Embed Size (px)
Citation preview

Immune-mediated neutropeniaand thrombocytopenia in a
patient with ulcerative colitis:An unusual hematological
association with IBDYOUNG-IN KIM MD FRCPC, AARON BRZEZINSKI MD FRCPC, JOSEPH BRANDWEIN MD FRCPC,
JEFFREY P BAKER MD FRCPC
EXTRAINTESTINAL MANIFESTATIONS
occur commonly in patients withinflammatory bowel disease (IBD) andaffect most organ systems of the body(1-5). Hematological complicationsoccur in approximately 25% of IBD pa-tients (6-17). Although thrombocy-topenia has been described in up to10% of patients with ulcerative colitis,there has been only one case reportedin the literature of immune-mediatedneutropenia and thrombocytopenia(17). Furthermore, there has been littledocumentation of the mechanismsleading to these hematological abnor-malities. We report a case of immune-mediated neutropenia and thrombocy-topenia in a patient with ulcerative co-litis during a period of relapse withoutevidence of other etiological factors.
CASE PRESENTATIONA 41-year-old Polish male with an
eight-year history of ulcerative procto-sigmoiditis presented with a one-month history of malaise, fatigue, ab-dominal bloating, periumbilical pain
BRIEF COMMUNICATION
Y-I KIM, A BRZEZINSKI, J BRANDWEIN, JP BAKER. Immune-mediated neutro-penia and thrombocytopenia in a patient with ulcerative colitis: An unusual he-matological association with IBD. Can J Gastroenterol 1995;9(2):96-100.Hematological manifestations of inflammatory bowel disease (IBD) are well de-scribed in the literature. However, the combination of immune-mediated neutro-penia and thrombocytopenia has only been reported once in association with IBD.A case is reported of immune-mediated neutropenia and thrombocytopenia in apatient with ulcerative colitis during a relapse. No obvious causes of these hema-tological abnormalities were found in the patient despite an exhaustive search.An immune-mediated process was confirmed by positive antineutrophil antibodyand platelet-associated antibody in the patient’s serum, and the demonstration ofbinding of the patient’s immunoglobulin G to autologous neutrophils. The pa-tient was treated with high-dose steroid, intravenous gamma-globulin and even-tually splenectomy. The platelet count subsequently normalized; although thesevere neutropenia recurred, it has subsequently improved without further treat-ment. Although a definitive cause-effect relationship cannot be established, theimmune-mediated neutropenia and thrombocytopenia may be an unusual hema-tological manifestation associated with ulcerative colitis. (Pour résumé, voir page97)
Key Words: Immune-mediated, Inflammatory bowel disease, Neutropenia, Thrombo-cytopenia, Ulcerative colitis
Divisions of Gastroenterology and Hematology, Department of Medicine, St Michael’sHospital, University of Toronto, Toronto, Ontario
Correspondence: Dr Young-In Kim, Vitamin Bioavailability Laboratory, USDA HumanNutrition Research Center on Aging at Tufts University, 711 Washington Street, Boston,MA 02111, USA. Telephone (617) 556-3194, Fax (617) 556-3344
Received for publication June 5, 1994. Accepted June 20, 1994
96 CAN J GASTROENTEROL VOL 9 NO 2 MARCH/APRIL 1995

