Embed Size (px)
Citation preview

MANAGEMENT OF HEART FAILURE (TE MEYER, SECTION EDITOR)
Impact of Intravenous Nitroglycerin in the Management of AcuteDecompensated Heart Failure
Corstiaan A. den Uil & Jasper J. Brugts
# Springer Science+Business Media New York 2014
Abstract Intravenous nitroglycerin is a well-known, but un-derused, treatment for acute decompensated heart failure.Nitroglycerin has a rapid onset of action and short half-lifeand there is a clear dose-response curve on both global hemo-dynamics and peripheral circulation. IV nitroglycerin reducesLVand RV filling pressures and afterload. In the case of acutedecompensated heart failure, there is a typical decreased bio-availability of nitric oxide (NO), which needs to be supple-mented by exogenous nitrates. Additionally, there is benefiton clinical endpoints, such as fast optimization of arterialoxygenation, lower rates of mechanical ventilation, and im-proved survival. Drawbacks of therapy include not only sideeffects such as headache, resistance, and development oftolerability to nitrates but also free radical production.However, nitrates in combination with diuretics remain thecornerstone of acute decompensated heart failure treatment.We propose a more aggressive use of nitrates and a morelimited use of inotropes (due to ischemic demand and pro-arrhythmogenic characteristics) in normo- or hypertensivepatients with acute heart failure.
Keywords Acute heart failure . Critical care . Emergencycare . Hemodynamics . Inodilators . Intensive care .
Microcirculation . Nitrates . Nitroglycerin . Perfusion .
Vasodilators
Introduction
Acute decompensated heart failure is characterized by failingcompensatory mechanisms utilized by the body in an attemptto restore the primary deficit in cardiac output. Patients oftenpresent with cold, mottled extremities, and signs and symp-toms of fluid overload. Nitroglycerin, among other nitratessuch as isosorbidemono- or dinitrate (ISMN or ISDN), is awell-known agent used for its vasodilatory properties in orderto lower cardiac filling pressures and to decrease systolicblood pressure. Intravenous nitroglycerin is often used in thetreatment of hospitalized patients with heart failure, but bothin Europe and in the USA, its use is inconsistent due to severalcontroversies [1•, 2, 3, 4•]. We will review its mode of action,when used intravenously, at the endothelial vascular and myo-cardial level. In addition, we will review the benefit of nitrateson hemodynamics and microcirculation in patients with acutedecompensated heart failure. The results of randomized clin-ical trials in this field will be presented. Finally, we willevaluate potential shortcomings of the therapy related tolong-term use.
Rationale of Nitroglycerin in Acute Heart Failure
In general, the beneficial hemodynamic effects of intravenousnitroglycerin in patients with decompensated heart failure arethe main reasons for its use in these patients. The hemody-namic effects include a substantial reduction in right and leftfilling pressures which is essential in the acute stage of treat-ment [5]. Furthermore, nitroglycerin lowers systemic andpulmonary vascular resistances as well as systemic bloodpressure. There is only a minor change in heart rate, whilecardiac output is likely to increase. The latter occurs byoptimization of the Frank-Starling mechanism as well as bya reduction in afterload for both ventricles.
This article is part of the Topical Collection on Management of HeartFailure
C. A. den Uil (*) : J. J. BrugtsDepartment of Cardiology, Erasmus Medical Center, Thoraxcenter,‘s-Gravendijkwal 230, 3015 CE Rotterdam, The Netherlandse-mail: [email protected]
Curr Heart Fail RepDOI 10.1007/s11897-014-0230-8

Additionally, heart failure results in neurohumoral adapta-tions that alter cellular, autocrine, and paracrine signalingsystems, and changes levels of vasoactive and inflammatorymediators, of which nitric oxide (NO) is of utmost importance.
NO is enzymatically formed from L-arginine by three iso-forms of nitric oxide synthetase (NOS): neuronal type (nNOS,NOS1), cytokine-inducible NOS (iNOS, NOS2), and theendothelial-type (eNOS, NOS3) [6]. NO induces vasorelax-ation in vascular smooth muscle through activation of solubleguanylate cyclase, which in turn increases intracellular con-centrations of cyclic guanosine monophosphate (cGMP).
