Embed Size (px)
Citation preview
C
12
34
A
stccOcbiigp©
K
1d
Critical Reviews in Oncology/Hematology 62 (2007) 84–91
Impact of breast cancer survivorship on quality of life in older women
Claire Robb a,∗, William E. Haley b, Lodovico Balducci c, Martine Extermann c,Elizabeth A. Perkins b, Brent J. Small b, James Mortimer d
a Department of Health Administration, Biostatistics and Epidemiology, College of Public Health,University of Georgia, Athens, GA 30602-7396, United States
b School of Aging Studies, University of South Florida, Tampa, FL, United Statesc H. Lee Moffitt Cancer Center and Research Center, Tampa, FL, United States
d Department of Epidemiology, College of Public Health, University of South Florida, Tampa, FL, United States
Accepted 10 November 2006
ontents
. Introduction. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 84
. Patients and methods . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 852.1. Study design and study sample . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 852.2. Measures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 852.3. Statistics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 86
. Results . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 86
. Discussion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 88Reviewers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 89Acknowledgement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 90References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 90Biographies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 90
bstract
Quality of life (QOL) is an important outcome for cancer survivors; but although age is a major risk factor, most breast cancer survivorshiptudies are conducted with younger women. The objective of our study was to compare QOL in a sample of older breast cancer survivorso a sample of older women who were never diagnosed with breast cancer. A sample of 127 older breast cancer survivors as identified by aancer registry was compared to a demographically equated sample of 87 older women participating in an epidemiological study. Both groupsompleted a questionnaire and participated in an interview to measure QOL. The older breast cancer survivors scored worse in the Medicalutcomes Study-Short Form, a measure of health-related QOL. Survivors reported no more depressive symptoms or anxious mood than the
omparison group, but scored lower in measures of positive psychosocial well-being, including life satisfaction, mastery, and spiritual well-eing, and reported more depressed mood and days affected by fatigue. Older breast cancer survivors show multiple indications of decrementsn their health-related quality of life, and lower psychosocial well-being than the comparison group. These decrements may represent deficits
n reserve capacity that predispose older cancer survivors to functional disability but may not be readily detected in typical clinical evaluationsiven the multiple impairments common in geriatric populations. Results suggest a need for greater attention to promoting functioning andsychological well-being among older cancer survivors, even when they may not have obvious cancer-related medical complications.2006 Elsevier Ireland Ltd. All rights reserved.
eywords: Elderly; Breast cancer; Survivor; Quality of life; Physical functioning
∗ Corresponding author. Tel.: +1 706 425 3222; fax: +1 706 425 3221.E-mail address: [email protected] (C. Robb).
1
a
040-8428/$ – see front matter © 2006 Elsevier Ireland Ltd. All rights reserved.oi:10.1016/j.critrevonc.2006.11.003
. Introduction
Breast cancer is a common and serious disease in women;nd, other than being a woman, age is the greatest risk factor.

Oncol
Iiaicbqpoa
mmgcpcocdiwOeic
tas[aphArfet[
iciaqQwtaistesr
tttfdidccWpqt
2
2
Ioawgt6wodepg
ipiiqvwgtt
2
lbic
C. Robb et al. / Critical Reviews in
n more recent years, breast cancer incidence rates havencreased only in women age 50 and older, and a womant age 70 is almost twice as likely to develop breast cancern the next year as a woman age 50 [1]. Survival rates haveontinued to increase, but most survivorship studies haveeen conducted in younger women [2,3]. At the same time,uality of life (QOL), a multidimensional concept encom-assing behavioral competence and health, perceived qualityf existence, and psychological well-being [4], has becomen important outcome measure for cancer patients [5].
While younger cancer survivors have been found to attainaximum physical and psychological functioning approxi-ately 1 year after primary treatment [6], or at a minimum,
ood emotional functioning [7], there are reasons to be con-erned that older adult cancer survivors may face additionalroblems that complicate their recovery from cancer. Olderancer survivors have been shown to have a higher prevalencef chronic diseases than younger survivors [8], and theseomorbid conditions can exacerbate the stress of a canceriagnosis [9]. Functional status may be dramatically alteredn older women, and reserve capacity may be diminishedith functional dependence increasing with advancing age.lder patients’ psychosocial disabilities are also often under-
stimated or unrecognized by physicians, and may play anmportant role in the quality of life experience by older breastancer survivors [3].
Older breast cancer survivors are a particularly impor-ant group to study in terms of survivorship, since olderge has been found to exacerbate the effects of more exten-ive surgery on symptoms that produce limitations in activity10]. Also, adjuvant treatment such as radiation, chemother-py and hormonal therapy represent substantial physical andsychosocial challenges [3,11,12]. Such physical impairmentas been shown to affect both mental health and quality of life.ge is thought to strongly influence the shaping of a woman’s
esponse to breast cancer. For example, the older women con-ronted with a diagnosis of breast cancer may have differentxpectations as to treatment [13], and may react differentlyo the threat to life, since they may also be facing other losses14].
