Embed Size (px)
Citation preview
Immunotherapy in Cancer: turning T cells against cancer
Frederick L. Locke, MDDirector, Immune Cell Therapy Program
Department of Blood and Marrow Transplant – Cellular ImmunotherapyMoffitt Cancer Center
Disclosures
• Consultant: Cellular BioMedicine Group • Scientific Advisory Board Member: Kite Pharma • Other: Moffitt Cancer Center has received research funding from Kite pharma
I will be discussing “off-label” uses of the following FDA approved medications:• Tocilizumab

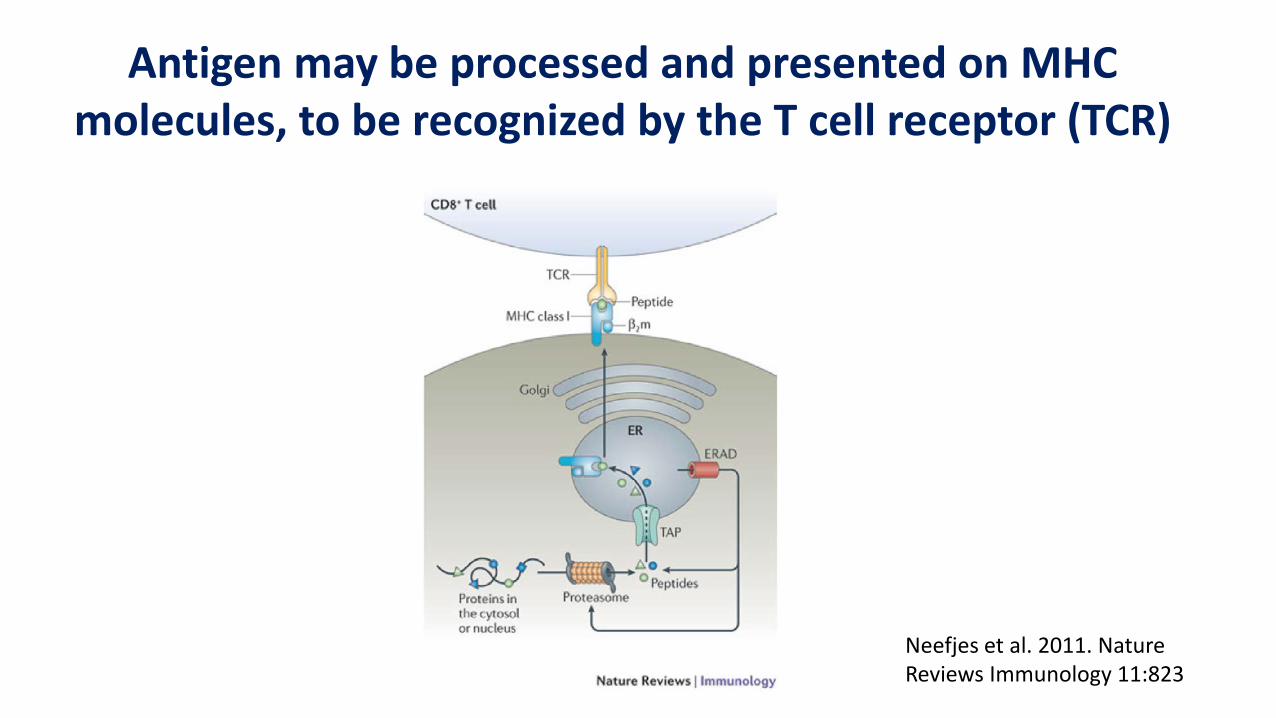
Antigen may be processed and presented on MHC molecules, to be recognized by the T cell receptor (TCR)
Neefjes et al. 2011. Nature Reviews Immunology 11:823
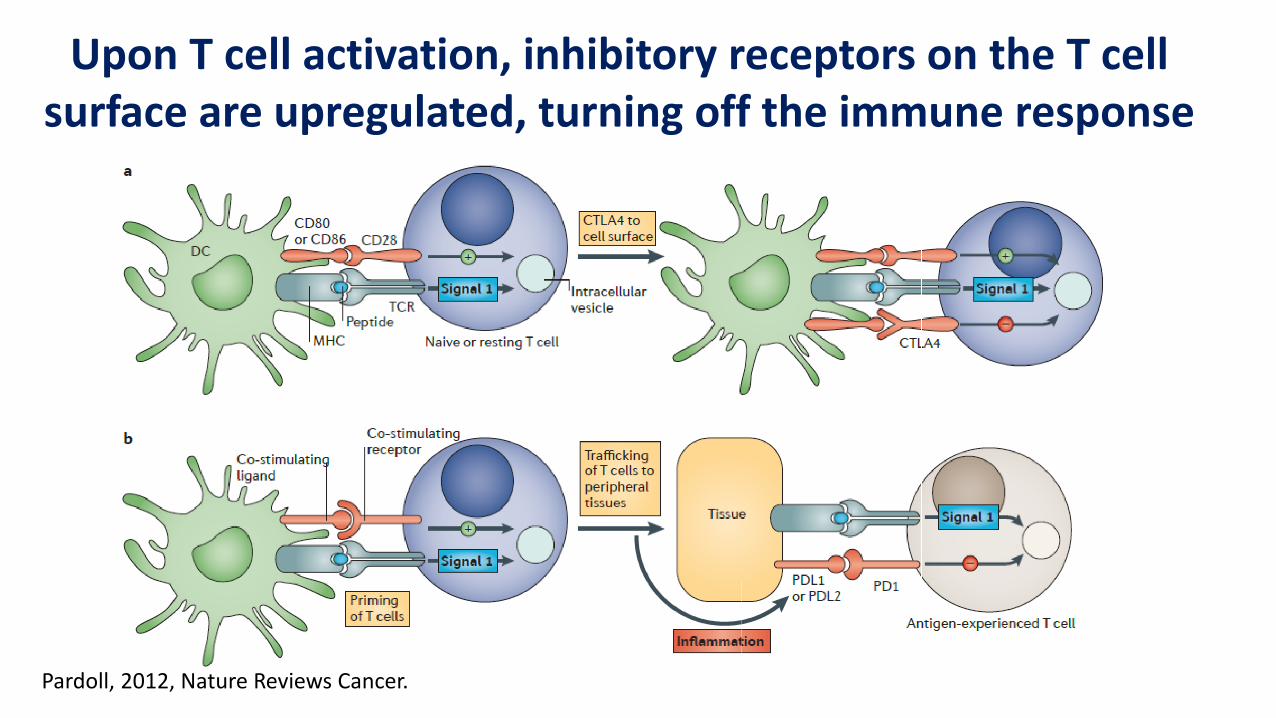
Pardoll, 2012, Nature Reviews Cancer.
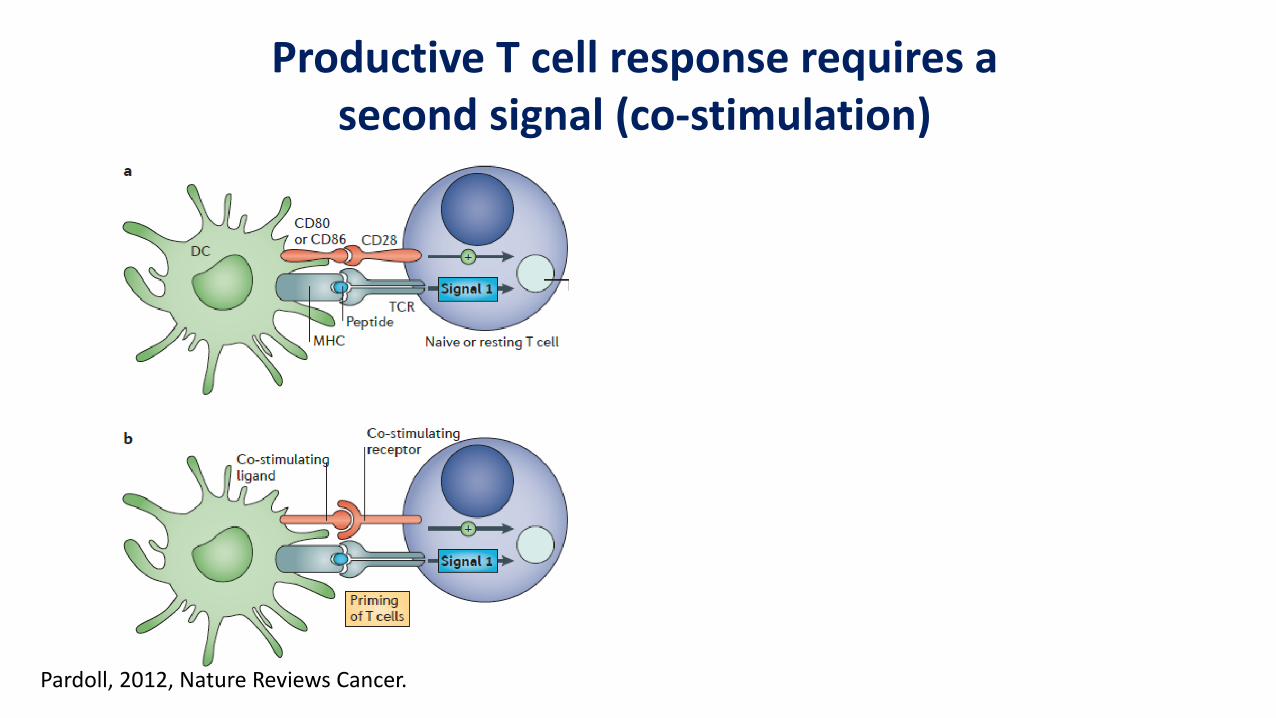
Productive T cell response requires a second signal (co-stimulation)
Pardoll, 2012, Nature Reviews Cancer.