There is strong evidence that experimental and clinicalheart failure is associated with arterial endothelial dysfunctionand impaired endothelium-dependent dilation. The mecha-nism is partly a diminished endothelial production of NO viaeNOS [7, 8], maybe caused by reduced gene expression ofeNOS [9]. In addition, endothelial release of NO is decreasedso that endothelium-dependent vasodilation by muscarinicstimulation was found to be impaired in patients with heartfailure [10, 11] and could be restored by low-dose nitroglyc-erin [12]. Finally, degradation of endothelial NO is enhancedin patients with heart failure, probably explained throughincreased free radicals that may inactivate endogenous NO[13].
There is less agreement on the changes in the expressionprofile and activity of NOS isoforms in the myocardium [14,15]. There appears to be increased levels of activity of eNOSand nNOS and increased NO production, whereas the expres-sion of iNOS was found to be correlated with the level oftumor necrosis factor alpha [16–18]. The net clinical effects ofincreased myocardial NO production in heart failure are yetunclear.
Mode of Action of Nitroglycerin
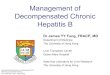
Current evidence suggests that glyceryl trinitrate (GTN, =ni-troglycerin) is biotransformated by complex, actually twodifferent intracellular pathways [19•]. When administered inlow concentrations in the laboratory setting (<1 μmol/L),nitric oxide (NO) is formed directly by interaction ofALDH2, or nitrite (NO2), as an intermediate, maybe reducedto NO by mitochondrial or cytoplasmatic oxidases (Fig. 1).The other nitrates (ISDN and ISMN) or nitroglycerin whenadministered at higher dosages are activated in the smoothendoplasmatic reticulum by P450 enzymes to form NO. NOactivates its intracellular receptor, soluble guanylyl cyclase,leading to increased concentrations of cGMP and activation ofcGMP-dependent protein kinases or cyclic nucleotide-gatedcalcium channels, resulting in decreased intracellular calciumconcentrations and relaxation of endothelial smooth musclecells and vasodilation. When given intravenously, nitroglyc-erin acts within minutes and has a short half-life of 2–4 min.
Nitrates are cleared by extraction through blood vessels, trans-formation in blood, and clearance by the liver [20].
Hemodynamic and Microcirculatory Effects
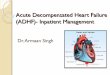
We previously demonstrated the beneficial effect of nitroglyc-erin on sublingual microcirculation as a surrogate for tissueperfusion in patients with acute heart failure [21]. In a recentstudy consisting of 17 patients with cardiogenic shock or(decompensated) end-stage heart failure, nitroglycerin dosedependently lowered cardiac filling pressures at a dosage of33 μg/min or higher (Fig. 2) [22]. Each infusion rate wasmaintained constant for 30 min. At higher dosages, meanarterial pressure decreased. These hemodynamic effects wereaccompanied by a modest increase in cardiac index.Interestingly, improvement of tissue perfusion (sublingualperfused capillary density and central-peripheral temperaturegradient) was observed at a lower dose of nitroglycerin(NTG), i.e., 17μg/min, than changes in global hemodynamics(Fig. 3) [22]. Changes in microcirculation were independentof cardiac index. These findings may contribute to futurestudies that should assess the value of microcirculation-directed therapy in patients with severe heart failure andcardiogenic shock [23, 24].
Fig. 1 Mechanisms of bioactivation of organic nitrates. Glyceryltrinitrate (=nitroglycerin) is metabolized by two different pathways.When administered in low concentrations (<1 μmol/L), nitric oxide(NO) is formed directly by interaction of ALDH2, or nitrite (NO2) maybe reduced to NO by oxidases in the mitochondrium or in the cytoplasm.The low-potency nitrates (ISDN and ISMN) or nitroglycerin when ad-ministered at higher dosages are activated in the smooth endoplasmaticreticulum by P450 enzymes to form NO. NO activates its intracellularreceptor, soluble guanylyl cyclase, leading to increased concentrations ofcGMP and activation of cGMP-dependent protein kinases or cyclicnucleotide-gated ion channels, resulting in relaxation of endothelialsmooth muscle cells and vasodilation. GTN glyceryl trinitrate (=nitro-glycerin), ALDH2 mitochondrial aldehyde dehydrogenase, NO2 nitrite,GDN glyceryl dinitrate, NO nitric oxide, sGC soluble guanylyl cyclase,cGMP cyclic guanosinemonophosphate, ISDN isosorbidedinitrate, ISMNisosorbidemononitrate
Curr Heart Fail Rep

Clinical Trials on Intravenous Nitrates in Acute Heart Failure
Hemodynamic Parameters Few randomized clinical trials in-vestigated the benefit of intravenous nitrates on hemodynamicparameters [25]. Characteristics and outcomes of these studiesare listed in Table 1.
