION. Patients with end-stage car-diomyopathy who underwent implantation of acontinuous-flow LVAD as a bridge to transplant or asdestination therapy between 2008 and 2014 at the
institutions comprising the Utah TransplantationAffiliated Hospitals Cardiac Transplant Program(i.e., University of Utah Health Science Center,Intermountain Medical Center, and the VeteransAdministration Salt Lake City Health Care System)were enrolled after obtaining informed consent.Patients with acute forms of HF, defined bysymptoms <3 months of duration with no evidence ofLV dilation, were prospectively excluded. Subjectswith hypertrophic or infiltrative cardiomyopathieswere also excluded from this study. The study wasapproved by the institutional review board of theparticipating institutions.
Chronic ICM was defined as a left ventricularejection fraction (LVEF) <40% and any of thefollowing: 1) a history of MI or revascularization; 2) ahistory of angina or chest pain and evidence of scar-ring in noninvasive imaging studies corresponding toprevious MI; 3) presence of $75% stenosis of the leftmain or proximal left anterior descending artery; or 4)presence of $75% stenosis of $2 epicardial vessels ina patient with unexplained cardiomyopathy. Patientswith a LVEF <40% and nonobstructive coronary ar-tery disease without evidence of prior MI or revas-cularization were considered to have NICM.PHARMACOLOGICAL THERAPY. Medical manage-ment was at the discretion of the treating physicianswithin the Utah Transplantation Affiliated HospitalsCardiac Transplant Program. The use of beta-blockers, angiotensin-converting enzyme inhibitors,and aldosterone antagonists (i.e., standard HF drugtherapy) after device implantation was encouraged.CLINICAL PROTOCOL. Clinically relevant data werecollected within 1 week preceding LVAD implanta-tion. Right heart catheterization was performedwithin 1 week preceding LVAD implantation andwithin 6 to 8 weeks after implantation to documentadequacy of left ventricular pressure unloading. Asper our clinical protocol, cardiac resynchronizationtherapy was discontinued in all study subjects.
Before patients were discharged home, the effectof LVAD unloading on cardiac size, shape, and func-tion was assessed by echocardiography. The devicespeed was adjusted to achieve adequate flows andoptimal LV and right ventricle decompression withpositioning of the interventricular and interatrialsepta in the midline plus minimum mitral valveregurgitation. Aortic valve opening was desirable butconsidered of lower priority compared with the con-ditions outlined previously. Subsequent adjustmentsof the speed were made as indicated by patients’symptoms or clinical events.ASSESSMENT OF CARDIAC RECOVERY. Surveillancefor functional recovery was undertaken using a
J A C C V O L . 6 8 , N O . 1 6 , 2 0 1 6 Wever-Pinzon et al.O C T O B E R 1 8 , 2 0 1 6 : 1 7 4 1 – 5 2 HF Etiology and LVAD-Induced Myocardial Recovery
1743
protocol developed and tested at the Utah CardiacRecovery Program (15). Briefly, we performed trans-thoracic echocardiograms within 2 weeks precedingLVAD implantation, and then at months 1, 2, 3, 4, 6, 9,and 12 after implantation. Echocardiographic mea-surements were made at full and reduced support orturn-down study (30 min after reducing speed to thelowest recommended by manufacturer). Turn-downstudies were not performed in patients with a his-tory of stroke, transient ischemic attack, LVADthrombosis, hemolysis, or with subtherapeutic inter-national normalized ratio. Complete 2-dimensional,M-mode, and Doppler images were recorded fromstandard views in accordance with current AmericanSociety of Echocardiography guidelines (16,17), and aswe previously described (15).
STATISTICAL ANALYSES. Standard summary de-scriptors were used (e.g., frequencies, percentages,and means). Measures of variation were presented inthe form of SD and SEM. Patient characteristiccomparisons between ICM and NICM groups weremade with a chi-square test or Fisher exact test, asappropriate for unordered categorical variables, witha Wilcoxon-Mann-Whitney test for ordered categori-cal variables, and with an independent sample Stu-dent t test for continuous variables.
For the comparison between groups, the primaryoutcome was defined as LVEF at 6 months post-LVAD,based on our previous results where peak of functionalimprovement after LVAD implantation was achievedat 6 months (15). All other outcomes and time pointsare secondary comparisons. In this primary-secondaryframework, there is no need to apply a multiple com-parison procedure to adjust the p values, because only1 comparison is required (18,19).
Separately, for each of the ischemic and non-ischemic patients, to describe changes from baselineto specific follow-up times, we used a paired sampleStudent t test. Because they are secondary endpointsdescribing the natural history of improvement, noadjustment for multiple comparison was made.
To estimate the effect size of the etiology of thecardiomyopathy on the chances for experiencingmeaningful recovery of cardiac function duringLVAD support, we created an operational definitionof sustained recovery where all of the followingconditions needed to be met: the presence of 2 ormore consecutive post-LVAD LVEF $40% at anyfollow-up time, and no LVEF <40% after the initialLVEF $40%. To adjust for confounding, we per-formed a propensity score analysis in 2 steps. In thefirst step, we used 9 potential confounders (age atLVAD implantation, body mass index, diabetes
mellitus, history of hypertension, LVAD indication,baseline LVEF, left ventricular end-diastolicdysfunction [LVEDD], serum sodium, and creati-nine levels). We identified these variables throughanalysis of pre-LVAD baseline characteristics of bothgroups as predictor variables for ischemic status in amultivariable logistic regression, using an interactivebackward variable selection until 6 of these variablesconfounders remained in the model with p < 0.20.The predicted probability of ICM status was obtainedfrom this logistic model to represent the propensityscore. In the derivation of the propensity score, weused hotdeck imputation of missing values, as 1variable (LVEDD) was missing 6.5% of its values, 2variables were missing 4.5% of their values (serumsodium and creatinine levels), and the remaindermissing either 1 or 2 values. In the second step, wefit a logistic regression model with sustained recov-ery as the outcome (1 ¼ recovered; 0 ¼ not recov-ered), ischemic status as the primary predictor, andthe propensity score as a covariate.
All analyses were performed using STATA softwareversion 14 (StataCorp LP, College Station, Texas).
RESULTS
CHARACTERISTICS OF PATIENTS BEFORE LVAD
IMPLANTATION. A total of 169 patients underwentLVAD implantation during the study period. We pro-spectively excluded subjects with acute forms of HF,including acute MI, acute myocarditis, and post-cardiotomy cardiogenic shock (n ¼ 13). By doing sowe eliminated a group of patients with a likely higherpropensity for natural cardiac recovery. We alsoexcluded 2 patients with hypertrophic and infiltrativecardiomyopathies. The remaining 154 subjects withchronic advanced cardiomyopathy were prospec-tively enrolled after obtaining informed written con-sent. The baseline characteristics of patients with ICMand NICM at the time of LVAD implantation areshown in Table 1. The ICM group was older (mean age,63 vs. 52 years) and had a significantly higher preva-lence of diabetes and hypertension when comparedwith the NICM group. As expected, given our inclu-sion and exclusion criteria, both groups had longduration of HF symptoms and LV dilation. The meanduration of symptoms was 7 years in the ICM groupand 6 years in the NICM group (p ¼ 0.48). The meanLVEDD was 6.5 cm in the ICM group and 7.0 cm in theNICM group (p < 0.01). There was no significant dif-ference between groups in terms of severity of HFsymptoms, use of temporary mechanical support, orLVAD indication.
