Embed Size (px)
Citation preview
General Recommendations on Immunization
9
2
This chapter discusses issues that are commonly encountered in vaccination practice. A more thorough discussion of issues common to more than one vaccine can be found in the General Recommendations on Immunization: Recommendations of the Advisory Committee on Immunization Practices. These recommendations are revised every 3 to 5 years as needed; the most current edition was published in January 2011 (MMWR 2011;60 (No. RR-2):1-61). All providers who administer vaccine should have a copy of this report and be familiar with its content. It can be downloaded from the MMWR website or ordered in print version from the Centers for Disease Control and Prevention.
Timing and Spacing of VaccinesThe timing and spacing of vaccine doses are two of the most important issues in the appropriate use of vaccines. Specific circumstances that are commonly encountered in immunization practice are the timing of antibody-containing blood products and live vaccines (particularly measles and varicella-containing vaccines), simultaneous and nonsimulta-neous administration of different vaccines, and the interval between subsequent doses of the same vaccine.
General Rule: Inactivated vaccines are generally not affected by circulating antibody to the antigen. Live attenuated vaccines may be affected by circulating antibody to the antigen.
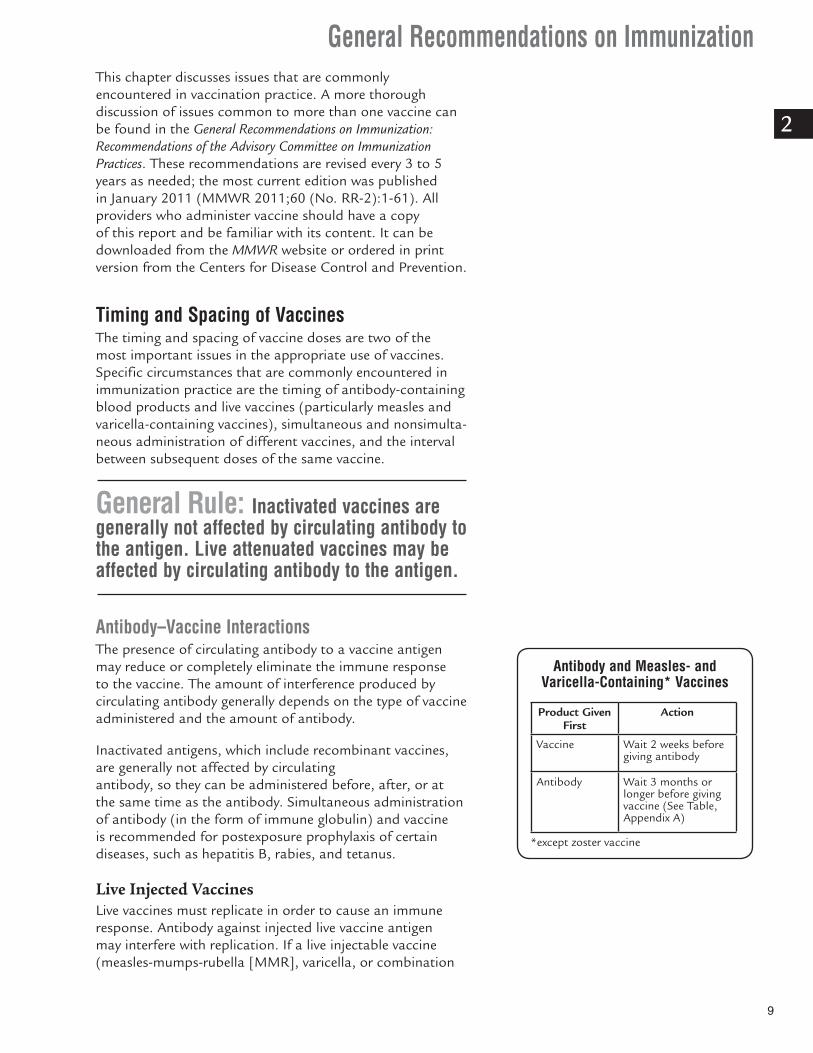
Antibody–Vaccine Interactions The presence of circulating antibody to a vaccine antigen may reduce or completely eliminate the immune response to the vaccine. The amount of interference produced by circulating antibody generally depends on the type of vaccine administered and the amount of antibody.
Inactivated antigens, which include recombinant vaccines, are generally not affected by circulating antibody, so they can be administered before, after, or at the same time as the antibody. Simultaneous administration of antibody (in the form of immune globulin) and vaccine is recommended for postexposure prophylaxis of certain diseases, such as hepatitis B, rabies, and tetanus.
Live Injected VaccinesLive vaccines must replicate in order to cause an immune response. Antibody against injected live vaccine antigen may interfere with replication. If a live injectable vaccine (measles-mumps-rubella [MMR], varicella, or combination
Antibody and Measles- and Varicella-Containing* Vaccines
Product Given First
Action
Vaccine Wait 2 weeks before giving antibody
Antibody Wait 3 months or longer before giving vaccine (See Table, Appendix A)
*except zoster vaccine

10
General Recommendations on Immunization
2
measles-mumps-rubella-varicella [MMRV]) must be given around the time that antibody is given, the two must be separated by enough time so that the antibody does not interfere with viral replication. If the live vaccine is given first, it is necessary to wait at least 2 weeks (i.e., an incubation period) before giving the antibody. If the interval between the vaccine and antibody is less than 2 weeks, the recipient should be tested for immunity or the vaccine dose should be repeated.
If the antibody is given before a dose of MMR or varicella-containing vaccine, it is necessary to wait until the antibody has waned (degraded) before giving the vaccine to reduce the chance of interference by the antibody. The necessary interval between an antibody-containing product and MMR or varicella-containing vaccine (except zoster vaccine) depends on the concentration of antibody in the product, but is always 3 months or longer. A table listing the recommended intervals between administration of antibody products and live vaccines (MMR and varicella-containing) is included in Appendix A and in the General Recommendations on Immunization (2011). The interval between administration of an antibody product and MMR or varicella vaccination can be as long as 11 months. Zoster vaccine is not known to be affected by circulating antibody so it can be administered at any time before or after receipt of an antibody-containing blood product.
Yellow fever vaccine also is not known to be affected by circulating antibody. Because few North Americans are immune to yellow fever, these products do not contain significant amounts of antibody to yellow fever virus.
Although passively acquired antibodies can interfere with the response to rubella vaccine, the low dose of anti-Rho(D) globulin administered to postpartum women has not been demonstrated to reduce the response to the rubella vaccine. Because of the importance of rubella and varicella immunity among childbearing age women, women without evidence of immunity to rubella or varicella should receive MMR or varicella vaccine (but not MMRV) in the postpartum period. Vaccination should not be delayed because of receipt of anti-Rho(D) globulin or any other blood product during the last trimester of pregnancy or at delivery. These women should be vaccinated immediately after delivery and, if possible, tested 3 months later to ensure immunity to rubella and, if necessary, to measles.
Live Oral and Intranasal VaccinesOral typhoid vaccine is not known to be affected by the administration of immune globulin or blood products. Oral typhoid vaccine may be given simultaneously with blood products, or separated by any interval. The replication of
General Recommendations on Immunization
11
2
live attenuated influenza (LAIV) and rotavirus vaccines are not believed to be affected by antibody-containing blood products. These can be given any time before or after administration of antibody-containing blood products.
