Embed Size (px)
Citation preview

J. Pathol. 189: 368–377 (1999)
IMMUNOMAGNETIC SEPARATION FOR ENRICHMENTAND SENSITIVE DETECTION OF DISSEMINATEDTUMOUR CELLS IN PATIENTS WITH HEAD AND
NECK SCC
. *, . , . .-.
King’s College School of Medicine and Dentistry, Denmark Hill, London SE5 8RX, U.K.
SUMMARY
Screening for malignant cells in the blood and bone marrow was introduced as a strategy for the improved detection of tumour spreadand may predict the development of distant metastases. The sensitivity of these approaches depends on several factors, including thechoice of antibody for immunocytochemistry (ICC) and the number of cells examined. In this study criteria have been defined for scoringcells reactive with a pan-cytokeratin antibody as tumour, by comparing immunostained cells in clinical samples obtained from head andneck cancer patients and a control group without epithelial malignancy. When leucocyte subfractions are prepared by density gradientseparation (DGS) from central venous blood obtained from patients with advanced head and neck squamous cell carcinoma (SCC) andscreened by ICC, epithelial tumour cells sediment preferentially with the mononuclear cells but may also be detected in the granulocyte(GC) fraction. Some cases were found to have more tumour cells in the GC fraction. Similar results were seen in model experiments.To increase the sensitivity of the ICC approach, the efficiency of positive immunomagnetic selection (IMS) using Dynabeads coated withan antibody recognizing the Ber-EP4 epitope has been compared with negative IMS using anti-CD45 Dynabeads. Tumour cells wererecovered from bone marrow aspirates for 2/17 cases using the positive enrichment technique and for 11/17 patients following negativeIMS. These findings justify prospective studies incorporating negative IMS to establish the prognostic significance of these disseminatedtumour cells for this group of patients. Copyright ? 1999 John Wiley & Sons, Ltd.
KEY WORDS—head and neck cancer; tumour; metastasis; antibodies; immunocytochemistry; cell separation; keratins; tumour antigens
*Correspondence to: Professor M. Partridge, Department of Oraland Maxillofacial Surgery Molecular Oncology, King’s College School
INTRODUCTION
Seventy years ago, head and neck cancer was consid-ered to be a local disease with the incidence of distantmetastases being less than 1 per cent.1 whereas nowmore than 20 per cent of patients die as a direct result ofdistant metastatic disease, with their tumour controlledboth at the primary site and in the neck.2 Post-mortemstudies reveal that the incidence of distant metastasesmay be as high as 40–55 per cent.3 At present, there areno histological or biological criteria which predict therisk of development of metastatic disease. Indirect prog-nostic criteria, such as tumour size, lymph node spread,and grade, are therefore used to establish a patient’s riskof developing systemic disease when planning surgeryand to determine whether or not post-operative adju-vant therapy should be given. However, despite the useof these criteria, improvements in surgery and radio-therapy, together with careful examination of surgicalmargins and lymph nodes for rare malignant cells, theoverall 5-year survival remains at a disappointing 45–50per cent.4 This suggests that tumour deposits, or precan-cerous cells, not detected by current investigative proce-dures, must remain in the body to account for thischanging pattern of clinical disease.
Three approaches have been devised to detect smallnumbers of disseminated tumour cells in patients with
of Medicine and Dentistry, Caldecot Road, London SE5 9RW, U.K.
CCC 0022–3417/99/120368–10$17.50Copyright ? 1999 John Wiley & Sons, Ltd.
solid tumours and to assess whether their presence in thehaematopoietic cell compartment is associated with thedevelopment of distant metastases. Immunocytochemis-try (ICC) is frequently used to look for expression ofepithelial cell specific targets.5–8 An alternative approachis based on reverse transcription-polymerase chain reac-tion for epithelial specific gene transcripts (for examplessee refs 9 and 10). Microsatellite analysis of DNA canalso be used to identify aberrations in serum sampleswhich are not present in lymphocytes.11
Disseminated epithelial cells have also been identifiedin mononuclear cells (MNCs) obtained from the bonemarrow of 41/108 (37 per cent)7 and 10/31 (32 per cent)8
cases with squamous cell carcinoma (SCC) of the headand neck, using an ICC technique. These disseminatedepithelial cells were detected in bone marrow obtainedfrom 26 per cent of early stage 1 tumours and 48 per centof stage 4 cases.7 Although the number of cases analysedto date is small and follow-up data are limited, this studyrevealed that a higher percentage of patients with apositive marrow developed either local or distant recur-rence and had a shorter disease-free survival.7 Thissuggests that although the skeleton is not the principalsite of distant metastases for patients with head andneck cancers, these disseminated cells may mark thebeginning of systemic disease.
ICC is frequently used to screen clinical samples forexpression of epithelial cell specific targets to detectdisseminated tumour cells in patients with head and
neck cancer. Keratins 8, 18, and 19 are frequentlyReceived 7 July 1998Revised 4 March 1999
Accepted 27 May 1999

immunoreaction is tumour-specific.
369DISSEMINATED TUMOUR CELLS IN HEAD AND NECK SCC
chosen as the target, since these polypeptides areexpressed by a proportion of head and neck SCCs,12,13
whereas they are only very rarely detected in haemato-poietic cells.14 However, the expression of these antigensalters with the state of epithelial differentiation andalthough most well and moderately differentiated headand neck SCCs express these simple keratins, levelsmay be only low, or absent in poorly differentiatedtumours.13 For this reason, most protocols based onICC employ pan-cytokeratin antibodies to maximize thechance that the assay will detect tumour cells.
However, there are contradictory reports in the litera-ture about the frequency of malignant cells in thehaematopoietic cell compartment and their prognosticsignificance for many tumour types.15–18 These discrep-ancies arise because several factors influence the sensi-tivity and specificity of the method used for tumour celldetection. These include the choice of target for tumourcell detection, the nature and number of leucocytesexamined, the criteria used to score a cell as tumour, theexistence of additional cell types which express thetarget, and other sources of cross-reactivity.