The combination of age as a risk factor for breast cancer,ncreased survivorship, and limited research with older breastancer survivors prompted our research. We were interestedn assessing the impact of breast cancer survivorship abovend beyond the effects of aging on QOL. We addressed thisuestion by comparing QOL in older cancer survivors withOL in a demographically similar sample of older womenho had never been diagnosed with breast cancer. In addi-
ion to conventional measures of health-rated QOL, we alsossessed important dimensions of well-being for older adultsncluding depressive symptoms, life satisfaction, mastery,pirituality, fatigue, and social support. We hypothesized that
he survivors as a group would report lower levels of QOL, asxemplified by poorer health-related QOL, more depressiveymptoms, lower mastery and life satisfaction, lower self-ated health, and more functional disability, compared withtmtc
ogy/Hematology 62 (2007) 84–91 85
he noncancer comparison population. Although some inves-igations have suggested that cancer survivorship is relatedo spiritual and psychological growth [15,16], we have notound studies of this issue in older adults. However, we pre-icted that this same positive association would be foundn older breast cancer survivors as well. We did not have airectional prediction on levels of social support. While can-er survivorship may heighten the need for social support,hronic illness may also deplete available social support [17].e also predicted that less invasive treatment and a longer
eriod of cancer survivorship would be associated with betteruality of life among cancer survivors, as women have moreime to recover from the trauma of cancer and its treatment.
. Patients and methods
.1. Study design and study sample
We used the H. Lee Moffitt Cancer Center and Researchnstitute cancer registry to identify 274 women age 70 andlder who had been diagnosed with breast cancer and hadt least 1 year survivorship. Of these women, 6 had died, 64ere unable to be contacted, and 77 refused to participate,iving us a final sample of 127 survivors, and a participa-ion rate of those survivors who were actually contacted of2%. Our comparison group was taken from a group of 119omen enrolled in a longitudinal follow-up of an epidemi-logical study on healthy aging. This core sample has beenescribed in other reports [18]. In this group, 24 women werexcluded because they were under age 70 and 8 women hadrior diagnosis of breast cancer, leaving a final comparisonroup of 87.
Upon agreement to participate and prior to an in-homenterview, survivors were sent a questionnaire packet to com-lete. The participants were advised to contact research stafff they encountered any difficulties in responding to questionsn the questionnaire packet. Within 2 weeks of receipt of theuestionnaire, research staff conducted semi-structured inter-iews at the participant’s home. All interviews of survivorsere conducted during April–August 2003. The comparisonroup completed questionnaires at home and were adminis-ered semi-structured interviews at a business site as part ofhe epidemiological study during February and March 2003.
.2. Measures
Demographic information, such as age, household incomeevel, ethnicity, and years of education was obtained fromoth the sample and the comparison group during thenterviews. To investigate comorbidity, 12 common chroniconditions were chosen. These conditions (e.g. osteoarthri-
is, heart disease, diabetes, etc.) were derived from a largeredical history questionnaire that had included acute condi-ions and childhood diseases previously administered to theontrol group [18]. Participants were asked to respond with

8 Oncol
yagtat
hta
tmcFahsmoiprdbbatmn(saetwtdcf
sGsdoylrstoqPeh
osidt
cwaisaawnwsiFWftbwwssdaqo
2
rmdtttqa
3
vMsB
6 C. Robb et al. / Critical Reviews in
es/no as to whether they had received a formal diagnosis bymedical doctor of each particular condition. The survivor
roup was also asked what types of primary cancer treatmenthey had received (i.e. mastectomy, lumpectomy, radiation,nd/or chemotherapy), and whether or not they were takingamoxifen.
The following standardized physical health, psychologicalealth and psychosocial measures used for both groups inhis study are well validated and have been widely used inssessing older populations.
Several variables assessing aspects of physical health sta-us including health-related QOL, and functioning, were
easured in this study. Health-related QOL was specifi-ally measured using the Medical Outcomes Study-Shortorm (SF-36). This is a 36-item instrument that is briefnd has been widely validated as a summary measure ofealth-related QOL [19]. In addition to an overall score, sub-cores for the two major dimensions of physical health andental health can be attained, as well as scores for each
f eight subscales. These subscales are physical function-ng, role-physical, bodily pain and general health under thehysical health dimension, and vitality, social functioning,ole-emotional and mental health under the mental healthimension. Each subscale is scored from 0 to 100 with 100eing the most favorable score (e.g. higher scores indicateetter functioning for physical, social, emotional, emotionalnd general health and less pain and limitations for the limita-ion subscales). Scores are expressed in a standardized t-score
etric, i.e. mean = 50, standard deviation ± 10. Physical vul-erability was assessed using the Vulnerable Elderly SurveyVES-13), a 13-item, function-based scoring system that con-iders age, self-rated health, limitation in physical functionnd functional disabilities, and which has been shown toffectively and efficiently identify older people at risk of func-ional decline and death over the next 2 years [20]. Fatigueas measured using the Multidimensional Fatigue Symp-
om Inventory-Short Form (MFSI-SF), a 13-item instrumenteveloped to assess the varied domains associated withancer-regulated fatigue. This measure has been validatedor use with heterogeneous samples of cancer patients [21].