Upon T cell activation, inhibitory receptors on the T cell surface are upregulated, turning off the immune response
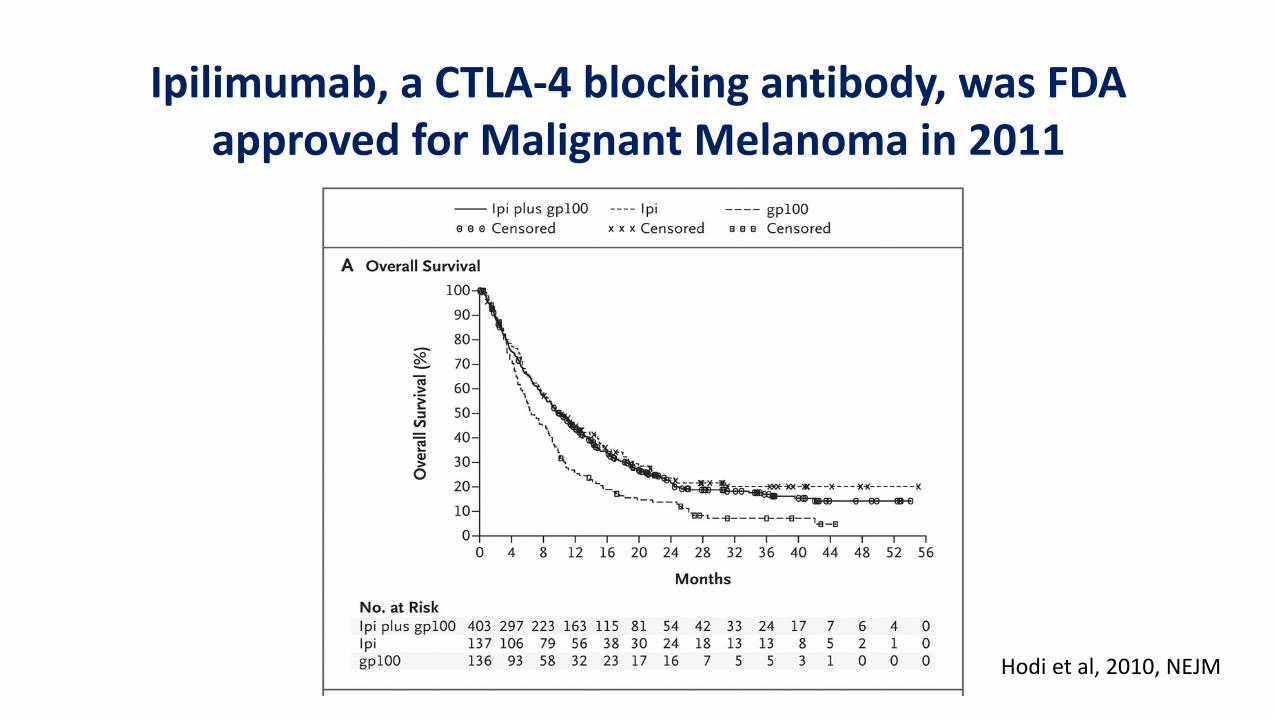
Ipilimumab, a CTLA-4 blocking antibody, was FDA approved for Malignant Melanoma in 2011
Hodi et al, 2010, NEJM
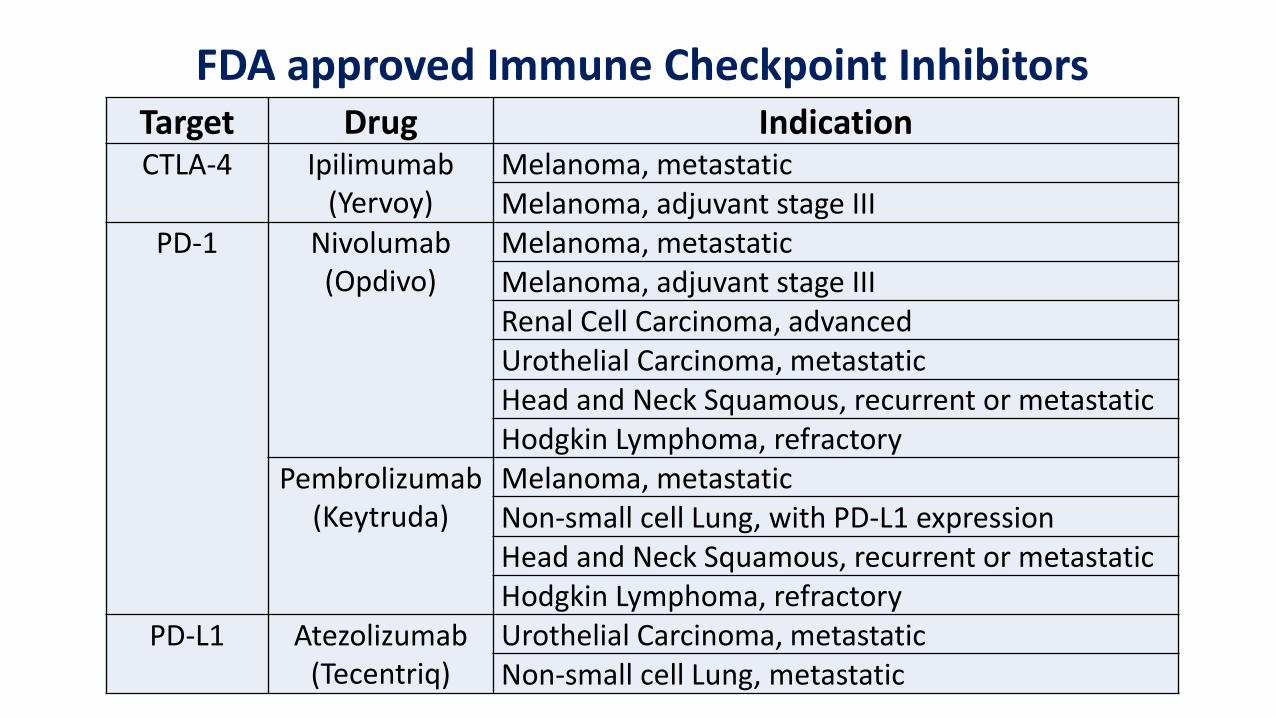
FDA approved Immune Checkpoint InhibitorsTarget Drug IndicationCTLA-4 Ipilimumab
(Yervoy)Melanoma, metastaticMelanoma, adjuvant stage III
PD-1 Nivolumab (Opdivo)
Melanoma, metastaticMelanoma, adjuvant stage IIIRenal Cell Carcinoma, advancedUrothelial Carcinoma, metastaticHead and Neck Squamous, recurrent or metastaticHodgkin Lymphoma, refractory
Pembrolizumab (Keytruda)
Melanoma, metastaticNon-small cell Lung, with PD-L1 expressionHead and Neck Squamous, recurrent or metastaticHodgkin Lymphoma, refractory
PD-L1 Atezolizumab(Tecentriq)
Urothelial Carcinoma, metastaticNon-small cell Lung, metastatic
In Girl’s Last Hope, Altered Immune Cells Beat LeukemiaDec. 9, 2012
New York Times
Chimeric Antigen Receptor (CAR) T cell therapy• Autologous Cellular Immunotherapy
• T cells removed and engineered to express a chimeric antigen receptor (CAR)
• Reprogramed T cells recognize cancer cell targets
• CD19 targeted CARs are furthest in development
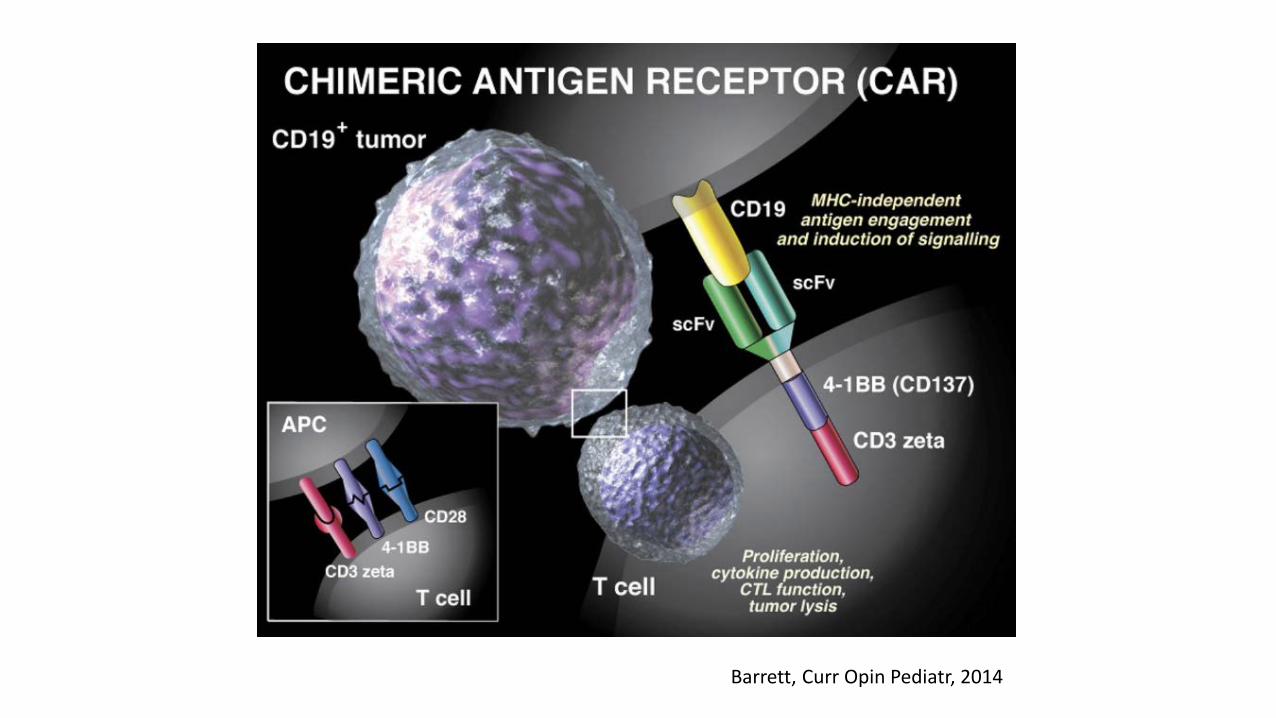
Barrett, Curr Opin Pediatr, 2014
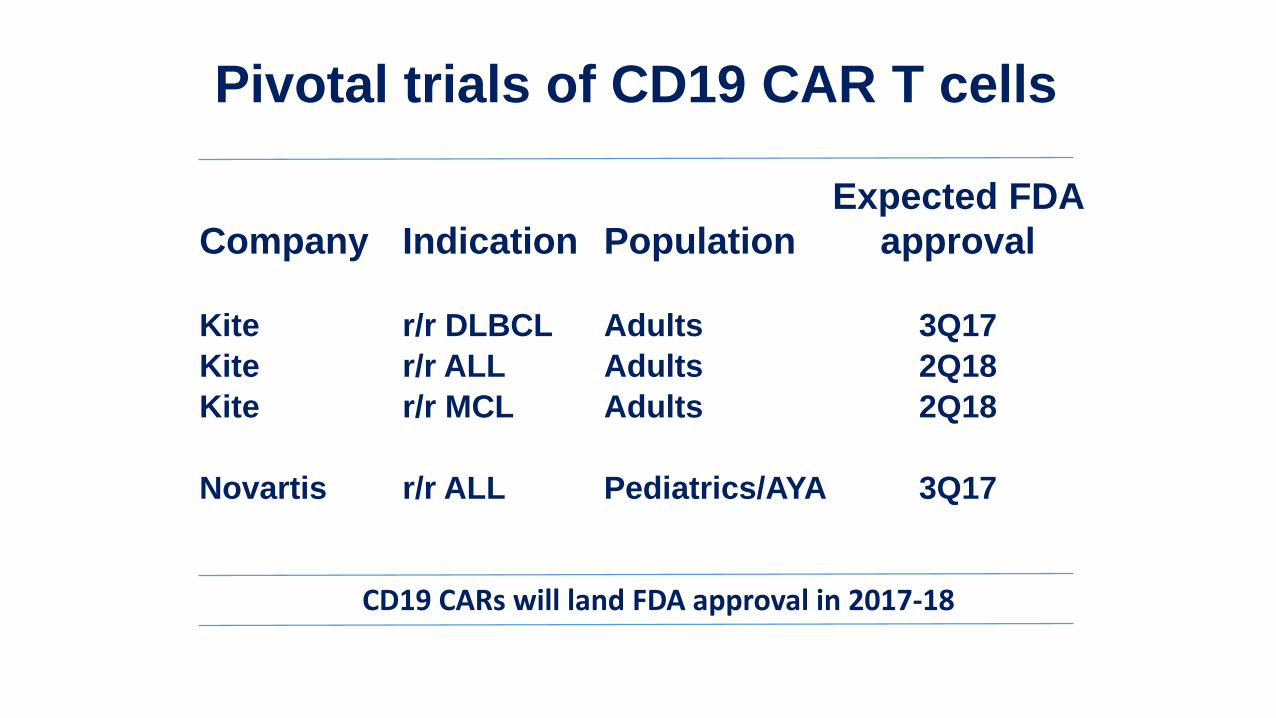
Pivotal trials of CD19 CAR T cells
Company Indication PopulationExpected FDA
approval
Kite r/r DLBCL Adults 3Q17Kite r/r ALL Adults 2Q18Kite r/r MCL Adults 2Q18
Novartis r/r ALL Pediatrics/AYA 3Q17
