Embed Size (px)
Citation preview

TAYLOR COLLISON LTD. www.taylorcollison.com.au
ABN 53008172450 AFSL 247083 1
Dr DENNIS HULME
+612 9377 1500
www.taylorcollison.com.au
Speculative Investment
Immutep (IMM)
Leading not LAGging
Our View
Immutep is developing therapies based on LAG-3 through in-house programs
and licensing deals with big pharma. Its share price fell last month when the
progression free survival benefit from adding its antigen presenting cell activator
‘efti’ to chemo in the AIPAC Phase IIb breast cancer study failed to reach
statistical significance. However, the higher tumour response rate in AIPAC
(48% vs 38%) indicates that efti activates the immune system. We view this as a
strong positive indicator for the continued success of ongoing studies of efti plus
the immune checkpoint inhibitors (ICI) Keytruda and Bavencio – response rates
for melanoma, lung and head and neck cancers have been at least 50% higher
than the rates reported for Keytruda alone. ICI combos are where the real value
in efti lies, in our view. IMM’s value is further supported by Phase II LAG-3
programs out-licensed to Novartis and GSK. We initiate coverage with a risk
adjusted DCF valuation of A$327m or $0.53/sh fully diluted ($0.83/sh undiluted).
Key Points
Efti plus chemo not sufficiently active in metastatic breast cancer –
Immutep’s lead in-house product, efti, delivered only modest, non-significant
improvements in tumour response rates and progression free survival when to
chemotherapy in breast cancer patients in AIPAC. We did not believe that
combining eft with chemo was the optimum therapeutic approach, as the
immunosuppressive local environment within tumours can shut down anti-
tumour immune responses. On the other hand, efti’s mechanism of action of
activating antigen presenting cells to initiate an immune response (pushing on
the accelerator) is complementary to checkpoint inhibitors which ‘take the brakes
off’ anticancer immune responses. We do not expect IMM to invest further funds
in the efti/chemo combo in breast cancer unless new data come to light.
A promising checkpoint inhibitor combo – ICI drugs such as Keytruda and
Opdivo have transformed the treatment of a number of cancers in recent years.
However, only a minority of patients respond to ICI therapy, and treatments
which can be combined with ICI drugs to improve response rates are being
urgently sought. Efti has reported high response rates from ICI combo studies
which should attract attention from potential pharma partners. The inclusion of
IMM’s update on the ICI combo study in the high impact paper session at the
AACR conference on 27/28 April suggests the data could be very encouraging.
By year-end data set will be comparable to Viralytics at time of $500m
Merck deal. Immutep’s strategy for efti is similar to that pursued by Viralytics in
its development of the Cavatak immuno-oncology therapy, which led to its
acquisition by Merck for ~$500m in 2018. Within the next 12 months Immutep
should have data on efti plus Keytruda in 120-130 patients with melanoma, lung
and head and neck cancer. This should be enough data for Merck to get a good
understanding of how well the drug works. If efti is an effective therapy, in our
view it should be worth more than Viralytics because it can be used in a much
wider range of cancer types. We do not believe that the potential for a significant
deal to occur in the next 12-18 months is reflected in the current share price.
Out-licensed LAG-3 programs in Phase II with big pharma - Immutep has
two additional LAG-3 programmes that that are partnered with big pharma and
could create significant value; both of these programs have recently progressed
to Phase II (mid-stage) trials which represent significant investments by the
pharma partner. These programs are an anti-LAG-3 antibody in cancer
partnered with Novartis and a LAG-3 depleting antibody in inflammatory
disorders partnered with and GSK.
22 April 2020
Recommendation: Outperform
Summary (AUD)
Market Capitalisation $59M
Share price $0.15
52 week low $0.11
52 week high $0.49
Cash as at 31 March 2020 $16.1m
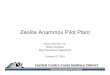
Share price graph (AUD)
Key Financials (AUD)
FY19A FY20E FY21E FY21F
Revenue 6.6 13.0 5.6 6.6
R&D (16.6) (19.8) (14.0) (16.6)
SG&A (7.4) (7.1) (7.3) (7.4)
EBITDA (17.4) (13.9) (15.7) (17.4)
Reported NPAT
(18.3) (13.8) (15.6) (18.3)
NPAT Adj. (18.3) (13.8) (15.6) (18.3)
EPS Adj. (c) (5.7) (3.8) (3.2) (5.7)
PE ratio (x) n/a n/a n/a n/a
DPS (c) 0.0 0.0 0.0 0.0
EV/Sales n/a n/a n/a
EV/EBITDA (x)
n/a n/a n/a n/a
ROE n/a n/a n/a n/a
0.00
0.10
0.20
0.30
0.40
0.50
0.60CGS
0.00
0.05
0.10
0.15
0.20
0.25
0.30
0.35
0.40
0.45
0.50IMM ASX Small Ords