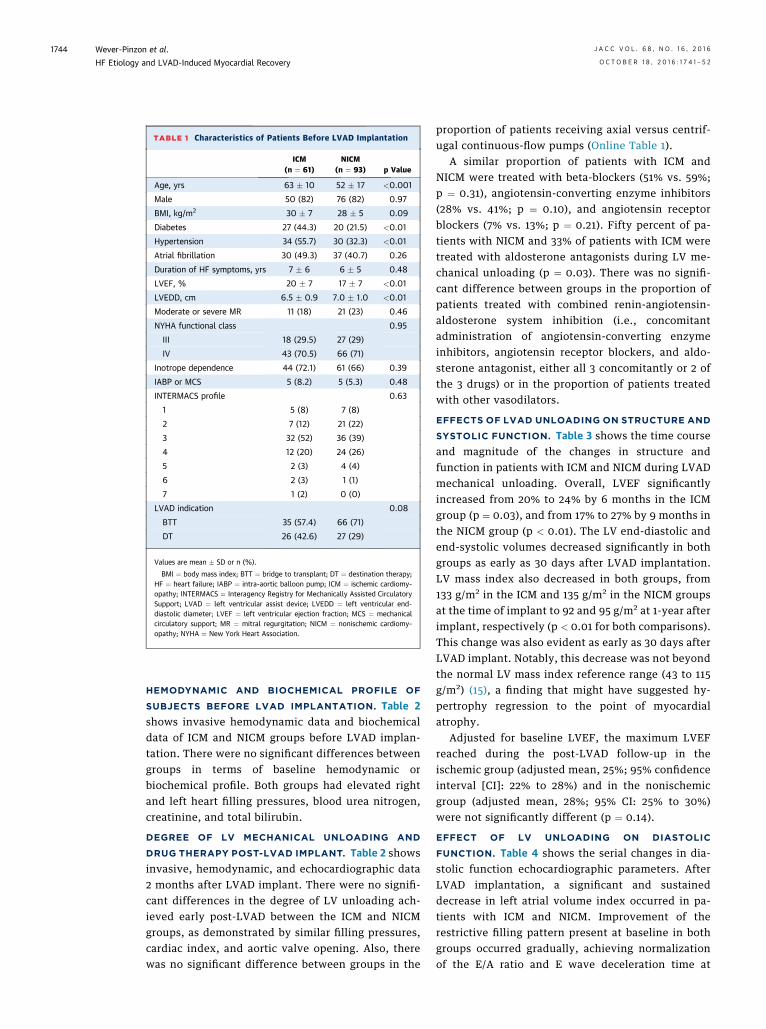
TABLE 1 Characteristics of Patients Before LVAD Implantation
ICM(n ¼ 61)
NICM(n ¼ 93) p Value
Age, yrs 63 � 10 52 � 17 <0.001
Male 50 (82) 76 (82) 0.97
BMI, kg/m2 30 � 7 28 � 5 0.09
Diabetes 27 (44.3) 20 (21.5) <0.01
Hypertension 34 (55.7) 30 (32.3) <0.01
Atrial fibrillation 30 (49.3) 37 (40.7) 0.26
Duration of HF symptoms, yrs 7 � 6 6 � 5 0.48
LVEF, % 20 � 7 17 � 7 <0.01
LVEDD, cm 6.5 � 0.9 7.0 � 1.0 <0.01
Moderate or severe MR 11 (18) 21 (23) 0.46
NYHA functional class 0.95
III 18 (29.5) 27 (29)
IV 43 (70.5) 66 (71)
Inotrope dependence 44 (72.1) 61 (66) 0.39
IABP or MCS 5 (8.2) 5 (5.3) 0.48
INTERMACS profile 0.63
1 5 (8) 7 (8)
2 7 (12) 21 (22)
3 32 (52) 36 (39)
4 12 (20) 24 (26)
5 2 (3) 4 (4)
6 2 (3) 1 (1)
7 1 (2) 0 (0)
LVAD indication 0.08
BTT 35 (57.4) 66 (71)
DT 26 (42.6) 27 (29)
Values are mean � SD or n (%).
BMI ¼ body mass index; BTT ¼ bridge to transplant; DT ¼ destination therapy;HF ¼ heart failure; IABP ¼ intra-aortic balloon pump; ICM ¼ ischemic cardiomy-opathy; INTERMACS ¼ Interagency Registry for Mechanically Assisted CirculatorySupport; LVAD ¼ left ventricular assist device; LVEDD ¼ left ventricular end-diastolic diameter; LVEF ¼ left ventricular ejection fraction; MCS ¼ mechanicalcirculatory support; MR ¼ mitral regurgitation; NICM ¼ nonischemic cardiomy-opathy; NYHA ¼ New York Heart Association.
Wever-Pinzon et al. J A C C V O L . 6 8 , N O . 1 6 , 2 0 1 6
HF Etiology and LVAD-Induced Myocardial Recovery O C T O B E R 1 8 , 2 0 1 6 : 1 7 4 1 – 5 2
1744
HEMODYNAMIC AND BIOCHEMICAL PROFILE OF
SUBJECTS BEFORE LVAD IMPLANTATION. Table 2shows invasive hemodynamic data and biochemicaldata of ICM and NICM groups before LVAD implan-tation. There were no significant differences betweengroups in terms of baseline hemodynamic orbiochemical profile. Both groups had elevated rightand left heart filling pressures, blood urea nitrogen,creatinine, and total bilirubin.
DEGREE OF LV MECHANICAL UNLOADING AND
DRUG THERAPY POST-LVAD IMPLANT. Table 2 showsinvasive, hemodynamic, and echocardiographic data2 months after LVAD implant. There were no signifi-cant differences in the degree of LV unloading ach-ieved early post-LVAD between the ICM and NICMgroups, as demonstrated by similar filling pressures,cardiac index, and aortic valve opening. Also, therewas no significant difference between groups in the
proportion of patients receiving axial versus centrif-ugal continuous-flow pumps (Online Table 1).
A similar proportion of patients with ICM andNICM were treated with beta-blockers (51% vs. 59%;p ¼ 0.31), angiotensin-converting enzyme inhibitors(28% vs. 41%; p ¼ 0.10), and angiotensin receptorblockers (7% vs. 13%; p ¼ 0.21). Fifty percent of pa-tients with NICM and 33% of patients with ICM weretreated with aldosterone antagonists during LV me-chanical unloading (p ¼ 0.03). There was no signifi-cant difference between groups in the proportion ofpatients treated with combined renin-angiotensin-aldosterone system inhibition (i.e., concomitantadministration of angiotensin-converting enzymeinhibitors, angiotensin receptor blockers, and aldo-sterone antagonist, either all 3 concomitantly or 2 ofthe 3 drugs) or in the proportion of patients treatedwith other vasodilators.
EFFECTS OF LVAD UNLOADING ON STRUCTURE AND
SYSTOLIC FUNCTION. Table 3 shows the time courseand magnitude of the changes in structure andfunction in patients with ICM and NICM during LVADmechanical unloading. Overall, LVEF significantlyincreased from 20% to 24% by 6 months in the ICMgroup (p ¼ 0.03), and from 17% to 27% by 9 months inthe NICM group (p < 0.01). The LV end-diastolic andend-systolic volumes decreased significantly in bothgroups as early as 30 days after LVAD implantation.LV mass index also decreased in both groups, from133 g/m2 in the ICM and 135 g/m2 in the NICM groupsat the time of implant to 92 and 95 g/m2 at 1-year afterimplant, respectively (p < 0.01 for both comparisons).This change was also evident as early as 30 days afterLVAD implant. Notably, this decrease was not beyondthe normal LV mass index reference range (43 to 115g/m2) (15), a finding that might have suggested hy-pertrophy regression to the point of myocardialatrophy.
Adjusted for baseline LVEF, the maximum LVEFreached during the post-LVAD follow-up in theischemic group (adjusted mean, 25%; 95% confidenceinterval [CI]: 22% to 28%) and in the nonischemicgroup (adjusted mean, 28%; 95% CI: 25% to 30%)were not significantly different (p ¼ 0.14).
EFFECT OF LV UNLOADING ON DIASTOLIC
FUNCTION. Table 4 shows the serial changes in dia-stolic function echocardiographic parameters. AfterLVAD implantation, a significant and sustaineddecrease in left atrial volume index occurred in pa-tients with ICM and NICM. Improvement of therestrictive filling pattern present at baseline in bothgroups occurred gradually, achieving normalizationof the E/A ratio and E wave deceleration time at
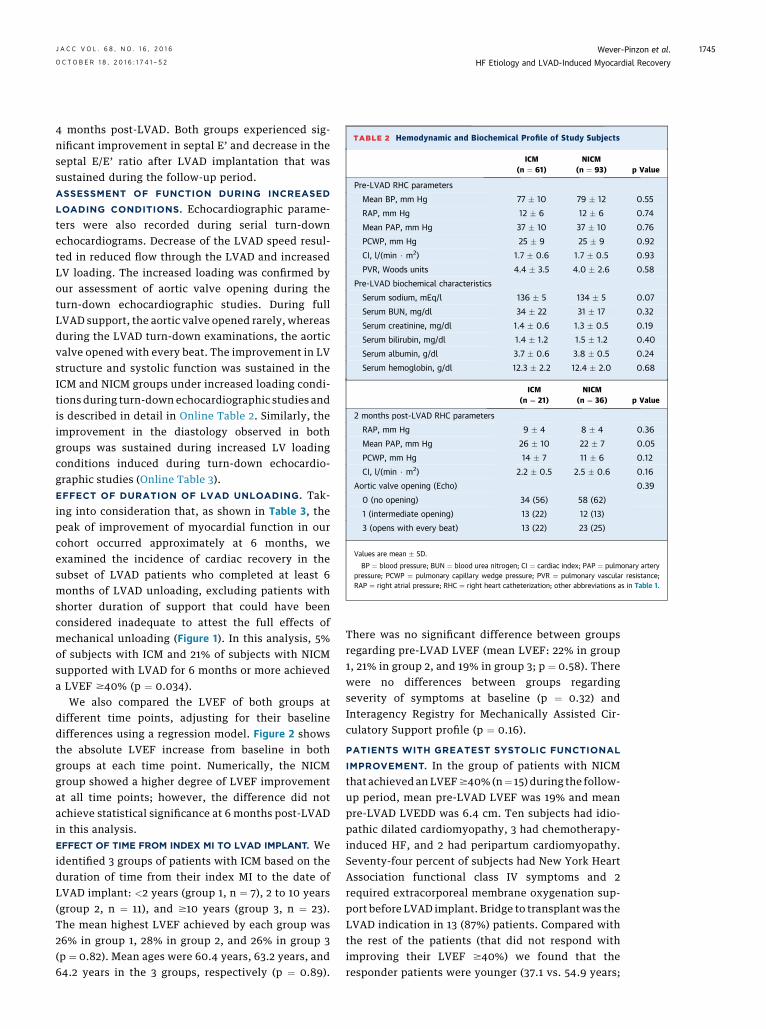
TABLE 2 Hemodynamic and Biochemical Profile of Study Subjects
ICM(n ¼ 61)
NICM(n ¼ 93) p Value
Pre-LVAD RHC parameters
Mean BP, mm Hg 77 � 10 79 � 12 0.55
RAP, mm Hg 12 � 6 12 � 6 0.74
Mean PAP, mm Hg 37 � 10 37 � 10 0.76
PCWP, mm Hg 25 � 9 25 � 9 0.92
CI, l/(min $ m2) 1.7 � 0.6 1.7 � 0.5 0.93
PVR, Woods units 4.4 � 3.5 4.0 � 2.6 0.58
Pre-LVAD biochemical characteristics
Serum sodium, mEq/l 136 � 5 134 � 5 0.07
Serum BUN, mg/dl 34 � 22 31 � 17 0.32
Serum creatinine, mg/dl 1.4 � 0.6 1.3 � 0.5 0.19
Serum bilirubin, mg/dl 1.4 � 1.2 1.5 � 1.2 0.40
Serum albumin, g/dl 3.7 � 0.6 3.8 � 0.5 0.24
Serum hemoglobin, g/dl 12.3 � 2.2 12.4 � 2.0 0.68
ICM(n ¼ 21)
NICM(n ¼ 36) p Value
2 months post-LVAD RHC parameters
RAP, mm Hg 9 � 4 8 � 4 0.36
Mean PAP, mm Hg 26 � 10 22 � 7 0.05
PCWP, mm Hg 14 � 7 11 � 6 0.12
CI, l/(min $ m2) 2.2 � 0.5 2.5 � 0.6 0.16
Aortic valve opening (Echo) 0.39
0 (no opening) 34 (56) 58 (62)
1 (intermediate opening) 13 (22) 12 (13)
3 (opens with every beat) 13 (22) 23 (25)
Values are mean � SD.