CD19 CARs will land FDA approval in 2017-18
Locke & Neelapu et al AACR 2017 #9986
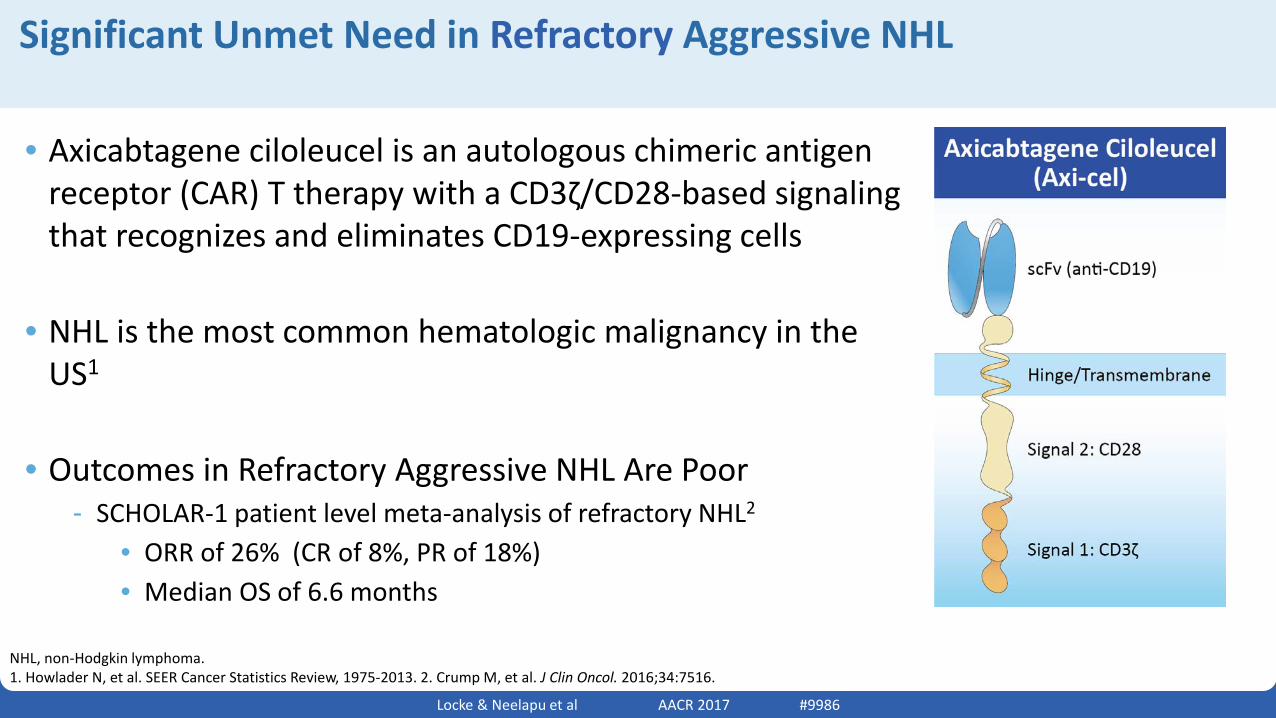
• Axicabtagene ciloleucel is an autologous chimeric antigen receptor (CAR) T therapy with a CD3ζ/CD28-based signaling that recognizes and eliminates CD19-expressing cells
• NHL is the most common hematologic malignancy in the US1
• Outcomes in Refractory Aggressive NHL Are Poor- SCHOLAR-1 patient level meta-analysis of refractory NHL2
• ORR of 26% (CR of 8%, PR of 18%)• Median OS of 6.6 months
Significant Unmet Need in Refractory Aggressive NHL
NHL, non-Hodgkin lymphoma. 1. Howlader N, et al. SEER Cancer Statistics Review, 1975-2013. 2. Crump M, et al. J Clin Oncol. 2016;34:7516.
(anti-CD19)
Locke & Neelapu et al AACR 2017 #9986
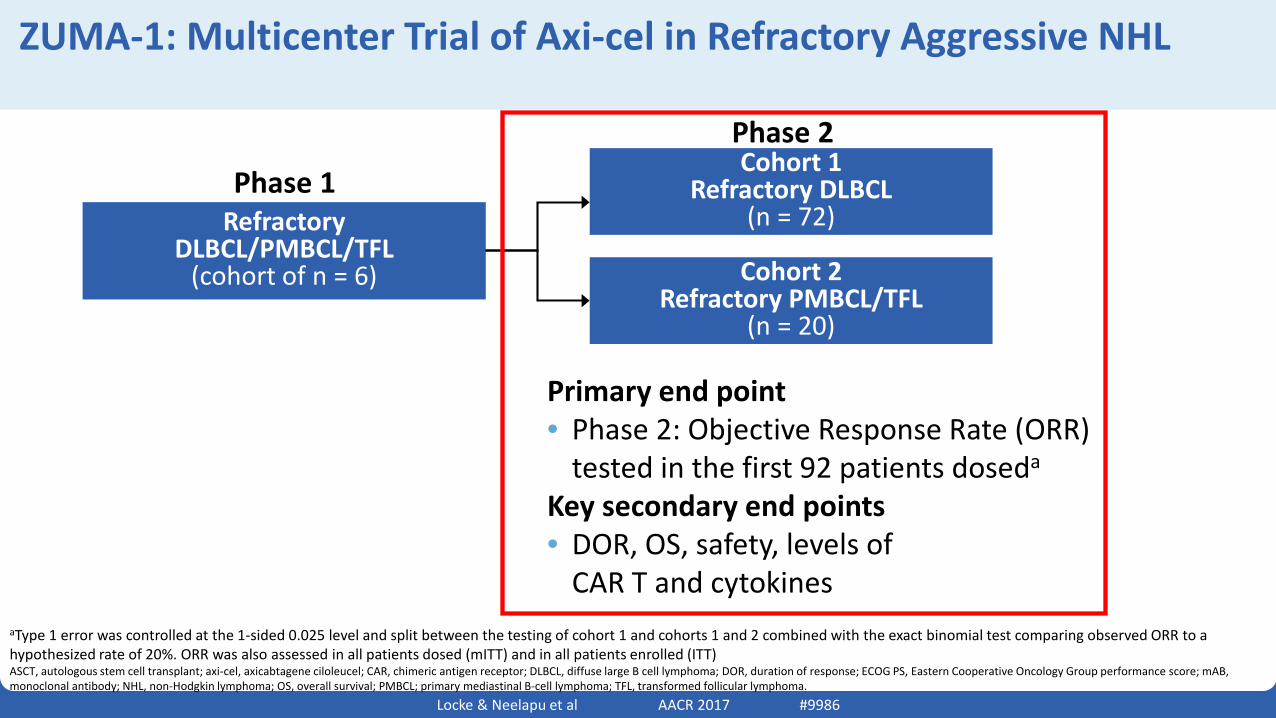
ZUMA-1: Multicenter Trial of Axi-cel in Refractory Aggressive NHL
aType 1 error was controlled at the 1-sided 0.025 level and split between the testing of cohort 1 and cohorts 1 and 2 combined with the exact binomial test comparing observed ORR to a hypothesized rate of 20%. ORR was also assessed in all patients dosed (mITT) and in all patients enrolled (ITT)ASCT, autologous stem cell transplant; axi-cel, axicabtagene ciloleucel; CAR, chimeric antigen receptor; DLBCL, diffuse large B cell lymphoma; DOR, duration of response; ECOG PS, Eastern Cooperative Oncology Group performance score; mAB, monoclonal antibody; NHL, non-Hodgkin lymphoma; OS, overall survival; PMBCL; primary mediastinal B-cell lymphoma; TFL, transformed follicular lymphoma.