Psychological health was investigated using three mea-ures. First, depressive symptoms were measured by theeriatric Depression Scale/Short Form (GDS-SF), a brief
elf-report specifically designed to measure expression ofepressive symptomatology in older adults and standardizedn older samples. The short form of this scale (15-item,es/no format) has been found to correlate highly with theong form and to have similar sensitivity and specificityates in identifying depressive disorders [22–24]. Second,tate anxiety was measured by the State-Trait Anxiety Inven-ory, which differentiates between the temporary conditionf “state anxiety” and the more general and long-standing
uality of “trait anxiety” and is a subscale of the State-Traitersonality Inventory (STPI) [25]. The essential qualitiesvaluated by the STAIS-Anxiety scale are feelings of appre-ension, tension, nervousness, and worry. The final measurehoys
ogy/Hematology 62 (2007) 84–91
f psychological functioning used was the State-Trait Depres-ion Inventory, which is also a subscale of the STPI. Thisnstrument was used to measure state depression that isepressive symptoms experienced “at the moment” versushose experienced generally [26].
In addition to demographic, physical health, and psy-hological health variables, several psychosocial variablesere also investigated. The individual’s perception of morale
nd general life satisfaction was assessed with the Life Sat-sfaction Index-Z (LSI-Z), a 13-item short form of a lifeatisfaction scale using the individual’s own evaluations aspoint of reference, rather than being dependent on level of
ctivity or social participation [22,27]. The sense of mastery,hich has been widely accepted as an asset in coping withegative life events (in this sense, a psychosocial resource),as measured by the seven-item Mastery Scale, a brief mea-
ure of with excellent psychometric characteristics [28]. Thendividual’s level of spiritual well-being was measured by theunctional Assessment of Chronic Illness Therapy-Spiritualell-Being (FACIT-Sp) scale. We utilized the total score
or spiritual well-being, and this measure has been foundo be a psychometrically sound measure of spiritual well-eing for patients with cancer and appropriate for individualsithout cancer [29]. Finally, a composite measure from theork of Krause and Borawski-Clark [30], was used to assess
ocial support as a functional aspect of social resources. Thecale used for this study examined received support in theimensions of instrumental support, informational supportnd emotional support, and respondents were asked specificuestions dealing with their access to these three dimensionsf social support and satisfaction with this support.
.3. Statistics
Initially, bivariate correlations were used to ascertain anyelationship between length of survivorship, types of treat-ent and health-related quality of life, life satisfaction and
epression. This helped us determine if it were reasonableo pool subjects across variation in survivorship and type ofreatment. Comparison of group means through use of mul-iple t-tests was used to determine significant differences inuality of life between survivors and comparison group. Anlpha level of .05 was used for all statistical tests.
. Results
Means for age and education of the breast cancer sur-ivors and the comparison group are presented in Table 1.ean age of the survivors was 78.23 years. There was no
ignificant difference between groups in age or education.oth samples were approximately 96% white and had median
ousehold incomes in the $30,000–49,999 range. Durationf survivorship ranged from 1 to 15 years and averaged 5.1ears. Frequencies of treatment regimens reported by theurvivors are also presented in Table 1.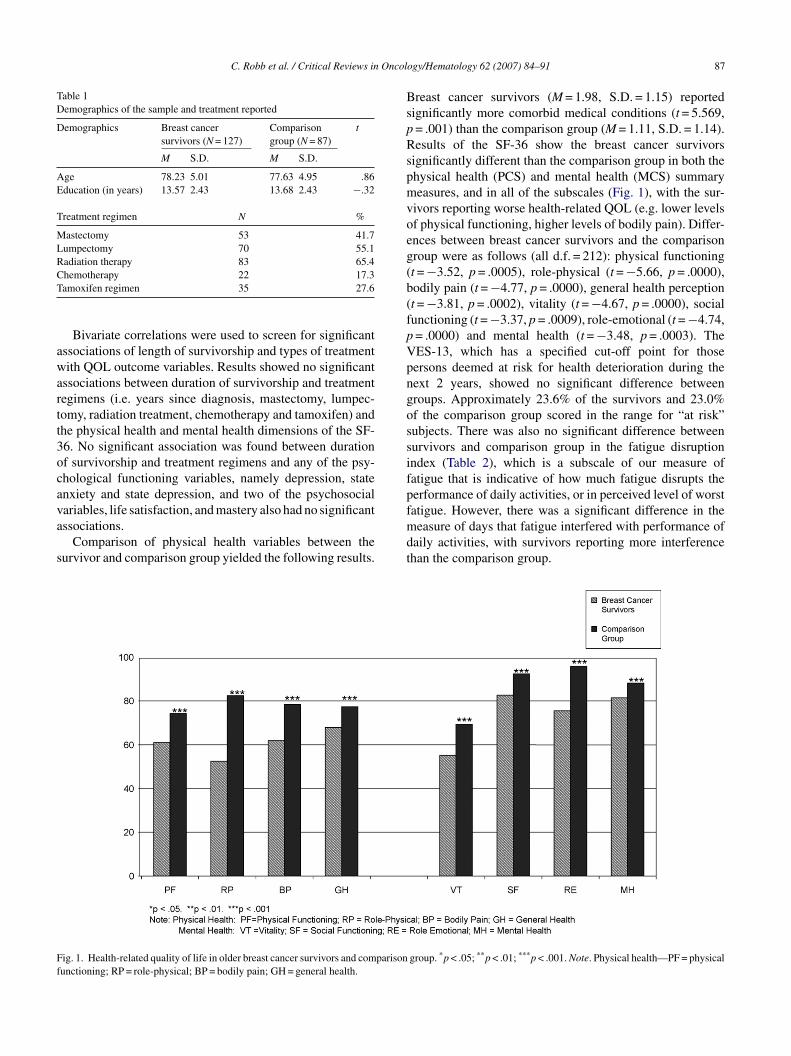
C. Robb et al. / Critical Reviews in Oncol
Table 1Demographics of the sample and treatment reported
Demographics Breast cancersurvivors (N = 127)
Comparisongroup (N = 87)
t
M S.D. M S.D.