Nelson et al. [26] and Verma et al. [27] used intravenousisosorbidedinitrate (ISDN) in complicated myocardial infarc-tion and found that filling pressures and mean arterial pressuredecreased to a greater extent in patients treated with ISDNcompared to those treated with furosemide.
Beltrame et al. [28] compared nitroglycerin (+free radicalscavenger) with morphine and furosemide in patients with acutepulmonary edema without myocardial infarction. Unfortunately,the patients were not equipped with a pulmonary artery catheter.No differenceswere observed in primary and secondary outcomemeasures consisting of ventilatory parameters.
Biomarkers Several small studies reported reductions in plas-ma natriuretic peptides, whereas neurohumoral markers such
as plasma aldosterone, cortisol, epinephrine, and plasma reninactivity may temporarily increase [29–31]. Chow et al. com-pared the effects of nesiritide compared with nitroglycerin in arandomized study of 89 patients with acute decompensatedheart failure [32]. They found similar hemodynamic effectsand significant reductions in NT-prohormone brain natriureticpeptide (proBNP) and BNP levels over time but not signifi-cantly different between both arms. Patients treated withnesiritide had lower nystatin C and IL-6 levels, but no differ-ence was observed for other inflammatory markers [33].
Clinical Endpoints There are some data on the clinical benefitof intravenous nitroglycerin. Aziz et al. performed a retrospec-tive study in 430 patients with acute decompensated heartfailure and chronic kidney disease, treated with neither di-uretics nor NTG, diuretics only, or both diuretics and NTG[34]. Patients treated with NTG had better survival at24 months compared to the other arms.
Cotter et al. performed a randomized trial in >100 patientswith acute decompensated heart failure who were randomizedbetween high-dose ISDN (+low-dose furosemide) and high-dose furosemide (+low-dose ISDN) [35]. Mechanical ventila-tion was less frequently required in patients treated with high-dose ISDN. In addition, myocardial infarction occurred lessfrequently in the high-dose ISDN group.
The same research group compared high-dose ISDN withstandard dose nitrate therapy and noninvasive ventilation (bi-level positive airway ventilation, BiPAP) in patients withsevere pulmonary edema, and this study was prematurelyterminated because of it significantly having more benefit inpatients treated with high-dose nitrate [36]. Eighty percent ofBiPAP-treated patients required intubation and mechanicalventilation compared to 20 % in the high-dose ISDN group(p<0.001). Myocardial infarction occurred more frequently inthe BiPAP group. The combined end point (death, mechanicalventilation, or MI) was observed in 17 (85 %) BiPAP-treatedpatients vs. in 5 (25 %) high-dose ISDN-treated patients(p<0.001). Arterial oxygen saturation increased more rapidlyin the high-dose ISDN group.
Fig. 2 Changes in global hemodynamic parameters in patients with increasing dosages of intravenous nitroglycerin. Data (mean±SD) found in 17patients with cardiogenic shock or end-stage heart failure [22]. **p<0.01, ***p<0.001
Fig. 3 Changes in microcirculation (sublingual perfused capillary den-sity) in patients with severe decompensated heart failure receiving in-creasing dosages of intravenous nitroglycerin. Data (mean±SD) found in17 patients with cardiogenic shock or end-stage heart failure [22].***p<0.001
Curr Heart Fail Rep

The Vasodilation in the Management of Acute CHF(VMAC) trial [37] compared the recombinant B-type natri-uretic peptide nesiritide (n=204) with either nitroglycerin (n=143) or placebo (n=142) in patients with decompensatedcongestive heart failure. Although the reduction in PCWPwas slightly greater in patients treated with nesiritide than innitroglycerin-treated patients, this did not translate into betterimprovement of self-reported symptoms in the nesiritide-treated group. A severe shortcoming of this trial included thatthe dose of nitroglycerin (median 13 μg/min) was actually toolow to improve global hemodynamic parameters, as wasdemonstrated by the almost complete lack of benefit on he-modynamic parameters of nitroglycerin-treated patients incomparison with the placebo arm (Table 1).