To overcome some of these problems, attempts havebeen made to standardize the detection of disseminatedtumour cells by screening 2#106 MNCs.19 However,patients with early-stage lung, breast, or head and neckcancer may have only 1–2 cells per 2#106 MNCs,5,6,8 sothat screening only this number can categorize somepatients with disseminated tumour as false negatives. Toimprove the sensitivity of tumour cell detection, largernumbers of leucocytes must be examined, withoutincreasing the number of microscope slides which needto be scored. To facilitate this, methods have beendeveloped to enrich MNCs for tumour cells, using eitherpositive or negative selection with antibodies boundto immunomagnetic beads. However, the potential toenrich clinical samples for tumour in this way must bebalanced against the downside that some tumourcells may be lost each time a clinical sample is manipu-lated, or if the target antigen is not expressed on thetumour cell.
To achieve high sensitivity for tumour cell detectionwhen blood and bone marrow aspirates are examined, itis important that leucocyte fractions which may harbourtumour cells are not discarded. To date, the majority ofstudies designed to detect disseminated tumour havebeen based on the analysis of MNCs prepared by DGS(for examples see refs 5, 6, and 20–23). In this study, wehave investigated whether epithelial tumour cells sedi-ment preferentially with the MNC or granulocyte (GC)fraction, in model experiments and by analysis of bloodand bone marrow obtained from patients with advancedhead and neck malignancy. To evaluate the suitability ofincorporating IMS into protocols for use in long-termprospective studies, we have compared the efficiency ofpositive IMS with Ber-EP4-coated Dynabeads, andnegative IMS with anti-CD45-coated beads, to enrichblood and bone marrow aspirates for disseminatedtumour cells. However, when ICC with a pan-cytokeratin reagent is used for the detection of tumourcells, there may also be rare false-positive immuno-reactive cells, as a small percentage of bone marrow
Copyright ? 1999 John Wiley & Sons, Ltd.
aspirates obtained from healthy volunteers contain cellswhich react with these antibodies.24,25 Thus, in order toensure high specificity of the ICC, we have incorporatedappropriate controls and morphological assessmentof the immunostained cells to demonstrate that the
24,25
MATERIALS AND METHODS
Cell lines derived from head and neck SCC, KB(American Type Culture Collection, Rockville, MD,U.S.A., CCL-17), SCC 25 and HN526 were maintained inDMEM with 10 per cent FCS (Gibco, Paisley, U.K.).Monolayers were washed in EDTA, incubated with0·25 per cent trypsin or with EDTA, and single cellsuspensions were prepared by mechanical disruption.
Clinical samples
Biopsies of 25 head and neck SCCs were taken at thetime of surgery and stored at "70)C until required.Ethical Committee approval for this project was grantedat King’s College Hospital. Central venous blood(50 ml) was collected pre-operatively from 20/25 of thesepatients. Cases 1–8 had recurrent tumours and cases9–20 were undergoing treatment for a primary malig-nancy. Bone marrow (up to 20 ml) was obtained fromthe same group of head and neck cancer patients, fromten cases previously treated for haematological malig-nancy and 20 individuals undergoing bone marrowbiopsy for other diagnostic purposes. Peripheral venousblood (50 ml) was also collected from patients withoutepithelial malignancy and healthy volunteers. Thesamples were collected with sodium citrate and mixedwith 0·1 vol. dextran (average MW 500 000, 6 per centw/v) to sediment the erythrocytes. Bone marrow aspi-rates were diluted 1:1 with phosphate-buffered saline(PBS) prior to preparation of leucocyte-rich plasma andthe leucocytes were washed in 10# volume PBS with 2per cent FCS to reduce the viscosity of the sample. Awhite cell count was obtained for each leucocyte-richplasma prepared to ensure that 2#107 cells were testedfor each patient. To assess whether tumour cells werelost into the erythrocyte pellet when leucocyte-richplasma was prepared, 10 ml of venous blood was spikedwith varying numbers of cultured tumour cells; aliquotsof the erythrocyte pellet were sedimented onto slidescoated with Cell-Tak= tissue adhesive (5 ìg/cm2; BectonDickinson Inc., Oxford, U.K.27), counterstained, andcontaminating tumour cells counted. For some exper-iments, leucocytes were concentrated by centrifugationat 350 g and analysed without DGS.
Density gradient separation (DGS) andimmunophenotyping
MNC and GC fractions were recovered by DGS ofleucocytes with Histopaque-1077 (Sigma, Poole, Dorset,U.K.). Red blood cells were lysed with 0·83 per cent w/vNH4Cl/10 n Hepes. To assess the purity of theMNC and GC subfractions, 106 cells were stained with
J. Pathol. 189: 368–377 (1999)

370 M. PARTRIDGE ET AL.
10 ìl of phyco-erythrin-conjugated anti-CD45 (Dako)for 20 min. After washing and fixation, 5000 cells wereanalysed with an EPICS XL flow cytometer.
Immunohistochemistry (IHC) and immunocytochemistry(ICC)
Frozen sections (5 ìm) from 20 head and neck SCCswere fixed in acetone for 10 min. After washing in TRIS-buffered saline (TBS), tissues were incubated for 10 minin fetal bovine serum (Gibco, Paisley, U.K.) diluted 1 in5 in TBS to block non-specific binding. Sections wereexamined with antibodies recognizing Ber-EP4 (1:20;Dynal, Oslo, Norway), MOC-31 (1:50; Dako, HighWycombe, U.K.), AE1/AE3 (1:50; Dako), CD61 (1:200;Dako), CD41 (1:200; Dako), CD68 (1:50; Dako), andCD38 (1:100; Dako). In all cases, cells and tissues wereincubated for 60 min with 100 ìl of the appropriateantibody in a humid chamber. After washing in TBS,sections were incubated for 30 min with 100 ìl of rabbitanti-mouse Ig antibody (Dako; 1:25) diluted in 20 percent human serum, washed again, and 100 ìl ofalkaline phosphatase/monoclonal mouse anti-alkalinephosphatase (APAAP complex, Dako; 1:30) was addedfor 30 min. After further washing, the reaction productwas developed with New Fuchsin substrate solution(Dako) containing levamisole (1 m) to block endogen-ous alkaline phosphatase activity for 10 min. Sectionswere washed with water and counterstained withhaematoxylin.28 Head and neck cell lines were reactedwith Ber-EP4, MOC-31, AE1/AE3, and the EPIMET=
epithelial cell detection kit (alkaline phosphatase-conjugated A45-B/B3, {fab} Micromet, Munich, Ger-many), according to the manufacturer’s instructions.The suitability of AE1/AE3 and the EPIMET= kit fortumour cell detection was determined by screening6#107 leucocytes obtained from peripheral blood andbone marrow aspirates from patients without epithelialmalignancy, using the protocol described above.