TAYLOR COLLISON LTD. www.taylorcollison.com.au
ABN 53008172450 AFSL 247083 2
Immutep (IMM)
22 April 2020
Immutep - Summary of Forecasts IMM 0.15$
PROFIT & LOSS SUMMARY (A$ m) BALANCE SHEET SUMMARY
Ye a r e nd June FY19 A FY2 0 E FY2 1E FY2 2 E Ye a r e nd June FY19 A FY2 0 E FY2 1E FY2 2 E
Sales, royalties, milestones 0.1 7.4 0.0 9.5 Cash 16.6 13.0 26.5 21.4
Other (includes R&D tax rebate) 6.5 5.6 5.6 5.6 Receivables 5.2 5.2 5.2 5.2
Tota l Re ve nue 6 .6 13 .0 5 .6 15 .1 Inventories 0.0 0.0 0.0 0.0
Growth (pcp) - 3.7% 96.4% - 56.8% 169.7% Other 1.8 1.8 1.8 1.8
R&D Expenses (16.6) (19.8) (14.0) (14.0) Total Current Assets 23.5 19.9 33.5 28.3
SG&A expenses (7.4) (7.1) (7.3) (7.5) Inventories 0.0 0.0 0.0 0.0
EBITDA (17 .4 ) (13 .9 ) (15 .7 ) (6 .4 ) Property Plant & Equip 0.1 0.1 0.2 0.3
Dep'n/Other Amort'n (1.9) (0.0) (0.0) (0.0) Intangibles 16.9 16.9 16.9 16.9
EBIT (19.2) (14.0) (15.7) (6.5) Other 0.0 0.0 0.0 0.0
Net Interest 0.4 0.2 0.1 0.3 Total Current Assets 17.0 17.1 17.2 17.2
Pre- Tax Profit (18.3) (13.8) (15.6) (6.2) TOTAL ASSETS 4 0 .5 3 7 .0 5 0 .7 4 5 .5
Tax Expense 0.0 0.0 0.0 0.0 Accounts Payable 5.1 5.1 5.1 5.1
Minorities 0.0 0.0 0.0 0.0 Borrowings 0.0 0.0 0.0 0.0
NPAT Adj. (18 .3 ) (13 .8 ) (15 .6 ) (6 .2 ) Provisions 0.2 0.2 0.2 0.2
Growth (pcp) n/a n/a n/a n/a Other 0.0 0.0 0.0 0.0
Adjustments 0.0 0.0 0.0 0.0 Total Current Liab 5.3 5.3 5.3 5.3
NPAT Reported (18.3) (13.8) (15.6) (6.2) Borrowings 0.0 0.0 0.0 0.0
Provisions 0.0 0.0 0.0 0.0
PER SHARE DATA Other 10.9 10.9 10.9 10.9
Ye a r e nd June FY19 A FY2 0 E FY2 1E FY2 2 E Total Non- Current Liab 10.9 10.9 10.9 10.9
EPS (c ) - Re porte d (5 .7 ) (3 .8 ) (3 .2 ) (1.1) TOTAL LIABILITIES 16 .2 16 .2 16 .2 16 .2
Growth (pcp) n/a n/a n/a n/a TOTAL EQUITY 2 4 .4 2 0 .9 3 4 .5 2 9 .4
EPS (c) - Adjusted (5.7) (3.8) (3.2) (1.1)
Growth (pcp) n/a n/a n/a n/a CASH FLOW SUMMARY
Dividend (c) 0.0 0.0 0.0 0.0 Ye a r e nd June FY19 A FY2 0 E FY2 1E FY2 2 E
Franking 0.0 0.0 0.0 0.0 EBIT (e xc l Abs/Extr) (19 .2 ) (14 .0 ) (15 .7 ) (6 .5 )
Gross CF per share (c) (4.7) (3.5) (3.0) (0.9) Add: Dep'n & Amort'n 1.9 0.0 0.0 0.0
NTA per share (c) 2.2 1.0 3.0 2.1 Other non- cash items (4.5) (1.4) (1.4) (1.7)
Less: Tax paid 0.0 0.0 0.0 0.0
KEY RATIOS Net Interest 0.4 0.2 0.1 0.3
Ye a r e nd June FY19 A FY2 0 E FY2 1E FY2 2 E Change in Rec. (1.8) 0.0 0.0 0.0
Net Debt : Equity (%) - 67.9% - 62.1% - 76.9% - 72.7% Change in Inv. 0.0 0.0 0.0 0.0
Net Debt: EBITDA (x) 1.0 0.9 1.7 3.3 Gross Cashflows (15.3) (12.7) (14.5) (5.1)
Current ratio (x) 4.4 3.8 6.3 5.3 Capex (0.0) (0.1) (0.1) (0.1)
ROE (%) - 63.4% - 60.9% - 56.4% - 19.5% Free Cashflows (15.3) (12.8) (14.6) (5.2)
ROIC (%) n/a n/a n/a n/a Share Issue Proceeds 8.0 9.2 28.2 0.0
Dividend Payout Ratio (%) n/a n/a n/a n/a Other 0.4 0.0 0.0 0.0
Dividends Paid 0.0 0.0 0.0 0.0
VALUATION MULTIPLES Ne t Ca shflows (6 .9 ) (3 .6 ) 13 .6 (5 .2 )
Ye a r e nd June FY19 A FY2 0 E FY2 1E FY2 2 E FX Effect on Cash 0.4 0.0 0.0 0.0
PE Ra tio (x) n/a n/a n/a n/a
Divide nd Y ie ld (%) 0 .0 % 0 .0 % 0 .0 % 0 .0 % IMM ba se c a se va lua tion summa ry (undilute d)
EV/Sales (x) n/a n/a n/a n/a Proba bilityVa lua tion Va lue
EV/EBITDA (x) n/a n/a n/a n/a (%) (A$ m) (A$ /sha re )
EV/EBIT (x) n/a n/a n/a n/a efti/ICI NSC lung cancer 15% 96.5 0.25
efti/ICI head & neck cancer 15% 46.4 0.12
CAPITAL RAIS ING ASSUMPTIONS efti/ICI melanoma 15% 11.4 0.03
Ye a r e nd June FY19 A FY2 0 E FY2 1E FY2 2 E efti/chemo breast cancer 2% 6.8 0.02
Shares Issued (m) 26.0 47.8 187.5 0.0 efti milestones - partner post TACTI- 002 15- 50% 80.5 0.21
Issue Price (A$) 0.34 0.21 0.16 LAG525 solid tumours (lung cancer) 20% 54.7 0.14
Cash Raised (A$m) 8.8 10.0 30.0 GSK’781 - ulcerative colitis 20% 54.9 0.14
SG&A - (23.8) (0.06)
Portfolio total - 327.4 0.84
Net cash end FY20e (incl conv note face value) - (0.8) (0.00)
Total Valuation - 326.7 0.83

TAYLOR COLLISON LTD. www.taylorcollison.com.au
ABN 53008172450 AFSL 247083 3
Immutep (IMM)
22 April 2020
Overview
Immutep is an ASX-listed immunotherapy company that is focused on developing products based on the lymphocyte activation
gene 3 (LAG-3) pathway, following the acquisition of a private French immunotherapy company in December 2014. Two of its
pipeline products, efti and LAG525, enhance anti-cancer immune responses. Two other products, GSK’781 and IMP761, target
LAG-3 to suppress undesirable immune responses in auto immune disease. Exhibit 1 summarises the 4 pipeline products and
Exhibit 2 illustrates how they target the immune system.
Its lead product, efti (eftilagimod alpha; IMP321), is in Phase II in combination with the checkpoint inhibitor Keytruda in lung and
head and neck cancers. Immutep retains all the product rights to efti except for China (where it is partnered with EOC Pharma).
LAG525, which is licensed to Novartis, is in Phase II studies for solid tumours and lymphoma in combination with a checkpoint
inhibitor. GSK’781, which is licensed to GSK, progressed to a Phase II study for ulcerative colitis in 2019, earning Immutep a
GBP4m (A$7.4m) milestone payment. Its newest product candidate, IMP761 for autoimmune disease, is currently undergoing
manufacture in preparation for a Phase I clinical trial. The company has facilities in Paris, France; Leipzig and Berlin, Germany;
and its headquarters are in Sydney, Australia.
Exhibit 1: Immutep’s pipeline of LAG-3 products
Product /Partner Indication Status Notes
efti/EOC, (China)/ Merck & Co clinical trial collaboration/ Merck KGaA & Pfizer clinical trial collaboration
lung cancer, head and neck cancer & melanoma + Keytruda; Solid tumours + Bavencio; Metastatic breast cancer + chemotherapy
Phase II Phase I Phase IIb/
Clinical trials underway of efti antigen-presenting cell activator combined with immune checkpoint inhibitors. Efti/Keytruda combo studies in lung cancer and head and neck cancer are being conducted in collaboration with Merck & Co (MSD). Efti/Bavencio combo study in solid tumours in collaboration with Merck KGaA and Pfizer. The Phase IIb AIPAC study of efti + chemo in metastatic breast cancer failed to significantly improve progression free survival. WuXi AppTec China produces efti under terms of partnership with EOC, to US European and Chinese GMP standards.
LAG525/ Novartis (worldwide)
Cancer and chronic infectious disease
Phase II Antagonist anti-LAG-3 antibody, activates T-cell proliferation, immune checkpoint blocker. Five Phase I/II or Phase II trials are underway in solid tumours including melanoma, breast, lung and neuroendocrine cancers as well as lymphoma.
GSK’781/ GSK (worldwide) Autoimmune disease/ulcerative colitis
Phase II Depleting anti-LAG-3 antibody, depletes activated T-cells. Phase I trial in patients with plaque psoriasis completed. Phase II in ulcerative colitis underway, topline data due 2022. Potential milestone payments of up to GBP64m + royalties.
IMP761 Autoimmune disease
Preclinical First in class LAG-3 agonist antibody. Aims to help treat autoimmune disease by temporarily switching off activated LAG-3+ T cells.
Source: Immutep, Taylor Collison research.
Exhibit 2: IMM products use LAG-3 technology to either stimulate or suppress immune responses
Source: Immutep.

