Embed Size (px)
Citation preview

e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 1 3 3 – 1 4 2
avai lab le at www.sciencedi rect .com
journa l homepage: www.europeanurology.com
Kidney Cancer
Impact of Gender in Renal Cell Carcinoma: An Analysisof the SEER Database
Monish Aron, Mike M. Nguyen, Robert J. Stein, Inderbir S. Gill *
Section of Laparoscopic and Robotic Surgery, Glickman Urological Institute, Cleveland Clinic Foundation, Cleveland, OH, USA
Article info
Article history:Accepted December 3, 2007Published online ahead ofprint on December 17, 2007
Keywords:GenderRenal cell carcinomaSurvivalSEER
Abstract
Objective: To evaluate gender differences in initial presentation, pathol-ogy, and outcomes with renal cell carcinoma (RCC).Materials and methods: The 1973–2004 Surveillance Epidemiology andEnd Results (SEER) 17-registries database was analyzed for renal tumorsfrom 1988 to 2004 coded as primary site ‘‘kidney and renal pelvis.’’ Aftervarious exclusions, a final study group of 35,336 cases with completedata was obtained. Demographic variables analyzed included age, sex,and race. Tumor variables included size, stage at diagnosis, grade, andhistology. Primary outcome variables included overall and cancer-specific survival.Results: Of the patients, 22,288 were male (63%). Females presented withsmaller tumors (5.9 vs. 6.1 cm, p < 0.0001) of lower grade ( p < 0.0001).Males had a higher incidence of regional or metastatic spread of renalcarcinoma ( p < 0.0001). Median overall survival from time of diagnosiswas 130 mo for females versus 110 mo for males ( p < 0.0001).In comparisons of males and females, 5-yr cancer-specific survivalwas 78% versus 81%, and 5-yr overall survival was 65% versus 69%( p < 0.0001). On multivariate analysis, cancer-specific survival was simi-lar (HR, 1.00, p = 0.960), whereas overall survival was significantly longerfor females (HR, 0.92, p < 0.0001). Older age at diagnosis, larger tumorsize, higher grade, higher SEER historic stage, and sarcomatoid, collect-ing duct, or ‘‘other’’ histology were related to worse cancer-specific andoverall survival.
present with larger, higher stage, higher grade RCCerall survival is better in women, whereas cancer-
Conclusions: Menthan women. Ov
is not significantly different.ociation of Urology. Published by Elsevier B.V. All rights reserved.
specific survival# 2007 European Ass
* Corresponding author. Glickman Urological Institute/A100, 9500 Euclid Ave,Cleveland Clinic Foundation, Cleveland, OH 44195, United States. Tel. +1 216 445 1530;Fax: +1 216 445 7031.E-mail address: [email protected] (I.S. Gill).
0302-2838/$ – see back matter # 2007 European Association of Urology. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.eururo.2007.12.001

e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 1 3 3 – 1 4 2134
1. Introduction
Renal cancer is expected to be the seventh leadingcause of cancer in men and the ninth leadingcause of cancer in women in the United States in2007, accounting for about 4% of all cancers inAmerican men and 3% of all cancers in Americanwomen, with a male: female ratio of about 1.6 [1].An estimated 51,190 new cases of renal cancerare expected in the United States in 2007, with12,890 deaths [1]. Renal cell carcinoma (RCC)accounts for 85% of all renal cancers. Approxi-mately a third of all patients with RCC initiallypresent with large, locally advanced, or metastaticdisease.
The incidence of renal cancer has increasedannually by 2.3% among white men, 3.1% amongwhite women, 3.9% among black men, and 4.3%among black women between 1975 and 1995 [2].Such an upward trend in incidence rate has beennoted in 17 of 20 countries across four continents(Sweden, Denmark, and Switzerland being excep-tions) between 1973 and 1992 [3]. The greatestincrease in incidence is noted for localized tumors,which has in part been attributed to a significantincrease in the use of cross-sectional abdominalimaging for the evaluation of unrelated abdominalsymptoms [2]. Detection of incidental renal tumorsincreased from 13% in 1982 to 59% in 1997, andapproximately 48–66% of all renal tumors todayare small, localized, and incidentally detected[4,5].