Development of a model system to identify the locationof epithelial tumour cells after preparation of leucocytesubfractions by DGS
A model system was developed by seeding varyingnumbers of tumour cells derived from SCC cell linesinto leucocytes obtained from healthy volunteers.Tumour cells were added in the range of 200–5000 per2#107 leucocytes. (Two hundred cells were isolatedwith a micromanipulator.) After centrifugation throughHistopaque-1077, MNC and GC fractions wereharvested and their purity was assessed by immuno-phenotyping. MNCs or GCs, together with any co-sedimenting tumour cells, were transferred onto slidescoated with Cell-Tak tissue adhesive for ICC withAE1/AE3. Assays were performed in duplicate with theSCC 25, KB and HN5 cell lines. All leucocytes obtainedafter DGS were counted for each spiked sample. Nega-tive control slides were 2#107 MNCs and GCs stainedwith AE1/AE3. SCC cell lines served as a positivecontrol. Immunoreactive cells were scored by twoindependent observers.
Copyright ? 1999 John Wiley & Sons, Ltd.
Detection of disseminated tumour cells in blood-derivedMNCs and GCs for patients with advanced head andneck SCC
MNC and GC fractions were prepared by DGS for 20cancer patients and 2#107 leucocytes screened by ICCwith AE1/AE3 essentially as described above, but withthe modification that 2#107 leucocytes incubated withmouse anti-FITC (Sigma, Poole, Dorset, U.K.) of thesame subclass (IgG1) and at the same concentration ofimmunoglobulin as AE1/AE3 was the negative control.6Immunoreactive cells detected after staining with AE1/AE3 were scored as tumour using criteria defined fol-lowing examination of false-positive immunoreactivecells identified after staining leucocytes obtained frompatients without epithelial malignancy with AE1/AE3and the isotype-matched control antibody (see Resultssection). When adequate numbers of leucocytes wereobtained from patients found to have disseminatedtumour in the haematopoietic cell compartment,aliquots of MNCs and GCs (6#106 cells) were alsoreacted with anti-CD41, anti-CD61, anti-CD68, andanti-CD38 to establish that the cells scored as tumourdid not express macrophage, monocyte, plasma cell ormegakaryocyte markers.
Positive and negative immunomagnetic selection (IMS).Model experiments and analysis of bone marrowaspirates from patients with advanced head and neckSCC
In model experiments, 20–500 SCC 25 cells (>50 percent react with the Ber-EP4 epitope, Table IV), werepositively selected from 2#107 leucocytes obtainedfrom healthy volunteers using M280 Dynabeads coatedwith monoclonal anti-Ber-EP4 according to the manu-facturer’s instructions (Dynabeads anti-epithelial celldetection kit, Dynal, Oslo, Norway). Twenty, 50, and200 cells were obtained with the aid of a single cellmicromanipulator. Rosetted cells were isolated and sedi-mented onto coated slides for ICC. Since the Ber-EP4antibody used for positive enrichment is attached to theimmunomagnetic beads with a sheep anti-mouse reagentto minimize cross-reactivity, tumour cells isolated usingthis approach were detected with the EPIMET= kit,which utilizes directly conjugated fab fragments of theantibody A45/B/B3. Negative IMS was assessed in simi-lar spiking experiments using anti-CD45-coated M450Dynabeads according to the manufacturer’s protocol. Inthis case, non-rosetted cells were sedimented onto coatedslides and stained with AE1/AE3, diluted 1:50 (Dako),using the APAAP technique described above. Negativecontrols were leucocytes from healthy volunteers,stained with AE1/AE3; positive controls were SCC25 cells.
Bone marrow aspirates from 17 patients with morethan 30 per cent Ber-EP4-positive tumour cells in theprimary lesion (Table IV) were analysed to compare thefrequency of tumour cell detection using the positive andnegative enrichment technique. 6#107 leucocytes wereexamined for each case. Following negative IMS,this protocol yields approximately 2#107 cells for
J. Pathol. 189: 368–377 (1999)
wt
371DISSEMINATED TUMOUR CELLS IN HEAD AND NECK SCC
sedimentation onto ten slides, with approximately 9 cm2
of Cell-Tak tissue adhesive, for ICC and screeningby light microscopy. After positive enrichment, theimmunomagnetic beads and remaining cells were sedi-mented in a similar fashion. Tumour cells were identifiedusing the EPIMET= kit following positive IMS andwith AE1/AE3 after negative enrichment, incorporatingappropriate negative (patient’s sample stained with theisotype-matched IgG) and positive controls (SCC 25cells). However, since ICC revealed that only 50 per centof head and neck SCCs were immunoreactive with theEPIMET= kit (see Results section), when clinicalsamples were analysed, cells which met the stringentmorphological criteria for definition as tumour, butwhich were weakly stained or unstained followingreaction with A45-B/B3 were counted as tumour inthe analysis. 6#106 leucocytes were also examined foreach patient sample, using the standard ICC protocol,
Copyright ? 1999 John Wiley & Sons, Ltd.
ithout enrichment, to compare the efficacy of IMS andhe standard ICC technique.