Age 78.23 5.01 77.63 4.95 .86Education (in years) 13.57 2.43 13.68 2.43 −.32
Treatment regimen N %
Mastectomy 53 41.7Lumpectomy 70 55.1Radiation therapy 83 65.4CT
awartt3ocava
s
BspRspmvoeg(b(fpVpngossifp
Ff
hemotherapy 22 17.3amoxifen regimen 35 27.6
Bivariate correlations were used to screen for significantssociations of length of survivorship and types of treatmentith QOL outcome variables. Results showed no significant
ssociations between duration of survivorship and treatmentegimens (i.e. years since diagnosis, mastectomy, lumpec-omy, radiation treatment, chemotherapy and tamoxifen) andhe physical health and mental health dimensions of the SF-6. No significant association was found between durationf survivorship and treatment regimens and any of the psy-hological functioning variables, namely depression, statenxiety and state depression, and two of the psychosocial
ariables, life satisfaction, and mastery also had no significantssociations.Comparison of physical health variables between theurvivor and comparison group yielded the following results.
fmdt
ig. 1. Health-related quality of life in older breast cancer survivors and comparisonunctioning; RP = role-physical; BP = bodily pain; GH = general health.
ogy/Hematology 62 (2007) 84–91 87
reast cancer survivors (M = 1.98, S.D. = 1.15) reportedignificantly more comorbid medical conditions (t = 5.569,= .001) than the comparison group (M = 1.11, S.D. = 1.14).esults of the SF-36 show the breast cancer survivors
ignificantly different than the comparison group in both thehysical health (PCS) and mental health (MCS) summaryeasures, and in all of the subscales (Fig. 1), with the sur-
ivors reporting worse health-related QOL (e.g. lower levelsf physical functioning, higher levels of bodily pain). Differ-nces between breast cancer survivors and the comparisonroup were as follows (all d.f. = 212): physical functioningt = −3.52, p = .0005), role-physical (t = −5.66, p = .0000),odily pain (t = −4.77, p = .0000), general health perceptiont = −3.81, p = .0002), vitality (t = −4.67, p = .0000), socialunctioning (t = −3.37, p = .0009), role-emotional (t = −4.74,= .0000) and mental health (t = −3.48, p = .0003). TheES-13, which has a specified cut-off point for thoseersons deemed at risk for health deterioration during theext 2 years, showed no significant difference betweenroups. Approximately 23.6% of the survivors and 23.0%f the comparison group scored in the range for “at risk”ubjects. There was also no significant difference betweenurvivors and comparison group in the fatigue disruptionndex (Table 2), which is a subscale of our measure ofatigue that is indicative of how much fatigue disrupts theerformance of daily activities, or in perceived level of worst
atigue. However, there was a significant difference in theeasure of days that fatigue interfered with performance ofaily activities, with survivors reporting more interferencehan the comparison group.