Currently RCC most commonly presents as asmall incidentally detected renal mass. Presenceor absence of symptoms as well as stage andgrade have been shown to be independentprognostic factors [6–9]. Incidental tumors aresmaller, with lower stage and lower grade, anda lower incidence of nodal and distant meta-stases [7]. The mode of detection is an inde-pendent prognostic variable in patients with RCC[7–9].
Overall, RCC is almost twice as common inmen than in women, and men account for nearlytwo thirds of deaths from RCC. Differencesin presentation, demographics, and pathologicalparameters have been reported from single seriesbetween men and women treated with kidneymasses [10,11]. However, to our knowledge, acomprehensive population-based evaluation ofthe differences among genders with regard topresentation, pathology, and outcomes of RCC hasnot been performed. Herein we report these resultsfrom an analysis of the comprehensive SEERdatabase.
2. Materials and methods
2.1. Patients and tumor characteristics
The latest 1973–2004 SEER 17 Registries database released in
April 2007 was analyzed for renal tumors from 1988 to 2004
coded as primary site ‘‘kidney and renal pelvis.’’ The SEER
program is administered by the National Cancer Institute. It
captures incident cancer cases from 17 population-based
cancer registries distributed across the United States. These
registries collectively cover approximately 26% of the US
population. Of 108,017 cases coded as primary site ‘‘kidney and
renal pelvis,’’ we excluded 14,678 transitional cell and other
nonrenal carcinomas on the basis of histology data (upper
tract transitional cell cancers [n = 12,436], Wilms’ tumors
[n = 1939], oncocytomas [n = 135], leiomyosarcomas [n = 121],
neuroblastomas [n = 34], rhabdomyosarcomas [n = 9], and
angiomyolipomas [n = 4]). Cases were selected from 1988
onward to maintain consistency of staging data because of
availability of ‘‘SEER Historic Stage A’’ for all cases following
1988. This process excluded 19,240 cases. Another 10,182
patients with missing size information were excluded.
Patients coded as ‘‘in situ’’ or ‘‘no tumor found’’ (n = 31) or
size greater than 40 cm (n = 77) were also excluded. Further-
more, cases with unknown age (n = 1) or with age at diagnosis
younger than 20 yr (n = 141) were excluded to focus on
nonpediatric tumors. Cases without stage data were also
removed (n = 234). We finally excluded 35,581 cases without
grade data, resulting in a final study group of 35,336 cases.
2.2. Variables assessed
Patient demographic variables analyzed included age, sex,
and race. Tumor variables included size, stage at diagnosis,
grade, and histology. Histology was based on the International
Classification of Diseases for Oncology, Third Edition (ICD-O-3)
system. Primary outcome variables included overall and
cancer-specific survival. Stage data were obtained from the
SEER historic stage A variable, which codes stage as ‘‘in situ,’’
‘‘localized,’’ ‘‘regional,’’ and ‘‘distant’’ for kidney tumors.
Descriptions of these stages are available on the SEER
website (http://seer.cancer.gov/manuals/CD2.SEERDic.pdf).
While SEER has now begun including TNM staging, this
information is available for only cases diagnosed in 2004 and
afterward.
2.3. Statistics
Summary statistics were constructed with means for con-
tinuous variables and percentages for categorical variables.
Chi-square tests were used for analysis of dichotomous
variables and t tests for continuous variables. Simple linear
and logistic regression was used for univariate analysis of
continuous and dichotomous dependent variables, respec-
tively. Overall survival and cancer-specific survival were
calculated for median survival and 5-yr survival. Survival
was compared between subgroups by log-rank testing. Median
follow-up in months was determined for both the entire
cohort and for censored patients only.

e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 1 3 3 – 1 4 2 135
Cox proportional hazards models were developed to
evaluate the effect of gender on overall and cancer-specific
survival. We incorporated additional independent variables
(age, race, tumor size, histology, tumor grade, tumor stage)
into a multivariate model to allow adjustment of their effects
on survival. Analysis was performed with the use of the
STATA 8 statistical software package (Stata Corp, College
Station, TX, USA). Statistical significance was set at 0.05 and all
tests were two-tailed.
3. Results
3.1. Demographic findings
Of 35,336 patients analyzed, 22,288 (63.1%) weremale. Compared with males, females presentedwith smaller tumors (5.9 cm vs. 6.1 cm, p < 0.0001)and with lower pathological grade ( p < 0.0001). Malepatients had a higher incidence of regional ormetastatic spread of renal carcinoma ( p < 0.0001).Females had a greater incidence of clear-cell(88.4% vs. 85.3%) and decreased incidence of papil-lary (3.0% vs. 5.6%) histology ( p < 0.0001). Table 1details the gender differences in demographicinformation for renal carcinoma patients.