RESULTS
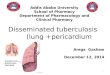
Fig. 1—Representative histograms showing (A) forward scatter (") vs. side scatter (ss) plot and (B) ss vs. fluorescent channel 2 (fl2) log plotidentifying lymphocytes, monocytes, and neutrophils. (C) ss vs. fl2 log plot after spiking SCC 25 cells into buffy coat cells obtained from a healthyvolunteer, followed by DGS. The pellet contains approximately 90 per cent neutrophils and 4·5 per cent lymphocytes and monocytes, whereas theinterface (D) contains approximately 70 per cent monocytes and 1 per cent lymphocytes and neutrophils
Preparation of MNC and GC leucocyte fractions byDGS
When preparing leucocyte subsets by sedimentation oferythrocytes through dextran, tumour cells were onlydetected in the erythrocyte pellet when venous bloodwas spiked with more than 1#105 tumour cells/ml (8–10cells/ml of pellet). No tumour cells were found in theerythrocyte pellet when samples obtained from head andneck cancer patients were examined. Immunophenotyp-ing confirmed that density gradient separation producedefficient separation of MNCs and GCs, and that the
J. Pathol. 189: 368–377 (1999)

372 M. PARTRIDGE ET AL.
MNCs contained less than 5 per cent GCs and the GCsless than 5 per cent MNCs (Fig. 1).
Establishment of criteria for scoring as tumourimmunoreactive cells detected with AE1/AE3 or theEPIMET= kit in the haematopoietic cell compartment
Examination of leucocyte-rich plasma obtained frombone marrow aspirates for 20 individuals without malig-nancy by ICC revealed weakly immunoreactive cellswith AE1/AE3 for 2/20 cases (1–3 cells/6#107 leuco-cytes examined) and for 3/10 patients with haematologi-cal malignancy (1–3 cells/6#107 leucocytes). These rareimmunoreactive cells were generally only weakly posi-tive and of similar size to adjacent haematopoietic cells.Most exhibited haematopoietic cell features. No immu-noreactive cells were seen when AE1/AE3 was used toexamine leucocyte-rich plasma derived from peripheralblood, or after staining leucocytes obtained fromhealthy volunteers with the EPIMET= detectionsystem.
Use of the isotype-matched control antibody to screenleucocytes obtained from healthy volunteers identified2/20 samples with immunoreactive cells (1–2 cells/6#107 leucocytes) and a single patient sample (case 8)with 1–2 immunoreactive cells with typical plasma cellmorphology. In contrast to these false-positive im-munostained cells, epithelial cells identified as tumourlacked recognizable haematopoietic characteristics andwere typically large, often with an irregular shape and ahigh nuclear:cytoplasmic ratio when compared with theMNCs and GCs. The presence of 2–3 immunoreactivecells meeting these criteria in a clinical sample wasconsidered to be helpful when scoring these preparations
Copyright ? 1999 John Wiley & Sons, Ltd.
as tumour-positive. Cases found to have a single immu-noreactive cell or cells which could not be categoricallyidentified as tumour due to morphological overlapbetween tumour and haematopoietic cells were scored asnegative when assessing the results.
Fig. 2—Tumour cell recovery from (a) MNC and (b) GC leucocyte subsets after spiking 2#107 leucocytes obtainedfrom healthy volunteers with 200, 500, 1000, and 5000 tumour cells. The results are the means of triplicateexperiments. The mean and range of tumour cells recovered are shown
Development of a model system to establish whethercells derived from head and neck SCC sediment with theMNC or GC subfractions and analysis of blood obtainedfrom patients with advanced head and neck SCC fordisseminated tumour cells
After spiking leucocytes obtained from healthy volun-teers with varying numbers of cells derived from headand neck SCC lines, the majority of tumour cells wereobserved to sediment with the MNC fraction (Fig. 2a).However, in all cases, tumour cells were also detected inthe GC fraction (Fig. 2b). We did not recover 100 percent of the tumour cell input, as some cells are lostduring DGS and the fixing and washing steps which arean integral part of the ICC protocol. A similar approachwas used to screen 2#107 leucocytes obtained fromblood from patients with advanced head and neck SCC;12/20 samples were found to be tumour-positive, withdisseminated cells being detected in both the MNC andthe GC fraction (range 0–6 tumour cells/2#107 MNCsand 0–5 tumour cells/2#107 GCs, Table I). Dissemi-nated tumour cells were identified in both the MNC andthe GC fraction for seven patients; three cases werefound to have tumour cells in the MNC fraction only;and two cases had tumour cells in the GC fraction only.Four cases had more tumour cells in the GC fractionthan were found following examination of MNCs.Immunophenotyping confirmed that the purity of the
J. Pathol. 189: 368–377 (1999)

373DISSEMINATED TUMOUR CELLS IN HEAD AND NECK SCC
MNC and GC fractions examined in this study was veryhigh, indicating that detection of tumour cells in the GCfraction was not due to contamination of granular cellswith MNCs. Aliquots of leucocytes examined for cases4, 6, and 9 were also reacted with anti-CD41, anti-CD68,anti-CD61 and anti-CD38, but were not found to con-tain cells scored as tumour on the basis of morphologywhich reacted with these reagents (data not shown).
Comparison of positive and negative IMS—modelexperiments and analysis of bone marrow aspirates frompatients with advanced head and neck SCC
The efficiency of tumour cell recovery from leucocytesobtained using protocols incorporating positive andnegative IMS was compared in model experiments. Thenegative enrichment protocol was found to result in therecovery of a higher percentage of the tumour cell inputthan positive IMS (Table II). Similar results were seenusing these protocols to screen leucocytes obtained frombone marrow aspirates from 17 head and neck cancerpatients with more than 30 per cent Ber-EP4-positivetumour cells in the primary lesion (Table III). Dissemi-
Copyright ? 1999 John Wiley & Sons, Ltd.
nated tumour cells were detected for 11/17 casespresenting with advanced malignancy using negativeenrichment techniques, whereas only 2/17 cases werescored as harbouring tumour when positive IMS wasused. When the frequency of tumour detection obtainedwith the standard ICC protocol (no enrichment) andIMS was compared, positive enrichment failed to iden-tify one case with disseminated tumour cells. In contrast,negative IMS identified a further nine cases with atumour-positive bone marrow aspirate.