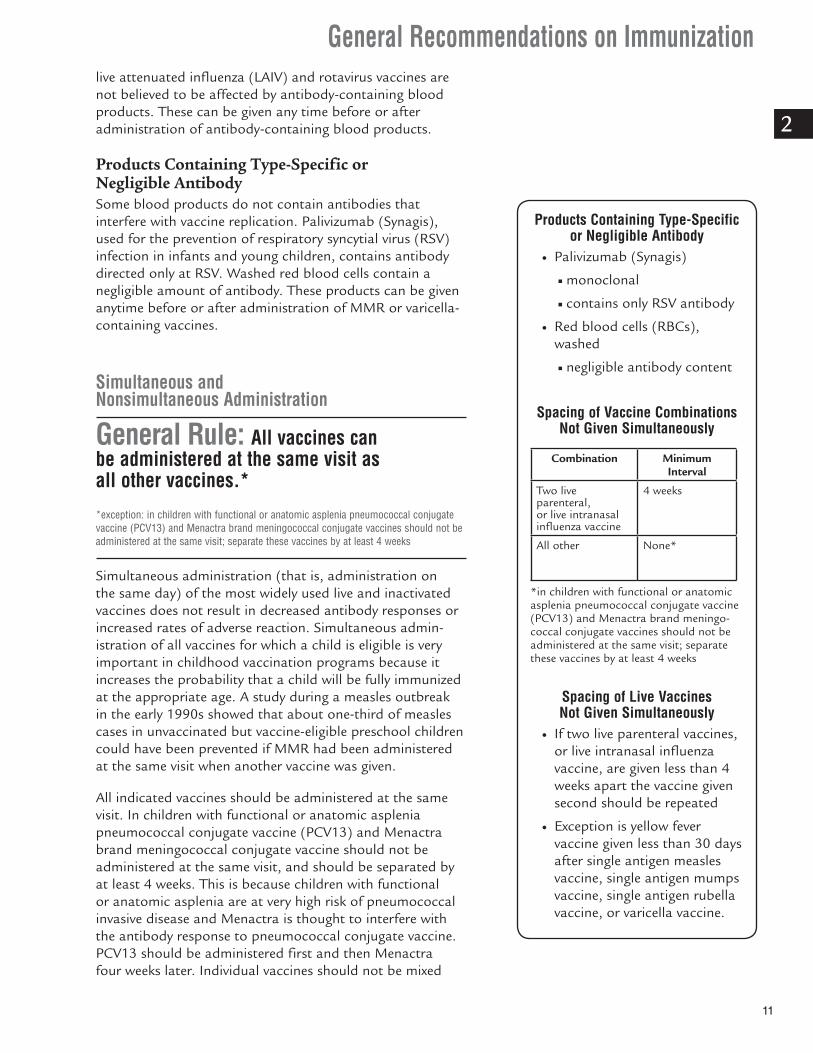
Products Containing Type-Specific or Negligible AntibodySome blood products do not contain antibodies that interfere with vaccine replication. Palivizumab (Synagis), used for the prevention of respiratory syncytial virus (RSV) infection in infants and young children, contains antibody directed only at RSV. Washed red blood cells contain a negligible amount of antibody. These products can be given anytime before or after administration of MMR or varicella-containing vaccines.
Simultaneous and Nonsimultaneous Administration
General Rule: All vaccines can be administered at the same visit as all other vaccines.*
*exception: in children with functional or anatomic asplenia pneumococcal conjugate vaccine (PCV13) and Menactra brand meningococcal conjugate vaccines should not be administered at the same visit; separate these vaccines by at least 4 weeks
Simultaneous administration (that is, administration on the same day) of the most widely used live and inactivated vaccines does not result in decreased antibody responses or increased rates of adverse reaction. Simultaneous admin-istration of all vaccines for which a child is eligible is very important in childhood vaccination programs because it increases the probability that a child will be fully immunized at the appropriate age. A study during a measles outbreak in the early 1990s showed that about one-third of measles cases in unvaccinated but vaccine-eligible preschool children could have been prevented if MMR had been administered at the same visit when another vaccine was given.
All indicated vaccines should be administered at the same visit. In children with functional or anatomic asplenia pneumococcal conjugate vaccine (PCV13) and Menactra brand meningococcal conjugate vaccine should not be administered at the same visit, and should be separated by at least 4 weeks. This is because children with functional or anatomic asplenia are at very high risk of pneumococcal invasive disease and Menactra is thought to interfere with the antibody response to pneumococcal conjugate vaccine. PCV13 should be administered first and then Menactra four weeks later. Individual vaccines should not be mixed
Products Containing Type-Specific or Negligible Antibody
● Palivizumab (Synagis)
■ monoclonal
■ contains only RSV antibody
● Red blood cells (RBCs), washed
■ negligible antibody content
Spacing of Vaccine Combinations Not Given Simultaneously
Combination Minimum Interval
Two live parenteral, or live intranasal influenza vaccine
4 weeks
All other None*
*in children with functional or anatomic asplenia pneumococcal conjugate vaccine (PCV13) and Menactra brand meningo-coccal conjugate vaccines should not be administered at the same visit; separate these vaccines by at least 4 weeks
Spacing of Live Vaccines Not Given Simultaneously
● If two live parenteral vaccines, or live intranasal influenza vaccine, are given less than 4 weeks apart the vaccine given second should be repeated
● Exception is yellow fever vaccine given less than 30 days after single antigen measles vaccine, single antigen mumps vaccine, single antigen rubella vaccine, or varicella vaccine.

12
General Recommendations on Immunization
2
in the same syringe unless they are licensed for mixing by the Food and Drug Administration. Only the sanofi-pasteur DTaP-IPV/Hib (Pentacel) vaccine is licensed for mixing in the same syringe. For additional guidelines, see the Vaccine Administration chapter.
Combination vaccines are generally preferred over simul-taneous administration of single component vaccines. Considerations should include an assessment of the number of injections, vaccine availability, likelihood of improved coverage, likelihood of patient return, and storage and costs. Considerations should also include patient choice and the potential for adverse events. Because of the increased risk of febrile seizures following the first dose of MMRV vaccine compared to MMR and varicella vaccines, for the first dose of vaccine to prevent measles, mumps, rubella and varicella, unless the parent or caregiver expresses a preference for MMRV vaccine, separate MMR and Varicella vaccines should be administered for children 12 through 47 months of age.
Nonsimultaneous Administration of Different VaccinesIf live parenteral (injected) vaccines (MMR, MMRV, varicella, zoster, and yellow fever) and live intranasal influenza vaccine (LAIV) are not administered at the same visit, they should be separated by at least 4 weeks. This interval is intended to reduce or eliminate interference from the vaccine given first on the vaccine given later. If two live parenteral vaccines or LAIV are administered at an interval of less than 4 weeks, then the vaccine given second should be repeated in 4 weeks or confirmed to have been effective by serologic testing of the recipient (serologic testing is not recommended following LAIV, varicella, or zoster vaccines). An exception to this recommendation is yellow fever vaccine administered less than 4 weeks after single-antigen measles vaccine. A 1999 study demonstrated that yellow fever vaccine is not affected by measles vaccine given 1–27 days earlier. The effect of nonsimultaneously administered yellow fever vaccine with each of the following vaccines: mumps; varicella; zoster; LAIV; and rubella is not known. So doses of mumps, varicella, zoster, LAIV, and rubella, when adminis-tered less than 30 days prior to yellow fever vaccine, can be counted.
Live vaccines administered by the oral route (oral polio vaccine [OPV] oral typhoid, and rotavirus) are not believed to interfere with each other if not given simultaneously. These vaccines may be given at any time before or after each other. Rotavirus vaccine is not approved for children older than 32 weeks, oral typhoid is not approved for children younger than 6 years of age, and OPV is no longer available in the United States, so these vaccines are not likely to be given to the same child.

General Recommendations on Immunization
13
2
Parenteral live vaccines (MMR, MMRV, varicella, zoster, and yellow fever) and LAIV are not believed to have an effect on live vaccines given by the oral route (OPV, oral typhoid, and rotavirus). Live oral vaccines may be given at any time before or after live parenteral vaccines or LAIV.
All other combinations of two inactivated vaccines, or live and inactivated vaccines, may be given at any time before or after each other. In children with functional or anatomic asplenia PCV13 and Menactra brand meningococcal conjugate vaccine should not be administered at the same visit.
Interval Between Doses of the Same Vaccine Immunizations are recommended for members of the youngest age group at risk for a disease for whom efficacy and safety of a vaccine have been demonstrated.
General Rule: Increasing the interval between doses of a multidose vaccine does not diminish the effectiveness of the vaccine.*Decreasing the interval between doses of a multidose vaccine may interfere with antibody response and protection.