Table 1 – Demographics according to gender for renal cell carc
Male SD/%
No. 22,288 63.1%
Age (yr) 61.7 12.5
Tumor size (cm) 6.1 3.8
Tumor grade
1 3763 16.9%
2 11,160 50.1%
3 5840 26.2%
4 1525 6.8%
Race
White 18,869 84.7%
Black 2002 9.0%
American Indian/Alaskan native 193 0.9%
Asian/Pacific Islander 1112 5.0%
Other 31 0.1%
Unknown 81 0.4%
SEER historic stage A
Localized 14,707 66.0%
Regional 5027 22.6%
Metastatic 2554 11.5%
Histology
Clear cell 19,016 85.3%
Papillary 1257 5.6%
Granular 618 2.8%
Chromophobe 438 2.0%
Sarcomatoid 217 1.0%
Collecting duct 46 0.2%
Other 696 3.1%
SD, standard deviation.
3.2. Clinicopathological features and survival according to
gender
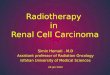
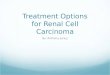
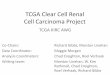
According to the primary outcome variable, medianfollow-up for the entire cohort was 29 mo (range,0–203), whereas median follow-up for censoredpatients was 34 mo (range, 0–203). The mediancancer-specific survival was not reached for eithermales or females. The median overall survival fromtime of diagnosis was 130 mo for females (range,1–203) versus 110 mo (range, 1–203) for malepatients. Kaplan-Meier survival curves accordingto gender are plotted in Figs. 1 and 2. Cancer-specificand overall survival rates were superior for females(log-rank test for equivalency of survival, p < 0.0001).Five-year cancer-specific survival was 78.2% formales and 81% for females, whereas 5-yr overallsurvival was 64.7% for males and 69% for females.
Univariate Cox proportional hazards modelingdemonstrated superior cancer-specific (HR, 0.85;p < 0.0001) and overall (HR, 0.86; p < 0.0001) survivalfor female gender compared with male gender.However, on multivariate analysis, cancer-specificsurvival was not significantly different betweenfemales and males (HR, 1.00; p = 0.960), whereas
inoma patients
Female SD/% p Test
13,048 36.9% —
62.4 13.5 <0.0001 t test
5.9 3.6 <0.0001 t test
<0.0001 x2
2995 23.0%
6365 48.8%
2872 22.0%
816 6.3%
0.687 x2
11,068 84.8%
1165 8.9%
131 1.0%
624 4.8%
19 0.2%
41 0.3%
<0.0001 x2
9358 71.7%
2403 18.4%
1287 9.9%
<0.0001 x2
11,536 88.4%
394 3.0%
322 2.5%
273 2.1%
103 0.8%
24 0.2%
396 3.0%

Fig. 1 – Kaplan-Meier cancer specific survival after diagnosis of renal carcinoma. Mean survival time for female patients was
significantly prolonged compared with male patients ( p < 0.0001). Numbers at risk listed below graph.
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 1 3 3 – 1 4 2136
overall survival remained significantly longer(HR, 0.92; p < 0.0001) for female patients (Tables 2and 3). Therefore female gender alone is not anindependent prognostic factor for renal tumors.Multivariate analysis additionally demonstrated
Fig. 2 – Kaplan-Meier overall survival after diagnosis of renal ca
significantly prolonged compared with male patients ( p < 0.000
that higher age at diagnosis, larger tumor size,higher histopathological grade, higher SEER historicstage, and sarcomatoid, collecting duct, or otherhistology were related to worse cancer-specific andoverall survival. Asian Pacific Islander or ‘‘unknown’’
rcinoma. Mean survival time for female patients was
1). Numbers at risk listed below graph.