TAYLOR COLLISON LTD. www.taylorcollison.com.au
ABN 53008172450 AFSL 247083 4
Immutep (IMM)
22 April 2020
Immutep’s lead product, efti, is a LAG-3 Ig fusion protein that is based on the soluble form of LAG-3 and can activate antigen
presenting cells (APCs) to stimulate the initial steps of the immune response. These activated APCs process tumour antigens,
transport the antigens to lymph nodes and present the tumour antigens to T lymphocytes, thus activating and amplifying the
immune response. Levels of CD4and CD8 T cells and natural killer cells are all elevated in response to efti treatment.
Exhibit 3: Efti LAG-3 fusion protein activates APCs
Source: Immutep. Note: IMP321= efti
Immutep is currently collaborating with Merck & Co (known as MSD outside the US and Canada) to investigate efti in
combination with Keytruda in lung cancer and head and neck cancer. Immutep recently reported the results of a Phase II study
of efti combined with chemotherapy in breast cancer. It is also collaborating with Germany-based Merck KGaA and Pfizer in an
earlier stage study investigating efti in combination with Bavencio (avelumab).
ICI drugs such as Keytruda and Opdivo have transformed the treatment of a number of cancers in recent years. Keytruda and
Opdivo generated sales of US$11.1bn and US$7.2bn respectively in 2019. According to the market research group
EvaluatePharma, they are expected to achieve sales of US$17bn and US$10.5bn respectively in 2024, so a successful ICI
combination therapy would be expected to generate substantial sales.
Scientist who discovered LAG3 part of the Immutep team
The scientist who discovered the LAG-3 gene in 1990, Professor Frédéric Triebel, is Immutep’s Chief Scientific Officer and Chief
Medical Officer. Professor Triebel’s deep understanding of LAG-3 and its potential applications in medicine has given Immutep a
position of scientific leadership in the LAG-3 space. While a number of companies are developing anti-LAG-3 antibodies as
checkpoint blockade therapies to enhance T-cell activity in cancer (including Immutep’s partner Novartis) no other company can
match the breadth of Immutep’s LAG-3 pipeline, with two different therapeutic approaches to enhance immune responses in
cancer (efti and LAG525), plus another two approaches to suppressing undesirable immune responses in autoimmune disease..
In addition to this scientific expertise, Immutep has and experienced management team with runs on the board. Chairman Dr
Russel Howard is an experienced scientist, entrepreneur and manager; he was a cofounder and CEO of Maxygen when it was
spun out of GSK and listed on NASDAQ. After leaving Maxygen in 2008 he started the cleantech company NovoNutrients Inc.
Deputy Chairman Pete Myers is the CFO of Eagle Pharmaceuticals (NASDAQ: EGRX) and was previously CFO of NASDAQ-
listed Motif Biosciences and TetraLogic Pharmaceuticals. CEO marc Voight joined Immutep in 2011 and was appointed CFO in
2012 and CEO in 2014; before joining Immutep Marc worked for a number of years as an investment manger for a mid-sized VC
fund base din Berlin, specialising in healthcare, and held management roles with Revotar Biopharmaceuticals, Caprotec
Bioanalytics and Medical Enzymes AG.
AIPAC – evidence of activity but progression free survival benefit falls short
Last month Immutep announced results showing that its AIPAC study failed to deliver a statistically significant improvement in
progression free survival (PFS) in breast cancer patients. The Phase IIb AIPAC trial compared efti plus paclitaxel chemotherapy
to chemotherapy alone in 227 patients with metastatic breast cancer who were undergoing first-line chemotherapy. The study
recruited women with hormone receptor positive, HER2 negative cancer, who comprise the largest subset of breast cancer
patients.

TAYLOR COLLISON LTD. www.taylorcollison.com.au
ABN 53008172450 AFSL 247083 5
Immutep (IMM)
22 April 2020
There was a modest 7% reduction in the risk of disease progression in patients receiving the efti combo, but the effect was not
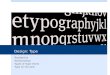
statistically significant (hazard ratio=0.93, p=0.34). As the chart below shows, there was a separation of the progression free
survival curves in favour of efti during the six month period when the patients received efti plus chemotherapy, but the curves
come together after the chemotherapy treatment stops. The median progression free survival was the same in both treatment
arms at 7.3 months.
The AIPAC study built on an earlier study published in 2010 which reported a response rate1 (at least 30% tumour shrinkage) of
50% among 30 women with hormone receptor positive, HER2 negative breast cancer. That paper compared the response rate
to response rate to paclitaxel monotherapy of 25%. A more recent study reported a response rate of 41% following paclitaxel
monotherapy in a similar, but not identical patient population (80% hormone receptor positive cancer)2.
The response rate in efti plus paclitaxel treatment arm of AIPAC in the was 48%, similar to the previous study, but the response
rate of 38% in patients treated with chemo alone was at the upper end of the range reported in previous studies. No p-values
were reported, but we suspect that the difference was not statistically significant.
Exhibit 4: Progression free survival curves for efti/chemo combo vs chemo alone in AIPAC
Source: Immutep. Note: efti is labelled as IMP321; data shown is for the blinded, centralised assessment of tumour progression by an independent investigator.
Immutep identified two patient subgroups where there was a large, but not statistically significant, improvement in progression
free survival. In patients with a low innate immune response at baseline, expressed as a low monocyte count, the efti- treated
group had a 39% reduction in disease progression (HR 0.61, p=0.08). The apparent benefit in this patient group makes sense,
given efti’s mechanism of action in stimulating the innate immune system, but the low monocyte count group only represented
around 21% subjects in the trial. Women with the more aggressive luminal B tumoural subtype also showed lower disease
progression (HR=0.65, p=0.06). These two subgroups could both be interesting areas of future research.
Immutep’s Chinese partner for efti, EOC Pharma, intends to continue with its ongoing Phase I study of the efti/chemo combo in
breast cancer patients, despite the disappointing AIPAC results. There could potentially be scope for EOC Pharma to
investigate one or both of the breast cancer subgroups on future studies of the combo.
1 Immutep reports objective tumour responses in AIPAC andTACTI-002 as defined by irRECIST, a set of published criteria designed to ensure consistent reporting of responses to treatment in clinical trials of anti-cancer drugs. Under irRECIST, up to 5 tumours are identified as target lesions and the longest diameter of each target lesion is recorded (the shortest diameter is recorded for metastatic lymph nodes selected as target lesions). The measure of overall tumour burden at baseline is defined as the sum of these target tumour diameters. Progressive disease (PD) is defined as a 20% increase in the sum of tumour diameters, or the appearance of one or more new lesions. A partial response (PR) is a 30% decrease in the sum of diameters, with no new lesions allowed. A complete response (CR) is the complete disappearance of all lesions. Stable disease is neither sufficient shrinkage to qualify as PR nor sufficient increase to qualify for PD, and no new lesions. If the response rate is the main efficacy endpoint of the study, then the responses should be confirmed at a second scan at least 4 weeks after the first. 2 Martin et al, Lancet Oncol 2011; 12: 369–76

TAYLOR COLLISON LTD. www.taylorcollison.com.au
ABN 53008172450 AFSL 247083 6
Immutep (IMM)
22 April 2020
Positive implications from AIPAC for ongoing ICI combo studies
We were looking AIPAC to answer two key questions:
• Firstly, is efti plus chemo an effective therapy in breast cancer?
• Secondly, is there evidence that efti is an active anti-cancer agent that could provide meaningful benefit to patients when
combined with immune checkpoint blockade?
The answer to the first question currently appears to be no, although the history of Provenge3 in prostate cancer means that it is
still possible that there could be an overall survival benefit. Overall survival data is expected to be reported later in 2020.
However, we find the AIPAC data much more encouraging as a pointer to the potential benefit of efti/ICI combo therapy. The
numerically higher response rate (48% vs 38%) and the separation of the progression free survival curves indicates to us that
efti has immune stimulating activity, in line with the proposed method of action, although the activity was not sufficient to be a
useful therapy in this treatment setting in breast cancer.
We have learnt over the past decade that many tumours are able to grow because of the immunosuppressive tumour
microenvironment created by tumours expressing immune checkpoint inhibitor molecules such as PD-L1 and PD-L2. One
possible explanation for the modest efficacy observed in AIPAC is that an immunosuppressive tumour microenvironment may
have limited the benefit that could be obtained by efti activating APCs to enhance the initial immune response.
In our view, this points to the logical step of combining efti with simultaneous blockade of immune checkpoint pathways by anti-
PD1/L1 antibodies as Keytruda (pembrolizumab) or similar drugs to overcome the immunosuppressive tumour
microenvironment. The company has already reported very encouraging response rates when efti was combined with Keytruda
in three different diseases, as described below. Based on the AIPAC results we believe that an efti/Keytruda/chemo triple
combo could be an effective therapy in metastatic breast cancer.
TACTI-002 reports high response rates from checkpoint inhibitor combo studies
Immutep has reported very encouraging results over the past six months from its TACTI-002 checkpoint inhibitor combo study.
TACTI-002 is investigating the safety and efficacy of efti plus Merck’s anti-PD1 ICI drug Keytruda (pembrolizumab) in head and
neck cancer and in first and second line lung cancer settings. The open label, single arm study (no placebo control group),
which is being conducted in collaboration with Merck & Co, is enrolling up to 109 patients at up to 13 sites in Europe, the US
and Australia.
Patients will receive 12 months of efti/Keytruda combination therapy, followed by a further 12 months of Keytruda monotherapy
(Exhibit 5). Treatment with efti (30mg by subcutaneous (SC) injection) starts on the same day as Keytruda; efti is administered
every two weeks for the first 24 weeks (8 cycles of Keytruda) after which efti is administered every three weeks, to align with the
Keytruda treatment schedule. The primary efficacy assessment is the overall response rate (ORR; as per irRECIST).
Exhibit 5: TACTI-002 trial design
Source: Immutep. Note: One cycle: three weeks; q2w: every two weeks; q3w: every three weeks; pembrolizumab= Keytruda
3 Provenge, which like efti targeted dendritic antigen presenting cells, produced a statistically significant improvement in overall survival despite only a non-significant 6% improvement in progression free survival (hazard ratio 0.94).