*after the series has been completed
Most vaccines in the childhood immunization schedule require two or more doses for development of an adequate and persisting antibody response. Studies have demon-strated that recommended ages and intervals between doses of the same antigen(s) provide optimal protection or have the best evidence of efficacy. Table 1 of the General Recommendations on Immunization (included in Appendix A) shows the recommended and minimal ages and intervals between doses of vaccines most frequently used in the United States.
Administering doses of a multidose vaccine at shorter than the recommended intervals might be necessary when an infant or child is behind schedule and needs to be brought up-to-date quickly or when international travel is pending. In these cases, an accelerated schedule using the minimum age or minimum interval criteria can be used. Accelerated schedules should not be used routinely.
For routine vaccination, vaccine doses should not be admin-istered at intervals less than the recommended minimal intervals or earlier than the minimal ages. Two exceptions to this may occur. The first is for measles vaccine during a measles outbreak or before travelling abroad. Infants 6
Minimum Intervals and AgesVaccine doses should not be administered at intervals less than the minimum intervals or earlier than the minimum age
14
General Recommendations on Immunization
2
through 11 months should receive one MMR dose, and this dose should not be counted (should be repeated at 12 months of age or older). The second exception involves administering a dose a few days earlier than the minimum interval or age, which is unlikely to have a substantially negative effect on the immune response to that dose. Although vaccinations should not be scheduled at an interval or age less than the recommended minimums, a child may have erroneously been brought to the office early, or may have come for an appointment not specifically for vaccination. In these situations, the clinician can consider administering the vaccine earlier than the minimum interval or age. If the parent/child is known to the clinician and the physician has confidence that the child will return for a visit, it is preferable to reschedule the child for vaccination closer to the recommended interval. If the parent/child is not known to the clinician or is not reliable (e.g., habitually misses appointments), it may be preferable to administer the vaccine at that visit than to reschedule a later appointment that may not be kept.
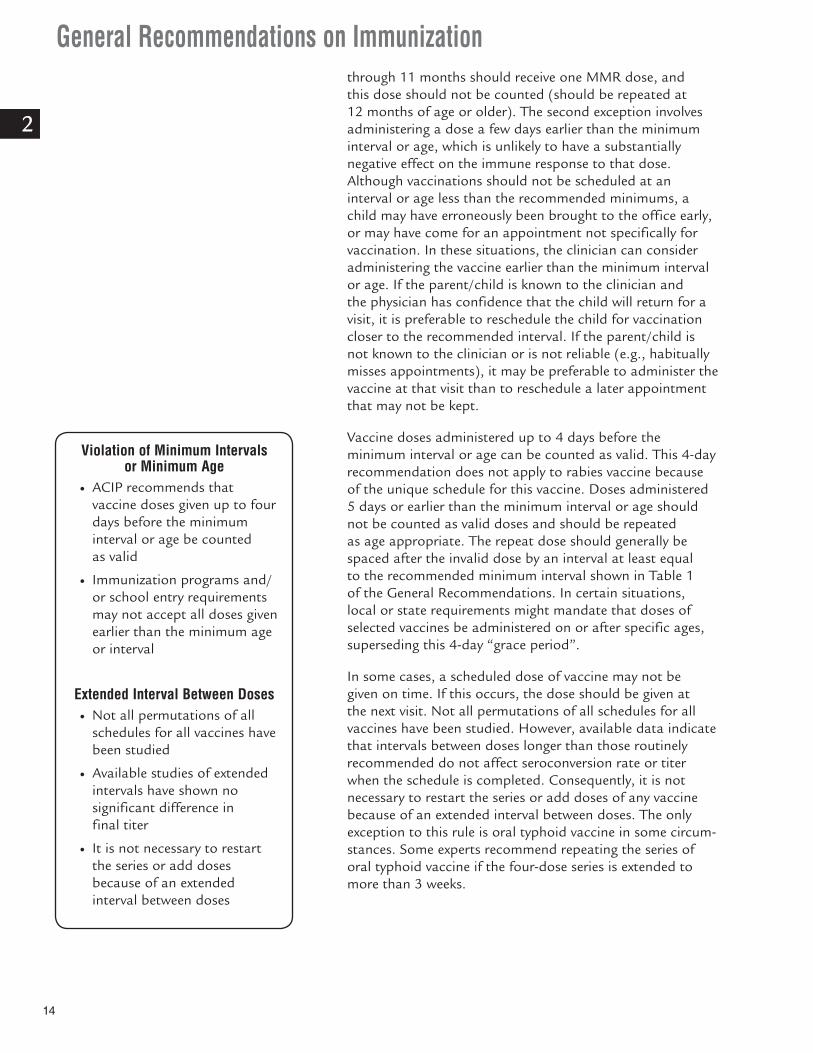
Vaccine doses administered up to 4 days before the minimum interval or age can be counted as valid. This 4-day recommendation does not apply to rabies vaccine because of the unique schedule for this vaccine. Doses administered 5 days or earlier than the minimum interval or age should not be counted as valid doses and should be repeated as age appropriate. The repeat dose should generally be spaced after the invalid dose by an interval at least equal to the recommended minimum interval shown in Table 1 of the General Recommendations. In certain situations, local or state requirements might mandate that doses of selected vaccines be administered on or after specific ages, superseding this 4-day “grace period”.
In some cases, a scheduled dose of vaccine may not be given on time. If this occurs, the dose should be given at the next visit. Not all permutations of all schedules for all vaccines have been studied. However, available data indicate that intervals between doses longer than those routinely recommended do not affect seroconversion rate or titer when the schedule is completed. Consequently, it is not necessary to restart the series or add doses of any vaccine because of an extended interval between doses. The only exception to this rule is oral typhoid vaccine in some circum-stances. Some experts recommend repeating the series of oral typhoid vaccine if the four-dose series is extended to more than 3 weeks.
Violation of Minimum Intervals or Minimum Age
● ACIP recommends that vaccine doses given up to four days before the minimum interval or age be counted as valid
● Immunization programs and/or school entry requirements may not accept all doses given earlier than the minimum age or interval
Extended Interval Between Doses ● Not all permutations of all
schedules for all vaccines have been studied
● Available studies of extended intervals have shown no significant difference in final titer
● It is not necessary to restart the series or add doses because of an extended interval between doses
General Recommendations on Immunization
15
2
Number of DosesFor live injected vaccines, the first dose administered at the recommended age usually provides protection. An additional dose is given to provide another opportunity for vaccine response in the small proportion of recipients who do not respond to the first dose. For instance, approximately 95% of recipients will respond to a single dose of measles vaccine. The second dose is given to ensure that nearly 100% of persons are immune (i.e., the second dose is “insurance”). Immunity following live vaccines is long-lasting, and booster doses are not necessary.
For inactivated vaccines, the first dose administered at the recommended age usually does not provide protection (hepatitis A vaccine is an exception). A protective immune response may not develop until the second or third dose. For inactivated vaccines, antibody titers may decrease (wane) below protective levels after a few years. This phenomenon is most notable for pertussis vaccine; tetanus and diphtheria vaccine immunity also wanes. For these vaccines, periodic “boosting” is required. An additional dose is given to raise antibody back to protective levels.
Not all inactivated vaccines require boosting throughout life. For example, additional doses of Hib vaccine are not required after completion of the infant primary series and 12-15 month old booster dose because Hib disease is very rare in children older than 5 years of age. Hepatitis B vaccine does not require boosting because of immunologic memory to the vaccine and the long incubation period of hepatitis B (which can produce an “autoboost”).
Adverse Reactions Following VaccinationVaccines are intended to produce active immunity to specific antigens. An adverse reaction is an untoward effect caused by a vaccine that is extraneous to the vaccine’s primary purpose of producing immunity. Adverse reactions are also called vaccine side effects. A vaccine adverse event refers to any medical event that occurs following vaccination. An adverse event could be a true adverse reaction or just a coin-cidental event, with further research needed to distinguish between them.