Table I—Detection of disseminated tumour cells followingexamination of MNC and GC leucocyte fractions frompatients with advanced head and neck SCC by ICC
Caseno.
No. of tumour cells detectedfollowing density gradient separation
MNC fraction GC fraction
1 2 12 0 43 3 24 5 05 4 36 6 27 2 58 0 29 4 0
12 1 215 1 018 4 2
Results obtained following analysis of 2#107 MNCs and GCs.
Table II—Tumour cell detection. Comparison of positive and negative IMS-model experiments
No. of SCC 25/2#107 leucocytes
Positive IMSTumour cell recovery
Negative IMSTumour cell recovery
No enrichmentTumour cell recovery*
20 6 (30%) 11 (55%) 15 (75%)50 11 (22%) 18 (36%) 35 (70%)
200 65 (32%) 126 (63%) 154 (77%)500 140 (28%) 318 (62%) 340 (68%)
Results shown are the means of triplicate experiments. Figures in parentheses have the percentages of tumour inputrecovered.
*2#106 leucocytes were examined using the standard ICC technique, but to facilitate comparison with the resultsobtained using protocols incorporating positive and negative IMS, the results are shown as the number of cells recoveredper 2#107 leucocytes.
Table III—Tumour cell detection. Comparison of positive andnegative IMS: analysis of bone marrow aspirates obtainedfrom patients with advanced SCC. Seventeen cases with morethan 30 per cent Ber-EP4-positive tumour cells were evaluatedusing both positive and negative IMS
Caseno.
No. of tumour cells detected
6#107 leucocytes 6#106 leucocytes
PositiveIMS
NegativeIMS
Noenrichment
1 0 2 02 0 1 03 0 2 14 1 2 05 1 2 16 0 2 17 0 1 08 0 0 09 0 1 0
12 0 1 018 0 1 0
Expression of the Ber-EP4 epitope by head and neckSCCs and reactivity with the EPIMET= epithelial celldetection system and AE1/AE3
Table IV summarizes the results of the IHC and ICCfor the cell lines and head and neck SCCs examined withthe antibodies recognizing surface epitopes and keratinpolypeptides. Strong expression of the Ber-EP4 epitopewas detected for SCC 25 with more than 50 per cent ofthe cells examined showing immunoreactivity. In con-trast, approximately 30 per cent of KB and HN5 cells
J. Pathol. 189: 368–377 (1999)

Table IV—Results obtained ith antibodies recognizing epithelial cell surface epitopes and keratin polypeptides
Head and neck SCC
EP4 MOC-31 AE1/AE3
No. of cases>50%+cells
No. of casespositive
No. of cases>50%+cells
No. of casespositive
No. of cases>50%+cells
Well-differentiated (15) 0 9 1 15 13Moderately differentiated (6 3 2 0 6 3Poorly differentiated (4) 1 2 0 4 1
EP4 MOC-31 AE1/AE3
Head and neck SCC cell lin >50%+cells Expressiondetected
>50%+cells Expressiondetected
>50%+cells
SCC 25 + + + + +KB " + " + +HN 5 " + " + +
374M
.P
AR
TR
IDG
EE
TA
L.
Copyright
?1999
JohnW
iley&
Sons,L
td.J.
Pathol.
189:368–377
(1999)
following staining of head and neck SCCs and cell lines w
Epimet kit Ber-
No. of casespositive
No. of cases>50%+cells
No. of casespositive
11 0 9) 3 0 5
1 0 3
Epimet kit Ber-
es Expressiondetected
>50%+cells Expressiondetected
+ + ++ " ++ " +
375DISSEMINATED TUMOUR CELLS IN HEAD AND NECK SCC
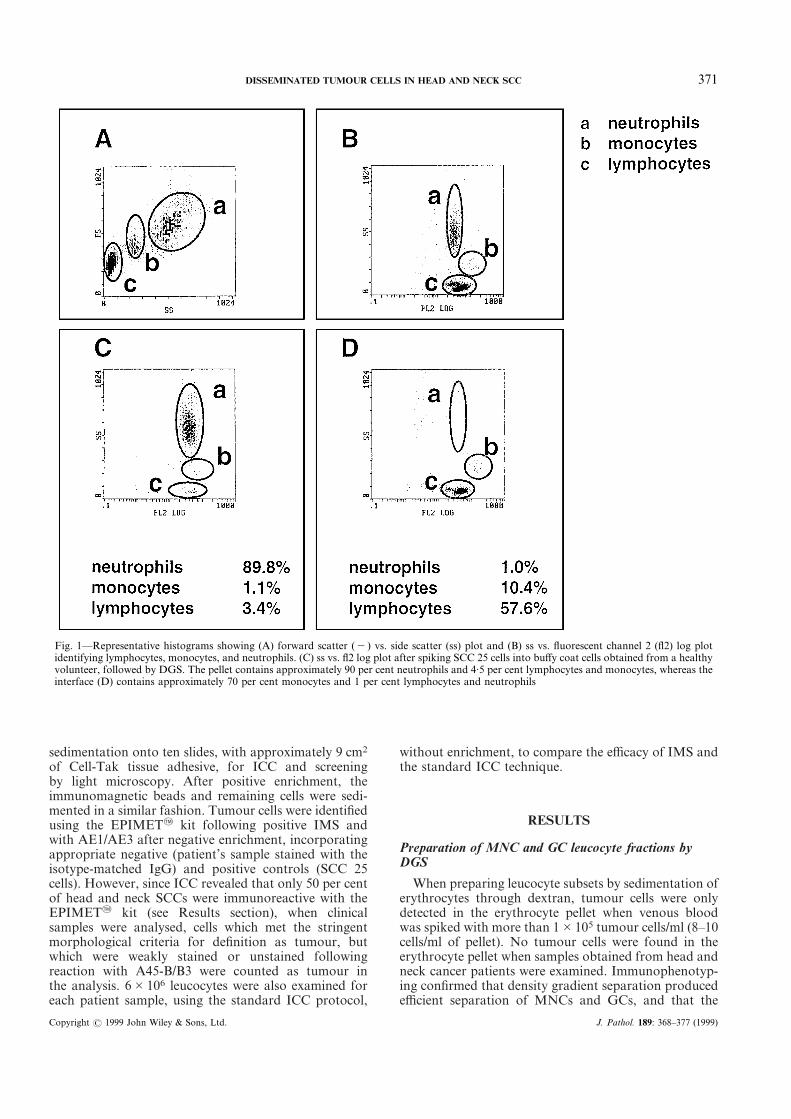
Fig. 3—Detection of tumour cells derived from head and neck SCC in(a) MNC and (b) GC fractions obtained following DGS after spikingtumour cells into leucocytes obtained from healthy volunteers.Tumour cells are identified following ICC using the pan-cytokeratinantibody AE1/AE3. (c) SCC stained with anti-Ber-EP4 showingexpression of this epitope limited to basal and suprabasal cells. Scalebar=100 ìm
were strongly positive, with many cells showing no orweak expression of this epitope. Seventeen of 25 headand neck SCCs were immunoreactive for Ber-EP4; 4/25tumours were scored as having more than 50 per centpositive; and 17/25 tumours were found to contain morethan 30 per cent Ber-EP4-positive tumour cells. Typi-cally, expression of this epitope was confined to theperipheral, basal-type cells of tumours described asbeing well or moderately well differentiated (Fig. 3c).Some patches of Ber-EP4-positive cells were also
Copyright ? 1999 John Wiley & Sons, Ltd.
