Embed Size (px)
Citation preview

Immunotherapy In Advanced Urothelial Cancer
Robert Dreicer, M.D., M.S., MACP, FASCOHead, Medical Oncology Section
Deputy Director University of Virginia Cancer CenterAssociate Director for Clinical Research
Co-Director Paul Mellon Urologic Oncology CenterProfessor of Medicine and Urology
University of Virginia School of Medicine

Disclosures
• Consultant: Orion, Astra Zeneca, Genentech/Roche, Sanofi-Genzyme, Janssen, Astellas, Bristol Myers Squibb, EMD Serono/Pfizer
• Research Funding: Genentech, Asana, Lilly, Bayer

Management Advanced Urothelial Cancer: Issues/Challenges
• A nasty aggressive epithelial cancer
• “Moderately” chemotherapy responsive, but few CR’s
• Impacts an “older” patient population
• Relatively high rate of patients with compromised performance status and/or renal function : The unfit patient

State of the Art Therapy in Advanced Urothelial Cancer Circa Spring 2016
1Loehrer JCO 1992; 2Von der Maase JCO 2000; 3 Bellmunt et al JCO 20124De Santis ASCO 2010; 5Linardou Urology 2004 6Nogué-Aliguer Cancer 2003; 7Rosenberg et al Lancet 2016
Setting Regimen Response RateMedian Survival
1st line CisplatinEligible
MVAC1
Gemcitabine +Cisplatin2
PGC3
40-50%12-15 months
Cisplatin Ineligible
Gemcitabine +Carboplatin4-6 36-56% 7-9 months
2nd line Single Agent Chemotherapy
~10% 5-8 months

Management of Metastatic Urothelial Cancer: Summary of Current Evidence
• Cisplatin-based combination chemotherapy provides the potential to cure in the range of 5-15%, primarily in good PS pts with low volume nodal disease
• Non-cisplatin based chemotherapy appears to be primarily palliative, may impact slightly on PFS
• A small group of highly selected patients may benefit from an integrated chemotherapy/surgical approach

Second Line Chemotherapy for Advanced Urothelial Cancer
• To date no level 1 evidence supporting improvement in survival from chemotherapy
• There is no current evidence for the superiority of salvage combination chemotherapy compared to monotherapy, or precise delineation of non-cross resistant regimens

PD-L1 Expression in Metastatic Bladder Cancer
Powles T et al. Nature. 2014;515:558-562.
IHC Score(N = 205)
Tumor-Infiltrating Immune Cells, n (%)
Tumor Cells, n (%)
IHC 3 18 (9) 14 (7)
IHC 2 37 (18) 8 (4)
IHC 1 89 (43) 37 (18)
IHC 0 61 (30) 146 (71)
PD-L1 Positivity in UBC Tumors by IHC

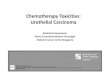
Tumor Response With Atezolizumab Anti–PD-L1 Therapy in Metastatic Bladder Cancer
Powles T et al. Nature. 2014;515:558-562.
a Patients with CRs who had ≤100% reduction of target lesions due to lymph node target lesions; all lymph nodes returned to normal size per RECIST v1.1.
Max
imu
m S
LD R
ed
uct
ion
Fro
m B
ase
line,
%
100
90
80
70
60
50
40
30
20
10
0
-10
-20
-30
-40
-50
-60
-70
-80
-90
-100
IHC (IC) 0IHC (IC) 1IHC (IC) 2IHC (IC) 3IHC (IC) Unknown
a
a

Expression characteristics of bladder cancer. Integrated analysis of mRNA, miRNA and protein data led to identification of distinct subsets of urothelial carcinoma
MARCH 2014 | VOL 507 | NATURE | 315

IMvigor 210: Phase 2 Atezolizumab in Metastatic UC
1. Rosenberg JE et al. Lancet. 2016;387:1909-1920.
Treatment
Patients
Cohort 1 (N = 119)1st-line cisplatin
ineligible
Atezolizumab 1,200 mg IV every 3 wk
until RECIST v1.1 progression
IMvigor 210
• Inoperable locally advanced or metastatic urothelial carcinoma
• Predominantly UC histology
• Tumor tissue evaluable for PD-L1 testinga
Atezolizumab 1,200 mg IV every 3 wk
until loss of clinical benefit
Cohort 2 (N = 310)Platinum-treated mUC
Co-primary endpoints: (1) Confirmed ORR by RECIST v1.1 and central IRF
(2) ORR by investigator-assessed modified RECIST
Key secondary endpoints: DOR, PFS, OS, safety