Acute vaccine adverse reactions fall into three general categories: local, systemic, and allergic. The most common type of adverse reactions are local reactions, such as pain, swelling, and redness at the site of injection. Local reactions may occur with up to 80% of vaccine doses, depending on the type of vaccine. Local adverse reactions generally occur within a few hours of the injection and are usually mild and self-limited. On rare occasions, local reactions may be very exaggerated or severe. Some of these reactions, referred to
Vaccine Adverse Reactions ● Adverse reaction
■ extraneous effect caused by vaccine
■ side effect
● Adverse event
■ any medical event following vaccination
■ may be true adverse reaction
■ may be only coincidental
● Local adverse reactions
■ pain, swelling, redness at site of injection
■ occur within a few hours of injection
■ usually mild and self-limited
● Systemic adverse reactions
■ fever, malaise, headache
■ nonspecific
■ may be unrelated to vaccine
● Severe allergic (anaphylaxis)
■ due to vaccine or vaccine component
■ rare
■ risk minimized by screening

16
General Recommendations on Immunization
2
as Arthus reactions, are most frequently seen with diphtheria and tetanus toxoids. Arthus reactions are not allergic reactions. Arthus reactions are believed to be due to very high titers of antibody, usually caused by too many doses of toxoid.
Systemic adverse reactions are more generalized events and include fever, malaise, myalgias (muscle pain), headache, loss of appetite, and others. These symptoms are nonspecific; they may occur in vaccinated persons because of the vaccine or may be caused by something unrelated to the vaccine.
Systemic adverse reactions were relatively frequent with DTP vaccine, which contained a whole-cell pertussis component. However, comparison of the frequency of systemic adverse events among vaccine and placebo recipients shows they are less common with inactivated vaccines currently in use, including acellular pertussis vaccine.
Systemic adverse reactions may occur following receipt of live attenuated vaccines. Live attenuated vaccines must replicate in order to produce immunity. The adverse reactions that follow live attenuated vaccines, such as fever or rash, represent symptoms produced from viral replication and are similar to a mild form of the natural disease. Systemic adverse reactions following live vaccines are usually mild, and occur 3–21 days after the vaccine was given (i.e., after an incubation period of the vaccine virus). LAIV replicates in the mucous membranes of the nose and throat, not in the lungs. As a result, LAIV may cause upper respiratory symptoms (like a cold) but not influenza-like symptoms.
A third type of acute vaccine adverse reactions are allergic reactions. Allergic reactions may be caused by the vaccine antigen itself or some other component of the vaccine, such as cell culture material, stabilizer, preservative, or antibiotic used to inhibit bacterial growth. Severe allergic reactions (anaphylaxis) may be life-threatening. Fortunately, they are rare. The risk of an allergic reaction can be decreased by good screening prior to vaccination. All providers who administer vaccines must have an emergency protocol and supplies to treat anaphylaxis.
Reporting Vaccine Adverse Events Providers should report any clinically significant adverse event that occurs after the administration of any vaccine licensed in the United States to the Vaccine Adverse Event Reporting System (VAERS), which includes reporting from both public and private sectors.
Live Attenuated Vaccines ● Must replicate to
produce immunity
● Symptoms usually mild
● Occur after an incubation period (usually 3-21 days)
General Recommendations on Immunization
17
2
Providers should report a clinically significant adverse event even if they are unsure whether a vaccine caused the event. The telephone number to call for answers to questions and to obtain VAERS forms is (800) 822-7967, or visit the VAERS website at http://vaers.hhs.gov. VAERS accepts reports of adverse reactions through their online system.
Contraindications and Precautions to VaccinationContraindications and precautions to vaccination generally dictate circumstances when vaccines will not be given. Many contraindications and precautions are temporary, and the vaccine can be given at a later time.
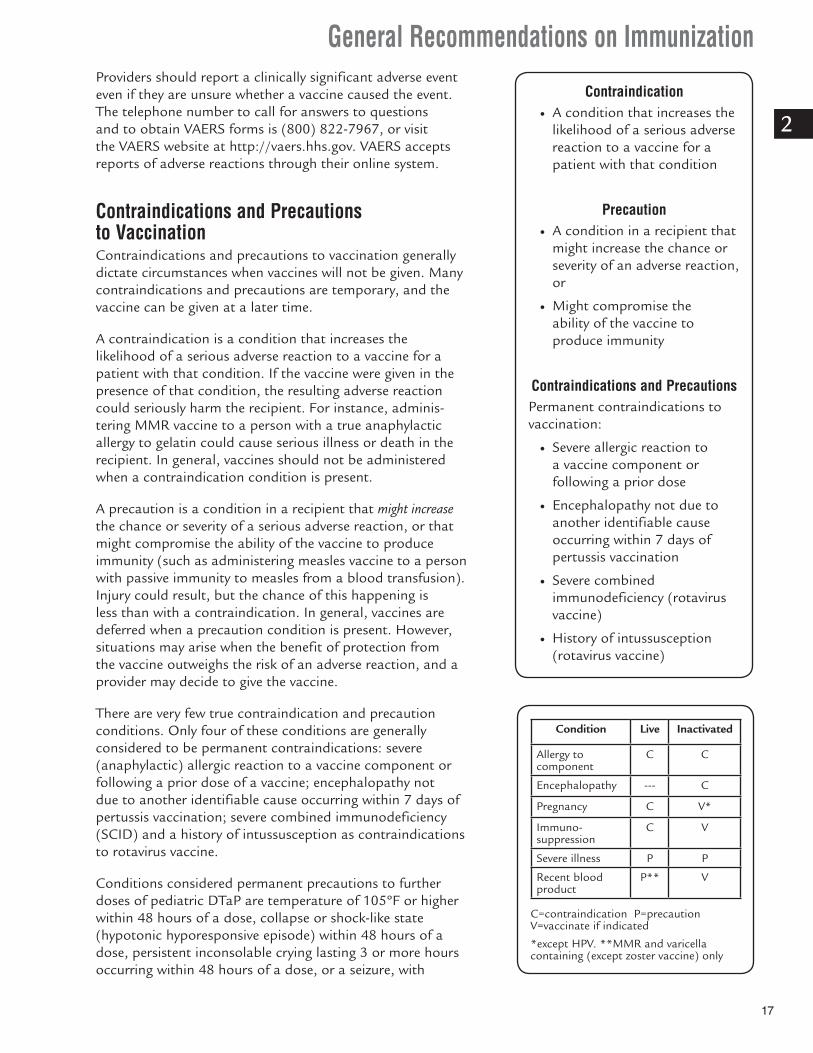
A contraindication is a condition that increases the likelihood of a serious adverse reaction to a vaccine for a patient with that condition. If the vaccine were given in the presence of that condition, the resulting adverse reaction could seriously harm the recipient. For instance, adminis-tering MMR vaccine to a person with a true anaphylactic allergy to gelatin could cause serious illness or death in the recipient. In general, vaccines should not be administered when a contraindication condition is present.
A precaution is a condition in a recipient that might increase the chance or severity of a serious adverse reaction, or that might compromise the ability of the vaccine to produce immunity (such as administering measles vaccine to a person with passive immunity to measles from a blood transfusion). Injury could result, but the chance of this happening is less than with a contraindication. In general, vaccines are deferred when a precaution condition is present. However, situations may arise when the benefit of protection from the vaccine outweighs the risk of an adverse reaction, and a provider may decide to give the vaccine.
There are very few true contraindication and precaution conditions. Only four of these conditions are generally considered to be permanent contraindications: severe (anaphylactic) allergic reaction to a vaccine component or following a prior dose of a vaccine; encephalopathy not due to another identifiable cause occurring within 7 days of pertussis vaccination; severe combined immunodeficiency (SCID) and a history of intussusception as contraindications to rotavirus vaccine.