RefractoryDLBCL/PMBCL/TFL
(cohort of n = 6)
Cohort 1Refractory DLBCL
(n = 72)
Cohort 2Refractory PMBCL/TFL
(n = 20)
Phase 1Phase 2
Primary end point• Phase 2: Objective Response Rate (ORR)
tested in the first 92 patients doseda
Key secondary end points• DOR, OS, safety, levels of
CAR T and cytokines
Locke & Neelapu et al AACR 2017 #9986
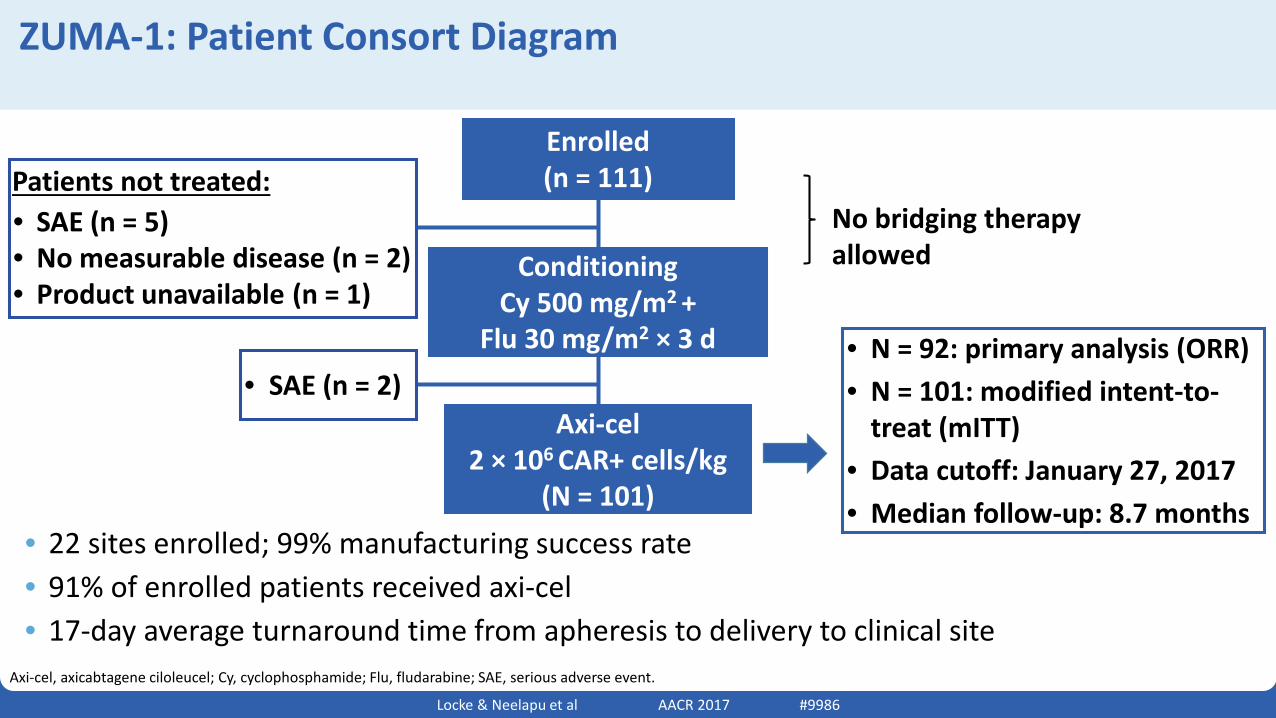
• 22 sites enrolled; 99% manufacturing success rate• 91% of enrolled patients received axi-cel• 17-day average turnaround time from apheresis to delivery to clinical site
ZUMA-1: Patient Consort Diagram
Axi-cel, axicabtagene ciloleucel; Cy, cyclophosphamide; Flu, fludarabine; SAE, serious adverse event.
Enrolled(n = 111)
Axi-cel 2 × 106 CAR+ cells/kg
(N = 101)
• N = 92: primary analysis (ORR)• N = 101: modified intent-to-
treat (mITT)• Data cutoff: January 27, 2017• Median follow-up: 8.7 months
Conditioning Cy 500 mg/m2 +
Flu 30 mg/m2 × 3 d
No bridging therapy allowed
• SAE (n = 5)• No measurable disease (n = 2)• Product unavailable (n = 1)
• SAE (n = 2)
Patients not treated:
Locke & Neelapu et al AACR 2017 #9986
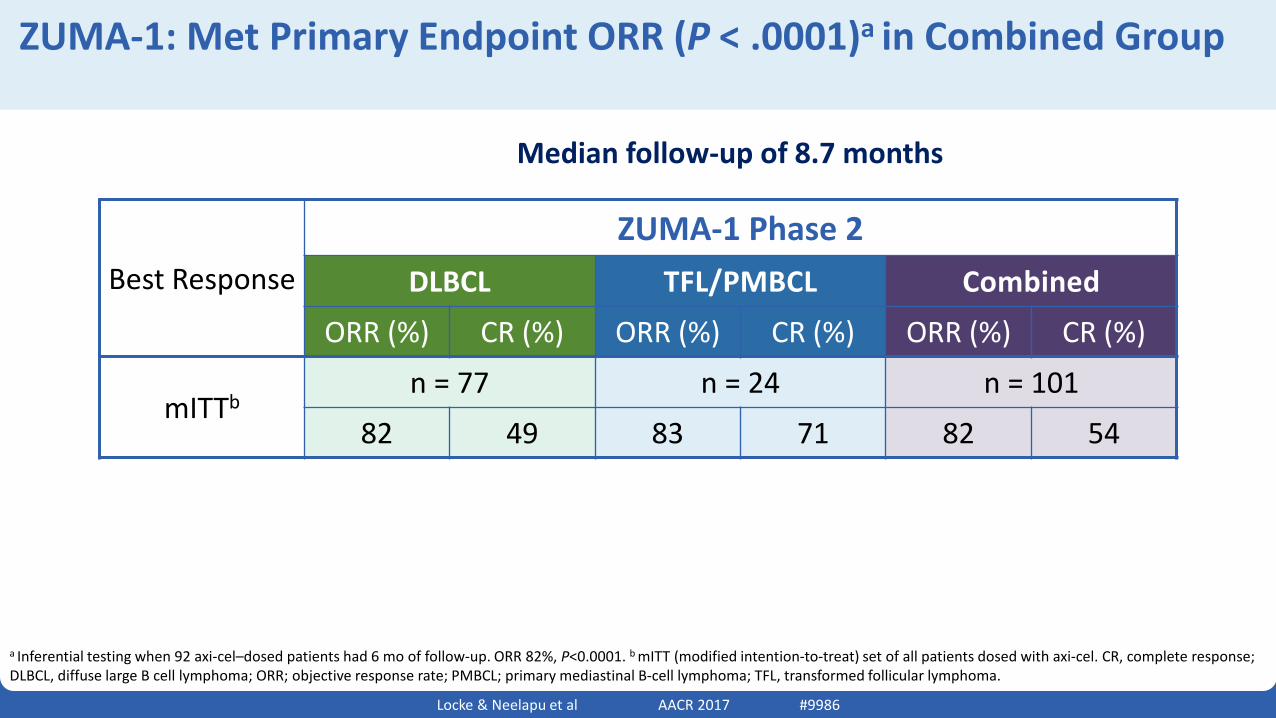
ZUMA-1: Met Primary Endpoint ORR (P < .0001)a in Combined Group
a Inferential testing when 92 axi-cel–dosed patients had 6 mo of follow-up. ORR 82%, P<0.0001. b mITT (modified intention-to-treat) set of all patients dosed with axi-cel. CR, complete response; DLBCL, diffuse large B cell lymphoma; ORR; objective response rate; PMBCL; primary mediastinal B-cell lymphoma; TFL, transformed follicular lymphoma.