TAYLOR COLLISON LTD. www.taylorcollison.com.au
ABN 53008172450 AFSL 247083 7
Immutep (IMM)
22 April 2020
The three patient populations targeted in TACTI-002 are:
• Part A: first-line advanced/metastatic non-small cell lung cancer (NSCLC) patients, who are PD-1/L-1 naive and have not
undergone systemic therapy for advanced/metastatic disease.
• Part B: second-line advanced/metastatic NSCLC patients who have experienced confirmed treatment failure (disease
progression) following treatment with any PD-1/PD-L1 regimen.
• Part C: second-line squamous cell carcinoma of the head and neck (HNSCC) patients who are PD-1/L1 naive.
The TACTI-002 study is using Simon’s two-stage design, in which the study only recruits the full number of subjects if the initial
cohort shows promising results. For each of the three treatment indications, an initial cohort of 17–23 patients is being treated.
For each indication, if the number of patients with tumour responses exceeds a pre-specified threshold, additional patients will
be recruited to take the total to ~37 for that indication, as shown in Exhibit 6. Recruitment has already progressed to the
expansion cohorts for parts A and C in first line lung cancer and head and neck cancer, respectively.
Exhibit 6: TACTI-002 trial design and summary interim data
Indication Recruitment in
initial cohort
Minimum number of responses
required
Number of responders reported in
initial cohort
Response rate in initial
cohort
Recruitment in expansion
cohort
Total patients
Keytruda monotherapy
ORR
Part A: NSCLC 1st line 17/17 5 8 47% 17/19 36.0 25%*
Part B: NSCLC PD1/L1 refractory 2nd line
18/23 2 - - -/13 36.0 N/A
Part C: HNSCC PD1/L1 naïve 2nd line
18/18 3 6 33% 6/19 37.0 16-18%**
Source: Immutep, Taylor Collison research. Note: #to aid clarity we have expressed the threshold as the minimum number of
responses to be achieved; *Keynote-001 study; **Keynote-012 study
The best overall response rates for efti/Keytruda combo reported so far have been 47% (8/17) in first line lung cancer (vs ~25%
ORR for Keytruda monotherapy) and 33% (6/18) in head and neck cancer (vs 16-18% ORR).
In the earlier Phase I TACTI-mel study of efti plus Keytruda therapy in melanoma, the response rate was ~50% (14 out of 27 or
28), which compares to the response rate of ~33% to Keytruda monotherapy in melanoma trials. In these three disease settings
the response rates to date have been at least 50% higher (melanoma) and up to 100% higher (head and neck cancer) than the
response rates reported following Keytruda monotherapy in similar patient populations.
Efti is well tolerated in combination with Keytruda, with no dose-limiting toxicities reported.
Lung cancer patients responded to efti/Keytruda combo at all PD-L1 expression levels
The interim data from the initial cohort in Part A of the study showed that 8 out of 17 (47%) first-line NSCLC patients had
achieved a partial response as of the data cut-off on 31 January. Ten patients were still receiving the combination therapy at
least 7 months after commencing treatment. Exhibit 7, below, shows that one of the subjects with stable disease is experiencing
ongoing tumour shrinkage which is approaching the 30% threshold that would qualify as a partial response; if this subject goes
on to experience a partial response then that would push the response rate over 50%. The exhibit also shows that the tumour
responses are long-lasting, with 7 of the 8 responders remaining on therapy with ongoing responses.
The expansion cohort in Part A of the study has recruited 17 out of the target of 19 additional subjects
Part A recruited all comers, regardless of the level of expression of the PD-L1 biomarker in their tumour.

TAYLOR COLLISON LTD. www.taylorcollison.com.au
ABN 53008172450 AFSL 247083 8
Immutep (IMM)
22 April 2020
Exhibit 7: Spider plot showing individual patient tumour responses in first line lung cancer (NSCLC) in TACTI-002
Source: Immutep. Note: the upper dashed line marks the 20% increase in tumour size that is the threshold for progressive disease and the lower dashed line marks the 30% decrease in tumour size that is the threshold for a partial response; NE = PD-L1 expression not evaluable in tumour tissue sample.
At the time of the data cut-off, Immutep was able to assess tumour samples from 13 of the 17 first-line NSCLC patients for
expression of the PD1 biomarker, which is a predictor of response rates to Keytruda monotherapy, as shown in Exhibits 7 and 8.
Exhibit 8 also shows the overall response rate reported for first line NSCLC patients with low, medium and high PD-L1
expression following Keytruda monotherapy treatment in the Keynote-001 study.4 We note that the Keynote-001 overall
response rate (ORR) data only incudes patients where the tumour shrinkage was confirmed in a second scan, whereas the best
overall response rate (BORR) reported for the ongoing TACTI-002 study includes patients with tumour responses that have not
yet been confirmed at a second scan, and so the data are not directly comparable. Despite this caveat, it is clear that the
response rate following efti/Keytruda combo therapy (BORR 47%) is much higher than the 25% ORR reported for a similar
patient population treated with Keytruda monotherapy in the Keynote-001 trial.
Exhibit 8: TACTI-002 Part A first line lung cancer responses by PD-L1 expression category
PD-L1 expression category Number of patients (% of
evaluable) in Part A
Historical distribution#
No. of responders in
Part A*
Best overall response
rate to efti/Keytruda
combo
Historical Keytruda
monotherapy ORR in first line
treatment** Low (<1%) 3 (23%) 32% 1 33% 14%
Medium (1-49%) 6 (46%) 44% 3 50% 19%
High (≥50%) 4 (31%) 25% 3 75% 47%
Not evaluable 4
1 25% N/A
Overall 17
8 47% 25%
Source: Immutep, Taylor Collison research. Note: # Garon et al 2015 (Keynote-001) Supplementary Table S9; *Includes
unconfirmed responses; ** Garon et al 2015, Supplementary Table S8 - ORR (overall response rate) includes only confirmed
responses.
NSCLC represents a substantial market opportunity. Lung cancer is the leading cause of cancer death in the US, making up
22% of all cancer deaths, and is expected to account for ~229,000 new cases and 136,000 deaths in 2020. NSCLC makes up
approximately 85% of lung cancers.
4 Garon et al, 2015. Pembrolizumab for the Treatment of Non–Small-Cell Lung Cancer. N Engl J Med; 372:2018-2028
0 8 16 24 32 40 48
-100
-80
-60
-40
-20
0
20
40
60
80
100
weeks
% c
ha
ng
e c
om
pare
d t
o s
tart
of
thera
py
n =17
< 1 %
PD-L1
>=50%
1-49 %
Part A* - 1st line NSCLC
* cut-off 31-Jan 2020
NE