Conditions considered permanent precautions to further doses of pediatric DTaP are temperature of 105ºF or higher within 48 hours of a dose, collapse or shock-like state (hypotonic hyporesponsive episode) within 48 hours of a dose, persistent inconsolable crying lasting 3 or more hours occurring within 48 hours of a dose, or a seizure, with
Contraindication ● A condition that increases the
likelihood of a serious adverse reaction to a vaccine for a patient with that condition
Precaution ● A condition in a recipient that
might increase the chance or severity of an adverse reaction, or
● Might compromise the ability of the vaccine to produce immunity
Contraindications and PrecautionsPermanent contraindications to vaccination:
● Severe allergic reaction to a vaccine component or following a prior dose
● Encephalopathy not due to another identifiable cause occurring within 7 days of pertussis vaccination
● Severe combined immunodeficiency (rotavirus vaccine)
● History of intussusception (rotavirus vaccine)
Condition Live Inactivated
Allergy to component
C C
Encephalopathy --- C
Pregnancy C V*
Immuno- suppression
C V
Severe illness P P
Recent blood product
P** V
C=contraindication P=precaution V=vaccinate if indicated
*except HPV. **MMR and varicella containing (except zoster vaccine) only

18
General Recommendations on Immunization
2
or without fever, occurring within 3 days of a dose. The occurrence of one of these events in a child following DTaP vaccine is not a precaution to later vaccination with the adolescent/adult formulation of pertussis vaccine (Tdap).
Two conditions are temporary precautions to vaccination: moderate or severe acute illness (all vaccines), and recent receipt of an antibody-containing blood product. The latter precaution applies only to MMR and varicella-containing (except zoster) vaccines. Two conditions are temporary contraindications to vaccination with live vaccines: pregnancy and immunosuppression.
Allergy A severe (anaphylactic) allergic reaction following a dose of vaccine will almost always contraindicate a subsequent dose of that vaccine. Anaphylactic reactions are those that are mediated by IgE, occur within minutes or hours of receiving the vaccine, and require medical attention. Examples of symptoms and signs typical of anaphylactic reactions are generalized urticaria (hives), swelling of the mouth and throat, difficulty breathing, wheezing, hypotension, or shock. These reactions are very rare following vaccination and can be further minimized with appropriate screening.
A table listing vaccine contents is included in Appendix B. Persons may be allergic to the vaccine antigen or to a vaccine component such as animal protein, antibiotic, preservative, or stabilizer. The most common animal protein allergen is egg protein found in vaccines prepared using embryonated chicken eggs (e.g., yellow fever and influenza vaccines). Ordinarily, a person who can eat eggs or egg products can receive vaccines that contain egg; persons with histories of anaphylactic or anaphylactic-like allergy to eggs or egg proteins should be referred for further evaluation. Asking persons whether they can eat eggs without adverse effects is a reasonable way to screen for those who might be at risk from receiving yellow fever and egg-containing influenza vaccines.
Studies have shown that children who have a history of severe allergy to eggs rarely have reactions to MMR vaccine. This is probably because measles and mumps vaccine viruses are both grown in chick embryo fibroblasts, not actually in eggs. It appears that gelatin, not egg, might be the cause of allergic reactions to MMR. As a result, in 1998, the ACIP removed severe egg allergy as a contraindication to measles and mumps vaccines. Egg-allergic children may be vaccinated with MMR without prior skin testing.
Certain vaccines contain trace amounts of neomycin. Persons who have experienced an anaphylactic reaction to neomycin should not receive these vaccines. Most often,

General Recommendations on Immunization
19
2
neomycin allergy presents as contact dermatitis, a manifes-tation of a delayed-type (cell-mediated) immune response, rather than anaphylaxis. A history of delayed-type reactions to neomycin is not a contraindication for administration of vaccines that contain neomycin.
Latex is sap from the commercial rubber tree. Latex contains naturally occurring impurities (e.g., plant proteins and peptides), which are believed to be responsible for allergic reactions. Latex is processed to form natural rubber latex and dry natural rubber. Dry natural rubber and natural rubber latex might contain the same plant impurities as latex but in lesser amounts. Natural rubber latex is used to produce medical gloves, catheters, and other products. Dry natural rubber is used in syringe plungers, vial stoppers, and injection ports on intravascular tubing. Synthetic rubber and synthetic latex also are used in medical gloves, syringe plungers, and vial stoppers. Synthetic rubber and synthetic latex do not contain natural rubber or natural latex, and therefore, do not contain the impurities linked to allergic reactions.
The most common type of latex sensitivity is contact-type (type 4) allergy, usually as a result of prolonged contact with latex-containing gloves. However, injection-procedure- associated latex allergies among diabetic patients have been described. Allergic reactions (including anaphylaxis) after vaccination procedures are rare. Only one report of an allergic reaction after administration of hepatitis B vaccine in a patient with known severe allergy (anaphylaxis) to latex has been published.
If a person reports a severe (anaphylactic) allergy to latex, vaccines supplied in vials or syringes that contain natural rubber should not be administered unless the benefit of vaccination clearly outweighs the risk of an allergic reaction to the vaccine. For latex allergies other than anaphylactic allergies (e.g., a history of contact allergy to latex gloves), vaccines supplied in vials or syringes that contain dry natural rubber or natural rubber latex can be administered.
PregnancyThe concern with vaccination of a pregnant woman is infection of the fetus and is theoretical. Only smallpox (vaccinia) vaccine has been shown to cause fetal injury. However, since the theoretical possibility exists, live vaccines should not be administered to women known to be pregnant.
Since inactivated vaccines cannot replicate, they cannot cause fetal infection. In general, inactivated vaccines may be administered to pregnant women for whom they are indicated. An exception is human papillomavirus vaccine,
Vaccination of Pregnant Women ● Live vaccines should not
be administered to women known to be pregnant
● In general inactivated vaccines may be administered to pregnant women for whom they are indicated
● HPV vaccine should be deferred during pregnancy
20
General Recommendations on Immunization
2
which should be deferred during pregnancy because of a lack of safety and efficacy data for this vaccine in pregnant women.
Pregnant women are at increased risk of complications of influenza. Any woman who will be pregnant during influenza season (generally December through March) should receive inactivated influenza vaccine. Pregnant women should not receive live attenuated influenza vaccine.
ACIP recommends that providers of prenatal care implement a Tdap immunization program for all pregnant women. Healthcare personnel should administer a dose of Tdap during each pregnancy, irrespective of the patient’s prior history of receiving Tdap. To maximize the maternal antibody response and passive antibody transfer to the infant, optimal timing for Tdap administration is between 27 and 36 weeks gestation although Tdap may be given at any time during pregnancy. For women not previously vaccinated with Tdap, if Tdap is not administered during pregnancy, Tdap should be administered immediately postpartum.
Studies on the persistence of antipertussis antibodies following a dose of Tdap show antibody levels in healthy, nonpregnant adults peak during the first month after vaccination, with subsequent antibody waning after 1 year. Antibody levels in pregnant women likely would be similar. Because antibody levels wane substantially during the first year after vaccination, ACIP concluded a single dose of Tdap at one pregnancy would be insufficient to provide protection for subsequent pregnancies.
Susceptible household contacts of pregnant women should receive MMR and varicella vaccines, and may receive LAIV, zoster and rotavirus vaccines if they are otherwise eligible.
ImmunosuppressionLive vaccines can cause severe or fatal reactions in immu-nosuppressed persons due to uncontrolled replication of the vaccine virus. Live vaccines should not be administered to severely immunosuppressed persons for this reason. Generally the ultimate determination of severe immuno-suppression should be made by the provider treating the immunosuppressed patient. Persons with isolated B-cell deficiency may receive varicella vaccine. Inactivated vaccines cannot replicate, so they are safe to use in immunosup-pressed persons. However, response to the vaccine may be decreased.
Both diseases and drugs can cause significant immunosup-pression. Persons with congenital immunodeficiency, leukemia, lymphoma, or generalized malignancy should not receive live vaccines. However, MMR, varicella, rotavirus,
Vaccination of Immunosuppressed Persons
● Live vaccines should not be administered to severely immunosuppressed persons
● Persons with isolated B-cell deficiency may receive varicella vaccine
● Inactivated vaccines are safe to use in immunosuppressed persons but the response to the vaccine may be decreased
Tdap Recommendations for Pregnant Women
● Healthcare personnel should implement a Tdap vaccination program for pregnant women who previously have not received Tdap
● Administer Tdap during each pregnancy, preferably between 27 and 36 weeks gestation
● If not administered during pregnancy, Tdap should be administered immediately postpartum

General Recommendations on Immunization
21
2
and LAIV vaccines may be given when an immunosuppressed person lives in the same house. Household contacts of immunosuppressed persons may receive zoster vaccine if indicated.