Table 2 – Multivariate Cox proportional hazards model of cancer-specific survival
Variable HR 95% confidence interval p
Age at diagnosis (yr) 1.02 1.01 1.02 <0.0001
Tumor size (cm) 1.06 1.06 1.07 <0.0001
Gender
Male — — — —
Female 1.00 0.95 1.06 0.960
Grade
Grade 1 — — — —
Grade 2 1.37 1.24 1.52 <0.0001
Grade 3 2.46 2.22 2.73 <0.0001
Grade 4 3.40 3.03 3.83 <0.0001
Race
Caucasian race — — — —
African American race 1.07 0.97 1.18 0.198
American Indian/Alaskan Native 1.13 0.88 1.45 0.327
Asian Pacific Islander 0.86 0.77 0.97 0.015
Other 0.54 0.18 1.69 0.291
Unknown 0.22 0.07 0.68 0.009
SEER historic stage
Localized — — — —
Regional 3.78 3.51 4.07 <0.0001
Distant 16.65 15.42 17.97 <0.0001
Histology
Clear cell/conventional — — — —
Papillary 0.66 0.53 0.83 <0.0001
Granular 1.04 0.90 1.20 0.618
Chromophobe 0.39 0.27 0.58 <0.0001
Sarcomatoid 1.40 1.19 1.66 <0.0001
Collecting duct 2.23 1.40 3.54 0.001
Other 1.94 1.74 2.15 <0.0001
HR, hazard ratio; SEER, Surveillance Epidemiology and End Results.
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 1 3 3 – 1 4 2 137
race and papillary or chromophobe histology werepredictive of improved cancer-specific and overallsurvival. African American race predicted shorteroverall survival (p < 0.0001) compared with Cauca-sian race, but cancer-specific survival was notsignificantly different (p = 0.198).
4. Discussion
In our analysis of 35,336 patients from the SEERdatabase with RCC, men comprised 63%, for a male:female ratio of 1.7:1. This ratio is commensuratewith several prior reports, suggesting that RCC isnearly twice as common in men as in women.Females presented with smaller tumors and withlower grade. Men had a higher incidence of regionalor metastatic spread of renal carcinoma. A potentialexplanation for women presenting with smallertumors and at an earlier stage than men could bethat women are more likely than men to haveincidental detection of tumors during imaging forabdominal or pelvic pathology [11]. The reasons for
women presenting with lower grade lesions is notknown. Interestingly, women had a higher inci-dence of clear-cell histology, which is associatedwith worse prognosis and raises the question of whywomen overall have a more favorable outcome. Thereason is not clear but may be associated with lowergrade and smaller size of the tumors at presentationdespite the histological subtype. In a recent study,Lane et al [12] estimated the predicted probability ofbenign disease for nonsmoking men and womenwith an incidentally detected 3-cm small renalmass. A younger woman was more likely to havebenign disease than a similarly aged man, whereasan older man was more likely to have benign diseasethan a similarly aged woman.
Median overall survival from time of diagnosiswas 130 mo for females versus 110 mo for malepatients. Prolonged cancer-specific and overallsurvival rates for females were observed. Five-yearcancer-specific survival was 78% for males and81% for females, whereas 5-yr overall survival was65% for males and 69% for females. On multivariateanalysis, however, cancer-specific survival was not

Table 3 – Multivariate Cox proportional hazards model of overall survival
Variable HR 95% confidence interval p
Age at diagnosis (yr) 1.03 1.03 1.04 <0.0001
Tumor size (cm) 1.04 1.04 1.05 <0.0001
Gender
Male — — — —
Female 0.92 0.88 0.96 <0.0001
Grade
Grade 1 — — — —
Grade 2 1.06 1.00 1.13 0.044
Grade 3 1.59 1.49 1.70 <0.0001
Grade 4 2.28 2.10 2.47 <0.0001
Race
Caucasian race — — — —
African American race 1.29 1.20 1.38 <0.0001
American Indian/Alaskan Native 1.09 0.90 1.32 0.399
Asian Pacific Islander 0.85 0.77 0.93 0.001
Other 0.58 0.24 1.40 0.228
Unknown 0.27 0.13 0.58 0.001
SEER historic stage
Localized — — — —
Regional 1.92 1.83 2.02 <0.0001
Distant 7.69 7.28 8.12 <0.0001
Histology
Clear cell/conventional — — — —
Papillary 0.83 0.72 0.95 0.008
Granular 0.99 0.89 1.11 0.916
Chromophobe 0.60 0.47 0.76 <0.0001
Sarcomatoid 1.55 1.33 1.81 <0.0001
Collecting duct 1.95 1.28 2.97 0.002
Other 1.92 1.77 2.08 <0.0001
HR, hazard ratio; SEER, Surveillance Epidemiology and End Results.