BP ¼ blood pressure; BUN ¼ blood urea nitrogen; CI ¼ cardiac index; PAP ¼ pulmonary arterypressure; PCWP ¼ pulmonary capillary wedge pressure; PVR ¼ pulmonary vascular resistance;RAP ¼ right atrial pressure; RHC ¼ right heart catheterization; other abbreviations as in Table 1.
J A C C V O L . 6 8 , N O . 1 6 , 2 0 1 6 Wever-Pinzon et al.O C T O B E R 1 8 , 2 0 1 6 : 1 7 4 1 – 5 2 HF Etiology and LVAD-Induced Myocardial Recovery
1745
4 months post-LVAD. Both groups experienced sig-nificant improvement in septal E’ and decrease in theseptal E/E’ ratio after LVAD implantation that wassustained during the follow-up period.ASSESSMENT OF FUNCTION DURING INCREASED
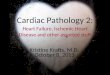
LOADING CONDITIONS. Echocardiographic parame-ters were also recorded during serial turn-downechocardiograms. Decrease of the LVAD speed resul-ted in reduced flow through the LVAD and increasedLV loading. The increased loading was confirmed byour assessment of aortic valve opening during theturn-down echocardiographic studies. During fullLVAD support, the aortic valve opened rarely, whereasduring the LVAD turn-down examinations, the aorticvalve opened with every beat. The improvement in LVstructure and systolic function was sustained in theICM and NICM groups under increased loading condi-tions during turn-down echocardiographic studies andis described in detail in Online Table 2. Similarly, theimprovement in the diastology observed in bothgroups was sustained during increased LV loadingconditions induced during turn-down echocardio-graphic studies (Online Table 3).EFFECT OF DURATION OF LVAD UNLOADING. Tak-ing into consideration that, as shown in Table 3, thepeak of improvement of myocardial function in ourcohort occurred approximately at 6 months, weexamined the incidence of cardiac recovery in thesubset of LVAD patients who completed at least 6months of LVAD unloading, excluding patients withshorter duration of support that could have beenconsidered inadequate to attest the full effects ofmechanical unloading (Figure 1). In this analysis, 5%of subjects with ICM and 21% of subjects with NICMsupported with LVAD for 6 months or more achieveda LVEF $40% (p ¼ 0.034).
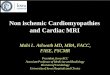
We also compared the LVEF of both groups atdifferent time points, adjusting for their baselinedifferences using a regression model. Figure 2 showsthe absolute LVEF increase from baseline in bothgroups at each time point. Numerically, the NICMgroup showed a higher degree of LVEF improvementat all time points; however, the difference did notachieve statistical significance at 6 months post-LVADin this analysis.EFFECT OF TIME FROM INDEX MI TO LVAD IMPLANT. Weidentified 3 groups of patients with ICM based on theduration of time from their index MI to the date ofLVAD implant: <2 years (group 1, n ¼ 7), 2 to 10 years(group 2, n ¼ 11), and $10 years (group 3, n ¼ 23).The mean highest LVEF achieved by each group was26% in group 1, 28% in group 2, and 26% in group 3(p ¼ 0.82). Mean ages were 60.4 years, 63.2 years, and64.2 years in the 3 groups, respectively (p ¼ 0.89).
There was no significant difference between groupsregarding pre-LVAD LVEF (mean LVEF: 22% in group1, 21% in group 2, and 19% in group 3; p ¼ 0.58). Therewere no differences between groups regardingseverity of symptoms at baseline (p ¼ 0.32) andInteragency Registry for Mechanically Assisted Cir-culatory Support profile (p ¼ 0.16).
PATIENTS WITH GREATEST SYSTOLIC FUNCTIONAL
IMPROVEMENT. In the group of patients with NICMthat achieved an LVEF$40% (n¼ 15) during the follow-up period, mean pre-LVAD LVEF was 19% and meanpre-LVAD LVEDD was 6.4 cm. Ten subjects had idio-pathic dilated cardiomyopathy, 3 had chemotherapy-induced HF, and 2 had peripartum cardiomyopathy.Seventy-four percent of subjects had New York HeartAssociation functional class IV symptoms and 2required extracorporeal membrane oxygenation sup-port before LVAD implant. Bridge to transplant was theLVAD indication in 13 (87%) patients. Compared withthe rest of the patients (that did not respond withimproving their LVEF $40%) we found that theresponder patients were younger (37.1 vs. 54.9 years;
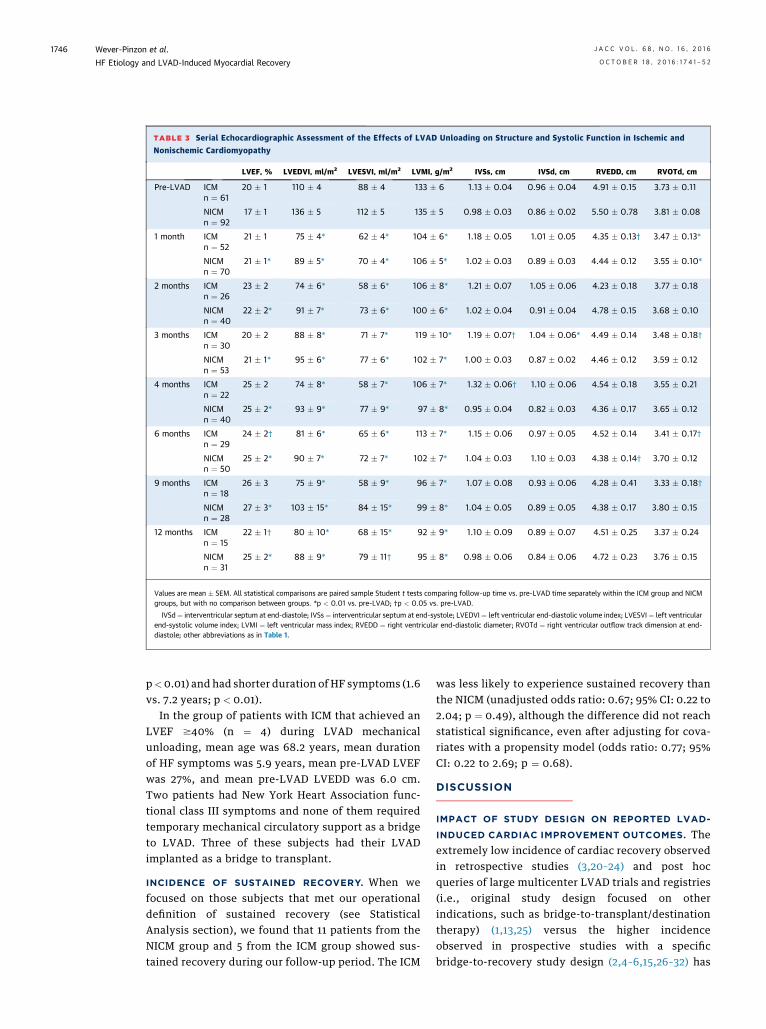
TABLE 3 Serial Echocardiographic Assessment of the Effects of LVAD Unloading on Structure and Systolic Function in Ischemic and
Nonischemic Cardiomyopathy
LVEF, % LVEDVI, ml/m2 LVESVI, ml/m2 LVMI, g/m2 IVSs, cm IVSd, cm RVEDD, cm RVOTd, cm
Pre-LVAD ICMn ¼ 61
20 � 1 110 � 4 88 � 4 133 � 6 1.13 � 0.04 0.96 � 0.04 4.91 � 0.15 3.73 � 0.11
NICMn ¼ 92
17 � 1 136 � 5 112 � 5 135 � 5 0.98 � 0.03 0.86 � 0.02 5.50 � 0.78 3.81 � 0.08
1 month ICMn ¼ 52