TAYLOR COLLISON LTD. www.taylorcollison.com.au
ABN 53008172450 AFSL 247083 9
Immutep (IMM)
22 April 2020
While ICI drugs such as Keytruda and Opdivo have transformed the treatment of lung cancer recent years there is an urgent
need to improve response rates and patient outcomes. For example, Keytruda as a single agent is approved for treating newly
diagnosed (first line) NSCLC with expression levels of the PD-L1 tumour biomarker of at least 1%, but the response rate in this
patient population in the pivotal Phase III study was only 27%. Keytruda is also approved for use in combination with
chemotherapy in first line NSCLC patients regardless of PD-L1 expression therapies; the response rates in this setting ranged
from 45% to 58% in different NSCLC subtypes.
We see two Key opportunities for efti combo therapies in NSCLC. The first opportunity is for an ICI/efti combo that generates
higher response rates than ICI single agent but without the unpleasant side effects of chemotherapy. The second key
opportunity in our view is as an ICI/chemo/efti triple combo where it has the potential to generate a meaningful increase in
response rates without adding to the side effect burden for patients.
Head and neck cancer response rate already 33% with more patients to come
Part C of the TATCTI-002 study, in second-line HNSCC patients who are PD-1/L1 naive, has already surpassed the threshold
response rate in the initial cohort, with 6 of the 18 subjects (33%) achieving a partial response as of the data cut-off point on 31
January, as shown in Exhibit 9. The 6 responders reported to date is well above then minimum of 3 responders required for
cohort expansion. Importantly, at that point 3 of the subjects had been on treatment for less than 9 weeks and had not yet
undergone an initial response assessment, so there is scope for the response rate to go higher when the additional 3 patients
are scanned.
In Merck’s Keynote-012 study of Keytruda monotherapy in second-line recurrent or metastatic HNSCC the confirmed ORR was
reported as 16% (n=174) in the Keytruda prescribing information, and in a subsequent publication as 18% among 192 patients
at long-term follow-up (Mehra et al 2018).5 Even bearing in mind the caveat that some of the responses reported by Immutep
from part C have not yet been confirmed at a repeat scan, the 33% response rate reported for HNSCC following efti/Keytruda
combo therapy is approximately double the response rate reported for a similar patient population following treatment with
Keytruda alone.
Exhibit 9: Waterfall plot patient tumour responses in second line head and neck cancer in TACTI-002
Source: Immutep.
Earlier TACTI-mel combo study reported similar increases in response rates in melanoma
Immutep had previously investigated efti/Keytruda combination therapy in melanoma patients in the TACTI-mel study. As this
was the first time efti had been administered in combination with a checkpoint inhibitor in humans, in Part A of the study efti
therapy commenced 12 weeks after administration of Keytruda began. This allowed patients to be monitored for adverse events
that coincided with efti therapy. Subjects were injected with 1, 6 and 30 mg of efti every 2 weeks, starting with the fifth cycle of
Keytruda. Subjects were assessed after 3 cycles of Keytruda monotherapy and only subjects who had a suboptimal response to
initial treatment with Keytruda were enrolled into the combination therapy study.
5 Mehra et al, 2018. British Journal of Cancer 119:153–159
ES1308ES1101ES1113UK2102ES1306US3103ES1110ES1407AU0101ES1116ES1111UK2203ES1203
-100
-75
-50
-25
0
25
50
75
100
be
st
% c
ha
ng
e f
rom
ba
se
lin
e iPD
iPR
Best response:
n = 13
Part C* - 2nd line HNSCC
* cut-off 31-Jan 2020
iSD

TAYLOR COLLISON LTD. www.taylorcollison.com.au
ABN 53008172450 AFSL 247083 10
Immutep (IMM)
22 April 2020
The response rate measured from the start of efti/Keytruda combo therapy (at the start of the fifth cycle of Keytruda therapy)
was 33% (6 out of 18 subjects). An exploratory analysis showed that the response rate measured from the first day of Keytruda
therapy was 61% (11 out of 18). However, the design of TACTI-mel Part A meant that the results could not be directly compared
to previous Keytruda monotherapy studies in melanoma patients.
In Part B of the TACTI-mel study subjects were administered with 30 mg of efti by subcutaneous injection every 2 weeks,
starting with the first cycle of Keytruda. The confirmed overall response rate was 50% (3/6), which confirms favourably to the
33% response rate in pivotal studies of Keytruda monotherapy in melanoma patients.
Management has indicated that approximately 22 subjects commenced Keytruda monotherapy during TACTI-mel Part A. Based
on this, we estimate that the response rate among all participants in TACT-mel Part A was also approximately 50% (11 out of
approximately 22 participants).
Efti had a favourable safety profile, with no dose limiting toxicities and no new safety signals observed.
Exhibit 10: Spider plot of tumour responses in TACTI-mel Part B
Source: Immutep. Note: Responses are evaluated according to irRC criteria, rather than irRECIST; irPD= progressive disease; irSD= stable disease; irPR= partial response
Multiple studies indicate that efti combination therapy delivers higher response rates
While indirect comparisons between clinical trials should always be treated with caution, response rates reported for immuno-
oncology studies tend to fall within a much narrower range than the response rates from studies of chemotherapy agents. This
gives us more confidence that the high response rates following efti/Keytruda combo therapy in melanoma, lung and head and
neck cancers are likely to be due to activation of the immune response by efti and are unlikely to be chance observations.
Furthermore, we believe the fact that the response rate following efti/chemo combo therapy in the AIPAC breast cancer study
was 10% higher than the response rate to chemo alone (48% vs 38%), also points to efti being an active anticancer agent. Even
though the difference in response rates was probably not statistically significant, it represents evidence of activity from a
randomised controlled study, rather than relying on cross trial comparisons.
Taking all of this evidence together, we believe that combining efti with an ICI such as Keytruda is likely to lead to a real and
reproducible increase in tumour response rates. Given the responses seen so far in TACTI-002 have been long lasting, we
expect the increased response rates to translate into improved patient survival. If subsequent studies confirm this belief, the
convenient subcutaneous administration and favourable side effect profile could potentially see efti combo therapy used in a
wide range of different cancer types, opening up a very large addressable market.
By year-end the efti data set could be comparable to Viralytics at the time of the A$500m Merck deal
Immutep currently has response data on almost 60 patients who have been treated with efti plus Keytruda in TACTI-mel and the
first two cohorts of TACTI-002. A further 27 subjects have already been recruited in TACTI-002 cohorts for which no response
data has been reported yet. TACTI-002 is currently planned to recruit at least 96 subjects, and a total of 109 subjects if TACTI-
002 Part B in PD1 refractory lung cancer proceeds to recruit the expansion cohort.
The ongoing investigator-initiated Insight study could also report additional data on efti in combination with Merck KGaA and
Pfizer’s checkpoint inhibitor Bavencio (avelumab), which would add to the data set.
0 8 16 24 32 40 48 56 64 72 80
-100
-75
-50
-25
0
25
50
75
100
125
weeks
% c
ha
ng
e c
om
pa
red
to
ba
se
lin
e
start of
therapy
n =6
irPD
Best response:
irSD
irPR
continues