Best ResponseZUMA-1 Phase 2
DLBCL TFL/PMBCL Combined
ORR (%) CR (%) ORR (%) CR (%) ORR (%) CR (%)
mITTbn = 77 n = 24 n = 101
82 49 83 71 82 54
Median follow-up of 8.7 months
Locke & Neelapu et al AACR 2017 #9986
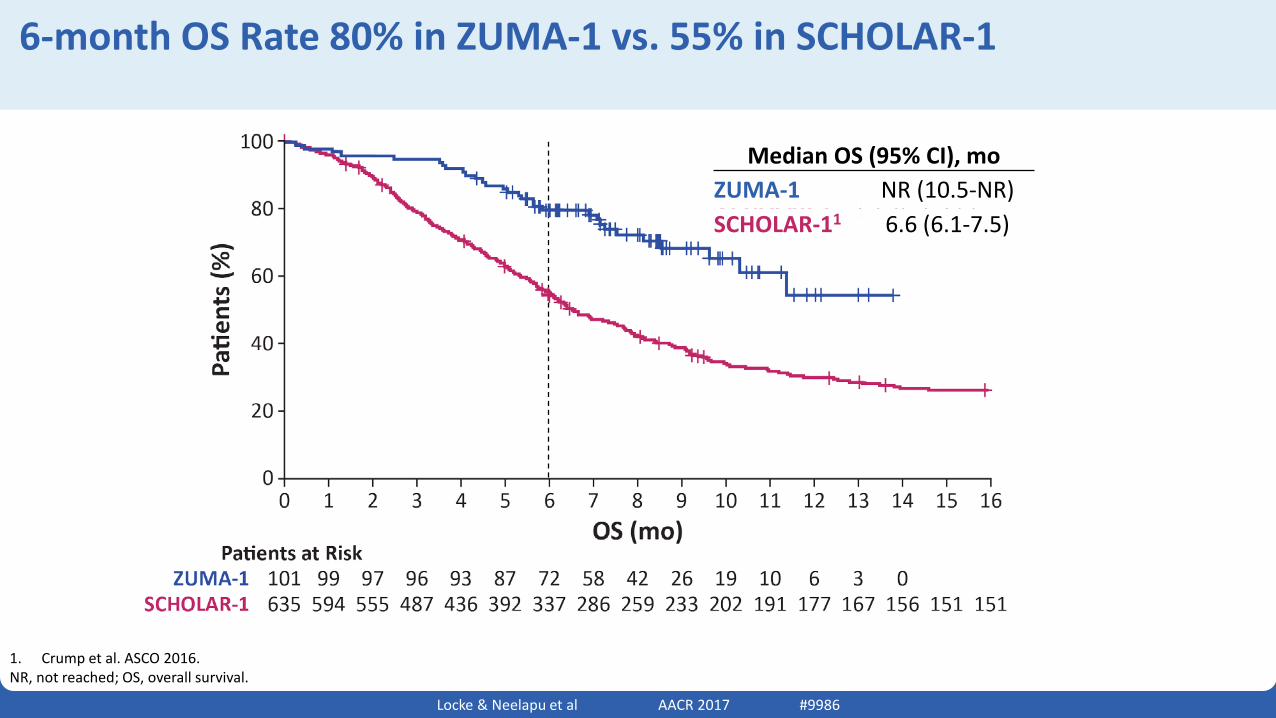
6-month OS Rate 80% in ZUMA-1 vs. 55% in SCHOLAR-1
1. Crump et al. ASCO 2016. NR, not reached; OS, overall survival.
Median OS (95% CI), moZUMA-1 NR (10.5-NR)SCHOLAR-11 6.6 (6.1-7.5)
Locke & Neelapu et al AACR 2017 #9986
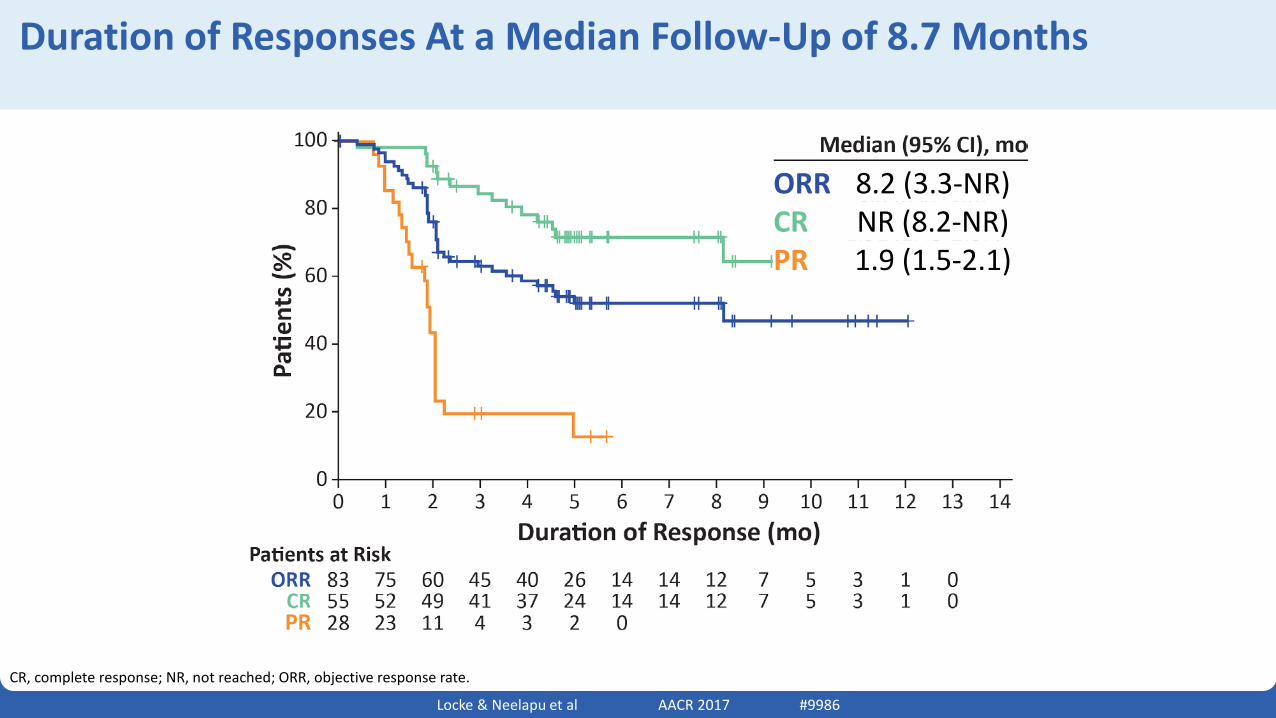
Duration of Responses At a Median Follow-Up of 8.7 Months
CR, complete response; NR, not reached; ORR, objective response rate.
ORR 8.2 (3.3-NR)CR NR (8.2-NR)PR 1.9 (1.5-2.1)
Locke & Neelapu et al AACR 2017 #9986
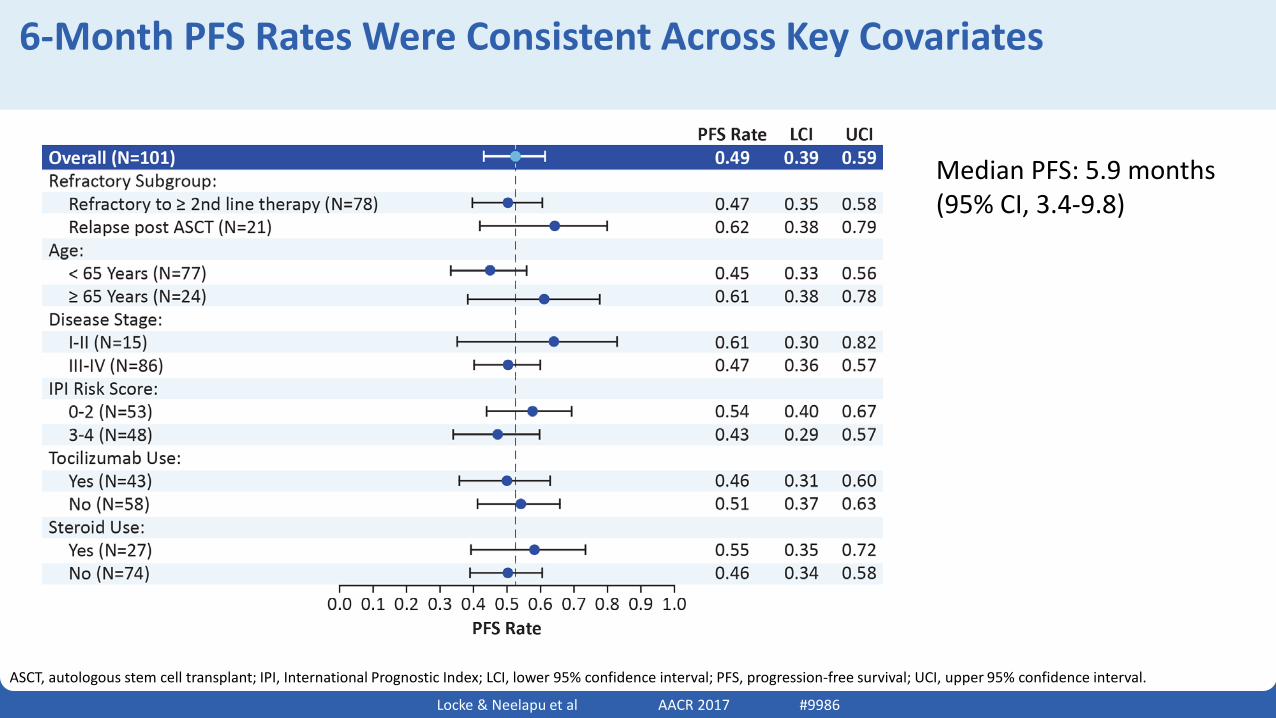
6-Month PFS Rates Were Consistent Across Key Covariates
ASCT, autologous stem cell transplant; IPI, International Prognostic Index; LCI, lower 95% confidence interval; PFS, progression-free survival; UCI, upper 95% confidence interval.