The Acute Decompensated Heart Failure National Registry(ADHERE) suggested a benefit of vasodilator therapy vs.positive inotropic therapy on reducing inhospital mortality inpatients hospitalized with acute decompensated heart failure[38] This was confirmed by the propensity score-matched datafrom the ADHERE database analysis that demonstrated thatpatients with acute decompensated heart failure treated withinotropes (dobutamine, dopamine, or milrinone) had highermortality than patients treated with diuretics +/− vasodilators(nitroglycerin or nesiritide) [39].
Potential Shortcomings and Hazards of Long-TermUse of Nitroglycerin
Side Effects Adverse effects of nitroglycerin during the first24 h after the start of therapy have been described in theVMAC study [37]. The most frequently reported side effectsare headache, nausea, and hypotension.
Nitrate Resistance and Tolerance An attenuated vasodilatoryresponse to intravenous nitroglycerin (independently of priornitrate use) has been reported in patients with heart failure, asdemonstrated by Katz et al., who found a higher femoral arteryblood flow velocity induced by nitroglycerin in normal subjectsas compared to patients with heart failure [40]. This reducedeffectiveness could be overcome by increasing the dosage.Multiple factors, such as activation of vasoconstrive mecha-nisms, may be involved in nitrate resistance in patients with heartfailure [41].
The hemodynamic and clinical effects of nitroglycerinwane upon continuous (>several hours) therapy. Elkayamet al. already reported in the year 1987 that tolerance tointravenous infusion of nitroglycerin in patients with coronaryheart disease or heart failure may develop within 24 h [42].The mechanism of nitrate tolerance is still not clear. Severalhypotheses were proposed, including pseudotolerance (i.e.,activation of neurohumoral systems [30]) or true vascularT
able1
Randomized
controlledtrialson
thehemodynam
iceffectsof
intravenousnitratetherapyin
acutedecompensated
heartfailure
Trial(year)
Populatio
nInterventio
n(I/C)
Sample
size
Nitrate
dosage
Follo
w-up
ΔPA
OP
(mmHgvs.
baselin
e)
ΔMAP
(mmHgvs.
baselin
e)
ΔCI(L/m
in/
m2vs.
baselin
e)
ΔPA
OP
(mmHgvs.
control)
ΔMAP
(mmHgvs.
control)
ΔCI(L/m
in/
m2vs.
control)
Nelson(1983)
[26]
AMI+
ADHF
ISDNvs.furosem
ide
14/14
50–200
μg/kg/h
90min
Meandifference
−8(p<0.01)
Meandifference
−9(p<0.01)
NS
Meandifference
−4(p<0.01)
Meandifference
−7(p<0.01)
NS
Verma(1987)
[27]
AMI+
ADHF
ISDNvs.furosem
ide
(vs.hydralazine
vs.prenalterol)
12/12(/12/12)
50–200
μg/kg/h
90min
Meandifference
−6(p<0.01)
Meandifference
−7(p<0.01)
NS
Meandifference
−2(sign?)
Meandifference
−3(sign?)
NS
Beltram
e(1998)
[28]
ADHF
Nitroglycerin/N-
acetylcysteine
vs.furosem
ide/
morphine
37/32
2.5–10
μg/min
24h
NA
Meansystolic
BP−2
8NA
NA
NS
NA
Cotter(1998)
[35]
ADHF
High-dose
ISDN
vs.high-dose
furosemide
52/52
Mean11.4mg
UntilSaO2≥9
6%
orMAP<90
mmHg
NA
Mean−2
5NA
NA
NS
NA
Sharon
(2000)
[36]
ADHF
High-dose
ISDN
vs.low
-dose
ISDN
+BiPAP
20/20
Mean10.8mg
UntilSaO2>96
%or
systolicBP
<110mmHg
(50min)
NA
Mean−2
2NA
NA
NS
NA
VMAC(2002)
[37]
ADHF
Nitroglycerinvs.