detected for lesions showing poor differentiation. Asimilar pattern of immunoreactivity was seen with theMOC-31 antibody, which recognizes the same epitope.Eleven of 15 well, 3/6 moderately and 1/4 poorly differ-entiated tumours were positive with the EPIMET= kit,although less than 50 per cent of the cells within eachtissue section were immunoreactive and more than 50per cent positive tumour cells were only detected forSCC 25. In contrast, all SCC lines tested and 17/25 headand neck SCCs showed more than 50 per cent positivecells with AE1/AE3.
DISCUSSION
At present, the UICC TNM tumour classificationsystem is an essential component of the measures usedfor predicting outcome for patients with head and neckcancers, although it does not always provide accurateprognostic information. This failure is due to the sensi-tivity limit of the current methods for detecting thespread of tumour cells and the requirement to takeinto account information about tumour site, histology,tumour size, and tumour biology in addition toconventional TNM criteria, when making importantpredictions about outcome and planning treatment.
Progress in this area can now be made by applyingnew diagnostics to detect small numbers of malignantcells which have spread away from the primary site. Anessential prerequisite for long-term prospective studies isthe development of protocols which are sensitive andspecific for tumour cell detection. It is well recognizedthat ICC methods for detection of tumour cells may leadto the staining of occasional haematopoietic cells. Forexample, 5·3 per cent and 26 per cent of healthy individ-uals have cells in their bone marrow which react withCK219 and AE1/AE3,24 respectively. In the presentstudy, 3/10 bone marrow aspirates obtained frompatients with haematological malignancy and 2/20 frompatients without malignancy had cells which reactedwith AE1/AE3 (Dako). This discrepancy may be relatedto the different ratio of AE1:AE3 in the reagent used inthe present study when compared with the earlierseries.24 A single patient sample (8) and two samplesobtained from healthy volunteers were also found tohave haematopoietic cells which reacted with theisotype-control antibody. A high proportion of immu-noreactive cells detected when leucocytes obtained fromindividuals without cancer are examined have beenshown to react directly with alkaline phosphatase and tostain positive for Igê/ë"light chains,24 findings compat-ible with a plasma cell phenotype. Thus, the immunore-active cells detected in samples obtained from healthyvolunteers stained with the isotype control are mostlikely to be plasma cells synthesizing antibodies toalkaline phosphatase. However, true expression ofcytokeratins by rare haematopoietic cells or cross-reactivity with the primary antibody cannot be excluded.Since plasma cells synthesizing antibodies against alka-line phosphatase are present at only low frequency,Borgen et al.24 recommended that the number of leuco-cytes included in isotype-matched negative controls
J. Pathol. 189: 368–377 (1999)

376 M. PARTRIDGE ET AL.
should equal the number of cells used for specificanti-epithelial staining, and this control has beenincorporated into the protocol for examination ofhaematopoietic cells for patients with head and neckcancer.
Based on the examination of immunostained haem-atopoietic cells from a control group without epithelialmalignancy, we can conclude that the immunoreactivecells detected in patient samples stained with the isotypecontrol are probably also plasma cells, although thepossibilities of cross-reactivity of other haematopoieticcells with the primary antibody, or true cytokeratinexpression by these cells, must also be excluded. Theaddition of morphological assessment of stained cells tothe protocol can confirm the presence of immunoreac-tive haematopoietic cells when positive cells are detectedin the isotype control, and can also minimize the risk ofscoring as tumour contaminating normal squamouscells, or rare cross-reacting haematopoietic cells in anypatient sample. However, scoring some cells as tumourremains a problem, due to the overlap in morphologybetween malignant and haematopoietic cells.