Dreicer R, et al. IMvigor210: atezolizumab in platinum-treated mUC. ASCO 2016

KEYNOTE-045 Phase 3 Trial (NCT02256436)1
1. Bellmunt J et al. Society for Immunotherapy of Cancer 2016 Annual Meeting (SITC 2016). Abstract 470.
Key Eligibility Criteria• Urothelial carcinoma of the renal pelvis,
ureter, bladder, or urethra• Transitional cell predominant• PD after 1-2 lines of platinum-based
chemo or recurrence within 12 mo of perioperative platinum-based therapy
• ECOG PS 0-2• Provision of tumor sample for biomarker
assessment
Stratification Factors• ECOG PS (0/1 vs 2)• Hemoglobin level (<10 vs ≥10 g/dL)• Liver metastases (yes vs no)• Time from last chemotherapy dose
(<3 vs ≥3 mo)
Pembrolizumab 200 mg IV Q3W for 2 y
Paclitaxel 175 mg/m2 Q3W, orDocetaxel 75 mg/m2 Q3W, orVinflunine 320 mg/m2 Q3W
n = 270
n = 272
R 1:1
N = 542
Key Endpoints• Primary: OS and PFS in total and in PD-L1 combined
positive score ≥10% populations• Secondary: ORR and DOR in total and in PD-L1
combined positive score ≥10% populations; safety in total population

Bellmunt J, et al.
published on
February 17 2017,
at NEJM.org.
DOI:
10.1056/NEJMoa1
613683

Bellmunt J, et al. published on February 17 2017, at NEJM.org.
DOI: 10.1056/NEJMoa1613683

Pembrolizumab as Second-Line Therapy for Advanced Urothelial Carcinoma
Overall Survival
10.3 mo in P vs 7.4 mo C
Progression Free Survival





IMvigor210, CheckMate 275, STUDY 1108 and JAVELIN: Recent Investigational and Registrational Trials in Pretreated mUC*
Patient number
Study Arms
Key Inclusion Criteria
Primary Endpoints
PD-L1 expressionPD-L1+PD-L1-NE/unknown
*No head-to-head studies have been conducted and direct comparisons cannot be made between these studies. †265 patients were evaluated for efficacy. ‡191 locally advanced/mUC patients enrolled and received treatment; 103 patients were eligible for efficacy analysis..§241 mUC patients were evaluated for safety and 153 mUC patients were evaluated for efficacy.BOR, best overall response; E1Loriot Y et al. Poster presentation at ESMO 2016. 783P; 2Sharma P, et al. Lancet Oncol. 2017; 3Powles T, et al. Poster presentation at ASCO GU. 286. 4Patel M et al. Poster presentation at ASCO GU. 330.
CheckMate 2752
NivolumabPhase 2
270†
Nivolumab 3 mg/kg IV q2w
• ≥1 Platinum-containing or ≤12 months of neoadjuvant/adjuvant treatment
• Tumor tissue for PD-L1 testing
• ECOG PS 0-1
• ORR
1% cut-off on TC• 46%• 54%
Study 11083
DurvalumabPhase 1/2
191‡
Durvalumab10 mg/kg IV q2w
• Histologically confirmed solid tumors
Locally advanced or mUC cohort:• Had progressed, on were
ineligible for, or refused any number of prior therapies
• ECOG PS 0-1
• Safety• ORR
25% cut-off on TC or IC• 51.3%• 41.4%• 7.3%
IMvigor 2101
Atezolizumab Phase 2
310 (Cohort 2)
Atezolizumab 1200 mg (IV) q3w
Cohort 2:• ≥1 Platinum-containing or ≤12
months of neoadjuvant/adjuvant treatment
• Tumor tissue for PD-L1 testing
• ECOG PS 0-1
• ORR
IC1/2/3 (1% cut-off on IC)• 67%• 33%
JAVELIN solid tumor4
AvelumabPhase 1
241§
Avelumab 10 mg/kg q2w
• Solid tumorsmUC cohort:• Had progressed post-platinum
treatment or cisplatin-ineligible• Unselected for PD-L1• ECOG PS 0-1
• BOR• Safety
5% cut-off on TC• 33.6%• 48.5%• 17.8%

Patients “Unfit” for Cisplatin-based Chemotherapy
• Represents 40-60% of patients with advanced urothelial cancer
• Widely accepted definition includes• ECOG 2 or greater
• Creatinine Clearance ≤ 60 ml/min
• Grade 2 or greater peripheral neuropathy/hearing loss

Carboplatin Combinations for Advanced Bladder Cancer Patients: EORTC Study 30986
De Santis M et al. J Clin Oncol. 2012;30:191-199.
(N = 238)
Gem/Carbo M-CAVI
9.3 months 8.1 months
Median OS
100
80
60
40
20
0Su
rviv
al, %
0 2 3 4 5 6 7
Time, y
M-CAVI
Gem/Carbo
Log-rank test P = .64
Treatmen
tM-CAVI
Gem/Carb
o
O n No. at Risk
44 15 5 2 2 1
37 13 7 3 1 1
119
119
110
108
1