Median PFS: 5.9 months (95% CI, 3.4-9.8)
Locke & Neelapu et al AACR 2017 #9986
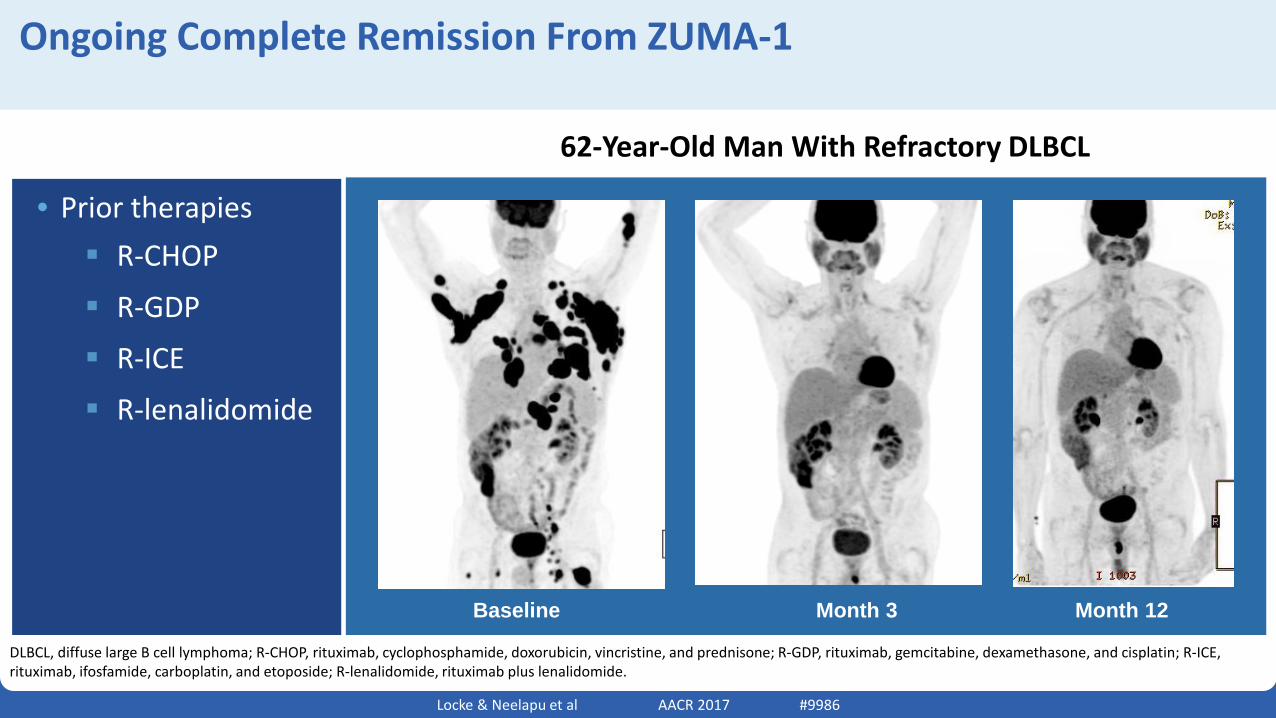
Ongoing Complete Remission From ZUMA-1
Baseline Month 3 Month 12
• Prior therapies R-CHOP
R-GDP
R-ICE
R-lenalidomide
62-Year-Old Man With Refractory DLBCL
DLBCL, diffuse large B cell lymphoma; R-CHOP, rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone; R-GDP, rituximab, gemcitabine, dexamethasone, and cisplatin; R-ICE, rituximab, ifosfamide, carboplatin, and etoposide; R-lenalidomide, rituximab plus lenalidomide.
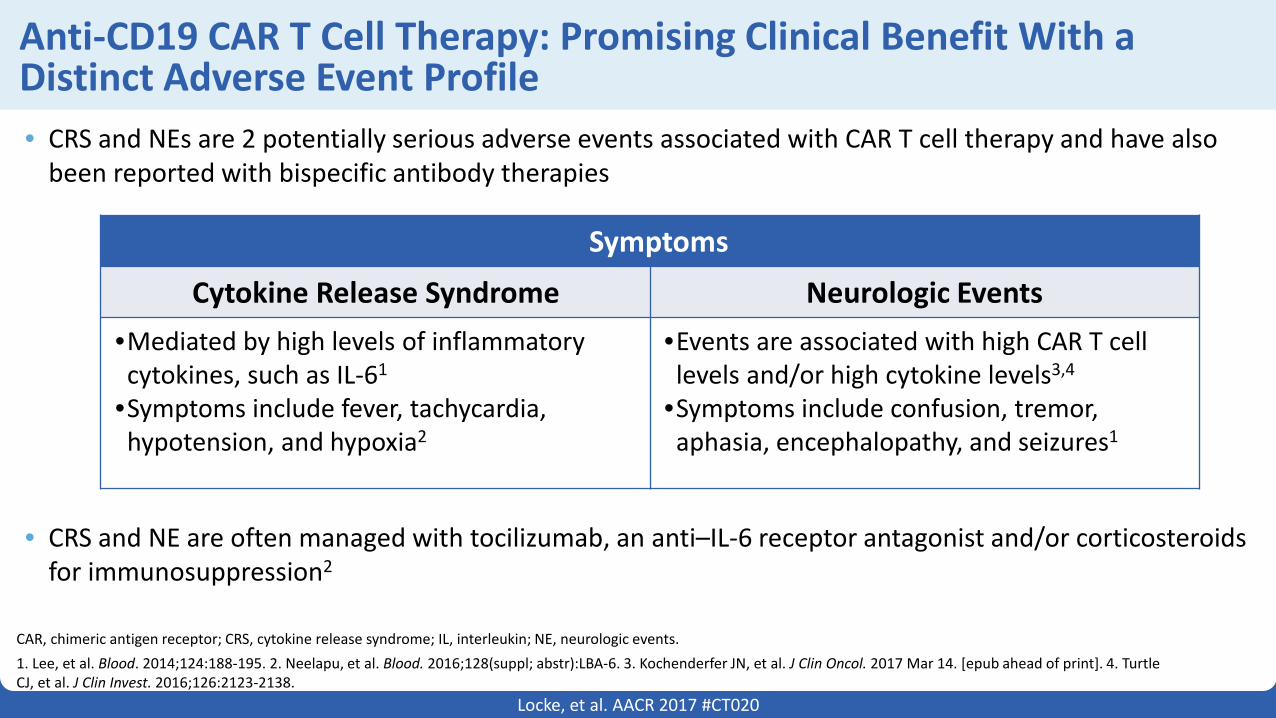
Anti-CD19 CAR T Cell Therapy: Promising Clinical Benefit With a Distinct Adverse Event Profile• CRS and NEs are 2 potentially serious adverse events associated with CAR T cell therapy and have also
been reported with bispecific antibody therapies
• CRS and NE are often managed with tocilizumab, an anti–IL-6 receptor antagonist and/or corticosteroids for immunosuppression2
Locke, et al. AACR 2017 #CT020
• Symptoms
Cytokine Release Syndrome Neurologic Events•Mediated by high levels of inflammatory cytokines, such as IL-61
•Symptoms include fever, tachycardia, hypotension, and hypoxia2
•Events are associated with high CAR T cell levels and/or high cytokine levels3,4
•Symptoms include confusion, tremor, aphasia, encephalopathy, and seizures1
CAR, chimeric antigen receptor; CRS, cytokine release syndrome; IL, interleukin; NE, neurologic events.1. Lee, et al. Blood. 2014;124:188-195. 2. Neelapu, et al. Blood. 2016;128(suppl; abstr):LBA-6. 3. Kochenderfer JN, et al. J Clin Oncol. 2017 Mar 14. [epub ahead of print]. 4. Turtle CJ, et al. J Clin Invest. 2016;126:2123-2138.
Locke & Neelapu et al AACR 2017 #9986
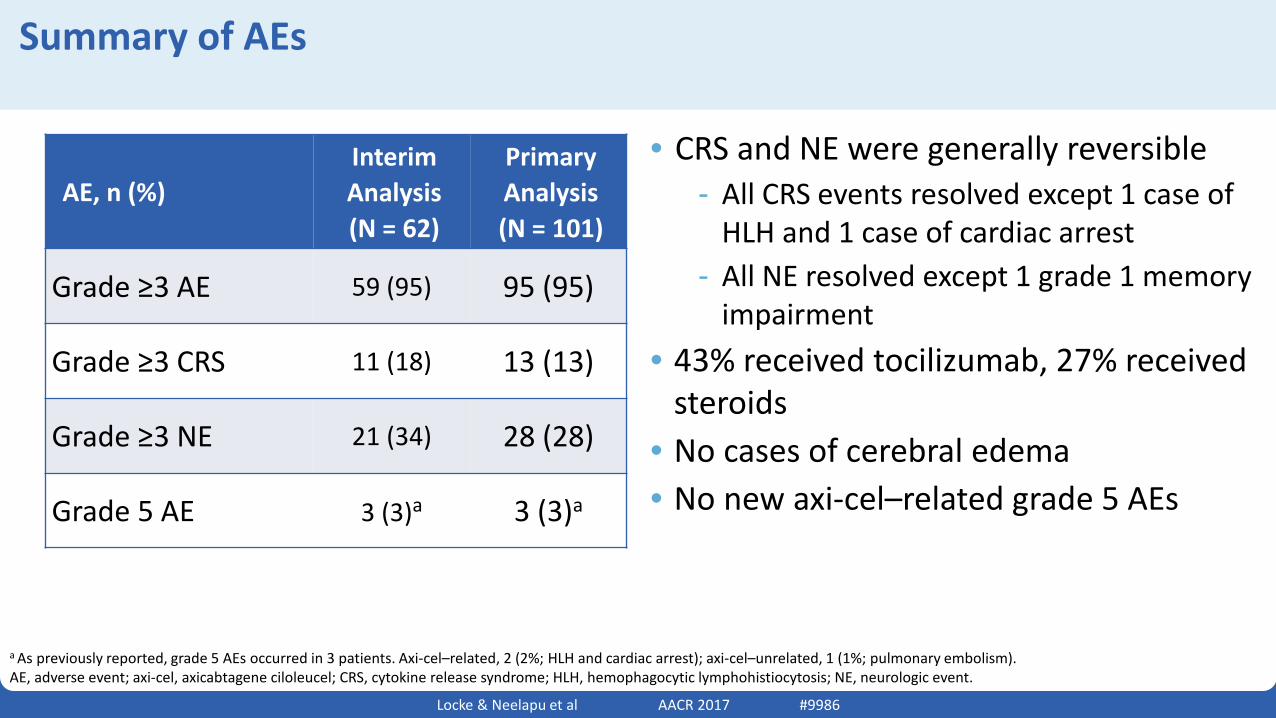
Summary of AEs
a As previously reported, grade 5 AEs occurred in 3 patients. Axi-cel–related, 2 (2%; HLH and cardiac arrest); axi-cel–unrelated, 1 (1%; pulmonary embolism).AE, adverse event; axi-cel, axicabtagene ciloleucel; CRS, cytokine release syndrome; HLH, hemophagocytic lymphohistiocytosis; NE, neurologic event.