21 � 1 75 � 4* 62 � 4* 104 � 6* 1.18 � 0.05 1.01 � 0.05 4.35 � 0.13† 3.47 � 0.13*
NICMn ¼ 70
21 � 1* 89 � 5* 70 � 4* 106 � 5* 1.02 � 0.03 0.89 � 0.03 4.44 � 0.12 3.55 � 0.10*
2 months ICMn ¼ 26
23 � 2 74 � 6* 58 � 6* 106 � 8* 1.21 � 0.07 1.05 � 0.06 4.23 � 0.18 3.77 � 0.18
NICMn ¼ 40
22 � 2* 91 � 7* 73 � 6* 100 � 6* 1.02 � 0.04 0.91 � 0.04 4.78 � 0.15 3.68 � 0.10
3 months ICMn ¼ 30
20 � 2 88 � 8* 71 � 7* 119 � 10* 1.19 � 0.07† 1.04 � 0.06* 4.49 � 0.14 3.48 � 0.18†
NICMn ¼ 53
21 � 1* 95 � 6* 77 � 6* 102 � 7* 1.00 � 0.03 0.87 � 0.02 4.46 � 0.12 3.59 � 0.12
4 months ICMn ¼ 22
25 � 2 74 � 8* 58 � 7* 106 � 7* 1.32 � 0.06† 1.10 � 0.06 4.54 � 0.18 3.55 � 0.21
NICMn ¼ 40
25 � 2* 93 � 9* 77 � 9* 97 � 8* 0.95 � 0.04 0.82 � 0.03 4.36 � 0.17 3.65 � 0.12
6 months ICMn ¼ 29
24 � 2† 81 � 6* 65 � 6* 113 � 7* 1.15 � 0.06 0.97 � 0.05 4.52 � 0.14 3.41 � 0.17†
NICMn ¼ 50
25 � 2* 90 � 7* 72 � 7* 102 � 7* 1.04 � 0.03 1.10 � 0.03 4.38 � 0.14† 3.70 � 0.12
9 months ICMn ¼ 18
26 � 3 75 � 9* 58 � 9* 96 � 7* 1.07 � 0.08 0.93 � 0.06 4.28 � 0.41 3.33 � 0.18†
NICMn ¼ 28
27 � 3* 103 � 15* 84 � 15* 99 � 8* 1.04 � 0.05 0.89 � 0.05 4.38 � 0.17 3.80 � 0.15
12 months ICMn ¼ 15
22 � 1† 80 � 10* 68 � 15* 92 � 9* 1.10 � 0.09 0.89 � 0.07 4.51 � 0.25 3.37 � 0.24
NICMn ¼ 31
25 � 2* 88 � 9* 79 � 11† 95 � 8* 0.98 � 0.06 0.84 � 0.06 4.72 � 0.23 3.76 � 0.15
Values are mean � SEM. All statistical comparisons are paired sample Student t tests comparing follow-up time vs. pre-LVAD time separately within the ICM group and NICMgroups, but with no comparison between groups. *p < 0.01 vs. pre-LVAD; †p < 0.05 vs. pre-LVAD.
IVSd¼ interventricular septum at end-diastole; IVSs ¼ interventricular septum at end-systole; LVEDVI¼ left ventricular end-diastolic volume index; LVESVI¼ left ventricularend-systolic volume index; LVMI ¼ left ventricular mass index; RVEDD ¼ right ventricular end-diastolic diameter; RVOTd ¼ right ventricular outflow track dimension at end-diastole; other abbreviations as in Table 1.
Wever-Pinzon et al. J A C C V O L . 6 8 , N O . 1 6 , 2 0 1 6
HF Etiology and LVAD-Induced Myocardial Recovery O C T O B E R 1 8 , 2 0 1 6 : 1 7 4 1 – 5 2
1746
p<0.01) and had shorter duration of HF symptoms (1.6vs. 7.2 years; p < 0.01).
In the group of patients with ICM that achieved anLVEF $40% (n ¼ 4) during LVAD mechanicalunloading, mean age was 68.2 years, mean durationof HF symptoms was 5.9 years, mean pre-LVAD LVEFwas 27%, and mean pre-LVAD LVEDD was 6.0 cm.Two patients had New York Heart Association func-tional class III symptoms and none of them requiredtemporary mechanical circulatory support as a bridgeto LVAD. Three of these subjects had their LVADimplanted as a bridge to transplant.
INCIDENCE OF SUSTAINED RECOVERY. When wefocused on those subjects that met our operationaldefinition of sustained recovery (see StatisticalAnalysis section), we found that 11 patients from theNICM group and 5 from the ICM group showed sus-tained recovery during our follow-up period. The ICM
was less likely to experience sustained recovery thanthe NICM (unadjusted odds ratio: 0.67; 95% CI: 0.22 to2.04; p ¼ 0.49), although the difference did not reachstatistical significance, even after adjusting for cova-riates with a propensity model (odds ratio: 0.77; 95%CI: 0.22 to 2.69; p ¼ 0.68).
DISCUSSION
IMPACT OF STUDY DESIGN ON REPORTED LVAD-
INDUCED CARDIAC IMPROVEMENT OUTCOMES. Theextremely low incidence of cardiac recovery observedin retrospective studies (3,20–24) and post hocqueries of large multicenter LVAD trials and registries(i.e., original study design focused on otherindications, such as bridge-to-transplant/destinationtherapy) (1,13,25) versus the higher incidenceobserved in prospective studies with a specificbridge-to-recovery study design (2,4–6,15,26–32) has
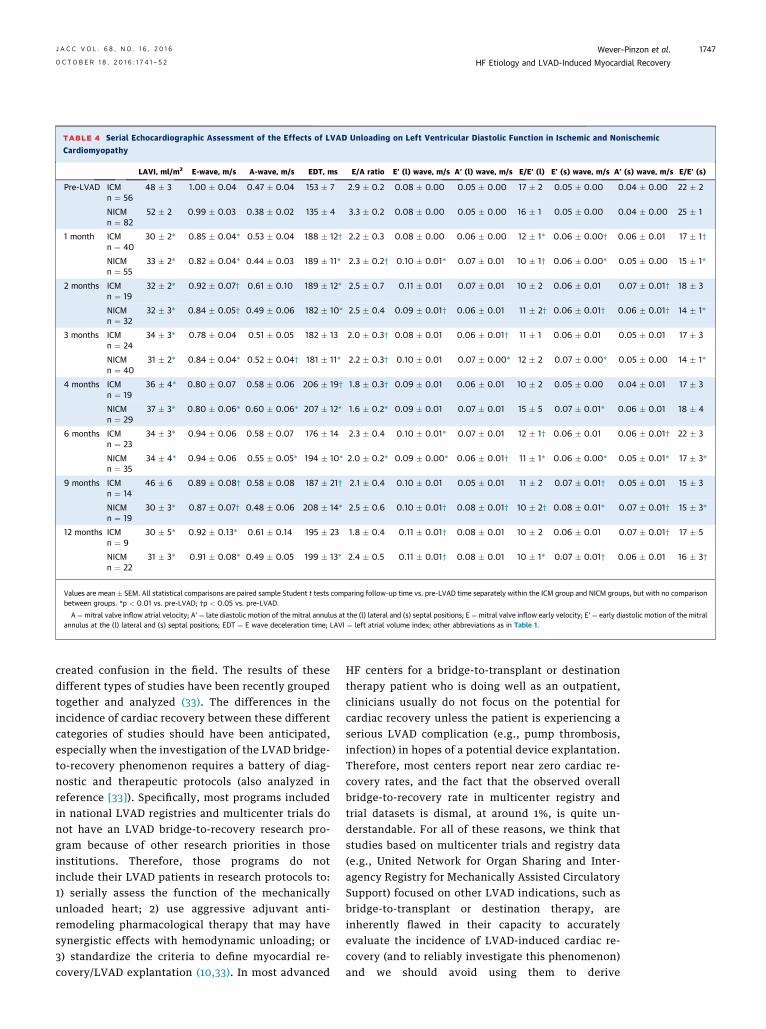
TABLE 4 Serial Echocardiographic Assessment of the Effects of LVAD Unloading on Left Ventricular Diastolic Function in Ischemic and Nonischemic
Cardiomyopathy
LAVI, ml/m2 E-wave, m/s A-wave, m/s EDT, ms E/A ratio E’ (l) wave, m/s A’ (l) wave, m/s E/E’ (l) E’ (s) wave, m/s A’ (s) wave, m/s E/E’ (s)
Pre-LVAD ICMn ¼ 56
48 � 3 1.00 � 0.04 0.47 � 0.04 153 � 7 2.9 � 0.2 0.08 � 0.00 0.05 � 0.00 17 � 2 0.05 � 0.00 0.04 � 0.00 22 � 2
NICMn ¼ 82
52 � 2 0.99 � 0.03 0.38 � 0.02 135 � 4 3.3 � 0.2 0.08 � 0.00 0.05 � 0.00 16 � 1 0.05 � 0.00 0.04 � 0.00 25 � 1
1 month ICMn ¼ 40
30 � 2* 0.85 � 0.04* 0.53 � 0.04 188 � 12† 2.2 � 0.3 0.08 � 0.00 0.06 � 0.00 12 � 1* 0.06 � 0.00† 0.06 � 0.01 17 � 1†
NICMn ¼ 55
33 � 2* 0.82 � 0.04* 0.44 � 0.03 189 � 11* 2.3 � 0.2† 0.10 � 0.01* 0.07 � 0.01 10 � 1† 0.06 � 0.00* 0.05 � 0.00 15 � 1*
2 months ICMn ¼ 19
32 � 2* 0.92 � 0.07† 0.61 � 0.10 189 � 12* 2.5 � 0.7 0.11 � 0.01 0.07 � 0.01 10 � 2 0.06 � 0.01 0.07 � 0.01† 18 � 3