TAYLOR COLLISON LTD. www.taylorcollison.com.au
ABN 53008172450 AFSL 247083 11
Immutep (IMM)
22 April 2020
If recruitment in the studies is able to continue despite the Covid-19 pandemic, then by the end of the year Immutep could have
data on over 100 patients treated with efti/Keytruda combo therapy.
This would give Immutep a similar amount of data on patients treated with checkpoint inhibitor combination therapy to the data
set that Viralytics had when it was acquired by Merck for ~A$500m in early 2018. The acquisition price was at a 160% premium
to the one-month VWAP of Viralytics shares.
Furthermore, we note that the response rates when efti is added to Keytruda is comparable to the efficacy of Cavatak plus
Keytruda. While the 59% (16/27) response rate following intralesional injection of Cavatak was higher than the ~50% ORR for
efti plus Keytruda in melanoma, the response rate following iv Cavatak plus Keytruda in second and third line NSCLC (31%,
5/16) was considerably lower than the 47% response rate (8/17) reported for efti plus Keytruda in first line NSCLC patients. In
metastatic bladder cancer the response rate following iv Cavatak plus Keytruda was not much higher than the response rate in
pivotal studies of Keytruda monotherapy (28% vs a 21%).
It is important to note that the convenient subcutaneous injections are used to administer efti for all of the different types of
cancer, whereas the highest response rates to Cavatak required direct injection into the tumour, a delivery method that is quite
cumbersome for most types of cancer. Response rates to Cavatak were lower when the intravenous delivery route was used.
Overall, the efficacy of efti plus Keytruda appears to be comparable to Cavatak plus Keytruda, although the efti combo may be
more efficacious than intravenous Cavatak.
We believe efti could attract a similar deal to Viralytics, but Epacadostat failure creates uncertainty
We believe that there are two key unanswered questions for investors about efti/checkpoint inhibitor combination therapy.
1. Will efti combo continue to deliver high response rates in the ongoing study?
2. Would Immutep be able to do a Viralytics style deal on the back of continued high response rates in TACTI-002.
The first point reflects the ongoing clinical trial risk that applies to all drug development programs, and cannot be avoided, but
the results so far are very encouraging, in our view.
On the second point, we believe that the failure of a once-promising immuno-oncology combination therapy a few months after
the Viralytics deal has dented investor confidence that high response rates in single arm studies will translate into efficacy in a
randomised controlled study. In April 2018 the Keynote-252 Phase III study showed that the addition of the IDO1 inhibitor
epacadostat (Incyte; NASDAQ: INCY) to Keytruda therapy failed to stop cancer progression in first-line melanoma patients,
compared with Keytruda alone. The overall response rate for patients treated with epacadostat plus Keytruda was almost the
same as that for Keytruda alone (34% vs 32%). The low response rate in the Phase III study was marked contrast to a previous
Phase I/II study where 56% of the 54 melanoma patients treated with the epacadostat/Keytruda combo achieved an objective
response. A single arm study of epacadostat combined with a different checkpoint inhibitor, Opdivo, in melanoma patients also
reported a high response rate (65%).
The lack of efficacy of epacadostat when added to Keytruda was confirmed in two subsequent randomised studies in lung
cancer, which showed that adding epacadostat resulted in lower response rates compared to Keytruda alone. In the Phase II
Keynote-654-05 study, in lung cancer patients with high expression of the PD-L1 biomarker, the overall response rate in patients
receiving the epacadostat/Keytruda combo was 33% vs 39% in patients given Keytruda plus placebo. Similarly, in the Keynote-
715-06 study the response rate in the Keytruda/chemo/epacadostat arm was 26% vs 45% for Keytruda/chemo/placebo treated
patients.
We don’t believe that the failure of epacadostat has a negative readthrough for efti. Firstly, IDO1 inhibitors like epacadostat act
in a different part of the immune system to efti. IDO1 inhibitors act on T cells which kill cancer cells, as do the anti-PD-1/L1
checkpoint inhibitors. In contrast, efti activates antigen presenting cells which are key actors in recognising tumour antigens and
triggers the initial steps of the immune response.
Secondly, given that there was a 10% difference in response rates in favour of the efti/chemo combo in the randomised AIPAC
study, it seems unlikely that efti would suffer the same fate as epacadostat and fail to show any benefit when added to
checkpoint inhibitor therapy in a randomised study. However, what future trials will need to determine is whether the benefit
would be large enough to make the combo and effective therapy with broad uptake in the clinic.
Another factor that may influence the prospects for attracting a pharma partner is that a large number of other therapies are
being investigated for efficacy in combination with checkpoint inhibitors. Other immuno-oncology agents which aim to enhance
anti-tumour immune responses include compounds targeting the STING (STimulator of INterferon Genes), TLR9 (Toll-like
Receptor 9), IL-12 (interleukin 12), TIGIT (T-cell immunoglobulin and ITIM domains) and PIN-2 pathways, as well as anti-LAG-3
checkpoint inhibitor antibodies. In addition to these combinations of two immuno-oncology agents, checkpoint inhibitors are also
being combined with chemotherapy and targeted therapies such as BRAF and MEK inhibitors. EvaluatePharma reported that
there were 765 ICI combo studies underway in 2017, and the number is likely to have grown since then.

TAYLOR COLLISON LTD. www.taylorcollison.com.au
ABN 53008172450 AFSL 247083 12
Immutep (IMM)
22 April 2020
Despite this competition, we believe that the high response rates reported for the efti/Keytruda combo in a range of cancer
types, its favourable side effect profile and the convenient subcutaneous route of administration mean that it is well placed to
attract interest from big pharma. We believe that there is a realistic prospect that IMM could achieve a significant licence deal or
M&A transaction in the next 12-18 months if efti continues to generate high response rates in the TACT-002 study. We do not
believe that the potential for a significant transaction in the next 12-18 months is reflected in the current share price, and
therefore that IMM represents an attractive opportunity for investors.
Programs partnered with big pharma have progressed to mid-stage trials
On top of the in-house efti program, Immutep has two additional LAG-3 programmes that that are partnered with big pharma
and could create significant value, both of which have already progressed to Phase II (mid-stage) trials. These programmes are
partnered with Novartis (anti-LAG-3 antibody in cancer) and GSK (LAG-3 depleting antibody in inflammatory disorders).
Novartis: Five LAG525 combo studies underway
LAG525 is an antibody which blocks the LAG-3-mediated inhibitory signal given to tumour-infiltrating T-cells and thus activates
T-cell proliferation and enhances the anti-tumour activity of anti-PD-1 ICI drugs. LAG525 is Novartis’s humanised version of
IMP701, which it in-licensed from Immutep. The total milestones and royalties payable to Immutep under the global license
agreement with Novartis have not been disclosed.
Novartis has five Phase I/II or Phase II studies of LAG525 underway. In each of these studies, LAG525 is combined with
Novartis’s in-development anti-PD-1 antibody PDR001 (also known as spartalizumab).
The original Phase I/II study of LAG525 as a single agent and in combination with PDR001 that commenced in June 2015, has
enrolled 490 subjects and is expected to reach final completion in July this year (Clinical trials.gov: NCT02460224; Novartis
protocol LAG525X2101C). The Phase II component of the study comprised cohorts with NSCLC, melanoma, renal cancer,
mesothelioma and triple-negative breast cancer (TNBC) who are being treated with LAG525 plus PDR001.
A second Phase II study of LAG525 plus PDR001 commenced in January 2018 (NCT03365791; Novartis protocol
CPDR001XUS01). This adaptive, open label Phase II study enrolled 76 patients with solid or haematological cancers including
small cell lung cancer, gastric/oesophageal, prostate, ovarian cancers or diffuse large B-cell lymphoma. Study completion is
expected in October 2020.
Novartis is conducting a randomised Phase II study in TNBC patients in which LAG525 is being combined with either PDR001
or carboplatin chemotherapy, or with both PDR001 and carboplatin (NCT03499899). The trial, which commenced in July 2018,
recruited 88 patients. Collection of top-line ORR data was completed in February 2020, and final study completion is expected in
January 2021.
LAG525 is one of four drugs being randomly assigned for use in combination with PDR001 in 230 patients with advanced
melanoma in the PLATforM Phase II study (NCT03484923). The study, which commenced in September 2018, was originally
intended to recruit 135 subjects, but was expanded to 230 subjects in April 2019. Final topline data is expected to be collected
in June 2021.
Lastly, Novartis has also initiated an open label triple combo Phase Ib study in TNBC patients in which LAG525 plus PRD001
will be combined with either the drugs NIR178 or capmatinib or the biologicals MCS110 or canakinumab (NCT03742349). The
trial, which commenced in January 2019, will recruit up to 220 patients. The expected primary completion date is January 2022.
Novartis Phase II supported by efficacy signals in combo Phase I/II and Phase II studies
Novartis reported6 encouraging signs of efficacy from the LAG525 in combination with PDR001 from the Phase I component of
its ongoing Phase I/II study (NCT02460224) in 2018. Among 121 patients with solid tumours treated with LAG525 plus PDR001
at a wide range of doses there were 13 durable responses, including 3/87 mesothelioma patients and 2/5 TNBC patients. In
TNBC tumour biopsies, there was a trend to conversion from immune-cold to immune-activated biomarker profiles. No
responses were observed in 134 patients treated with LAG525 alone.
Novartis presented preliminary data on the NCT03365791 Phase II study at ASCO in 2019. Efficacy was assessed based on the
clinical benefit rate (CBR) which comprises either a tumour response or stable disease. Three cancers, small cell lung cancer;
neuroendocrine tumours (NETs) and diffuse large B-cell lymphoma (DLBCL), entered the cohort expansion phase having met
the CBR target threshold. The CBR reported for the 3 cancers were 27%, 86% and 43%, respectively. Assessment in three
cancers which had not met the expansion thresholds was ongoing (prostate and ovarian cancer and soft tissue sarcoma), while
the gastroesophageal cancer cohort was stopped for futility.
6 Hong et al 2018. http://novartis.medicalcongressposters.com/Default.aspx?doc=e07a1 7 3/8 includes an additional partial response after the data cut-off date for the conference abstract.