Placebo
(vs.nesiritide)
143/142
(/204)
Median13
μg/
min
3h
Mean−4
Meansystolic
BP−6
Mean+0.2
NS
Meansystolic
BP−2
(p<0.05)
NS
AMIacutemyocardialinfarctio
n,ADHFacutedecompensated
heartfailu
re,CAD
coronary
artery
disease,ISDNisosorbidedinitrate,BiPAPbi-level
positiv
eairw
aypressure,PA
OPpulm
onaryartery
occlusionpressure,M
APmeanarterialpressure,B
Pbloodpressure,C
Icardiacindex,
NAnotavailable,NSnotsignificant
Curr Heart Fail Rep

tolerance by impaired GTN biotransformation, increased vas-cular superoxide production, or desensitization of solubleguanylate cyclase [19]. Nitrate tolerance may be accompaniedby nitrated-induced impairment of endogenous NO produc-tion (maybe induced by oxidative stress) [43]. However, thesepotential unfavorable effects of longer-term nitrate treatmentmight be offset by co-treatment with ACE inhibitors [44],hydralazine [45–48], carvedilol [49], or atorvastatin [50].
Future Perspectives
Other vasodilators like nesiritide [37, 51, 52] andlevosimendan [53] have not proved definite benefit in thesetting of acute decompensated heart failure. Furthermore,nitrates share a clearer dose-response curve and shorter half-life in comparison to phosphodiesterase inhibitors. Therefore,intravenous nitrates remain, together with diuretic therapy, thecornerstone of modern urgent acute heart failure treatment.Therapies using novel vasodilators such as serelaxin are cur-rently tested [54] and should ideally be compared to mean-ingful dosages of intravenous nitrate therapy in adequatelypowered randomized controlled trials.
Conclusions
Nitroglycerin has clear benefits on hemodynamics and tissuemicrocirculation, as well as on clinical endpoints. Togetherwith diuretics, nitrates remain the cornerstones of acute de-compensated heart failure treatment. We propose unlimiteduse, at least at short term, in normo- or hypertensive patientswith acute heart failure.
Compliance with Ethics Guidelines
Conflict of Interest Corstiaan A. den Uil and Jasper J. Brugts declarethat they have no conflict of interest.
Human and Animal Rights and Informed Consent This article doesnot contain any studies with human or animal subjects performed by anyof the authors.
References
Papers of particular interest, published recently, have beenhighlighted as:• Of importance
1.• Singer AJ, Skopicki H, Thode HC, Peacock WK. Hemodynamicprofiles of ED patients with acute decompensated heart failure and
their association with treatment. Am J Emerg Med. 2014;32:302–5.This study is an example of the fact that less than 50 % of patientswith acute decompensated heart failure is currently treated withvasodilators.
2. Collins SP, Pang PS, Lindsell CJ, Kyriacou DN, Storrow AB, et al.International variations in the clinical, diagnostic, and treatmentcharacteristics of emergency department patients with acute heartfailure syndromes. Eur J Heart Fail. 2010;12:1253–60.
3. Mentz RJ, Cotter G, Cleland JG, Stevens SR, Chiswell K, et al.International differences in clinical characteristics, management,and outcomes in acute heart failure patients: better short-termoutcomes in patients enrolled in Eastern Europe and Russia in thePROTECT trial. Eur J Heart Fail. 2014;16:614–24.
4.• Tarvasmäki T, Harjola VP, Tolonen J, Siirilä-Waris K, NieminenMS, et al. Management of acute heart failure and the effect ofsystolic blood pressure on the use of intravenous therapies. EurHeart J Acute Cardiovasc Care. 2013;2:219–25. This study is anexample of the fact that less than 50 % of patients with acutedecompensated heart failure is currently treated with vasodilators.
5. Elkayam U, Janmohamed M, Habib M, Hatamizadeh P.Vasodilators in the management of acute heart failure. Crit CareMed. 2008;36:S95–105.