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 1 3 3 – 1 4 2138
significantly different between females and males,whereas overall survival was significantly longer forfemale patients. Equivalency of cancer-specificsurvival is likely explained by correction for differ-ences in grade and stage with multivariate analysis.Overall survival being longer in women is likely afunction of superior longevity among women in thegeneral population.
Multivariate analysis also demonstrated thatgreater age at diagnosis, larger tumor size, higherhistopathological grade, higher SEER historic stage,and sarcomatoid, collecting duct, or other histologywere related to worse cancer-specific and overallsurvival. Although this finding is intuitive for tumorsize, stage, grade, and aggressive histologies, it is notimmediately apparent why advanced age shouldadversely affect cancer-specific survival.
Asian Pacific Islander or unknown race andpapillary or chromophobe histology were predictiveof improved cancer-specific and overall survival.African American race predicted shorter overallsurvival compared with Caucasian race, but cancer-specific survival was not significantly different. This
finding could be attributed to poorer access tomedical care among African American patients.
In epidemiological studies of RCC, the associa-tions between gender and RCC have not been wellexamined. In a population-based case-control studyinvolving 422 women with RCC, and an equalnumber of sex-, age-, and race-matched controlsin Los Angeles, California, women who had under-gone hysterectomy were at higher risk for RCC (oddsratio, 1.8; 95% confidence interval, 1.3–2.5). Parityand hormone replacement therapy were not riskfactors when adjusted for hysterectomy. No asso-ciation between RCC and use of oral contraceptiveswas found. The authors do not support an endocrineexplanation for the observed hysterectomy-RCCassociation. Instead they hypothesized that unin-tentional injury to the ureter during hysterectomyresults in renal cell damage and consequent renalcell proliferation, which may be a cause of theincreased risk of RCC after hysterectomy [13].
In another case-control study from Iowa from1986 to 1989, 261 men and 145 women with RCC werecompared with 1598 men and 831 women controls.

e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 1 3 3 – 1 4 2 139
In age-adjusted analysis, there was a decrease inRCC risk for women who reported consuming morethan three servings of alcohol per week (odds ratio,0.5; 95% confidence interval, 0.2–0.9) comparedwith never drinkers. No evidence of an associationamong men was noted (odds ratio, 1.1; 95%confidence interval, 0.8–1.5). Multivariate adjust-ment for anthropometric, lifestyle, smoking, anddietary factors did not alter the findings [14].
Another study looked at gender differences inRCC on the basis of exposure to organic solvents in asample of 438 RCC cases (273 men and 165 women)and 687 controls (462 men and 225 women). Overall,34% of men and 21% of women with RCC wereexposed to organic solvents. The risk of RCC wassignificantly higher among women exposed to allorganic solvents (odds ratio, 2.3; 95% CI, 1.3–4.2).Among men, no significant excess risk was observedwith exposure to all organic solvents combined. Onthe basis of small numbers, the authors conjecturedthat these differences could be explained by chance,or by the differences in body fat content, metabolicactivity, the rate of elimination from the body, or bydifferences in the level of exposure between menand women [15].
In a retrospective study [16] from Japan encom-passing nearly 40 yr (1957–1995), of 768 RCC patients,all of whom underwent nephrectomy, 662 wereclassified as clear-cell carcinoma, 43 as papillaryRCC, 36 as chromophobe RCC, and 27 as cyst-associated RCC. Of those with clear-cell carcinoma,women had a better prognosis than men ( p = 0.012).No other subtype of RCC was associated with asignificant difference in survival between thegenders. There were a smaller proportion of patientswith stage IV and a larger proportion with stage Idisease in women ( p < 0.05). Of stage I patients,women had a better prognosis than men ( p < 0.011).Women also had better survival after tumor recur-rence than men ( p = 0.007).