group. *p < .05; **p < .01; ***p < .001. Note. Physical health—PF = physical
88 C. Robb et al. / Critical Reviews in Oncology/Hematology 62 (2007) 84–91
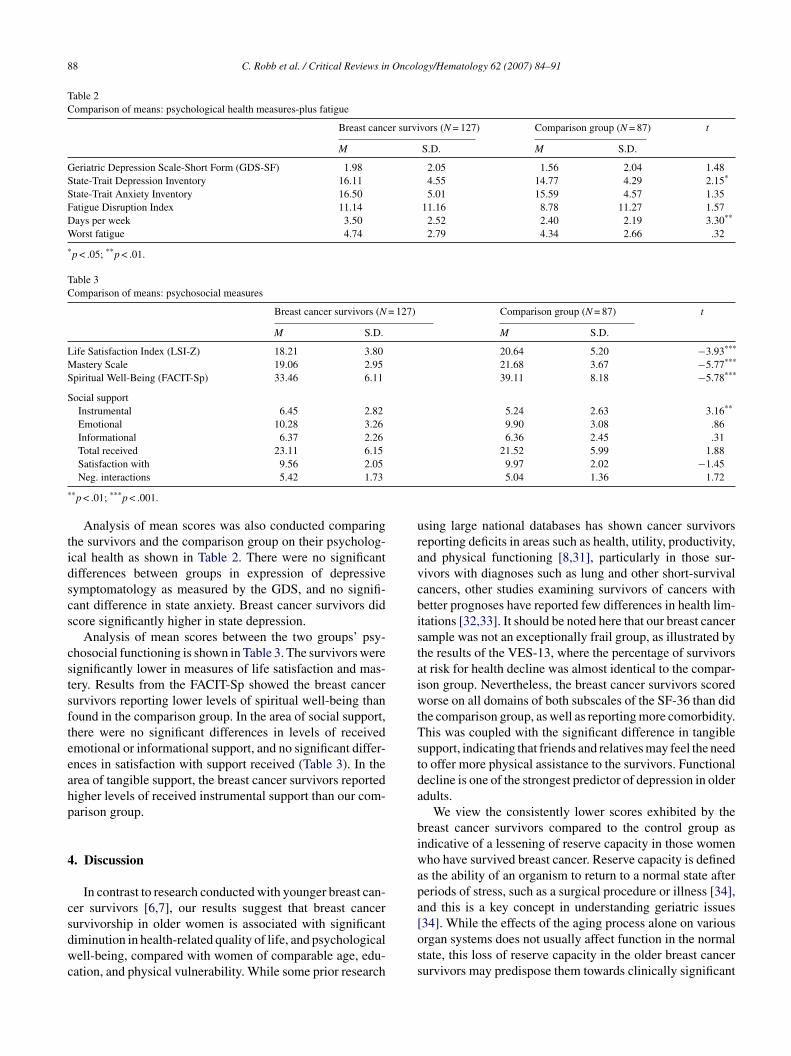
Table 2Comparison of means: psychological health measures-plus fatigue
Breast cancer survivors (N = 127) Comparison group (N = 87) t
M S.D. M S.D.
Geriatric Depression Scale-Short Form (GDS-SF) 1.98 2.05 1.56 2.04 1.48State-Trait Depression Inventory 16.11 4.55 14.77 4.29 2.15*
State-Trait Anxiety Inventory 16.50 5.01 15.59 4.57 1.35Fatigue Disruption Index 11.14 11.16 8.78 11.27 1.57Days per week 3.50 2.52 2.40 2.19 3.30**
Worst fatigue 4.74 2.79 4.34 2.66 .32
*p < .05; **p < .01.
Table 3Comparison of means: psychosocial measures
Breast cancer survivors (N = 127) Comparison group (N = 87) t
M S.D. M S.D.
Life Satisfaction Index (LSI-Z) 18.21 3.80 20.64 5.20 −3.93***
Mastery Scale 19.06 2.95 21.68 3.67 −5.77***
Spiritual Well-Being (FACIT-Sp) 33.46 6.11 39.11 8.18 −5.78***
Social supportInstrumental 6.45 2.82 5.24 2.63 3.16**
Emotional 10.28 3.26 9.90 3.08 .86Informational 6.37 2.26 6.36 2.45 .31Total received 23.11 6.15 21.52 5.99 1.88
*
tidscs
cstsfteeahp
4
csdwc
uravcbistaiwtTstda
biwapa
Satisfaction with 9.56 2.05Neg. interactions 5.42 1.73
*p < .01; ***p < .001.
Analysis of mean scores was also conducted comparinghe survivors and the comparison group on their psycholog-cal health as shown in Table 2. There were no significantifferences between groups in expression of depressiveymptomatology as measured by the GDS, and no signifi-ant difference in state anxiety. Breast cancer survivors didcore significantly higher in state depression.
Analysis of mean scores between the two groups’ psy-hosocial functioning is shown in Table 3. The survivors wereignificantly lower in measures of life satisfaction and mas-ery. Results from the FACIT-Sp showed the breast cancerurvivors reporting lower levels of spiritual well-being thanound in the comparison group. In the area of social support,here were no significant differences in levels of receivedmotional or informational support, and no significant differ-nces in satisfaction with support received (Table 3). In therea of tangible support, the breast cancer survivors reportedigher levels of received instrumental support than our com-arison group.
. Discussion
In contrast to research conducted with younger breast can-er survivors [6,7], our results suggest that breast cancer
urvivorship in older women is associated with significantiminution in health-related quality of life, and psychologicalell-being, compared with women of comparable age, edu-ation, and physical vulnerability. While some prior research
[oss
9.97 2.02 −1.455.04 1.36 1.72
sing large national databases has shown cancer survivorseporting deficits in areas such as health, utility, productivity,nd physical functioning [8,31], particularly in those sur-ivors with diagnoses such as lung and other short-survivalancers, other studies examining survivors of cancers withetter prognoses have reported few differences in health lim-tations [32,33]. It should be noted here that our breast cancerample was not an exceptionally frail group, as illustrated byhe results of the VES-13, where the percentage of survivorst risk for health decline was almost identical to the compar-son group. Nevertheless, the breast cancer survivors scoredorse on all domains of both subscales of the SF-36 than did
he comparison group, as well as reporting more comorbidity.his was coupled with the significant difference in tangibleupport, indicating that friends and relatives may feel the needo offer more physical assistance to the survivors. Functionalecline is one of the strongest predictor of depression in olderdults.