TAYLOR COLLISON LTD. www.taylorcollison.com.au
ABN 53008172450 AFSL 247083 13
Immutep (IMM)
22 April 2020
GSK is conducting a Phase II study of GSK’781 in ulcerative colitis
GSK’781 (GSK2831781), which is based on the IMP731 antibody that GSK in-licensed from Immutep in 2011, is an anti-LAG-3
depleting antibody that will kill the few LAG-3 positive activated T-cells that infiltrate autoimmune disease sites. The licence deal
involved potential milestone payments pf approximately GBP64m (~A$125m) plus undisclosed royalties payable to Immutep.
According to the clinicaltrials.gov registry entry (NCT03893565), GSK started a Phase II study of GSK’781 in May 2019. The
study will investigate the safety, tolerability, efficacy and dose response of GSK’781 in up to 280 subjects with moderate to
severe ulcerative colitis. The estimated primary completion date is April 2022.
Ulcerative colitis is a type of inflammatory bowel disease. Ulcerative colitis and Crohn’s disease are the most common types of
inflammatory bowel diseases. The US Centers for Disease Control and Prevention estimates that the prevalence of ulcerative
colitis is 0.24% of the population, which is equivalent to 780,000 patients in the US.
The key drugs for ulcerative colitis are Humira (adalimumab), Entyvio (vedolizumab), Remicade (infliximab) and Simponi
(golimumab). Allied Market Research forecasts the global ulcerative colitis market to grow to US$7.5bn by 2023.
GSK completed a Phase I study of GSK’781 in psoriasis patients in March 2018. We believe that the Phase I study was
conducted in psoriasis patients because it is easy to assess responses to treatment in psoriasis skin lesions, and because it is
convenient to collect tissue biopsy samples from the skin lesions in order to assess the impact of the treatment on inflammatory
markers in the tissue. We suspect that ulcerative colitis as the lead indication for GSK’781 because it represents a larger
commercial opportunity than psoriasis.
IMP761 LAG-3 a potential treatment for autoimmune diseases
Immutep’s novel LAG-3 agonist IMP761 inhibited immune responses, including infiltration by inflammatory lymphocytes, in a
non-human primate study. This proof-of-concept (PoC) study confirmed that IMP761 has potential as a treatment for
inflammatory autoimmune disorders.
The company’s manufacturing partner for IMP761 has developed a high-yielding cell line as it prepares for the manufacture of
GMP-grade IMP761 product for use in clinical studies.
IMP761 is the first known therapeutic antibody with agonist properties that enable it to activate the LAG-3 receptor on the
surface of activated T cells, and thereby down-regulate T cell activation and proliferation. In contrast, LAG525 and the other
known anti-cancer LAG-3 antibodies are antagonist antibodies that block LAG-3 signalling and thereby prevent the down-
regulation of T cell immune responses.
The mechanism of action of IMP761 is also different to the company’s partnered GSK’781 cytotoxic mAb, which aims to treat
autoimmune disease by killing LAG-3-positive T cells. IMP761 offers the opportunity to fine-tune immune responses, which
could benefit sufferers of autoimmune diseases by temporarily switching off activated LAG-3-positive T cells that are damaging
tissue or causing inflammation.
Valuation
We initiate coverage of Immutep with a valuation of $327 or 83c per share (undiluted), based on a risk-adjusted discounted cash
flow model. On a fully diluted basis, our valuation is 53c per share, after taking into account the options, warrants and
convertible notes on issue, and a $30m capital raise that we model in FY21. Exhibit 11 summarises the constituent parts of our
valuation, which is based on a discount rate of 12.5%.
We forecast the company’s gross cash balance at end FY20 to be $13.0m. For valuation purposes we deduct the $13.75m face
value of the Ridgeback Capital convertible note in calculating end-FY20e net debt of ($0.8m) as shown in Exhibit 11. We note
that this is different to the accounting treatment of the convertible note, which includes only the A$7.6m estimated fair value of
the convertible note as a non-current liability, with the remainder treated as equity.
We model Immutep outlicensing efti at the completion of the TACTI-002 study in a deal that includes an upfront payment of
US$85m and US$540m of milestone payments. We model a licencing deal being finalized in FY22, although we see a realistic
prospect of a deal in FY21. We assume that 50% (US$270m) of the milestone payments are for the achievement of clinical and
regulatory milestones, with the remaining 50% assumed to be based on sales hurdles. We risk adjust the US$85m upfront and
US$270m clinical and regulatory milestones with a 15-50% probability (50% probability of signing a license deal, 15% for
approval milestones). We do not include any potential sales-based milestones in our forecasts, and instead model a 15% royalty
rate. The modelled deal terms are based on relevant benchmarks over the last few years (sourced from EvaluatePharma and a
report produced by the industry group BIO).
Exhibit 11 shows our key assumptions for each product included in the valuation and the rNPV for each product. We have offset
the risk-adjusted trial cost of a potential Phase IIb study of efti against potential efti milestone revenue.