Certain drugs may cause immunosuppression. For instance, persons receiving cancer treatment with alkylating agents or antimetabolites, or radiation therapy should not be given live vaccines. Live vaccines can be given after chemotherapy has been discontinued for at least 3 months. Persons receiving large doses of corticosteroids should not receive live vaccines. For example, this would include persons receiving 20 milligrams or more of prednisone daily or 2 or more milligrams of prednisone per kilogram of body weight per day for 14 days or longer. See Varicella chapter for more information about administration of zoster vaccine to immunosuppressed persons.
Aerosolized steroids, such as inhalers for asthma, are not contraindications to vaccination, nor are alternate-day, rapidly tapering, and short (less than 14 days) high-dose schedules, topical formulations, and physiologic replacement schedules.
The safety and efficacy of live attenuated vaccines admin-istered concurrently with recombinant human immune mediators and immune modulators are not known. There is evidence that use of therapeutic monoclonal antibodies, especially the anti-tumor necrosis factor (TNF) agents adalimumab, infliximab, and etanercept, may lead to reactivation of latent tuberculosis infection and tuberculosis disease and predispose to other opportunistic infections. Because these drugs vary dramatically in the scope and number of immune system targeted components, it is prudent to avoid administration of live attenuated vaccines while patients are taking these drugs. For immuniza-tion against seasonal influenza and typhoid, inactivated injectable alternatives are available.
The period of time providers should wait after discontinu-ation of immune modulator drugs before administering a live-virus vaccine is not specified by ACIP or other authori-tative guidelines (except in the case of zoster vaccine). Consultation with the prescribing physician (and possibly a hospital pharmacist) is recommended for management of individual patients and guidance in estimating a particular patient’s degree of immunosuppression. No basis exists for interpreting laboratory studies of immune parameters with vaccines’ safety or efficacy. Some experts recommend waiting 1 month after discontinuing etanercept and 3 months after discontinuing the other anti-TNF agents. Lymphocyte depleting agents such as alemtuzumab and rituximab may cause prolonged immunosuppression.
Immunosuppression ● Disease
■ congenital immunodeficiency
■ leukemia or lymphoma
■ generalized malignancy
● Chemotherapy
■ alkylating agents
■ antimetabolites
■ radiation
● Corticosteroids
■ 20 mg or more per day of prednisone*
■ 2 mg/kg or more per day of prednisone*
■ NOT aerosols, alternate-day, short courses, topical
*for 14 days or longer

22
General Recommendations on Immunization
2
Restarting immunosuppression after live viral vaccination has not been studied, but some experts would recommend at least a 1-month period.
Inactivated vaccines may be administered to immunosup-pressed persons. Certain vaccines are recommended or encouraged specifically because immunosuppression is a risk factor for complications from vaccine-preventable diseases (i.e., influenza, invasive pneumococcal disease, invasive meningococcal disease, invasive Haemophilus influenzae type b disease, and hepatitis B). However, response to the vaccine may be poor depending on the degree of immunosuppres-sion present. Because a relatively functional immune system is required to develop an immune response to a vaccine, an immunosuppressed person may not be protected even if the vaccine has been given. Additional recommendations for vaccination of immunosuppressed persons are detailed in the General Recommendations on Immunization.
HIV InfectionPersons infected with human immunodeficiency virus (HIV) may have no disease manifestations, or they may be severely immunosuppressed. In general, the same vaccination recom-mendations apply as with other types of immunosuppres-sion. Live-virus vaccines are usually contraindicated in those with severe immunosuppression (defined by the treating provider) but inactivated vaccines may be administered if indicated.
Varicella can be a very severe illness in persons with HIV infection and is often associated with complications. Varicella vaccine can be considered for persons with HIV infection who are not severely immunosuppressed. Zoster vaccine should not be given to persons with AIDS or clinical manifestations of HIV infection. Persons with HIV infection should not receive LAIV; they should receive inactivated influenza vaccine (IIV). Yellow fever vaccine should be considered for persons who do not have AIDS or other symptomatic manifestations of HIV infection, who have established laboratory verification of adequate immune system function, and who cannot avoid potential exposure to yellow fever virus.
Household contacts without evidence of immunity to measles, mumps, rubella, or varicella should receive MMR and varicella vaccines, and may receive rotavirus, zoster and LAIV vaccines if otherwise eligible.
General Recommendations on Immunization
23
2
Vaccination of Hematopoietic Cell Transplant RecipientsHematopoietic cell transplant (HCT) is the infusion of hematopoietic cells from a donor into a patient who has received chemotherapy and often radiation, both of which are usually bone marrow ablative. HCT is used to treat a variety of neoplastic diseases, hematologic disorders, immu-nodeficiency syndromes, congenital enzyme deficiencies, and autoimmune disorders. HCT recipients can receive either their own cells (i.e., autologous HCT) or cells from a donor other than the transplant recipient (i.e., allogeneic HCT).
Antibody titers to vaccine-preventable diseases (e.g., tetanus, poliovirus, measles, mumps, rubella, and encapsulated bacteria [i.e., Streptococcus pneumoniae and Haemophilus influenzae type b]) decline during the 1–4 years after allogeneic or autologous HCT if the recipient is not revaccinated. HCT recipients are at increased risk for certain vaccine-preventable diseases. As a result, HCT recipients should be routinely revaccinated after HCT, regardless of the source of the transplanted cells. Revaccination with inactivated vaccines should begin 6 months after HCT. Influenza vaccine also should be administered at 6 months after HCT, but can be given as early as 4 months after HCT. In this circumstance an additional dose should be given. Influenza vaccine should be given annually thereafter for the life of the recipient. Three doses of PCV13 should be given 6 months after HCT, followed by a dose of PPSV23. Revaccination to prevent pertussis should involve a primary series of DTaP followed by a Tdap booster. A dose of MCV4 should be given.
MMR and varicella vaccines should be administered 24 months after transplantation if the HCT recipient is presumed to be immunocompetent.
Household and other close contacts of HCT recipients and healthcare providers who care for HCT recipients should be appropriately vaccinated, particularly against influenza, measles, mumps, rubella, and varicella. Additional details of vaccination of HCT recipients and their contacts can be found in the ACIP statement titled General Recommendations on Immunization.
Moderate or Severe Acute IllnessThere is no evidence that a concurrent acute illness reduces vaccine efficacy or increases vaccine adverse events. The concern is that an adverse event (particularly fever) following vaccination could complicate the management of a severely ill person. If a person has a moderate or severe acute illness, vaccination with both live and inactivated vaccines should be delayed until the patient has recovered from the illness.
Vaccination of Hematopoietic Cell Transplant (HCT) Recipients
● Antibody titers to VPDs decline during the 1-4 years after allogeneic or autologous HCT if the recipient is not revaccinated
● HCT recipients are at increased risk of some VPDs, particularly pneumococcal disease
● Revaccination recommended beginning 6-12 months post-transplant
● Inactivated influenza vaccine at least 6 months following transplant and annual thereafter
● Inactivated vaccines (DTaP/Td, IPV, hepatitis B, Hib, PCV13, PPSV23) at 6 months
● MMR and varicella vaccines at 24 months if immunocompetent
Vaccination of Household Contacts of Hematopoietic Cell Transplant
(HCT) Recipients ● Healthy household contacts
of HCT recipients should receive MMR and varicella vaccines and annual influenza vaccination

24
General Recommendations on Immunization
2
Invalid Contraindications to VaccinationSome healthcare providers inappropriately consider certain conditions or circumstances to be contraindica-tions or precautions to vaccinations. Such conditions or circumstances are known as invalid contraindications; these misperceptions result in missed opportunities to administer needed vaccines. Some of the most common invalid contraindications are mild illnesses, conditions related to pregnancy and breastfeeding, allergies that are not anaphy-lactic in nature, and certain aspects of the patient’s family history.