We view the consistently lower scores exhibited by thereast cancer survivors compared to the control group asndicative of a lessening of reserve capacity in those womenho have survived breast cancer. Reserve capacity is defined
s the ability of an organism to return to a normal state aftereriods of stress, such as a surgical procedure or illness [34],nd this is a key concept in understanding geriatric issues
34]. While the effects of the aging process alone on variousrgan systems does not usually affect function in the normaltate, this loss of reserve capacity in the older breast cancerurvivors may predispose them towards clinically significant
Oncol
da
bsmnsfpmmcawd
ippifhfh
cpoceosFclrctFeyaiipabim
itciC
apwious[
Fisnfiwmbcitfmrsscpatiwi
toeFhtdmcdmrniti
R
C. Robb et al. / Critical Reviews in
eclines in well-being when combined with aging and otherge-associated comorbid conditions.
In the area of fatigue, we found no significant differenceetween groups in the fatigue disruption index, which is aubscale of our measure of fatigue that is indicative of howuch fatigue disrupts the performance of daily activities,
or was the worst level of fatigue reported by the groupsignificantly different. We did, however, see a significant dif-erence in the measure of days that fatigue interfered witherformance of daily activities, with the survivors havingore interference than the comparison group. Since treat-ent with tamoxifen is also associated with fatigue [35], we
onducted a post hoc analysis of the survivor group using hier-rchical regression to determine if fatigue levels of survivorsere impacted by presence of this treatment. No significantifference was found.
In light of these results in levels of fatigue, it is interest-ng to note that breast cancer survivors consistently reportedoorer levels of health and physical functioning than the com-arison group. Since the survivor group reported less fatiguen both the fatigue disruption index and worst experiencedatigue, we believe that this is illustrative of the fact thatealth status and fatigue are two distinct constructs. There-ore, fatigue needs to be analyzed separately from perceivedealth status in studies of breast cancer survivors.
As predicted, beyond commonly used measures of physi-al health status and health-related QOL, there were areas ofsychological and psychosocial well-being where the groupf breast cancer survivors in our study fared worse than ouromparison group. While we found no significant differ-nce between groups in psychological functioning in termsf depressive symptomatology, or state anxiety, breast cancerurvivors reported did report higher levels of state depression.urthermore, with regard to psychosocial variables, breastancer survivors also reported significantly lower levels ofife satisfaction, mastery, and spiritual well-being. Theseesults are contrary to previous reports from younger breastancer survivors suggesting their survivorship leads to post-raumatic growth [16,36] and increases in spirituality [37].or older adults, surviving breast cancer may have a differ-nt psychological meaning and psychosocial impact than forounger patients, given the relatively shorter life expectancynd greater likelihood of comorbid illness and functionalmpairment. More in-depth research on these issues of mean-ng of illness in older patients is warranted. Diminution inositive indicators of psychosocial well-being, even in thebsence of significant depressive symptoms, is of concernecause these positive states are important psychosocial cop-ng resources that can help older adults adapt when they face
ajor stressors [38,39].Qualitative data obtained from the breast cancer survivors
ndicated that they did not generally attribute any problems
hey reported to having cancer. In fact, most of the olderancer survivors in our sample attributed any functional lim-tations they experienced to other illnesses, such as arthritis.ancer survivors may not report that their cancer is currentlymC
ogy/Hematology 62 (2007) 84–91 89
ffecting them, even though our results clearly show multi-le negative sequelae in health-related QOL and psychosocialell-being associated with survivorship. This underscores the
mportance of using age-matched comparison groups to studylder cancer survivors, and suggests that clinicians shouldndertake thorough geriatric assessment with older cancerurvivors in order to detect subtle but important impairments40,41].
Our study had several limitations which should be noted.irst, our study was cross-sectional thereby precluding any
nference of causality or change over time. Secondly, ourample and our comparison group were not racially or eco-omically diverse, thereby limiting generalizability of ourndings. Also, medical conditions and functional abilitiesere based on self-report and are subject to recall bias. Theeasure of comorbidity used in this study was restricted
y the need to match the measure already utilized in theontrol group. More sophisticated assessment of comorbid-ty would be very advantageous to future investigations inhis area. Furthermore, subsequent studies would also benefitrom incorporating performance-based measures to deter-ine functional status to minimize the potential impact of
esponse bias on self-reports. Finally, there was no mea-urement of cognitive functioning or formal assessment ofensory impairment included in this study. These aspectsan undoubtedly affect QOL, and would be useful to incor-orate into a comprehensive and multidimensional geriatricssessment. In the present study, as both groups were rela-ively highly functioning, we feel there was likely minimalmpact of cognitive and sensory impairment as all participantsere lucid, alert, and were fully able to complete face-to-face
nterviews with no apparent visual or hearing difficulties.As breast cancer survival rates continue to improve and as
he average life expectancy continues to increase, it is obvi-us that more and more older women will be faced with anxtended number of years of life as breast cancer survivors.unctional health has been shown to correlate with mentalealth both in large studies where functional health and men-al health are measured, as well as in other studies that haveemonstrated a general association between physical andental health [42]. Functional decline can be considered as a
hronic stressor, which may induce stress responses such asepression [43]. Future research should assess whether decre-ents such as those found in our study represent declines in
eserve capacity that may predispose toward clinically sig-ificant declines in well-being and functioning, and considernterventions not only to address clinically significant symp-oms, but also to enhance well-being and functional capacityn older cancer survivors.