TAYLOR COLLISON LTD. www.taylorcollison.com.au
ABN 53008172450 AFSL 247083 14
Immutep (IMM)
22 April 2020
Exhibit 11: Immutep risk-adjusted DCF base case valuation and assumptions
Value driver Base case success
likelihood (%)
rNPV ($m)
rNPV/ share ($)
Assumptions
efti+anti-PD1 ICI NSCLC 15% 96.5 $0.25 Global peak sales of US$2.1bn. We assume 121,270 NSCLC deaths in the US each year, 75% eligible for therapy, 15% penetration; pricing US$60k per patient; global sales double US sales; launch 2027; 15% net royalty.
efti+anti-PD1 ICI head and neck
15% 46.4 $0.12 Global peak sales of US1.0bn. We assume 65,630 new cases; 10% penetration; pricing US$60k per patient; global sales double US sales; launch 2027; 15% net royalty
efti+anti-PD1 ICI melanoma 15% 11.4 $0.03 Global peak sales of US$120m. We assume 100,350 new cases;16% advanced or metastatic (Stage III&IV); 10% penetration; pricing US$60k per patient; global sales double US sales; launch 2027; 15% net royalty
efti+chemo breast cancer 2% 6.8 $0.02 Global peak sales of US$1.1bn. We assume 276,480 new cases; 65% HR positive, HER2 negative. 40% advanced or metastatic; 15% penetration; pricing US$60k per patient; global sales double US sales; launch 2027; 15% net royalty. We assume a 2% success probability as OS data is still pending.
efti milestones – assume partnered post TACTI-002
15-50% 80.5 $0.21 R&D cost: Assumes A$30m for randomised Phase IIb study if licence deal is delayed beyond FY22
LAG525 solid tumours (lung cancer)
20% 54.7 $0.14 NSCLC as indicative indication. Global peak sales of US$2.1bn. We assume 121,270 NSCLC deaths in the US each year, 75% eligible for therapy, 15% penetration; pricing US$60k per patient; global sales double US sales; launch 2027; 5% net royalty
GSK’781- autoimmune disease (ulcerative colitis)
20% 54.9 $0.14 Global peak sales of US$1.1bn – 15% share of US$7.5bn global market; launch 2027; 8% net royalty. GBP55m of total GBP64m potential milestones from GSK (risk adjusted to GBP17m)
SG&A to 2024 -23.8 -$0.06
Portfolio total 327.4 $0.84
Cash end FY20e (incl. conv. note at face value)
-0.8 $0.00
Enterprise total 326.7 $0.83
Source: Taylor Collison research. Note: NPV adjusted for tax at an effective tax rate of 20%. We assume that the addressable markets grow at 2% per year.
Potential dilution
We note that Viralytics raised ~$30m in a placement to fund a pivotal study of Cavatak December 2017, approximately two
months before the Merck transaction was announced. We model IMM similarly raising $30m in FY21 so that it would be in a
position to proceed with a randomised Phase IIb study of efti plus a checkpoint inhibitor if it does not reach agreement with a
pharma partner. Viralytics had ~$22m cash at the time the placement was announced.
Exhibit 12 shows that in addition to the 391.6m Immutep shares in issue, there are a further 345.3m potential shares that could
be issued in the assumed FY21 placement and on the exercise of options, warrants, performance rights and convertible notes,
all of which would be in the money at our 83c per share undiluted valuation. Exhibit 12 shows that after taking into account
these potential shares, our diluted valuation is 53c per share.

TAYLOR COLLISON LTD. www.taylorcollison.com.au
ABN 53008172450 AFSL 247083 15
Immutep (IMM)
22 April 2020
Exhibit 12: Potential further dilution and value per share
Average exercise price (A$) m
Current number of shares
391.6
Ridgeback convertible note potential shares 0.200 68.8
Ridgeback warrants* 0.235 38.0
2017, 2018 placement warrants 0.385 36.3
Other warrants 0.472 0.2
Performance rights** 0.000 14.5
A$30m placement @ 16c in FY21 0.160 187.5
Total potential new shares 345.3
Total potential diluted number of shares 736.9
Net cash from placement and options exercise (A$m) $51.2
Debt expunged on Conv note conversion (A$m) $13.8
Valuation (above plus additional cash)
$391.6
Diluted value per share
$0.53
Source: Taylor Collison research. Note: *3.63m ADS warrants converted to ordinary shares at the long-term exchange rate.
**Both vested and unvested performance rights have been included.
We include risk-adjusted milestones payable by current partners GSK for GSK’781 and Novartis for LAG525, plus milestones
from prospective deals for efti. The breadth of the LAG-3 pipeline means there could be further upside if Immutep or its partners
launch additional products into the clinic or broaden the indications being studied.
Risks
Immutep is subject to clinical trial, regulatory and commercialisation risks common to all biotech companies. The key sensitivity
is clinical progress of its pipeline of LAG-3 candidates, primarily the internally funded efti. While Immutep has funds to complete
the Phase I/II TACTI-002 study of efti in combination with Keytruda, it would require a partnership or alternative forms of funding
to advance efti/checkpoint inhibitor comb therapy into randomised studies (we model a $30m capital raise to fund this). Existing
partnerships with big pharma reduce the financial and execution risk for LAG525 and GSK’781; in addition, if the proof of
concept study of GSK’781 in ulcerative colitis reveals evidence of efficacy, it could lead GSK to extend the study to additional
indications including rheumatoid arthritis, psoriasis and multiple sclerosis, which could increase the potential peak sales and
therefore the value of the product. The Covid19 pandemic is likely to slow down recruitment in clinical trials, especially in
countries such as the UK and Spain. TACTI-002 has already recruited 70% of the total patients and INSIGHT has recruited 91%
of the total.

TAYLOR COLLISON LTD. www.taylorcollison.com.au
ABN 53008172450 AFSL 247083 16
Immutep (IMM)
22 April 2020
Disclaimer
The following Warning, Disclaimer and Disclosure relate to all material presented in this document and should be read before making any investment decision.
Warning (General Advice Only): Past performance is not a reliable indicator of future performance. This report is a private communication to clients and intending clients and is not intended for public circulation or publication or for the use of any third party, without the approval of Taylor Collison Limited ABN 53 008 172 450 (“Taylor Collison”), an Australian Financial Services Licensee and Participant of the ASX Group. TC Corporate Pty Ltd ABN 31 075 963 352 (“TC Corporate”) is a wholly owned subsidiary of Taylor Collison Limited. While the report is based on information from sources that Taylor Collison considers reliable, its accuracy and completeness cannot be guaranteed. This report does not take into account specific investment needs or other considerations, which may be pertinent to individual investors, and for this reason clients should contact Taylor Collison to discuss their individual needs before acting on this report. Those acting upon such information and recommendations without contacting one of our advisors do so entirely at their own risk.
This report may contain “forward-looking statements”. The words “expect”, “should”, “could”, “may”, “predict”, “plan” and other similar expressions are intended to identify forward-looking statements. Indications of and guidance on, future earnings and financial position and performance are also forward-looking statements. Forward-looking statements, opinions and estimates provided in this report are based on assumptions and contingencies which are subject to change without notice, as are statements about market and industry trends, which are based on interpretations of current market conditions.
Any opinions, conclusions, forecasts or recommendations are reasonably held at the time of compilation but are subject to change without notice and Taylor Collison assumes no obligation to update this document after it has been issued. Except for any liability which by law cannot be excluded, Taylor Collison, its directors, employees and agents disclaim all liability (whether in negligence or otherwise) for any error, inaccuracy in, or omission from the information contained in this document or any loss or damage suffered by the recipient or any other person directly or indirectly through relying upon the information.
Disclosure: Analyst remuneration is not linked to the rating outcome. Taylor Collison may solicit business from any company mentioned in this report. For the securities discussed in this report, Taylor Collison may make a market and may sell or buy on a principal basis. Taylor Collison, or any individuals preparing this report, may at any time have a position in any securities or options of any of the issuers in this report and holdings may change during the life of this document.
Analyst Interests: The Analyst holds 123,500 shares in IMM.ASX, but this may change during the life of this document.
Other Staff (including Principal accounts) may hold shares in IMM.ASX, in personal and family related accounts; a Principal account holds 100,000 shares in IMM. These holdings may change during the life of this document.
Analyst Certification: The Analyst certifies that the views expressed in this document accurately reflect their personal, professional opinion about the financial product(s) to which this document refers.
Date Prepared: April 2020
Analyst: Dr Dennis Hulme
Release Authorised by: Campbell Taylor
TAYLOR COLLISON LIMITED
Sharebrokers and Investment Advisors
Established 1928
ADELAIDE
Level 16, 211 Victoria Square
Adelaide SA 5000
GPO Box 2046
Adelaide SA 5001
Telephone 08 8217 3900
Facsimile 08 8321 3506
SYDNEY
Level 10, 151 Macquarie Street
Sydney NSW 2000
GPO Box 4261
Sydney NSW 2001
Telephone 02 9377 1500
Facsimile 02 9232 1677
Participant of the Australian Securities Exchange
(ASX) Group.
ABN 53008172450
AFSL 247083