Pembrolizumab
200 mg every 3 wk
Primary Endpoints
• ORR in all patients
• ORR in patients with
PD-L1–positive tumors
Patients (N = 350)
• Advanced urothelial
cancer
• No prior chemotherapy
for metastatic disease
• ECOG PS 0-2
• Ineligible for cisplatin
based on ≥1 of the
following:
– CrCl <60 mL/min
– ECOG PS 2
– ≥ Grade 2 neuropathy
or hearing loss
– NYHA class III CHF
• Secondary Endpoints: DOR, PFS, OS, and ORR in all
patients, PD-L1–positive and PD-L1–high expressing
patients; safety and tolerability
• First 100 patients included in planned interim analysis
– Determine the PD-L1–high expression cutpoint
KEYNOTE-052: Pembrolizumab as Front-Line Therapy
1. Balar A et al. ESMO 2016. Abstract LBA32_PR.

Patient Characteristics:Keynote-052
Balar A et al. Lancet Oncol 2017Published OnlineSeptember 26, 2017http://dx.doi.org/10.1016/S1470-2045(17)30616-2

KEYNOTE-052: Efficacy
Balar A et al. Lancet Oncol 2017 Published Online September 26, 2017 http://dx.doi.org/10.1016/ S1470-2045(17)30616-2

KEYNOTE-052: Efficacy
Balar A et al. Lancet Oncol 2017 Published Online September 26, 2017 http://dx.doi.org/10.1016/ S1470-2045(17)30616-2
Response in Total Study Population

KEYNOTE-052 Adverse Events
AE, % (N = 370) Any Grade Grade 3-5
Any 46 16
Fatigue 15 2
Pruritus 14 1
Pyrexia 5 1
Decreased appetite 10 2
Diarrhea 8 1
Rash 9 1
ALT/AST increase 11/13 3/3
Nausea 8 1
Muscle spasms 2 2
Balar A et al. Lancet Oncol 2017 Published Online September 26, 2017 http://dx.doi.org/10.1016/ S1470-2045(17)30616-2

Standard Therapy in Advanced Urothelial Cancer
Setting Regimen Response Rate Median Survival
1st line
Cisplatineligible
MVAC1
Gemcitabine + cisplatin2
PGC3
40%-50%12-15 mo
Cisplatin ineligible
Gemcitabine +carboplatin4-6 36%-56% 7-9 mo
Atezolizumab Pembrolizumab
~24%~15.9 months (atezolizumab)
2nd line
Atezolizumab7
Nivolumab, Durvalumab, AvelumabPembrolizumab 15%-19% 7.9-10.3 mo
Single-agent chemotherapy
~10% 5-8 mo
1. Loehrer PJ Sr et al. J Clin Oncol. 1992;10:1066-1073. 2. von der Maase H et al. J Clin Oncol. 2000;18:3068-3077. 3. Bellmunt J et al. J Clin Oncol. 2012;30:1107-1113. 4. De
Santis M et al. J Clin Oncol. 2012;30:191-199. 5. Linardou H et al. Urology. 2004;64:479-484. 6. Nogué-Aliguer M et al. Cancer. 2003;97:2180-2186. 7. Rosenberg JE et al. Lancet.
2016;387:1909-1920.

CheckMate-032: Open-Label, Multicenter Phase 1/2 Study
• Treatment beyond progression was permitted if nivolumab was tolerated and clinical benefit was noted
• Patients in the monotherapy arm could cross over to nivolumab combined with ipilimumab after progression if they met prespecified criteria
Nivolumab3 mg/kg IV Q2W
(n = 78)
Nivolumab 3 mg/kg IV Q2W
Pretreated patients with locally advanced or metastatic urothelial carcinoma
Nivolumab 1 mg/kg + ipilimumab 3 mg/kg IV Q3W for 4 cycles
(n = 26)
Nivolumab 3 mg/kg + ipilimumab 1 mg/kg IV Q3W for 4 cycles
(n = 105)
http://www.clinicaltrials.gov/ct2/show/NCT01928394. Accessed May 15, 2017.

Summary
• Immune checkpoint therapy is a standard of care for patients progressing on front-line therapy platinum-based chemotherapy
• For many “unfit” patients front line checkpoint inhibitor therapy is appropriate, although subsets of patients may benefit from cytotoxic therapy used upfront
• PDL1 expression as a biomarker to decide therapy is not useful in making therapy decisions
• Combinatorial immunomodulatory therapies are being broadly investigated
• For a modest but real subset of patients checkpoint inhibitor therapy has provided a paradigm shifting benefit