Mild IllnessChildren with mild acute illnesses, such as low-grade fever, upper respiratory infection (URI), colds, otitis media, and mild diarrhea, should be vaccinated on schedule. Several large studies have shown that young children with URI, otitis media, diarrhea, and/or fever respond to measles vaccine as well as those without these conditions. There is no evidence that mild diarrhea reduces the success of immunization of infants in the United States.
Low-grade fever is not a contraindication to immunization. Temperature measurement is not necessary before immu-nization if the infant or child does not appear ill and the parent does not say the child is currently ill. ACIP has not defined a body temperature above which vaccines should not be administered. The decision to vaccinate should be based on the overall evaluation of the person rather than an arbitrary body temperature.
Antimicrobial TherapyAntibiotics do not have an effect on the immune response to most vaccines. The manufacturer advises that Ty21a oral typhoid vaccine should not be administered to persons receiving sulfonamides or other antibiotics; Ty21a should be administered at least 72 hours after a dose of an antibacte-rial drug.
No commonly used antimicrobial drug will inactivate a live-virus vaccine. However, antiviral drugs may affect vaccine replication in some circumstances. Live attenuated influenza vaccine should not be administered until 48 hours after cessation of therapy using antiviral drugs active against influenza (amantadine, rimantadine, zanamivir, oseltamivir). Antiviral drugs active against herpesviruses (acyclovir, famciclovir) should be discontinued 24 hours before admin-istration of a varicella-containing vaccine, if possible.
Invalid Contraindications to Vaccination
● Mild illness
● Antimicrobial therapy
● Disease exposure or convalescence
● Pregnant or immunosuppressed person in the household
● Breastfeeding
● Preterm birth
● Allergy to products not present in vaccine or allergy that is not anaphylactic
● Family history of adverse events
● Tuberculin skin testing
● Multiple vaccines

General Recommendations on Immunization
25
2
Disease Exposure or ConvalescenceIf a person is not moderately or severely ill, he or she should be vaccinated. There is no evidence that either disease exposure or convalescence will affect the response to a vaccine or increase the likelihood of an adverse event.
Pregnant or Immunosuppressed Person in the HouseholdIt is critical that healthy household contacts of pregnant women and immunosuppressed persons be vaccinated. Vaccination of healthy contacts reduces the chance of exposure of pregnant women and immunosuppressed persons.
Most vaccines, including live vaccines (MMR, varicella, zoster, rotavirus, LAIV, and yellow fever) can be adminis-tered to infants or children who are household contacts of pregnant or immunosuppressed persons, as well as to breastfeeding infants (where applicable). Vaccinia (smallpox) vaccine should not be administered to household contacts of a pregnant or immunosuppressed person in a nonemergency situation. Live attenuated influenza vaccine should not be administered to persons who have contact with persons who are hospitalized and require care in a protected environment (i.e., who are in isolation because of immunosuppression). LAIV may be administered to contacts of persons with lesser degrees of immunosuppression.
Transmission of measles and mumps vaccine viruses to household or other contacts has never been documented. Rubella vaccine virus has been shown to be shed in human milk, but transmission to an infant has rarely been documented. Transmission of varicella vaccine virus has been reported very rarely, and most women and older immunosuppressed persons are immune from having had chickenpox as a child. Transmission of zoster vaccine virus to household or other close contacts has not been reported.
BreastfeedingBreastfeeding does not decrease the response to routine childhood vaccines and is not a contraindication for any vaccine except smallpox. Yellow fever vaccine should be avoided in breastfeeding women. However, when nursing mothers cannot avoid or postpone travel to areas endemic for yellow fever in which risk for acquisition is high, these women should be vaccinated. Breastfeeding also does not extend or improve the passive immunity to vaccine-prevent-able disease that is provided by maternal antibody except possibly for Haemophilus influenzae type b. Breastfed infants should be vaccinated according to recommended schedules.

26
General Recommendations on Immunization
2
Although rubella vaccine virus might be shed in human milk, infection of an infant is rare. LAIV may be administered to a woman who is breastfeeding if she is otherwise eligible; the risk of transmission of vaccine virus is unknown but is probably low.
Preterm BirthVaccines should be started on schedule on the basis of the child’s chronological age. Preterm infants have been shown to respond adequately to vaccines used in infancy.
Studies demonstrate that decreased seroconversion rates might occur among preterm infants with very low birth weight (less than 2,000 grams) after administration of hepatitis B vaccine at birth. However, by 1 month chronological age, all preterm infants, regardless of initial birth weight or gestational age are as likely to respond as adequately as older and larger infants. All preterm infants born to hepatitis B surface antigen (HBsAg)-positive mothers and mothers with unknown HBsAg status must receive immunoprophylaxis with hepatitis B vaccine within 12 hours after birth. Hepatitis B immunoglobulin (HBIG) also must be given to these infants. If the maternal HBsAg status is unknown, and the infant weighs 2,000 grams or more, HBIG must be given within 7 days of birth. If the maternal HBsAg status is positive or the infant weighs less than 2,000 grams, HBIG must be given within 12 hours of birth. Note that if the infant weighs less than 2,000 grams, the initial hepatitis B vaccine dose should not be counted toward completion of the hepatitis B vaccine series, and three additional doses of hepatitis B vaccine should be administered beginning when the infant is 1 month of age.
Preterm infants with a birth weight of less than 2,000 grams who are born to women documented to be HBsAg-negative at the time of birth should receive the first dose of the hepatitis B vaccine series at 1 month of chronological age or at the time of hospital discharge.
Allergy to Products Not Present in VaccineInfants and children with nonspecific allergies, duck or feather allergy, or allergy to penicillin, children who have relatives with allergies, and children taking allergy shots can and should be immunized. No vaccine available in the United States contains duck antigen or penicillin.
Allergy That is Not AnaphylacticAnaphylactic allergy to a vaccine component (such as egg or neomycin) is a true contraindication to vaccination. If an allergy to a vaccine component is not anaphylactic or is not severe, it is not a contraindication to that vaccine.

General Recommendations on Immunization
27
2
Family History of Adverse EventsA family history of seizures is a precaution for the use of MMRV vaccine. Immunosuppression may affect the decision for varicella vaccine. A family history of adverse reactions unrelated to immunosuppression or family history of seizures or sudden infant death syndrome (SIDS) is not a contraindication to vaccination. Varicella vaccine should not be administered to persons who have a family history of congenital or hereditary immunodeficiency in first-degree relatives (e.g., parents and siblings) unless the immunocom-petence of the potential vaccine recipient has been clinically substantiated or verified by a laboratory.
Tuberculin Skin Test Infants and children who need a tuberculin skin test (TST) can and should be immunized. All vaccines, including MMR, can be given on the same day as a TST, or any time after a TST is applied. For most vaccines, there are no TST timing restrictions.
MMR vaccine may decrease the response to a TST, potentially causing a false-negative response in someone who actually has an infection with tuberculosis. MMR can be given the same day as a TST, but if MMR has been given and 1 or more days have elapsed, in most situations a wait of at least 4 weeks is recommended before giving a routine TST. No information on the effect of varicella-containing vaccine or LAIV on a TST is available. Until such information is available, it is prudent to apply rules for spacing measles vaccine and TST to varicella-containing vaccine and LAIV.
There is a type of tuberculosis test known as an interferon-gamma release assay (IGRA). Even though this test improves upon the TST because it is less affected by previous doses of BCG vaccine and less affected by previous doses of tuberculosis diagnostic testing, it still may be affected by previous doses of other live vaccines so it is prudent to apply the same spacing rules as for TST.
Multiple VaccinesAs noted earlier in this chapter, administration at the same visit of all vaccines for which a person is eligible is critical to reaching and maintaining high vaccination coverage. Varicella vaccine should not be administered simultaneously with smallpox vaccine; and PCV13 and Menactra should not be administered simultaneously in children with functional or anatomic asplenia.