In a Norwegian retrospective study of 368 RCCpatients treated with nephrectomy over a span of22 yr, 29% had incidentally detected tumors. Inci-dental tumors were smaller (6 vs. 7 cm, p < 0.0001),of lower stage ( p = 0.02), and had better 5-yr cancer-specific survival (81% vs. 62%, p = 0.0048) comparedwith symptomatic tumors. The frequency of womenwas significantly higher in the incidental tumorgroup compared with the symptomatic tumorgroup, with male: female ratio being nearly 1 forincidental and 1.7 for symptomatic tumors( p = 0.02). Women had more low-stage (I–II) tumors( p = 0.02) and superior cancer-specific survival( p = 0.05), which may be explained by better femalesurvival among symptomatic patients and the
higher proportion of women with incidental tumors.There was no difference in tumor size between thesexes. Multivariate analysis revealed tumor stage asthe only significant independent prognostic factor.Data on pathological subtype and grade were notprovided [11].
In a recent single-center study focused on genderdifferences in presentation and pathology, 1015patients treated with nephrectomy over a span of15 yr were studied [10]. Men accounted for 66% ofpatients. There were no differences in age and racedistribution among the sexes. Size of primary tumorwas similar for men and women. Men were morelikely to have bilateral tumors (9.4% vs. 3.5%,p = 0.009) and malignant histology (91% vs. 83%,p = 0.001) than women. The rate of malignancy forwomen increased from 44.5% for tumors < 1 cm to93% for tumors >10 cm, whereas no differences inmalignant histology rates were seen in men bytumor size. Univariate analysis revealed male sex,tumor size, stage, and grade as significant predictorsof malignancy. For patients with a pathologicaldiagnosis of RCC, men had less clear-cell histology(70.5% vs. 77.2%), more papillary tumors (17.4% vs.4.5%), and fewer chromophobe tumors (5% vs. 11%)compared with women. There was no significantdifference in overall survival, disease-specific sur-vival, and disease-free survival on the basis of sexin univariate Kaplan-Meier analysis. Multivariateanalyses revealed male sex, tumor size, grade, andchief complaint were predictive of overall survival,whereas tumor size, grade, stage and chief complaintwere predictive of cancer-specific survival [10].
Contrary to these findings, in our study, womenpresented at an older age (62.4 vs. 61.7 yr, p < 0.0001)and with smaller tumors (5.9 cm vs. 6.1 cm,p < 0.0001). Grade I–II lesions accounted for 72%and 67% of tumors in women and men, respectively( p < 0.0001). Localized disease was seen in 72% and66% of women and men, respectively ( p < 0.0001).Similar to the above study, clear-cell histology wasmore common (88.4% vs. 85.3%) and papillaryhistology was less common (3% vs. 5.6%) in women.Contrary to the study by Pierorazio et al [10], wefound superior overall survival in women, althoughcancer-specific survival was similar.
Limitations of our study include its retrospectivenature, relatively short follow-up, and the lack ofdata in the SEER database pertaining to comorbid-ities, which could explain the gender differences inoverall survival. Information about gender differ-ences with regard to potential risk factors, symp-toms, and incidental detection rates is also notavailable. Such information may be potentiallyuseful in explaining observed differences in size

e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 1 3 3 – 1 4 2140
and stage at presentation. Lastly, the underlyingmechanism behind the differences we observed ingrade and histologic subtype between the genderscannot be further explained with the use of this typeof data set, which represent an additional limitation.
5. Conclusions
Population-based data from the SEER RCC databasesuggest that women present at a slightly olderage than men with tumors that are smaller, lowerstage, and lower grade. Although overall survival issuperior in women, the cancer-specific survivalwhen adjusted for stage and grade is similar to men.
Gender differences in RCC biology and epidemiol-ogy are incompletely understood. Further researchis indicated to define the fundamental basis of theseobserved differences.
Conflicts of interest
Inderbir S. Gill is a consultant and stockholder forHansen Medical, Mountain View, CA, USA.
Source of funding: None.
References
[1] Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. Cancer
statistics, 2007. CA Cancer J Clin 2007;57:43–66.
[2] Chow WH, Devesa SS, Warren JL, Fraumeni Jr JF. Rising
incidence of renal cell cancer in the united states. JAMA
1999;281:1628–31.
[3] Mathew A, Devesa SS, Fraumeni Jr JF, Chow WH. Global
increases in kidney cancer incidence, 1973–1992. Eur J
Cancer Prev 2002;11:171–8.