• CRS and NE were generally reversible- All CRS events resolved except 1 case of
HLH and 1 case of cardiac arrest- All NE resolved except 1 grade 1 memory
impairment• 43% received tocilizumab, 27% received
steroids• No cases of cerebral edema• No new axi-cel–related grade 5 AEs
AE, n (%)Interim Analysis (N = 62)
Primary Analysis(N = 101)
Grade ≥3 AE 59 (95) 95 (95)
Grade ≥3 CRS 11 (18) 13 (13)
Grade ≥3 NE 21 (34) 28 (28)
Grade 5 AE 3 (3)a 3 (3)a
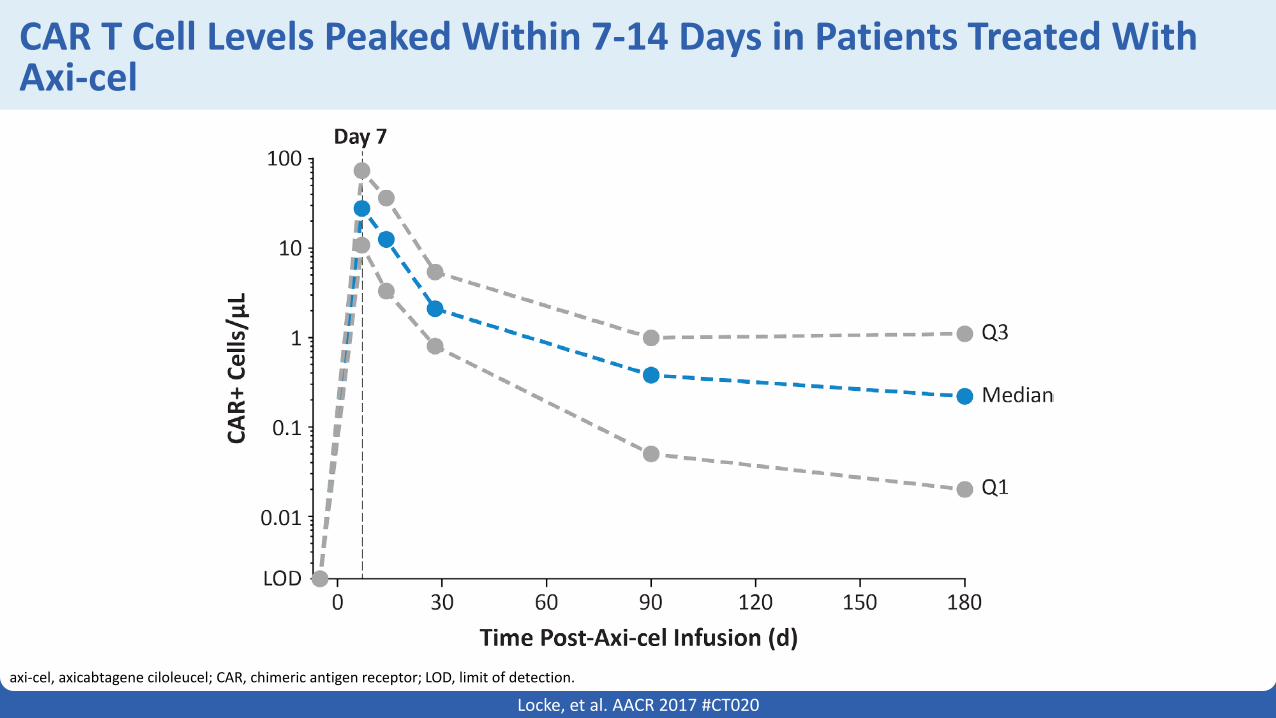
CAR T Cell Levels Peaked Within 7-14 Days in Patients Treated With Axi-cel
axi-cel, axicabtagene ciloleucel; CAR, chimeric antigen receptor; LOD, limit of detection.
Locke, et al. AACR 2017 #CT020
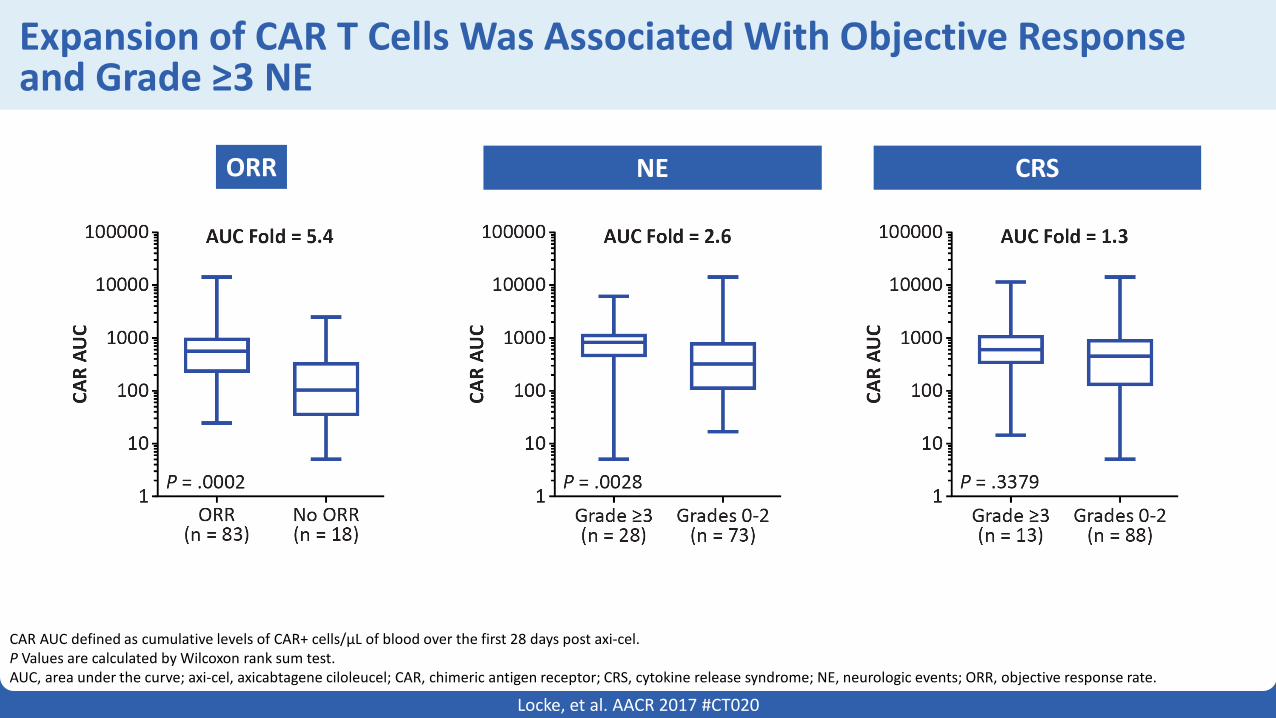
Expansion of CAR T Cells Was Associated With Objective Response and Grade ≥3 NE
CAR AUC defined as cumulative levels of CAR+ cells/µL of blood over the first 28 days post axi-cel.P Values are calculated by Wilcoxon rank sum test.AUC, area under the curve; axi-cel, axicabtagene ciloleucel; CAR, chimeric antigen receptor; CRS, cytokine release syndrome; NE, neurologic events; ORR, objective response rate.