Another factor which must be considered when devel-oping sensitive assays for tumour cell detection is thatthe ability of antibodies to recognize epitopes present ona high proportion of tumour cells must be tested onadequate numbers of primary tumours and cell lines,since expression of the commonly used antigens isheterogeneous (see Table IV and refs 5 and 16) anddifferent when tumours which develop at different sitesare compared. A further problem is that the commonlyused protocols to purify MNCs for the detection ofdisseminated tumour cells involve the use of densitygradient medium. These approaches may not recover allof the malignant cells present in clinical samples. In thisstudy, we have shown that when DGS is used to prepareMNC and GC fractions when tumour cells are spikedinto buffy coat cells, malignant cells sediment preferen-tially with the MNCs, although they may also bedetected in the GC fraction (Fig. 2). Tumour cells werealso detected in the GC fraction when blood obtainedfrom patients with advanced head and neck SCC wasscreened for the presence of tumour cells expressingkeratin polypeptides, for cytological features associatedwith epithelial malignancy, for the absence of haemato-poietic cell morphology, and for the lack of expressionof monocyte, macrophage, plasma cell or megakaryo-cyte markers (Table I). Nine of 12 head and neck cancerpatients with evidence of disseminated tumour in theblood were found to have more tumour cells in theMNC fraction than the GCs, whereas 4/12 cases hadmore malignant cells in the GC fraction. Two cases haddisseminated cells in the GC fraction only (Table I).Most studies screening for disseminated malignant cellsarising from tumours of epithelial surfaces have exam-ined only the MNC fraction.7–10,18–23 However, gradientseparation of keratinocytes through Ficoll is an efficientmethod for separating keratinocytes based on density.29
The findings from this study indicate that tumour cellsmay be missed if only MNCs are examined. We there-fore recommend examination of all buffy coat cells,whole blood or bone marrow aspirates when prospective
Copyright ? 1999 John Wiley & Sons, Ltd.
clinical trials are carried out to establish the prognosticsignificance of disseminated tumour cells for this groupof patients.
Analysis of leucocytes for tumour by ICC is thetechnique most widely used to detect disseminatedmalignant cells,7–10,18–23 but screening 2#106 cells mayfail to detect some cases with malignant cells in thehaematopoietic cell compartment, as the frequency oftumour cells may be very low. Previous study of headand neck cancers has revealed that most patients hadless than 10 tumour cells/106 MNCs analysed, althougha single case had more than 200 cells/106 MNCs.8 Thus,in order to increase the sensitivity of the assay fortumour cell detection, larger numbers of haematopoieticcells need to be screened for the presence of disseminatedtumour.
When central venous blood obtained from head andneck cancer patients was analysed, the frequency oftumour cell detection without the use of enrichmenttechniques was 0–5 tumour cells/2#107 leucocytes(Table I). However, it is not feasible to score thisnumber of leucocytes for every case without incorpor-ating a tumour enrichment technique. Negative IMSincreases the sensitivity of tumour detection; thisapproach makes it feasible to screen more leucocytes fordisseminated malignant cells, because the number ofcells which are sedimented for ICC and screened by lightmicroscopy is reduced by approximately 65 per cent.The alternative approach is to use positive IMS andsediment the beads and remaining cells for ICC. Com-parison of the frequency of tumour cell detection withstandard ICC (no enrichment), and following positive ornegative IMS (Table III), reveals that incorporation ofthe negative enrichment technique when screening bonemarrow aspirates identified nine cases scored as tumour-negative using the standard ICC technique. This illus-trates that this approach, by increasing the number ofleucocytes screened for tumour, has the potential toincrease the sensitivity of tumour cell detection, eventhough some cells are inevitably lost during the process,due to the increased number of manipulations.
When the patient samples were analysed, and inmodel experiments, negative IMS was found to recovera higher percentage of the tumour cell input than thepositive enrichment technique (Tables II and III). Thesediscrepancies are likely to reflect differences in expres-sion of surface antigens by the different tumour types.The antibody which recognizes the Ber-EP4 epitopereacts with two glycopeptides (MW 34 000 and 39 000)present on the surface and in the cytoplasm of someepithelial cells, but does not recognize haematopoieticcells.21 Examination of the distribution of the Ber-EP4antigen for head and neck SCC revealed heterogeneousexpression, with immunoreactivity confined principallyto the outer basal-type cells of clumps of tumour (TableIV and Fig. 3c). Taken together with the results basedon analysing clinical samples (Table III), this suggeststhat heterogeneous expression of the Ber-EP4 glycopep-tide on head and neck tumour cells precludes the use ofthis target for tumour cell detection. Another factorwhich must be considered is the finding that not alltumour cells were detected using the EPIMET= kit,
J. Pathol. 189: 368–377 (1999)

377DISSEMINATED TUMOUR CELLS IN HEAD AND NECK SCC
ACKNOWLEDGEMENTS
We gratefully acknowledge the contribution ofProfessor J. D. Langdon and Mr M. Danford, whoallowed their patients to be recruited to this study; theprovision of technical assistance from Dynal, Oslo,Norway; and thank Dr E. Borgen, Oslo, Norway forhelpful discussion to establish the criteria for diagnosisof disseminated tumour cells.
REFERENCES1. Crile G Jr. Excision of cancer of the head and neck. With special reference
to the plan of dissection based on 132 operations. J Am Med Assoc 1906; 47:1780–1786.
2. Fardy MJ, Langdon JD. The changing pattern of oral cancer 1977–1995.Br J Oral Maxillofac Surg 1995; 33: 328.
3. Zbaren P, Lehmann W. Frequency and sites of distant metastases in headand neck squamous cell carcinoma. Arch Otolaryngol Head Neck Surg 1987;113: 762–764.
4. Parker SL, Tong T, Bolden S, et al. Cancer statistics, 1996. C A Cancer JClin 1996; 46: 5–27.
although due allowance has been made for this whencounting malignant cells.
Our results highlight several issues which must beaddressed when developing sensitive and specific proto-cols for the detection of disseminated tumour in thisgroup of patients. The finding of tumour cells in thehaematopoietic cell compartment for 12/17 assessableadvanced cases (11/17 with a tumour-positive bonemarrow and blood, and a further case with a tumour-positive blood) justifies prospective studies incorporat-ing negative IMS to establish the prognostic significanceof these disseminated tumour cells, but it will also beimportant to establish whether the number of dissemi-nated cells falls post-operatively. Study of other cancertypes suggests that some tumour cells which remain aftersurgery are recognized and destroyed by the immunesystem within 3 months, whereas in other cases, dissemi-nated cells persist after this time and represent trueminimal residual disease.30 In support of the notion thatnot all disseminated tumour cells are clinically signifi-cant, a recent analysis of the changing pattern of headand neck cancer has shown that distant metastases arethe cause of death for 20 per cent of cases,2 whereasapproximately 50 per cent of all head and neck cancerpatients have evidence of disseminated epithelial cells(data from the present study and refs 7 and 8). Theapplication of in vitro techniques to study the geneticcharacteristics of these disseminated cells and establishtheir proliferative capacity will also provide new insightinto heterogeneity within the tumour cell population.Taken together, the results from these studies shouldhelp to identify patients with disseminated tumourcells which are the true micrometastases, capable offorming new attachments and proliferating to form newfoci of tumour if the local environment is suitable—aninteraction commonly referred to as the seed and soilhypothesis.31
Copyright ? 1999 John Wiley & Sons, Ltd.