[4] Luciani LG, Cestari R, Tallarigo C. Incidental renal cell
carcinoma-age and stage characterization and clinical
Editorial Comment on: Impact of Gender inRenal Cell Carcinoma: An Analysis of theSEER DatabaseMasaru MuraiDepartment of Urology, Keio University School ofMedicine, International Goodwill Hospital,Tokyo, [email protected]
The incidence of renal cell carcinoma (RCC)has been increasing worldwide. Men have twicethe incidence of developing RCC as women. Aronet al. elucidated the differences between the
implications: study of 1092 patients (1982–1997). Urology
2000;56:58–62.
[5] Volpe A, Panzarella T, Rendon RA, Haider MA, Kondylis FI,
Jewett MA. The natural history of incidentally detected
small renal masses. Cancer 2004;100:738–45.
[6] Patard J-J, Leray E, Rodriguez A, Rioux-Leclercq N, Guille F,
Lobel B. Correlation between symptom graduation, tumor
characteristics and survival in renal cell carcinoma. Eur
Urol 2003;44:226–32.
[7] Bretheau D, Lechevallier E, Eghazarian C, Grisoni V, Cou-
lange C. Prognostic significance of incidental renal cell
carcinoma. Eur Urol 1995;27:319–23.
[8] Ficarra V, Prayer-Galetti T, Novella G, et al. Incidental
detection beyond pathological factors as prognostic
predictor of renal cell carcinoma. Eur Urol 2003;43:
663–9.
[9] Lam JS, Shvarts O, Pantuck AJ. Changing concepts in the
surgical management of renal cell carcinoma. Eur Urol
2004;45:692–705.
[10] Pierorazio PM, Murphy AM, Benson MC, McKiernan JM.
Gender discrepancies in the diagnosis of renal cortical
tumors. World J Urol 2007;25:81–5.
[11] Beisland C, Medby PC, Beisland HO. Renal cell carcinoma:
gender difference in incidental detection and cancer-spe-
cific survival. Scand J Urol Nephrol 2002;36:414–8.
[12] Lane BR, Babineau D, Kattan MW, et al. A preoperative
prognostic nomogram for solid enhancing renal tumors
7 cm or less amenable to partial nephrectomy. J Urol
2007;178:429–34.
[13] Gago-Dominguez M, Castelao JE, Yuan JM, Ross RK, Yu
MC. Increased risk of renal cell carcinoma subsequent
to hysterectomy. Cancer Epidemiol Biomarkers Prev
1999;8:999–1003.
[14] Parker AS, Cerhan JR, Lynch CF, Ershow AG, Cantor KP.
Gender, alcohol consumption, and renal cell carcinoma.
Am J Epidemiol 2002;155:455–62.
[15] Dosemeci M, Cocco P, Chow WH. Gender differences in
risk of renal cell carcinoma and occupational exposures
to chlorinated aliphatic hydrocarbons. Am J Ind Med
1999;36:54–9.
[16] Onishi T, Oishi Y, Goto H, Yanada S, Abe K. Gender as a
prognostic factor in patients with renal cell carcinoma.
BJU Int 2002;90:32–6.
genders in terms of cancer progression. Men tendto present with a larger size tumor, a higher stageand a higher grade RCC than women. In contrast,women tend to demonstrate smaller and lowergrade tumors. Men also have a higher incidenceof regional or metastatic spread [1]. There are fewreports of a male survival advantage [2]. Thesedifferences suggest that the hormonal status, i.e.estrogen has an impact on the course of cancer.
The clinical use of anti-angiogenesis agents forthe treatment of metastatic RCC suggest that RCCgrowth is supported by endothelial cells. Macro-phages or fibroblasts might also support the cancer

growth or metastatic spread. In these processes,growth factors including vascular endothelialfactor (VEGF) or inflammatory cytokines includinginterleukin-6, -8 might play a role. Adipocytokinesmay also play a role because obesity is one of theclassic risk factors along with smoking and hyper-tension. Gender differences are prominent in someadipocytokines [3]. Furthermore, recent reportsdescribe that leptin, an adipocytokine, is relatedto invasiveness and the progression of RCC [4].
A recent report has shown the IL-6 production tohave a gender disparity in a chemically inducedanimal model of liver cancer [5]. The hormonalenvironment may link the cytokines or growthfactors related to cancer progression. In themicroenviroment where renal cancer cells prolif-erate, these cancer cells may be supported byendothelial cells, macrophages, fibroblasts andadipocytes via growth factors, inflammatory cyto-kines or adipocytokines. To elucidate the under-lying mechanism of gender differences in RCC,further investigations of the microenviromentmaintained by the cytokines are thus called for.