28
General Recommendations on Immunization
2
Screening for Contraindications and Precautions to VaccinationThe key to preventing serious adverse reactions is screening. Every person who administers vaccines should screen every patient for contraindications and precautions before giving the vaccine dose. Effective screening is not difficult or complicated and can be accomplished with just a few questions.
Is the child (or are you) sick today?There is no evidence that acute illness reduces vaccine efficacy or increases vaccine adverse events. However, as a precaution, with moderate or severe acute illness, all vaccines should be delayed until the illness has improved. Mild illnesses (such as otitis media, upper respiratory infections, and diarrhea) are NOT contraindications to vaccination. Do not withhold vaccination if a person is taking antibiotics.
Does the child have allergies to medications, food, or any vaccine?A history of anaphylactic reaction such as hives (urticaria), wheezing or difficulty breathing, or circulatory collapse or shock (not fainting) from a previous dose of vaccine or vaccine component is a contraindication for further doses. It may be more efficient to inquire about allergies in a generic way (i.e., any food or medication) rather than to inquire about specific vaccine components. Most parents will not be familiar with minor components of vaccine, but they should know if the child has had an allergic reaction to a food or medication that was severe enough to require medical attention. If a person reports anaphylaxis after eating eggs, a specific protocol should be followed that includes ascer-taining the symptoms experienced. For specific information, see Influenza chapter.
Has the child had a serious reaction to a vaccine in the past?A history of anaphylactic reaction to a previous dose of vaccine or vaccine component is a contraindication for subsequent doses. A history of encephalopathy within 7 days following DTP/DTaP is a contraindication for further doses of pertussis-containing vaccine. Precautions to DTaP (not Tdap) include (a) seizure within 3 days of a dose, (b) pale or limp episode or collapse within 48 hours of a dose, (c) continuous crying for 3 hours within 48 hours of a dose, and (d) fever of 105°F (40°C) or higher within 48 hours of a previous dose. There are other adverse events that might have occurred following vaccination that constitute contraindications or precautions to future doses. Usually vaccines are deferred when a precaution is present. However,
Screening Questions ● Is the child (or are you)
sick today?
● Does the child have allergies to medications, food, or any vaccine?
● Has the child had a serious reaction to a vaccine in the past?
● Has the child had a seizure, brain or nerve problem?
● Has the child had a health problem with asthma, lung disease, heart disease, kidney disease, metabolic disease such as diabetes, or a blood disorder?
● Does the child have cancer, leukemia, AIDS, or any other immune system problem?
● Has the child taken cortisone, prednisone, other steroids, or anticancer drugs, or had x-ray treatments in the past 3 months?
● Has the child received a transfusion of blood or blood products, or been given a medicine called immune (gamma) globulin in the past year?
● Is the person pregnant or is there a chance she could become pregnant during the next month?
● Has the child received vaccinations in the past 4 weeks?
General Recommendations on Immunization
29
2
situations may arise when the benefit outweighs the risk (e.g., during a community pertussis outbreak). A local reaction (redness or swelling at the site of injection) is not a contraindication to subsequent doses.
Has the child had a seizure, or brain or nerve problem?DTaP and Tdap are contraindicated for children who have a history of encephalopathy not attributed to an identifi-able cause within 7 days following DTP/DTaP. An unstable progressive neurologic problem is a precaution to the use of DTaP and Tdap. Children with stable neurologic disorders (including seizures) unrelated to vaccination may be vaccinated as usual.
A history of Guillain-Barré syndrome is a precaution for tetanus-containing and influenza vaccines.
Patients with a personal or family history of febrile or afebrile seizures have a precaution for MMRV vaccine. Simultaneous MMR and varicella vaccine administration (the single component vaccines) is not associated with an increased risk of fever or seizures and is therefore the acceptable alternative to MMRV.
Has the child had a health problem with asthma, lung disease, heart disease, kidney disease, metabolic disease such as diabetes, or a blood disorder?Children with any of these conditions should not receive LAIV. Children with these conditions should receive inactivated influenza vaccine only.
Does the child have cancer, leukemia, AIDS, or any other immune system problem?Live-virus vaccines (e.g., MMR, varicella, rotavirus, and the intranasal live attenuated influenza vaccine [LAIV]) are usually contraindicated in severely immunocompromised children. Persons with severe immunosuppression should not receive MMR, varicella, rotavirus, or LAIV vaccines. However, there are exceptions. For example, MMR and varicella vaccines are recommended for HIV-infected children who do not have evidence of severe immunosuppression. For details, consult the ACIP recommendations for each vaccine.

30
General Recommendations on Immunization
2
Has the child taken cortisone, prednisone, other steroids, or anticancer drugs, or had x-ray treatments in the past 3 months?Live-virus vaccines (e.g., MMR, varicella, zoster, LAIV) should be postponed until after chemotherapy or long-term, high-dose steroid therapy has ended. Details and the length of time to postpone vaccination are described elsewhere in this chapter and in the General Recommendations on Immunization.
Has the child received a transfusion of blood or blood products, or been given a medicine called immune (gamma) globulin in the past year?Certain live virus vaccines (e.g., MMR and varicella) may need to be deferred, depending on the type of blood product and the interval since the blood product was administered. Information on recommended intervals between immune globulin or blood product administration and MMR or varicella vaccination is in Appendix A and in the General Recommendations on Immunization.
Is the person pregnant or is there a chance she could become pregnant during the next month?Live-virus vaccines (e.g., MMR, varicella, zoster, LAIV) are contraindicated during pregnancy because of the theoretical risk of virus transmission to the fetus. Sexually active young women who receive MMR or varicella vaccination should be instructed to practice careful contraception for 1 month following receipt of either vaccine. On theoretical grounds, inactivated poliovirus vaccine should not be given during pregnancy; however, it may be given if the risk of exposure is imminent (e.g., travel to endemic-disease areas) and immediate protection is needed.
Has the child received vaccinations in the past 4 weeks?If the child was given either live attenuated influenza vaccine or an injectable live-virus vaccine (e.g., MMR. varicella, yellow fever) in the past 4 weeks, he or she should wait 28 days before receiving another live vaccine. Inactivated vaccines may be given at the same time or at any time before or after a live vaccine.
Every person should be screened for contraindications and precautions before vaccination. Standardized screening forms for both children and adults have been developed by the Immunization Action Coalition and are available at http://www.immunize.org.
General Recommendations on Immunization
31
2
Selected References American Academy of Pediatrics. Active and passive immu-nization. In: Pickering LK, Baker CJ, Kimberlin DW, Long SS, eds. Red Book: 2012 Report of the Committee on Infectious Diseases. 29th edition. Elk Grove Village, IL: American Academy of Pediatrics; 2012.
Atkinson WL, Kroger AT, Pickering LK. General immuniza-tion practices. In: Plotkin SA, Orentsein WA, Offit PA. eds. Vaccines. 5th ed., China: Saunders; 2008.
CDC. General recommendations on immunization: recom-mendations of the Advisory Committee on Immunization Practices. MMWR 2011;60(No. RR-2):1–61.
Dietz VJ, Stevenson J, Zell ER, et al. Potential impact on vaccination coverage levels by administering vaccines simul-taneously and reducing dropout rates. Arch Pediatr Adolesc Med 1994;148:943–9.
James JM, Burks AW, Roberson RK, Sampson HA. Safe administration of the measles vaccine to children allergic to eggs. N Engl J Med 1995;332:1262–9.
King GE, Hadler SC. Simultaneous administration of childhood vaccines: an important public health policy that is safe and efficacious. Pediatr Infect Dis J 1994;13:394–407.
Plotkin SA. Vaccines, vaccination and vaccinology. J. Infect Dis 2003;187:1349–59.
Tomblyn M, Chiller T, Einsele H, et. al. Guidelines for preventing infectious complications among hematopoietic cell transplant recipients: a global perspective. Biol Blood Marrow Transplant 2009;15:1143-1238.
Wood, RA, Berger M, Dreskin M, et. al. An algorithm for treatment of patients with hypersensitivity reactions after vaccines. Pediatrics 2008;122 (No. 3) e771-7.
32
General Recommendations on Immunization
2