NICMn ¼ 32
32 � 3* 0.84 � 0.05† 0.49 � 0.06 182 � 10* 2.5 � 0.4 0.09 � 0.01† 0.06 � 0.01 11 � 2† 0.06 � 0.01† 0.06 � 0.01† 14 � 1*
3 months ICMn ¼ 24
34 � 3* 0.78 � 0.04 0.51 � 0.05 182 � 13 2.0 � 0.3† 0.08 � 0.01 0.06 � 0.01† 11 � 1 0.06 � 0.01 0.05 � 0.01 17 � 3
NICMn ¼ 40
31 � 2* 0.84 � 0.04* 0.52 � 0.04† 181 � 11* 2.2 � 0.3† 0.10 � 0.01 0.07 � 0.00* 12 � 2 0.07 � 0.00* 0.05 � 0.00 14 � 1*
4 months ICMn ¼ 19
36 � 4* 0.80 � 0.07 0.58 � 0.06 206 � 19† 1.8 � 0.3† 0.09 � 0.01 0.06 � 0.01 10 � 2 0.05 � 0.00 0.04 � 0.01 17 � 3
NICMn ¼ 29
37 � 3* 0.80 � 0.06* 0.60 � 0.06* 207 � 12* 1.6 � 0.2* 0.09 � 0.01 0.07 � 0.01 15 � 5 0.07 � 0.01* 0.06 � 0.01 18 � 4
6 months ICMn ¼ 23
34 � 3* 0.94 � 0.06 0.58 � 0.07 176 � 14 2.3 � 0.4 0.10 � 0.01* 0.07 � 0.01 12 � 1† 0.06 � 0.01 0.06 � 0.01† 22 � 3
NICMn ¼ 35
34 � 4* 0.94 � 0.06 0.55 � 0.05* 194 � 10* 2.0 � 0.2* 0.09 � 0.00* 0.06 � 0.01† 11 � 1* 0.06 � 0.00* 0.05 � 0.01* 17 � 3*
9 months ICMn ¼ 14
46 � 6 0.89 � 0.08† 0.58 � 0.08 187 � 21† 2.1 � 0.4 0.10 � 0.01 0.05 � 0.01 11 � 2 0.07 � 0.01† 0.05 � 0.01 15 � 3
NICMn ¼ 19
30 � 3* 0.87 � 0.07† 0.48 � 0.06 208 � 14* 2.5 � 0.6 0.10 � 0.01† 0.08 � 0.01† 10 � 2† 0.08 � 0.01* 0.07 � 0.01† 15 � 3*
12 months ICMn ¼ 9
30 � 5* 0.92 � 0.13* 0.61 � 0.14 195 � 23 1.8 � 0.4 0.11 � 0.01† 0.08 � 0.01 10 � 2 0.06 � 0.01 0.07 � 0.01† 17 � 5
NICMn ¼ 22
31 � 3* 0.91 � 0.08* 0.49 � 0.05 199 � 13* 2.4 � 0.5 0.11 � 0.01† 0.08 � 0.01 10 � 1* 0.07 � 0.01† 0.06 � 0.01 16 � 3†
Values are mean � SEM. All statistical comparisons are paired sample Student t tests comparing follow-up time vs. pre-LVAD time separately within the ICM group and NICM groups, but with no comparisonbetween groups. *p < 0.01 vs. pre-LVAD; †p < 0.05 vs. pre-LVAD.
A ¼mitral valve inflow atrial velocity; A’ ¼ late diastolic motion of the mitral annulus at the (l) lateral and (s) septal positions; E ¼mitral valve inflow early velocity; E’ ¼ early diastolic motion of the mitralannulus at the (l) lateral and (s) septal positions; EDT ¼ E wave deceleration time; LAVI ¼ left atrial volume index; other abbreviations as in Table 1.
J A C C V O L . 6 8 , N O . 1 6 , 2 0 1 6 Wever-Pinzon et al.O C T O B E R 1 8 , 2 0 1 6 : 1 7 4 1 – 5 2 HF Etiology and LVAD-Induced Myocardial Recovery
1747
created confusion in the field. The results of thesedifferent types of studies have been recently groupedtogether and analyzed (33). The differences in theincidence of cardiac recovery between these differentcategories of studies should have been anticipated,especially when the investigation of the LVAD bridge-to-recovery phenomenon requires a battery of diag-nostic and therapeutic protocols (also analyzed inreference [33]). Specifically, most programs includedin national LVAD registries and multicenter trials donot have an LVAD bridge-to-recovery research pro-gram because of other research priorities in thoseinstitutions. Therefore, those programs do notinclude their LVAD patients in research protocols to:1) serially assess the function of the mechanicallyunloaded heart; 2) use aggressive adjuvant anti-remodeling pharmacological therapy that may havesynergistic effects with hemodynamic unloading; or3) standardize the criteria to define myocardial re-covery/LVAD explantation (10,33). In most advanced
HF centers for a bridge-to-transplant or destinationtherapy patient who is doing well as an outpatient,clinicians usually do not focus on the potential forcardiac recovery unless the patient is experiencing aserious LVAD complication (e.g., pump thrombosis,infection) in hopes of a potential device explantation.Therefore, most centers report near zero cardiac re-covery rates, and the fact that the observed overallbridge-to-recovery rate in multicenter registry andtrial datasets is dismal, at around 1%, is quite un-derstandable. For all of these reasons, we think thatstudies based on multicenter trials and registry data(e.g., United Network for Organ Sharing and Inter-agency Registry for Mechanically Assisted CirculatorySupport) focused on other LVAD indications, such asbridge-to-transplant or destination therapy, areinherently flawed in their capacity to accuratelyevaluate the incidence of LVAD-induced cardiac re-covery (and to reliably investigate this phenomenon)and we should avoid using them to derive
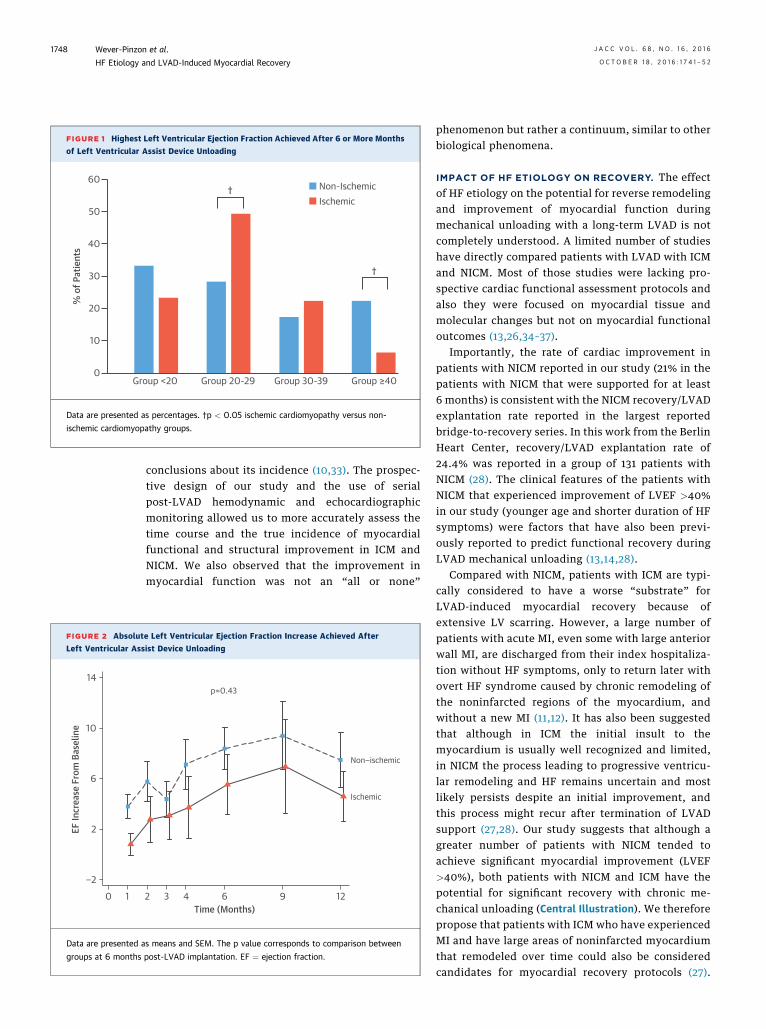
FIGURE 1 Highest Left Ventricular Ejection Fraction Achieved After 6 or More Months
of Left Ventricular Assist Device Unloading
60
50
40
30
20
10
0Group <20 Group 20-29 Group 30-39 Group ≥40
% o
f Pat
ient
s
Non-IschemicIschemic
†
†
Data are presented as percentages. †p < 0.05 ischemic cardiomyopathy versus non-
ischemic cardiomyopathy groups.