Locke, et al. AACR 2017 #CT020
ORR NE CRS
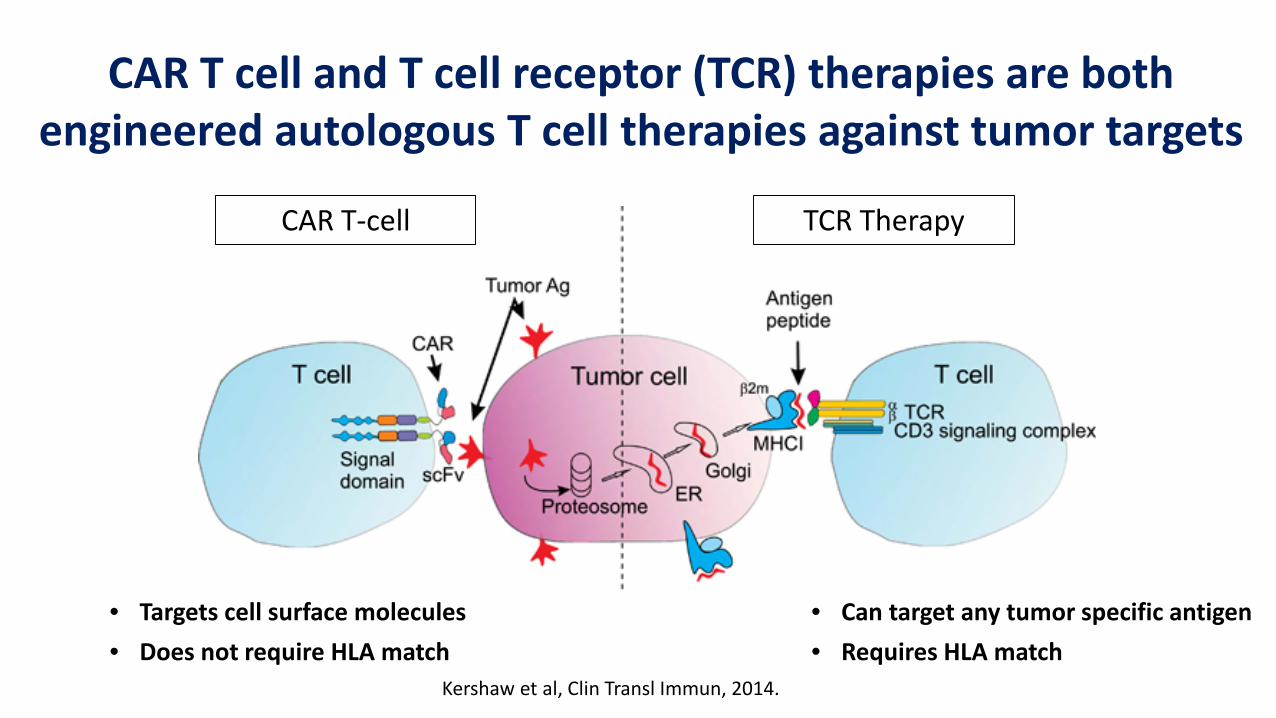
CAR T-cell TCR Therapy
CAR T cell and T cell receptor (TCR) therapies are both engineered autologous T cell therapies against tumor targets
Kershaw et al, Clin Transl Immun, 2014.
• Targets cell surface molecules• Does not require HLA match
• Can target any tumor specific antigen• Requires HLA match
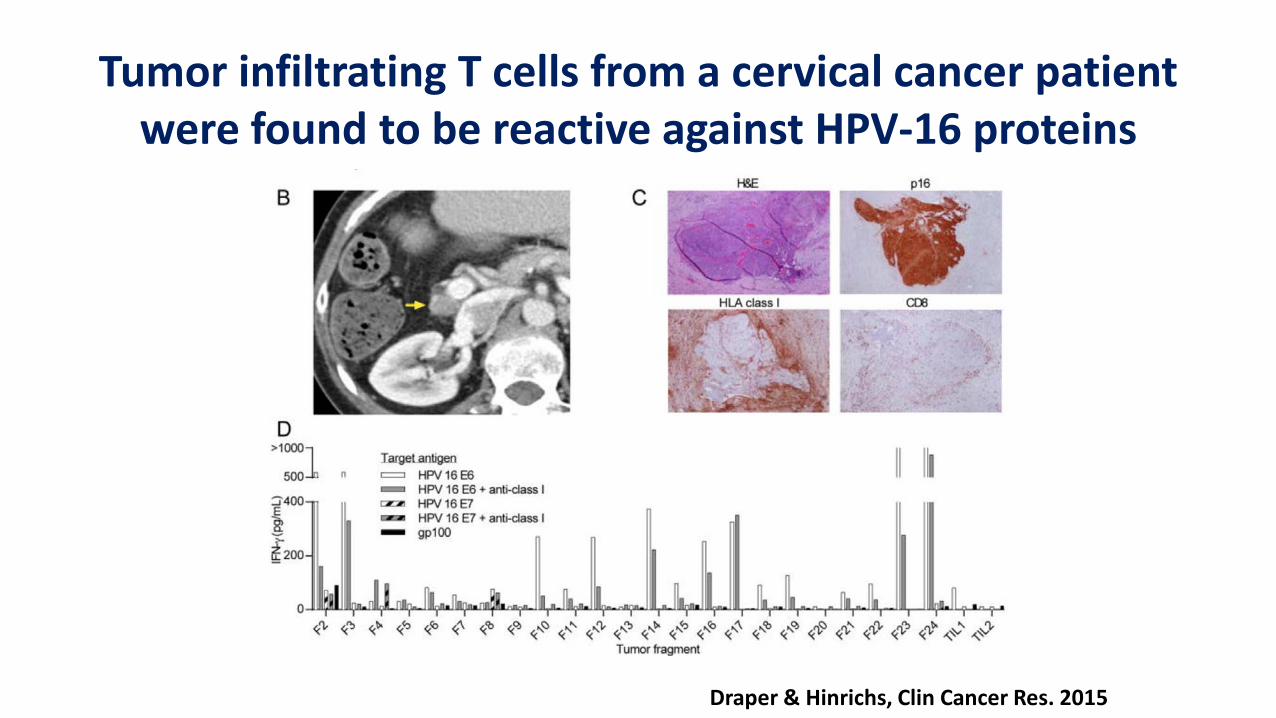
Tumor infiltrating T cells from a cervical cancer patient were found to be reactive against HPV-16 proteins
Draper & Hinrichs, Clin Cancer Res. 2015
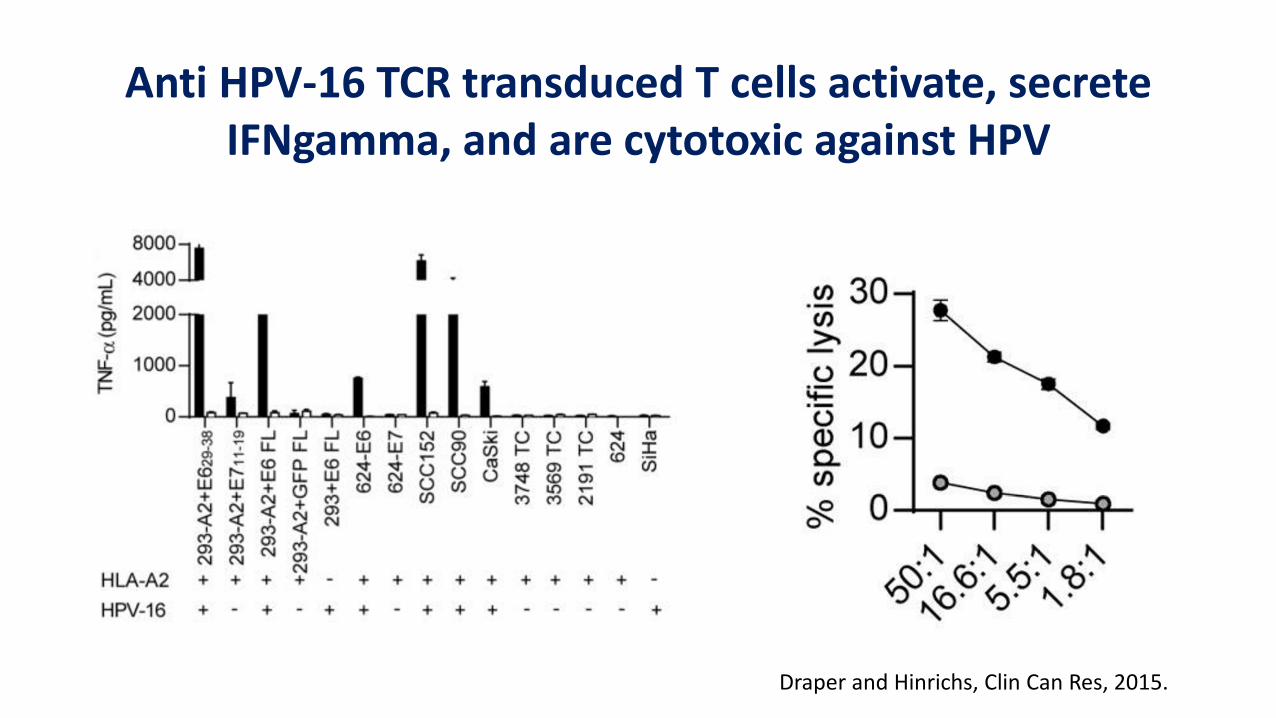
Anti HPV-16 TCR transduced T cells activate, secrete IFNgamma, and are cytotoxic against HPV
Draper and Hinrichs, Clin Can Res, 2015.
Ongoing clinical trials are testing out TCR engineered autologous T cell therapy for solid tumors
• HPV-16 E6• HPV-16 E7• MAGE A3• NY-ESO-1
Clinicaltrials.gov
“We always overestimate the change that will occur in the next two years and underestimate the change that will occur in the next ten. Don't let yourself be lulled into inaction.”
Bill Gates
AcknowledgmentsImmunology Working Group
•Abate Daga, Daniel•Antonia, Scott•Chung, Christine H.•Djeu, Julie Y.•Linda Kelley•Mulé, James J.•Mullinax, John E.•Pilon-Thomas, Shari A.•Ruffell, Brian•Sahebjam, Solmaz•Sarnaik, Amod A.•Soliman, Hatem H.•Wei, Sheng•Wright, Ken
+ Immune Cell Therapy Service
• Almhanna, Khaldoun• Anasetti, Claudio• Brayer, Jason B.• Chavez, Julio C.• Creelan, Ben C.• Davila, Marco L.• Druta, Mihaela• Kharfan-Dabaja, Mohamed A.• Fernandez, Hugo• Lancet, Jeffrey E.• Nishihori, Taiga• Pinilla Ibarz, Javier• Shah, Bijal• Sweet, Kendra L.
Kite Pharma
• Will Go• Jeff Wiezorek• Adrian Bot• John Rossi• Dustin Khiem
• Sattva Neelapu• All investigators
and study staff that participated on Zuma 1
• Matt Scott• Donna Evans• Austin Lannon
NCI-K23 Award (Locke)NCI-Cancer Clinical Investigator Team Leadership Award (Locke)