5. Pantel K, Izbicki R, Angstwurm M, et al. Immunocytological detection ofbone marrow micrometastasis in operable non-small cell lung cancer.Cancer Res 1993; 53: 1027–1031.
6. Naume B, Borgen E, Beiske K, et al. Immunomagnetic techniques for theenrichment and detection of isolated breast carcinoma cells in bone marrowand peripheral blood. J Haematother 1997; 6: 103–114.
7. Wollenberg B, Ollesch A, Maag K, et al. Micrometastases in bone marrowof patients with squamous cell carcinoma of the head and neck. LaryngoRhino Otol 1994; 73: 88–93.
8. Gath HJ, Heissler E, Hell B, et al. Immunocytologic detection of isolatedtumour cells in bone marrow of patients with squamous cell carcinomas ofthe head and neck region. Int J Oral Maxillofac Surg 1995; 24: 351–355.
9. Neuramier M, Gerhard M, Wagener C. Diagnosis of disseminated epithelialcells by the amplification of tissue-specific genes. Gene 1995; 159: 43–47.
10. Soeth E, Vogel I, Roder C, et al. Comparative analysis of bone marrow andvenous blood isolates from gastrointestinal cancer patients for the detectionof disseminated tumour cells using reverse transcription PCR. Cancer Res1997; 57: 3106–3110.
11. Nawroz H, Koch W, Anker P, et al. Microsatellite alterations in serumDNA of head and neck cancer patients. Nature Med 1996; 2: 1035–1037.
12. Schulz J, Ermich T, Kasper M, et al. Cytokeratin pattern of clinically intactand pathologically changed oral mucosa. Int J Oral Maxillofac Surg 1992;21: 35–39.
13. Ogden GR, Chisholm DM, Adi M, et al. Cytokeratin expression in oralcancer and its relationship to tumour differentiation. J Oral Pathol Med1993; 22: 82–86.
14. Traweek ST, Liu J, Battifora H. Keratin expression in non-epithelial tissues.Am J Pathol 1993; 142: 1111–1118.
15. Braun B, Muller M, Hepp F, et al. Micrometastatic breast cancer cells inbone marrow at primary surgery; prognostic value in comparison withnodal status. J Natl Cancer Inst 1998; 90: 1099–1100.
16. Jauch KW, Friess S, Grutzner U, et al. Prognostic significance of dissemi-nated epithelial cells. Oncologie 1995; 18: 525–532.
17. Diel IJ, Kaufmann M, Costa SD, et al. Micrometastatic breast cancer cellsin bone marrow at primary surgery: prognostic value in comparison withnodal status. J Natl Cancer Inst 1996; 88: 1652–1658.
18. Funke I, Schraut W. Meta analyses of studies on bone marrow micromet-astases: an independent prognostic impact remains to be substantiated.J Clin Oncol 1998; 16: 557–566
19. Pantel K, Schlimok G, Angstwurm M, et al. Methodological analysis ofimmunocytochemical screening for disseminated epithelial tumour cells inbone marrow. J Hematother 1994; 3: 165–173.
20. Schlimok G, Dunke I, Pantel KS, et al. Micrometastatic tumour cells inbone marrow in patients with gastric cancer: methodological aspects ofdetection and prognostic significance. Eur J Cancer 1991; 27: 1461–1465.
21. Diel IJ, Kaufmann M, Goerner R, et al. Detection of tumour cells in bonemarrow of patients with primary breast cancer: a prognostic factor fordistant metastasis. J Clin Oncol 1992; 10: 1534–1539.
22. Lindemann F, Schimlok G, Dirschedl P, et al. Prognostic significance ofmicrometastatic cells in bone marrow of colorectal cancer patients. Lancet1992; 340: 685–689.
23. Harbeck N, Untch M, Pache L, et al. Tumour cell detection in the bonemarrow of breast cancer patients at primary therapy: results of a 3 yearmedian follow up. Br J Cancer 1994; 69: 566–571.
24. Borgen E, Beiske K, Trachsel S, et al. Immunocytological detection ofisolated epithelial cells in bone marrow: non-specific staining and contri-bution by plasma cells directly reactive to alkaline phosphatase. J Pathol1998; 185: 427–434
25. Rheinwald JG Beckett MA. Tumourigenic keratinocyte lines requiringanchorage and fibroblast support from cultured human squamous cellcarcinomas. Cancer Res 1981; 41: 1657–1663.
26. Easty DM, Easty GC, Carter RL, et al. Ten human carcinoma cell linesderived from squamous carcinomas of the head and neck. Br J Cancer 1981;43: 772–779.
27. Theocharous P, Lowdell MW, Jones AL, et al. Immunocytochemicaldetection of breast cancer cells: a comparison of three attachment factors.J Hematother 1997; 6: 21–29.
28. Partridge M, Kiguwa S, Emilion GG, et al. Expression of bFGF, KGF andreceptors on normal oral mucosa and SCC. Eur J Cancer, Oral Oncol 1996;32: 76–82.
29. Fischer SM, Nelson KDG, Reiners JJ, et al. Separation of epidermal cellsby density centrifugation: a new technique for studies on normal andpathological differentiation. J Cut Pathol 1982; 4: 43–49.
30. O’Sullivan GC, Collins JK, Kelly J, et al. Micrometastases: marker ofmetasiatic potential or evidence of residual disease? Gut 1977; 40: 512–515.
31. Paget S. The distribution of secondary growth in cancer of the breast.Lancet 1889; i: 571–573.
J. Pathol. 189: 368–377 (1999)