eviewers
Catherine Terret, MD, PhD, Centre Leon Berard, Depart-ent of Medical Oncology, 28, rue Laennec, 69373 Lyonedex 08, France.

9 Oncol
C9
A
t
R
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[[
[
[
[
[
B
0 C. Robb et al. / Critical Reviews in
Etienne G.C. Brain, MD, PhD, Rene Huguenin Cancerentre, Department of Medical Oncology, 35 rue Dailly,2210 Saint-Cloud, France.
cknowledgement
This study was funded by a grant from the National Insti-ute on Aging (NIA), Award #1R03AG21210-01
eferences
[1] American Cancer Society, Cancer facts and figures. Atlanta, GA:Author; 2004.
[2] Ganz PA, et al. Breast cancer in older women: quality of life and psy-chosocial adjustment in the 15 months after diagnosis. J Clin Oncol2003;21(21):4027–33.
[3] Deimling GT, et al. Cancer survivorship and psychological distress inlater life. Psychooncology 2002;11(6):479–94.
[4] Lawton MP. A multidimensional view of quality of life in frail elders.In: Birren JE, et al., editors. The concept and measurement of qualityof life in the frail elderly. New York: Academic Press; 1991. p. 3–27.
[5] Arndt V, et al. Age-specific detriments to quality of life amongbreast cancer patients one year after diagnosis. Eur J Cancer2004;40(5):673–80.
[6] Ganz PA, et al. Breast cancer survivors: psychosocial concerns andquality of life. Breast Cancer Res Treat 1996;38(2):183–99.
[7] Ganz PA, et al. Quality of life at the end of primary treatment of breastcancer: first results from the moving beyond cancer randomized trial.J Natl Cancer Inst 2004;96(5):376–87.
[8] Hewitt M, Rowland JH, Yancik R. Cancer survivors in the UnitedStates: age, health and disability. J Gerontol Ser A: Biol Sci Med Sci2003;58A(1):82–91.
[9] Sammarco A. Quality of life among older survivors of breast cancer.Cancer Nurs 2003;26(6):431–8.
10] Vinokur AD, et al. The process of recovery from breast cancer foryounger and older patients. Changes during the first year. Cancer1990;65(5):1242–54.
11] Demissie S, Silliman RA, Lash TL. Adjuvant tamoxifen: predictors ofuse, side effects, and discontinuation in older women. J Clin Oncol2001;19(2):322–8.
12] Moyer A, Salovey P. Psychosocial sequelae of breast cancer and itstreatment. Ann Behav Med 1996;18(2):110–25.
13] Mandelblatt JS, et al. Predictors of long-term outcomes in older breastcancer survivors: perceptions versus patterns of care. J Clin Oncol2003;21(5):855–63.
14] Cimprich B, Ronis DL, Martinez-Ramos G. Age at diagnosis and qual-ity of life in breast cancer survivors. Cancer Pract 2002;10(2):85–93.
15] Gall TL, Cornblat MW. Breast cancer survivors give voice: a qualitativeanalysis of spiritual factors in long-term adjustment. Psychooncology2002;11(6):524–35.
16] Cordova MJ, et al. Posttraumatic growth following breast cancer: acontrolled comparison study. Health Psychol 2001;20(3):176–85.
17] Reinhardt JP. Predicting individual change in social support overtime among chronically impaired older adults. Psychol Aging2003;18(4):2003.
18] Small BJ, et al. Is APOE-epsilon4 a risk factor for cognitive impairmentin normal aging? Neurology 2000;54(11):2082–8.
19] Ware JE, Sherbourne CD. The MOS 36-item short-form health sur-
vey (SF-36). I. Conceptual framework and item selection. Med Care1992;30(6):473–83.20] Saliba D, et al. The Vulnerable Elders Survey: a tool for identify-ing vulnerable older people in the community. J Am Geriatr Soc2001;49(12):1691–9.
idc
ogy/Hematology 62 (2007) 84–91
21] Stein KD, et al. Further validation of the multidimensional fatiguesymptom inventory-short form. J Pain Symptom Manage 2004;27(1):14–23.
22] Yesavage JA. Development and validation of a geriatric depressionscreening scale: a preliminary report. J Psychiatr Res 1983;17:37–49.
23] Shaver PR, Brennan KA. Measures of depression and loneliness. In:Robinson JP, Shaver PR, editors. Measures of personality and socialpsychological attitudes. San Diego, CA: Academic Press, Inc.; 1991.p. 195–289.