References
[1] Aron M, Nguyen MM, Stein RJ, Gill IS. Impact of gender in
renal cell carcinoma: an analysis of the SEER database.
Eur Urol 2008;54:133–42.
[2] Micheli A, Mariotto A, Giorgi RA, et al. The prognostic
role of gender in survival of adult cancer patients.
Eur J Cancer 1998;34:2271–8.
[3] Bottner A, Kratzsch J, Muller G, et al. Gender differences
of adiponectin levels develop during the progression of
puberty and are related to serum androgen levels. J Clin
Endocrinol Metab 2007;89:4053–61.
[4] Horiguchi A, Sumitomo M, Asakuma J, et al. Increased
serum leptin levels and over expression of leptin recep-
tors are associated with the invasion and progression of
renal cell carcinoma. J Urol 2006;176:1631–5.
[5] Naugler WE, Sakurai T, Kim S, et al. Gender disparity in
liver cancer due to sex differences in MyD88-dependent
IL-6 production. Science 2007;317:121–4.
DOI: 10.1016/j.eururo.2007.12.002
DOI of original article: 10.1016/j.eururo.2007.12.001
Editorial Comment on: Impact of Gender inRenal Cell Carcinoma: An Analysis of theSEER DatabaseJean-Jacques PatardDepartment of Urology, Rennes University Hospital,Rennes, [email protected]
This paper provides interesting informationbecause it deals with an issue that has been poorlyexplored so far. However, when we read carefullythe results that are presented here by Aron et al, itis obvious that important biologic issues could behidden just behind clinical and pathologic findings[1]. Data presented in this manuscript have beenextracted from the National Cancer Institute Sur-veillance, Epidemiology and End Results Program(SEER) database and >35,000 records have beenexamined. The authors demonstrate that menpresented with larger, higher stage, higher graderenal tumors than women. Interestingly, althoughgender was clearly associated with better survival inunivariate analysis, it was not retained as anindependent prognostic variable when other majorclinical or pathologic renal cell carcinoma prognos-tic variables were introduced into the model.
In our multi-institutional database including>10,000 observations from 24 academic centers wefound basically the same trends. Female genderwas associated with lower T stage, lower Fuhrmangrades, and less propensity for tumors to exhibitperinephritic fat invasion (19.4% vs 23.2%) or topresent with distant metastases (13.3% vs. 16.6%,p = 0.0001). In our series, tumor size, N stage, andadrenal, renal vein, or inferior vena cava invasionrates did not appear to be significantly differentaccording to the male-to-female ratio. However,similar to the results reported by Aron et al, femalegender was associated with a more favorableoutcome than male gender for either overallsurvival (median not reached vs. 210 mo,p = 0.0001) or cancer-specific survival (160 vs. 130mo, p = 0.0001). Again, gender was not retained asan independent prognostic variable for the entirecohort. The biologic enigma behind these data isthat we also found that women were more likely tohave tumors with clear-cell histologic subtype (86%vs. 83.8%, p = 0.0001) and were more likely topresent with symptoms at diagnosis (46.4% vs.43.3%, p = 0.0001) or with poor performance status(Eastern Cooperative Oncology Group �1; 33.1% vs30.0%, p = 0.0001). These data together should
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 1 3 3 – 1 4 2 141

prompt us to further study the role of gender indifferent age categories [2] to indirectly assess theinfluence of hormonal status on tumor aggressive-ness. Finally, from a basic research viewpoint, geneexpression profiling comparing tumors accordingto age and sex categories should be encouraged [3].
References
[1] Aron M, Nguyen MM, Stein RI, Gill IS. Impact of gender in
renal cell carcinoma: an analysis of the SEER database.
Eur Urol 2008;54:133–42.
[2] Verhoest G, Veillard D, Guille F, et al. Relationship
between age at diagnosis and clinicopathologic features
of renal cell carcinoma. Eur Urol 2007;51:1298–305.
[3] Furge KA, Tan MH, Dykema K, et al. Identification of
deregulated oncogenic pathways in renal cell carci-
noma: an integrated oncogenomic approach based on
gene expression profiling. Oncogene 2007;26:1346–50.
DOI: 10.1016/j.eururo.2007.12.003
DOI of original article: 10.1016/j.eururo.2007.12.001
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 1 3 3 – 1 4 2142