6. Forstermann U, Closs EI, Pollock JS, Nakane M, Schwarz P, et al.Nitric oxide synthase isozymes. Characterization, purification, mo-lecular cloning, and functions. Hypertension. 1994;23:1121–31.
7. Katz SD, Khan T, Zeballos GA, Matthew L, Potharlanka P, et al.Decreased activity of the L-arginine-nitric oxide metabolic pathwayin patients with congestive heart failure. Circulation. 1999;99:2113–7.
8. Mohri M, Egashira K, Tagawa T, Kuga T, Tagawa H, et al. Basalrelease of nitric oxide is decreased in the coronary circulation inpatients with heart failure. Hypertension. 1997;1(Pt 1):50–6.
9. Smith CJ, Sun D, Hoegler C, Roth BS, Zhang X, et al. Reducedgene expression of vascular endothelial NO synthase andcyclooxygenase-1 in heart failure. Circ Res. 1996;78:58–64.
10. Kubo SH, Rector TS, Bank AJ, Williams RE, Heifetz SM.Endothelium-dependent vasodilation is attenuated in patients withheart failure. Circulation. 1991;84:1589–96.
11. Katz SD, Krum H, Khan T, Knecht M. Exercise-induced vasodila-tion in forearm circulation of normal subjects and patients withcongestive heart failure: role of endothelium-derived nitric oxide.J Am Coll Cardiol. 1996;28:585–90.
12. Schwarz M, Katz SD, Demopoulos L, Hirsch H, Yuen JL, et al.Enhancement of endothelium-dependent vasodilation by low-dosenitroglycerin in patients with congestive heart failure. Circulation.1994;89:1609–14.
13. Hornig B, Arakawa N, Kohler C, Drexler H. Vitamin C improvesendothelial function of conduit arteries in patients with chronicheart failure. Circulation. 1998;97:363.
14. Barouch LA, Harrison RW, SkafMW, Rosas GO, Cappola TP, et al.Nitric oxide regulates the heart by spatial confinement of nitricoxide synthase isoforms. Nature. 2002;416:337–9.
15. Simon JN, Duglan D, Casadei B, Carnicer R. Nitric oxide synthaseregulation of cardiac excitation-contraction coupling in health anddisease. J Mol Cel Cardiol. 2014;73C:80–91.
16. Stein B, Eschenhagen T, Rudiger J, Scholz H, Forstermann U, et al.Increased expression of constitutive nitric oxide synthase III, butnot inducible nitric oxide synthase II, in human heart failure. J AmColl Cardiol. 1998;32:1179–86.
17. Damy T, Ratajczak P, Shah AM, Camors E, Marty I, et al. Increasedneuronal nitric oxide synthase-derived NO production in the failinghuman heart. Lancet. 2004;363:1365–7.
18. Comini L, Bachetti T, Agnoletti L, Gaia G, Curello S, et al.Induction of functional inducible nitric oxide synthase in mono-cytes of patients with congestive heart failure. Link with tumournecrosis factor-alpha. Eur Heart J. 1999;20:1503–13.
Curr Heart Fail Rep

19.• Munzel T, Daiber A, Gori T. Good review article on the currentevidence for mode of action of nitrates and the development oftolerance. Circulation. 2011;123:2132–44. Good review article onthe current evidence for mode of action of nitrates and the devel-opment of tolerance.
20. Fung HL. Pharmacokinetic determinants of nitrate action. Am JMed. 1984;76:22–6.
21. Den Uil CA, LagrandWK, Spronk PE, van der Ent M, Jewbali LS,et al. Low-dose nitroglycerin improved microcirculation in hospi-talized patients with acute heart failure. Eur J Heart Fail. 2009;11:386–90.
22. Den Uil CA, Caliskan K, LagrandWK, Van der Ent M, Jewbali LS,et al. Dose-dependent benefit of nitroglycerin on microcirculationof patients with severe heart failure. Intensive Care Med. 2009;35:1893–9.
23. Den Uil CA, LagrandWK, Van der Ent M, Jewbali LS, Cheng JM,et al. Impaired microcirculation predicts poor outcome of patientswith acute myocardial infarction complicated by cardiogenic shock.Eur Heart J. 2010;31:3032–9.