FIGURE 2 Absolut
Left Ventricular Ass
−2
2
6
10
14
EF In
crea
se F
rom
Bas
elin
e
0 1
Data are presented a
groups at 6 months
Wever-Pinzon et al. J A C C V O L . 6 8 , N O . 1 6 , 2 0 1 6
HF Etiology and LVAD-Induced Myocardial Recovery O C T O B E R 1 8 , 2 0 1 6 : 1 7 4 1 – 5 2
1748
conclusions about its incidence (10,33). The prospec-tive design of our study and the use of serialpost-LVAD hemodynamic and echocardiographicmonitoring allowed us to more accurately assess thetime course and the true incidence of myocardialfunctional and structural improvement in ICM andNICM. We also observed that the improvement inmyocardial function was not an “all or none”
e Left Ventricular Ejection Fraction Increase Achieved After
ist Device Unloading
p=0.43
Non−ischemic
Ischemic
2 3 4 6 9 12Time (Months)
s means and SEM. The p value corresponds to comparison between
post-LVAD implantation. EF ¼ ejection fraction.
phenomenon but rather a continuum, similar to otherbiological phenomena.
IMPACT OF HF ETIOLOGY ON RECOVERY. The effectof HF etiology on the potential for reverse remodelingand improvement of myocardial function duringmechanical unloading with a long-term LVAD is notcompletely understood. A limited number of studieshave directly compared patients with LVAD with ICMand NICM. Most of those studies were lacking pro-spective cardiac functional assessment protocols andalso they were focused on myocardial tissue andmolecular changes but not on myocardial functionaloutcomes (13,26,34–37).
Importantly, the rate of cardiac improvement inpatients with NICM reported in our study (21% in thepatients with NICM that were supported for at least6 months) is consistent with the NICM recovery/LVADexplantation rate reported in the largest reportedbridge-to-recovery series. In this work from the BerlinHeart Center, recovery/LVAD explantation rate of24.4% was reported in a group of 131 patients withNICM (28). The clinical features of the patients withNICM that experienced improvement of LVEF >40%in our study (younger age and shorter duration of HFsymptoms) were factors that have also been previ-ously reported to predict functional recovery duringLVAD mechanical unloading (13,14,28).
Compared with NICM, patients with ICM are typi-cally considered to have a worse “substrate” forLVAD-induced myocardial recovery because ofextensive LV scarring. However, a large number ofpatients with acute MI, even some with large anteriorwall MI, are discharged from their index hospitaliza-tion without HF symptoms, only to return later withovert HF syndrome caused by chronic remodeling ofthe noninfarcted regions of the myocardium, andwithout a new MI (11,12). It has also been suggestedthat although in ICM the initial insult to themyocardium is usually well recognized and limited,in NICM the process leading to progressive ventricu-lar remodeling and HF remains uncertain and mostlikely persists despite an initial improvement, andthis process might recur after termination of LVADsupport (27,28). Our study suggests that although agreater number of patients with NICM tended toachieve significant myocardial improvement (LVEF>40%), both patients with NICM and ICM have thepotential for significant recovery with chronic me-chanical unloading (Central Illustration). We thereforepropose that patients with ICM who have experiencedMI and have large areas of noninfarcted myocardiumthat remodeled over time could also be consideredcandidates for myocardial recovery protocols (27).
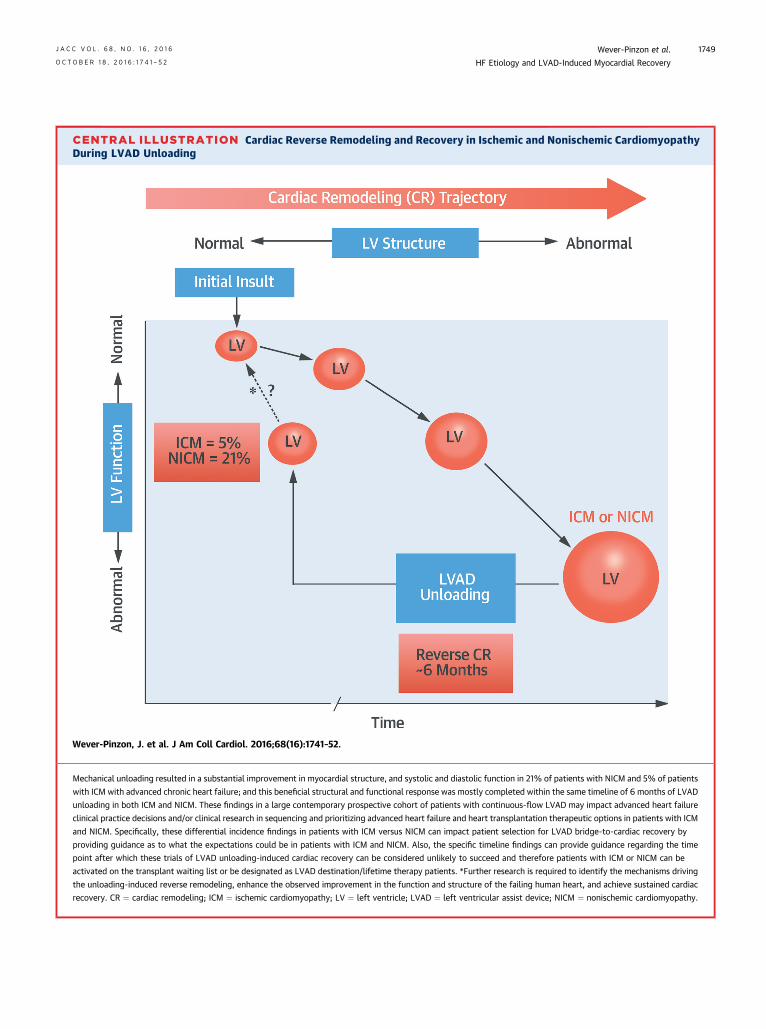
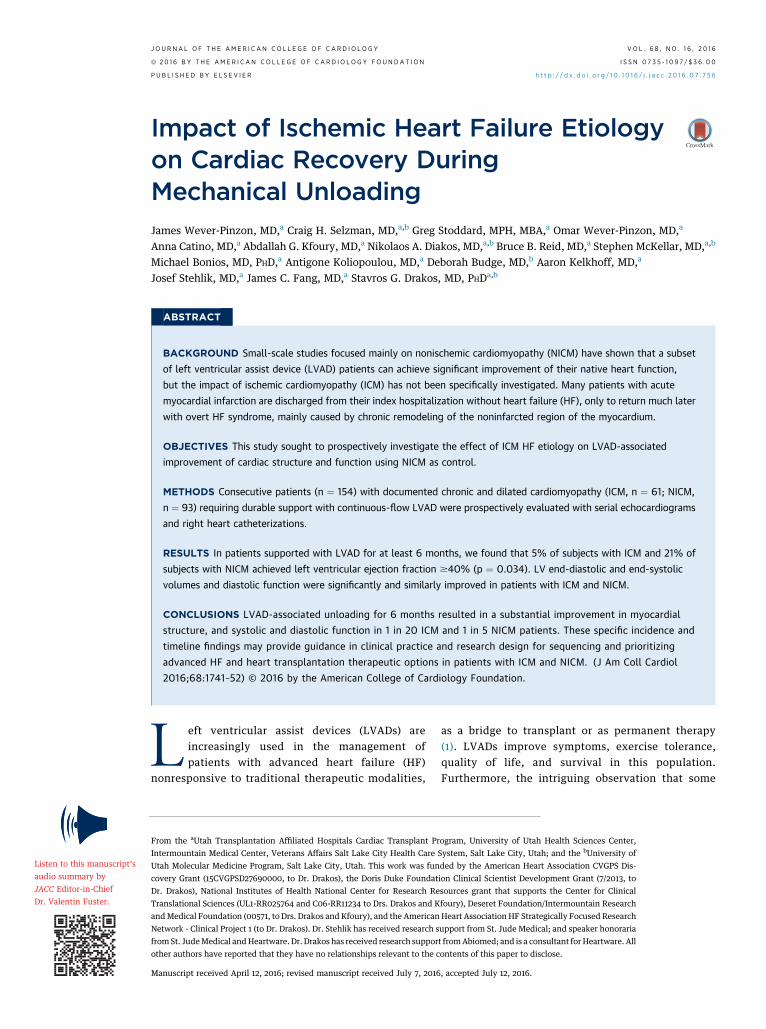
CENTRAL ILLUSTRATION Cardiac Reverse Remodeling and Recovery in Ischemic and Nonischemic CardiomyopathyDuring LVAD Unloading
Wever-Pinzon, J. et al. J Am Coll Cardiol. 2016;68(16):1741–52.