24] Lesher EL, Berryhill JS. Validation of the Geriatric Depression Scale-Short Form among inpatients. J Clin Psychol 1994;50(2):256–60.
25] Spielberger C. Understanding stress and anxiety. New York: Harper &Row; 1979.
26] Endler NS, Macrodimitris SD, Kokovski NL. Anxiety and depression:congruent, separate, or both? J Appl Biobehav Res 2003;8(1):42–60.
27] Andrews FM, Robinson JP. Measures of subjective well-being. In:Robinson JP, Shaver PR, editors. Measures of personality and socialpsychological attitudes. San Diego, CA: Academic Press, Inc.; 1991.p. 61–114.
28] Pearlin LI, Schooler C. The structure of coping. J Health Soc Behav1978;19(1):2–21.
29] Peterman AH, et al. Measuring spiritual well-being in people withcancer: the functional assessment of chronic illness therapy—SpiritualWell-being Scale (FACIT-Sp). Ann Behav Med 2002;24(1):49–58.
30] Krause N, Borawski-Clark E. Social class differences in social supportamong older adults. Gerontologist 1995;35(4):498–508.
31] Yabroff KR, et al. Burden of illness in cancer survivors: find-ings from a population-based national sample. J Natl Cancer Inst2004;96(17):1322–30.
32] Dorval M, et al. Long-term quality of life after breast cancer: com-parison of 8-year survivors with population controls. J Clin Oncol1998;16(2):487–94.
33] Ramsey SD, et al. Quality of life in long term survivors of colorectalcancer. Am J Gastroenterol 2002;97(5):1228–34.
34] Evers BM, Townsend Jr CM, Thompson JC. Organ physiology of aging.Surg Clin North Am 1994;74(1):23–39.
35] Mast ME. Correlates of fatigue in survivors of breast cancer. CancerNurs 1998;21(2):136–42.
36] Manne S, et al. Posttraumatic growth after breast cancer: patient, part-ner, and couple perspectives. Psychosom Med 2004;66(3):442–54.
37] Helgeson VS, Tomich PL. Surviving cancer: a comparison of 5-yeardisease-free breast cancer survivors with healthy women. Psychoon-cology; 2004.
38] Lawton MP. The varieties of well-being. Exp Aging Res 1983;9:65–72.39] Bradburn N. The structure of psychological well-being. Chicago:
Aldine; 1969.40] Wedding U, Hoffken K. Care of breast cancer in the elderly
woman—what does comprehensive geriatric assessment (CGA) help?Support Care Cancer 2003;11(12):769–74.
41] Extermann M, et al. A comprehensive geriatric intervention detectsmultiple problems in older breast cancer patients. Crit Rev OncolHematol 2004;49(1):69–75.
42] Lawton MP. Functional status and aging well. Generations1991;15:31–4.
43] Kempen GIJ, et al. The relationship of functional limitations todisability and the moderating effects of psychological attributes incommunity-dwelling older persons. Social Sci Med 1999;48:1161–72.
iographies
Claire Robb, Ph.D., MPH, received her doctorate degreen Aging Studies and her Master of Public Health in Epi-emiology from the University of South Florida in 2003. Sheompleted a 2-year NCI-sponsored fellowship in behavioral

Oncol
oHRPa
Aasp
gOOOC
o
aSw
tMiS
ojaCInstitute.
C. Robb et al. / Critical Reviews in
ncology with the Senior Adult Oncology Program at the. Lee Moffitt Cancer Center and Research Institute. Dr.obb is currently an Assistant Professor in the College ofublic Health at the University of Georgia and has a jointppointment with the Institute of Gerontology at UGA.
William E. Haley, Ph.D., is Director of the School ofging Studies at the University of South Florida and is alsomember of the Moffitt Cancer Center. Dr. Haley has exten-
ive experience in conducting longitudinal research on thesychosocial consequences of chronic illness in older adults.
Lodovico Balducci, M.D., is the chief of the section oferiatric oncology within the Department of Interdisciplinaryncology at the University of South Florida, Professor ofncology and Medicine and the founder of the Senior Adult
ncology Program (SAOP) at the H. Lee Moffitt Cancerenter and Research Institute.Martine Extermann, M.D., Ph.D., is Associate Professorf Oncology and Medicine at the University of South Florida
iF
ogy/Hematology 62 (2007) 84–91 91
nd attending physician at the H. Lee Moffitt Cancer Center.he is a Faculty in the Senior Adult Oncology Program, ofhich she is the research director.
Elizabeth A. Perkins, RNMH, B.A., received her nurseraining at the Hereford and Worcester College of Nursing and
idwifery, Worcester, England. She is a doctoral candidaten the Ph.D. in Aging Studies Program at the University ofouth Florida.
Brent J. Small, Ph.D., is Associate Professor in the Schoolf Aging Studies at the University of South Florida, holds aoint appointment in the Department of Psychology at USFnd is an Associate Professor in the Biostatistics Resourceore at the H. Lee Moffitt Cancer Center and Research
James Mortimer, Ph.D., is Professor of Epidemiologyn the College of Public Health at the University of Southlorida.