24. Den Uil CA, Lagrand WK, Valk SD, Spronk PE, Simoons ML.Management of cardiogenic shock: focus on tissue perfusion. CurrProbl Cardiol. 2009;34:330–49.
25. Wakai A, McCabe A, Kidney R, Brooks SC, Seupaul RA, et al.Nitrates for acute heart failure syndromes. Cochrane Database SystRev. 2013;8, CD005151.
26. Nelson GI, Silke B, Ahuja RC, Hussain M, Taylor SH.Haemodynamic advantages of isosorbide dinitrate over furosemidein acute heart failure following myocardial infarction. Lancet.1983;1:730–3.
27. Verma SP, Silke B, Hussain M, Nelson GI, Reynolds GW, et al. First-line treatment of left ventricular failure complicating acute myocardialinfarction: a randomised evaluation of immediate effects of diuretic,venodilator, arteriodilator, and positive inotropic drugs on left ventric-ular function. J Cardiovasc Pharmacol. 1987;10:38–46.
28. Beltrame JE, Zeitz CJ, Unger SA, Brennan RJ, Hunt A, et al. Nitratetherapy is an alternative to furosemide/morphine therapy in themanagement of acute cardiogenic pulmonary edema. J Card Fail.1998;4:271–9.
29. Webster MW, Sharpe DN, Coxon R, et al. Effect of reducing atrialpressure on atrial natriuretic factor and vasoactive hormones incongestive heart failure secondary to ischemic and nonischemicdilated cardiomyopathy. Am J Cardiol. 1989;63:217–21.
30. Dupuis J, Lalonde G, Lemieux R, et al. Tolerance to intra-venous NTG in patients with congestive heart failure: role ofincreased intravascular volume, neurohumoral activation andlack of prevention with N-acetylcysteine. J Am Coll Cardiol.1990;16:923–31.
31. Dakak N, Makhoul N, Merdler A, et al. Haemodynamic and neu-rohumoral effects of flosequinan in severe heart failure: Similaritiesand differences compared with intravenous NTG therapy. Eur HeartJ. 1993;14:836–44.
32. Chow SL, O'Barr SA, Peng J, Chew E, Pak F, et al. Renal functionand neurohormonal changes following intravenous infusions ofnitroglycerin versus nesiritide in patients with acute decompensatedheart failure. J Card Fail. 2011;17:181–7.
33. Chow SL, O'Barr SA, Peng J, Chew E, Pak F, et al. Modulation ofnovel cardiorenal and inflammatory biomarkers by intravenousnitroglycerin and nesiritide in acute decompensated heart failure.Circ Heart Fail. 2011;4:450–5.
34. Aziz EF, Kukin M, Javed F, Pratap B, Sabharwal MS, et al.Effect of adding nitroglycerin to early diuretic therapy onthe morbidity and mortality of patients with chronic kidneydisease presenting with acute decompensated heart failure.Hosp Pract. 1995;39:126–32.
35. Cotter G, Metzkort E, Kaluski E, Faigenberg Z, Miller R, et al.Randomised trial of high-dose isosorbide dinitrate plus low-dose
furosemide versus high-dose furosemide plus low-dose isosorbidedinitrate in severe pulmonary oedema. Lancet. 1998;351:389–93.
36. Sharon A, Shpirer I, Kaluski E, Moshkovitz Y, MilovanovO, et al. High-dose intravenous isosorbide-dinitrate is saferand better than Bi-PAP ventilation combined with conven-tional treatment for severe pulmonary edema. J Am CollCardiol. 2000;36:832–7.
37. VMAC. Intravenous nesiritide vs nitroglycerin for treatment ofdecompensated congestive heart failure: a randomized controlledtrial. JAMA. 2002;287:1531–40.
38. Abraham WT, Adams KF, Fonarow GC, Costanzo MR, BerkowitzRL, et al. In-hospital mortality in patients with acute decompensat-ed heart failure requiring intravenous vasoactive medications. J AmColl Cardiol. 2005;46:57–64.