Mechanical unloading resulted in a substantial improvement in myocardial structure, and systolic and diastolic function in 21% of patients with NICM and 5% of patients
with ICM with advanced chronic heart failure; and this beneficial structural and functional response was mostly completed within the same timeline of 6 months of LVAD
unloading in both ICM and NICM. These findings in a large contemporary prospective cohort of patients with continuous-flow LVAD may impact advanced heart failure
clinical practice decisions and/or clinical research in sequencing and prioritizing advanced heart failure and heart transplantation therapeutic options in patients with ICM
and NICM. Specifically, these differential incidence findings in patients with ICM versus NICM can impact patient selection for LVAD bridge-to-cardiac recovery by
providing guidance as to what the expectations could be in patients with ICM and NICM. Also, the specific timeline findings can provide guidance regarding the time
point after which these trials of LVAD unloading-induced cardiac recovery can be considered unlikely to succeed and therefore patients with ICM or NICM can be
activated on the transplant waiting list or be designated as LVAD destination/lifetime therapy patients. *Further research is required to identify the mechanisms driving
the unloading-induced reverse remodeling, enhance the observed improvement in the function and structure of the failing human heart, and achieve sustained cardiac
recovery. CR ¼ cardiac remodeling; ICM ¼ ischemic cardiomyopathy; LV ¼ left ventricle; LVAD ¼ left ventricular assist device; NICM ¼ nonischemic cardiomyopathy.
J A C C V O L . 6 8 , N O . 1 6 , 2 0 1 6 Wever-Pinzon et al.O C T O B E R 1 8 , 2 0 1 6 : 1 7 4 1 – 5 2 HF Etiology and LVAD-Induced Myocardial Recovery
1749

Wever-Pinzon et al. J A C C V O L . 6 8 , N O . 1 6 , 2 0 1 6
HF Etiology and LVAD-Induced Myocardial Recovery O C T O B E R 1 8 , 2 0 1 6 : 1 7 4 1 – 5 2
1750
This concept deserves further investigation and couldcombine the excision of scarred myocardium, usingLV reconstruction techniques (e.g., Dor operation),with LVAD unloading. It can be argued that with thisapproach the initial insult that triggered the cascadeof cardiac remodeling progression (i.e., the post-MIscar) has been eliminated (27).
Interestingly, the subset of patients with ICM withthe highest functional response in our study were notyounger and did not have shorter time from index MIto LVAD implant or shorter duration of HF symptoms(as found for the patients with NICM). We believeimprovement of myocardial function in ICM maydepend on other factors. For example, up to 50% ofpatients with advanced ICM have hibernatingmyocardium (38–42), but do not undergo revasculari-zation for several reasons. LVAD support in this pop-ulation offers a stable platform to test the viable andjeopardized myocardium at risk as a potential thera-peutic target to induce reverse remodeling andmyocardial recovery. Although we could not establisha relationship between functional improvement andviability/hibernating myocardium at baseline, thenumber of patients with ICM that had viability testingbefore LVAD implant was small (less than one-third)and this is a limitation of our study. Prospectivestudies with pre-specified protocols to test for viabilitybefore and after LVAD implant maybe warranted.
IMPACT OF DURATION OF LVAD UNLOADING. Ourstudy showed that peak LVEF in ICM and NICM sub-jects is achieved approximately 6 months after LVADimplantation (Central Illustration). These findingssuggest that, just as many other cardiac-specifictherapies need a reasonable amount of time beforeexerting their curative effect, a critical duration ofmechanical unloading may be necessary to inducereverse remodeling and functional improvement.Translational LVAD studies have also attempted toidentify this optimal time when maximal potentiationof myocardial recovery occurs (26,43,44). In com-parison with those studies the peak of recovery in ourstudy was achieved later during mechanical supportand with no sign of regression subsequently. How-ever, it is likely that the optimal duration of me-chanical support may vary among patients, because itcould be affected by underlying patient characteris-tics (e.g., age, duration of HF symptoms, HF etiology,comorbidities) or even device characteristics (pulsa-tile vs. continuous flow, centrifugal vs. axial flow, andso forth). This argument could explain individualvariations in the time to highest LVEF achieved afterLVAD support within a single study. A long-standingquestion directly related to the sustainability of
LVAD-induced cardiac improvement is whether pro-longed LVAD unloading induces regression of cardiachypertrophy to the point of atrophy and degenera-tion. Our results show that the LV mass decreased inICM and NICM with continuous-flow LVAD unload-ing, but remained within the normal reference rangeduring the 1-year follow-up period. These findings arein agreement with our prior findings that demon-strated no histological, microstructural, molecular,and metabolic evidence of induced atrophy in anLVAD population (45).
STUDY LIMITATIONS. The reliability of LVAD turn-down studies to predict long-term sustainability ofmyocardial recovery (e.g., after device explantation)has not been established and as such this is a limita-tion of our study. The protocol to induce increasedloading conditions on the LV used in our study issimilar to published protocols used in bridge-to-recovery LVAD studies that led to sustained myocar-dial recovery post-LVAD explant (2,4,28). In thelargest series reported so far this protocol was asso-ciated with a 5-year freedom of HF recurrence of 69%(28). More importantly, our findings that during LVADturn-down studies some failing human hearts cansubstantially improve in structure and function,whereas other similarly sick hearts undergoing thesame LVAD chronic unloading do not show anyimprovement, strongly suggest that the observedreverse remodeling and structural and functionalimprovement during mechanical unloading is a realphenotype (and not a universal acute phenomenonattributed to the acute removal of load). These resultsinvite further clinical and translational investigationsthat could significantly advance the field of cardiacrecovery.
The number of observations at each pre-specifiedtime point decreased gradually as subjects got trans-planted or as some died from their disease or com-plications. Online Table 4 shows the frequencies offatalities and heart transplants. To reduce the impactof a decreasing number of individuals, either becauseof death of “sicker” patients or because of hearttransplantation in the healthier subset, we studiedchanges in the outcome variables from baseline tospecific time points using paired sample Student t testanalysis. In addition, we reported on and emphasizedthe outcomes of the subset of patients that was sup-ported with a LVAD for at least 6 months.
Our study did not assign LVAD patients to standardHF drug therapy versus no HF drug therapy so wecannot reliably determine the contribution of medicaltherapy during LVAD support to the observed degreeof cardiac improvement (randomizing LVAD patients

PERSPECTIVES
COMPETENCY IN MEDICAL KNOWLEDGE: The
improvement of myocardial function after mechanical unloading
in patients with end-stage heart failure is not restricted to
nonischemic cardiomyopathy, but also occurs in those with
chronic ischemic cardiomyopathy.
TRANSLATIONAL OUTLOOK: Future research should explore
the mechanisms by which mechanical unloading enhances car-
diac recovery in patients with end-stage ischemic
cardiomyopathy.
J A C C V O L . 6 8 , N O . 1 6 , 2 0 1 6 Wever-Pinzon et al.O C T O B E R 1 8 , 2 0 1 6 : 1 7 4 1 – 5 2 HF Etiology and LVAD-Induced Myocardial Recovery
1751
to no HF drug therapy would have been inappropriategiven the current national and international HF andmechanical circulatory support guidelines). However,a similar proportion of patients with ICM andNICM were treated with beta-blockers, angiotensin-converting enzyme inhibitors, and angiotensin re-ceptor blockers or their combination. We did notinclude the average dose of medications in eachgroup and this is a limitation of our study.
Our research protocol did not include routine car-diopulmonary testing in this population and, there-fore, we cannot correlate structural and functionalchanges with exercise response and peak oxygenconsumption.
CONCLUSIONS
In a significant subset of patients with NICM and asmaller subset of patients with ICM, continuous-flowLVAD unloading induced early improvement inmyocardial structure and systolic and diastolic func-tion. These improvements plateaued after approxi-mately 6 months of support with no evidence ofsubsequent improvement regression. Future studiesare needed to prospectively investigate which char-acteristics specific to ICM (myocardial scar size,viability, or others) and NICM can help predict dura-ble cardiac recovery after device explantation.
In addition, considering that the observed improve-ment was induced in patients with end-stage cardio-myopathy, these prospective findings demonstratethe clinical and translational potential of the field ofmechanical unloading and cardiac recovery for thebroader, less ill HF populations.
REPRINT REQUESTS AND CORRESPONDENCE: Dr.Stavros G. Drakos, Division of Cardiovascular Medi-cine, University of Utah, 15 North 2030 East, Room4420, Salt Lake City, Utah. E-mail: [email protected].
RE F E RENCE S
1. Kirklin JK, Naftel DC, Pagani FD, et al. SixthINTERMACS annual report: a 10,000-patientdatabase. J Heart Lung Transplant 2014;33:555–64.
2. Birks EJ, Tansley PD, Hardy J, et al. Left ven-tricular assist device and drug therapy for thereversal of heart failure. N Engl J Med 2006;355:1873–84.
3. Matsumiya G, Monta O, Fukushima N, et al. Whowould be a candidate for bridge to recovery duringprolonged mechanical left ventricular support inidiopathic dilated cardiomyopathy? J Thorac Car-diovasc Surg 2005;130:699–704.
4. Birks EJ, George RS, Hedger M, et al. Reversalof severe heart failure with a continuous-flow leftventricular assist device and pharmacologicaltherapy: a prospective study. Circulation 2011;123:381–90.
5. Patel SR, Saeed O, Murthy S, et al. Combiningneurohormonal blockade with continuous-flowleft ventricular assist device support for myocar-dial recovery: a single-arm prospective study.J Heart Lung Transplant 2013;32:305–12.