39. Costanzo MR, Johannes RS, Pine M, Gupta V, Saltzberg M, et al.The safety of intravenous diuretics alone versus diuretics plusparenteral vasoactive therapies in hospitalized patients with acutelydecompensated heart failure: a propensity score and instrumentalvariable analysis using the Acutely Decompensated Heart FailureNational Registry (ADHERE) database. Am Heart J. 2007;154:262–77.
40. Katz SD, Biasucci L, Sabba C, et al. Impaired endothelium medi-ated vasodilation in the peripheral vasculature of patients withcongestive heart failure. J Am Coll Cardiol. 1992;19:918–25.
41. Elkayam U, Mehra A, Shotan A. Nitrate resistance and tolerance:potential limitations in the treatment of congestive heart failure. AmJ Cardiol. 1992;70:98B–104.
42. Elkayam U, Kulick D, McInthosh N, Roth A, Hsueh W, et al.Incidence of early tolerance to hemodynamic effects of continuousinfusion of nitroglycerin in patients with coronary artery diseaseand heart failure. Circulation. 1987;76:577–84.
43. Gori T, Mak SS, Kelly S, Parker JD. Evidence supporting abnor-malities in nitric oxide synthase function induced by nitroglycerinin humans. J Am Coll Cardiol. 2001;38:1096–101.
44. Mehra A, Ostrzega E, Shotan A, Johnson JV, ElkayamU. Persistenthemodynamic improvement with short-term nitrate therapy in pa-tients with chronic congestive heart failure already treated withcaptopril. Am J Cardiol. 1992;70:1310–4.
45. Daiber A, Oelze M, Coldewey M, Kaiser K, Huth C, et al.Hydralazine is a powerful inhibitor of peroxynitrite formation as apossible explanation for its beneficial effects on prognosis in pa-tients with congestive heart failure. Biochem Biophys ResCommun. 2005;338:1865–74.
46. Muunzel T, Kurz S, Rajagopalan S, Thoenes M, Berrington WR,et al. Hydralazine prevents nitroglycerin tolerance by inhibitingactivation of a membrane-bound NADH oxidase: a new action foran old drug. J Clin Invest. 1996;98:1465–70.
47. Cohn JN. Effect of vasodilator therapy on mortality in chroniccongestive heart failure. Eur Heart J. 1988;9:171–3.
48. Cohn JN, Tam SW, Anand IS, Taylor SH, Sabolinski ML, et al.Isosorbide dinitrate and hydralazine in a fixed-dose combinationproduces further regression of left ventricular remodeling in a well-treated black population with heart failure: results from A-HeFT. JCard Fail. 2007;13:331–9.
49. Watanabe H, Kakihana M, Ohtsuka S, Sugishita Y.Preventive effects of carvedilol on nitrate tolerance: a ran-domized, double-blind, placebo-controlled comparative studybetween carvedilol and arotinolol. J Am Coll Cardiol.1998;32:1201–6.
50. Liuni A, Luca M, Uxa A, Mariani J, Gori T, et al. Coadministrationof atorvastatin prevents nitroglycerin-induced endothelial dysfunc-tion and nitrate tolerance in humans in vivo. J Am Coll Cardiol.2011;3:93–8.
51. O'Connor CM, Starling RC, Hernandez AF, Armstrong PW,Dickstein K, et al. Effect of nesiritide in patients with acute decom-pensated heart failure. N Engl J Med. 2011;365:32–43.
Curr Heart Fail Rep

52. Chen HH, AnstromKJ, GivertzMM, Stevenson LW, SemigranMJ,et al. Low-dose dopamine or low-dose nesiritide in acute heartfailure with renal dysfunction: the ROSE acute heart failure ran-domized trial. JAMA. 2013;310:2533–43.
53. Unverzagt S, Wachsmuth L, Hirsch K, Thiele H, Buerke M, et al.Inotropic agents and vasodilator strategies for acute myocardial
infarction complicated by cardiogenic shock or low cardiac outputsyndrome. Cochrane Database Syst Rev. 2014;1, CD009669.
54. Filippatos G, Teerlink JR, Farmakis D, Cotter G, Davison BA, et al.Serelaxin in acute heart failure patients with preserved left ventric-ular ejection fraction: results from the RELAX-AHF trial. Eur HeartJ. 2014;35:1041–50.
Curr Heart Fail Rep