6. Frazier OH, Baldwin AC, Demirozu ZT, et al.Ventricular reconditioning and pump explantationin patients supported by continuous-flow leftventricular assist devices. J Heart Lung Transplant2015;34:766–72.
7. Terracciano CM, Hardy J, Birks EJ, Khaghani A,Banner NR, Yacoub MH. Clinical recovery fromend-stage heart failure using left-ventricular assistdevice and pharmacological therapy correlateswith increased sarcoplasmic reticulum calciumcontent but not with regression of cellular hy-pertrophy. Circulation 2004;109:2263–5.
8. Hall JL, Birks EJ, Grindle S, et al. Molecularsignature of recovery following combination leftventricular assist device (LVAD) support andpharmacologic therapy. Eur Heart J 2007;28:613–27.
9. Canseco DC, Kimura W, Garg S, et al. Humanventricular unloading induces cardiomyocyte pro-liferation. J Am Coll Cardiol 2015;65:892–900.
10. Drakos SG, Kfoury AG, Stehlik J, et al. Bridgeto recovery: understanding the disconnect be-tween clinical and biological outcomes. Circulation2012;126:230–41.
11. Bolognese L, Neskovic AN, Parodi G, et al. Leftventricular remodeling after primary coronaryangioplasty: patterns of left ventricular dilationand long-term prognostic implications. Circulation2002;106:2351–7.
12. Hellermann JP, Jacobsen SJ, Redfield MM,et al. Heart failure after myocardial infarction:clinical presentation and survival. Eur J Heart Fail2005;7:119–25.
13. Goldstein DJ, Maybaum S, MacGillivray TE,et al. Young patients with nonischemic cardiomy-opathy have higher likelihood of left ventricularrecovery during left ventricular assist device sup-port. J Card Fail 2012;18:392–5.
14. Mano A, Nakatani T, Oda N, et al. Which fac-tors predict the recovery of natural heart functionafter insertion of a left ventricular assist system?J Heart Lung Transplant 2008;27:869–74.
15. Drakos SG, Wever-Pinzon O, Selzman CH, et al.Magnitude and time course of changes induced bycontinuous-flow left ventricular assist deviceunloading in chronic heart failure: insights intocardiac recovery. J Am Coll Cardiol 2013;61:1985–94.
16. Lang RM, Badano LP, Mor-Avi V, et al. Rec-ommendations for cardiac chamber quantificationby echocardiography in adults: an update from theAmerican Society of Echocardiography and theEuropean Association of Cardiovascular Imaging.J Am Soc Echocardiogr 2015;28:1–39. e14.
17. Nagueh SF, Appleton CP, Gillebert TC, et al.Recommendations for the evaluation of left ven-tricular diastolic function by echocardiography.J Am Soc Echocardiogr 2009;22:107–33.
18. International Conference on Harmonisation E9Expert Working Group. ICH harmonised tripartiteguideline: statistical principles for clinical trials.Stat Med 1999;18:1905–42.
Wever-Pinzon et al. J A C C V O L . 6 8 , N O . 1 6 , 2 0 1 6
HF Etiology and LVAD-Induced Myocardial Recovery O C T O B E R 1 8 , 2 0 1 6 : 1 7 4 1 – 5 2
1752
19. Freemantle N. Interpreting the results of sec-ondary end points and subgroup analyses in clin-ical trials: should we lock the crazy aunt in theattic? BMJ 2001;322:989–91.
20. Mancini DM, Beniaminovitz A, Levin H, et al.Low incidence of myocardial recovery after leftventricular assist device implantation in patientswith chronic heart failure. Circulation 1998;98:2383–9.
21. Saito S, Toda K, Miyagawa S, et al. Hemody-namic changes during left ventricular assistdevice-off test correlate with the degree of car-diac fibrosis and predict the outcome after deviceexplantation. J Artif Organs 2015;18:27–34.
22. Komoda T, Komoda S, Dandel M, Weng Y,Hetzer R. Explantation of INCOR left ventricularassist device after myocardial recovery. J CardSurg 2008;23:642–7.
23. Simon MA, Kormos RL, Murali S, et al.Myocardial recovery using ventricular assistdevices: prevalence, clinical characteristics, andoutcomes. Circulation 2005;112 Suppl 9:I32–6.
24. Farrar DJ, HolmanWR, McBride LR, et al. Long-term follow-up of Thoratec ventricular assistdevice bridge-to-recovery patients successfullyremoved from support after recovery of ventricularfunction. J Heart Lung Transplant 2002;21:516–21.
25. Strueber M, Larbalestier R, Jansz P, et al. Re-sults of the post-market Registry to Evaluate theHeartWare Left Ventricular Assist System(ReVOLVE). J Heart Lung Transplant 2014;33:486–91.
26. Maybaum S, Mancini D, Xydas S, et al. Cardiacimprovement during mechanical circulatory sup-port: a prospective multicenter study of the LVADWorking Group. Circulation 2007;115:2497–505.
27. Drakos SG, Terrovitis JV, Anastasiou-Nana MI,Nanas JN. Reverse remodeling during long-termmechanical unloading of the left ventricle. J MolCell Cardiol 2007;43:231–42.
28. Dandel M, Weng Y, Siniawski H, Potapov E,Lehmkuhl HB, Hetzer R. Long-term results in pa-tients with idiopathic dilated cardiomyopathy afterweaning from left ventricular assist devices. Cir-culation 2005;112 Suppl 9:I37–45.
29. Lamarche Y, Kearns M, Josan K, et al. Suc-cessful weaning and explantation of the Heart-mate II left ventricular assist device. Can J Cardiol2011;27:358–62.
30. Khan T, Delgado RM, Radovancevic B, et al.Dobutamine stress echocardiography predictsmyocardial improvement in patients supported byleft ventricular assist devices (LVADs): hemody-namic and histologic evidence of improvementbefore LVAD explantation. J Heart Lung Trans-plant 2003;22:137–46.
31. Boehmer JP, Starling RC, Cooper LT, et al. Leftventricular assist device support and myocardialrecovery in recent onset cardiomyopathy. J CardFail 2012;18:755–61.
32. Liden H, Karason K, Bergh CH, Nilsson F,Koul B, Wiklund L. The feasibility of left ventric-ular mechanical support as a bridge to cardiacrecovery. Eur J Heart Fail 2007;9:525–30.
33. Drakos SG, Mehra M. Clinical myocardial re-covery during long-term mechanical support inadvanced heart failure: insights into moving thefield forward. J Heart Lung Transplant 2016;35:413–20.
34. Drakos SG, Kfoury AG, Hammond EH, et al.Impact of mechanical unloading on microvascula-ture and associated central remodeling features ofthe failing human heart. J Am Coll Cardiol 2010;56:382–91.
35. Heerdt PM, Schlame M, Jehle R, Barbone A,Burkhoff D, Blanck TJ. Disease-specific remodelingof cardiac mitochondria after a left ventricularassist device. Ann Thorac Surg 2002;73:1216–21.
36. Hall JL, Grindle S, Han X, et al. Genomicprofiling of the human heart before and aftermechanical support with a ventricular assist devicereveals alterations in vascular signaling networks.Physiol Genomics 2004;17:283–91.
37. Blaxall BC, Tschannen-Moran BM, Milano CA,Koch WJ. Differential gene expression andgenomic patient stratification following left ven-tricular assist device support. J Am Coll Cardiol2003;41:1096–106.
38. al-Mohammad A, Mahy IR, Norton MY, et al.Prevalence of hibernating myocardium in patients
with severely impaired ischaemic left ventricles.Heart 1998;80:559–64.
39. Auerbach MA, Schoder H, Hoh C, et al. Prev-alence of myocardial viability as detected bypositron emission tomography in patients withischemic cardiomyopathy. Circulation 1999;99:2921–6.
40. Schinkel AF, Bax JJ, Boersma E, Elhendy A,Roelandt JR, Poldermans D. How many patientswith ischemic cardiomyopathy exhibit viablemyocardium? Am J Cardiol 2001;88:561–4.
41. Fox KF, Cowie MR, Wood DA, et al. Coronaryartery disease as the cause of incident heart failurein the population. Eur Heart J 2001;22:228–36.
42. Schinkel AF, Bax JJ, Sozzi FB, et al. Prevalenceof myocardial viability assessed by single photonemission computed tomography in patients withchronic ischaemic left ventricular dysfunction.Heart 2002;88:125–30.
43. Madigan JD, Barbone A, Choudhri AF, et al.Time course of reverse remodeling of the leftventricle during support with a left ventricularassist device. J Thorac Cardiovasc Surg 2001;121:902–8.
44. Oriyanhan W, Tsuneyoshi H, Nishina T,Matsuoka S, Ikeda T, Komeda M. Determination ofoptimal duration of mechanical unloading forfailing hearts to achieve bridge to recovery in a ratheterotopic heart transplantation model. J HeartLung Transplant 2007;26:16–23.
45. Diakos NA, Selzman CH, Sachse FB, et al.Myocardial atrophy and chronic mechanicalunloading of the failing human heart: implica-tions for cardiac assist device-induced myocar-dial recovery. J Am Coll Cardiol 2014;64:1602–12.
KEY WORDS cardiac recovery, ischemiccardiomyopathy, left ventricular assistdevice, mechanical unloading, myocardialfunction, myocardial structure
APPENDIX For supplemental tables, pleasesee the online version of this article.