and up to 10 loose bowel movementsdaily with intermittent dark red blood.He complained of anorexia, weaknessand postural lightheadedness. He alsoexperienced intermittent nocturnal fe-ver and had lost 13 kg of weight. Hehad no extraintestinal manifestationsof ulcerative colitis during this period.There was no epistaxis, bleeding orpurpura.
His ulcerative colitis had alwaysbeen limited to the distal 15 cm of thecolorectum and its course had beencharacterized by multiple exacerba-tions. Due to a poor response to oralsulfasalazine (up to 4 g/day), anenteric-coated delayed release form ofmesalamine (Asacol; Procter & Gam-ble) was substituted for sulfasalazine asinduction and maintenance therapiesfive years prior to his current presenta-tion. Since then, each exacerbationhad been treated with oral Asacol up to4 g/ day and 5-aminosalicylic acid (5-
ASA) enemas (Salofalk; Interfalk Can-ada Inc) with a good response. He hadbeen in remission for one year on Asacol1.2 g/ day up to the time of his presenta-tion. He had never had any extraintes-tinal manifestations during the courseof his disease. Since his first referral tothe authors in 1984, his completeblood count (CBC) had always beennormal; six months prior to this presen-
tation CBC showed hemoglobin 152g/L, platelets 256x109/L, white bloodcount (WBC) 6.3x109/L with a normaldifferential count, and erythrocytesedimentation rate (ESR) 15 mm/h. Hehad never been transfused.
On examination, the patient ap-peared pale but there was no rash, ec-chymosis or purpura. No lymphadeno-pathy was noted. His blood pressurewas 100/60 mmHg with mild posturaldrop and heart rate was 100 beats/minwith postural tachycardia. His initialcore body temperature was 37.0oC. Afew petechiae were seen on the palatebut there were no bullous lesions. Ab-dominal examination revealed slighttenderness in left upper quadrant with-out peritoneal signs. There was no massor hepatosplenomegaly. The rectal ex-amination was normal. A flexible sig-moidoscopy revealed moderately ac-tive inflammation up to 60 cm and asigmoid colon biopsy was consistentwith active ulcerative colitis.
The patient was admitted to thehospital. Initial blood work showed he-moglobin 125 g/L, mean corpuscularvolume (MCV) 79.9, platelets26x109/L, WBC 2.3x109/L (granulo-cytes 11%, bands 2%, lymphocytes35%, monocytes 30%, eosinophils21%, basophils 1%) and ESR 84 mm/h.The blood smear showed slight micro-
cytosis, moderately decreased platelets,few tear drop cells and few fragments.Electrolytes, renal function, glucose,amylase and liver enzymes were nor-mal. Total protein was 66 g/L and albu-min 30 g/L. Abdominal ultrasound andupper endoscopy were normal.
On the day of admission, the pati-ent’s temperature was up to 39.0oCwithout obvious source of infectionsexcept for a furuncle on the left but-tock. The chest x-ray was negative.Blood, urine, sputum and throat cul-tures were all negative. Stool culturesfor bacteria, ova and parasites, andClostridium difficile toxin were negative.Asacol was discontinued. The patientwas started empirically on intravenousgentamicin, cefazolin and metronida-zole but continued to run a low gradefever (37.5 to 38.0oC).
Bone marrow examination showedmarked granulocytic hyperplasia up tothe band stage with numerous mega-karyocytes and normal erythroid activ-ity. Iron stores were adequate and themarrow biopsy showed no evidence ofinfiltrative or myelodysplastic pro-cesses. Rheumatoid factor, antinuclearfactor, and complement components 3and 4 were normal. Direct and indirectCoombs’ tests were negative.Prothrombin time, partial thrombo-plastin time and fibrinogen were nor-mal, and fibrin degradation productswere not elevated. Serum and erythro-cyte folate and serum vitamin B12 werenormal. The serological test for the hu-man immunodeficiency virus (HIV) byboth ELISA and Western Blot donenine months later was negative. Serumimmunoglobulin (Ig) G antineutrophilantibodies were positive by indirect as-say using two normal donors; neutro-phil count was too low for directtesting. Direct assay by flow cytometryshowed positive platelet-associated(PA) IgG but negative PA IgM.
The patient’s WBC remained around1.0 to 1.5x109/L with an absolute neu-trophil count (ANC) less than0.25x109/L. However, the plateletcount continued to drop to 24x109/Lon day 9 after admission. The patientwas started on oral prednisone 80 mg/day and his platelet count and WBC
gradually increased (platelet count
Neutropénie et thrombocytopénie à médiation immunitaire chez unpatient souffrant de colite ulcéreuse : signe hématologique inhabitueldans la MII
RÉSUMÉ : Les manifestations hématologiques de la maladie inflammatoire del’intestin (MII) sont bien décrites dans la littérature. Toutefois, l’associationd’une neutropénie et d’une thrombocytopénie à médiation immunitaire n’a étérapportée qu’une seule fois en lien avec la MII. Un tel cas est présenté ici chez unpatient atteint de colite ulcéreuse, durant une rechute. Aucune cause évidente detelles anomalies hématologiques n’a été décelée chez le patient malgré une re-cherche approfondie. Un processus à médiation immunitaire a été confirmé parl’identification d’anticorps antineutrophiles et d’anticorps associés auxplaquettes dans le sérum du patient et la démonstration d’une liaison des immu-noglobulines G du patient aux neutrophiles autologues. Le patient a été traité parcorticostéroïdes à fortes doses, par gamma-globulines intraveineuses et ensuitepar splénectomie. La numération des plaquettes s’est par la suite normalisée. Bienqu’une neutropénie grave soit survenue, elle s’est par la suite améliorée sanstraitement ultérieur. Même si l’on ne peut établir de façon définitive une relationde cause à effet, la neutropénie et la thrombocytopénie à médiation immunitairepeuvent être une manifestation hématologique inhabituelle associée à la coliteulcéreuse.
CAN J GASTROENTEROL VOL 9 NO 2 MARCH/APRIL 1995 97
Immune-mediated neutropenia and thrombocytopenia in IBD

83x109/L, WBC 2.1x109/L with ANC
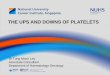
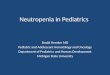
more than 0.5x109/L by day 12) (Fig-ure 1). The patient defervesced and hisconstitutional and gastrointestinalsymptoms all resolved within a few daysafter the initiation of prednisone.
However, on day 15, his plateletcount began to drop and by day 18 itwas 10x109/L. The patient was startedon intravenous gamma-globulin(Gamimune N; Miles Canada Inc)0.4 g/kg (total dose 30 g) on day 20, andoral prednisone was continued at 80 mg/day with an increase in the plateletcount (86x109/L), WBC (6.7x109/L)and ANC (0.7x109/L) by day 24.
On day 26, the patient underwentan uneventful splenectomy. He wascontinued on intravenous gamma-globulin up to the time of the opera-tion. At laparotomy, the spleen wasnoted to be enlarged and microscopicexamination showed perifollicularfoamy macrophages in the splenic redpulp and the malpighian corpusclesand congestion of the splenic sinusoids.These changes were felt to be nonspe-cific.
Blood counts improved steadily ontapering doses of prednisone after sple-nectomy (Figure 1) and the patient wasdischarged home on day 32 with hemo-globin 97 g/L, WBC 6.6x109/L andplatelet count 103x109/L.
Prednisone was discontinued within
two months of discharge. Asacol 2.4 g/day orally was reinstituted two monthsfollowing discharge, and he has re-mained asymptomatic with no furthergastrointestinal symptoms. His plateletcount has remained above 100x109/Lsince splenectomy, with no PA IgG de-monstrable at eight months follow-up.At most recent follow-up, 18 monthspostsplenectomy, his platelet countwas 275x109/L.
Neutropenia recurred two monthspostsplenectomy and the patient re-mained severely neutropenic for sixmonths, with ANC less than 0.6x109/L,although there was no evidence of a re-lapse of his ulcerative colitis. Sincethen, ANC has gradually risen withouttreatment, and is 1.85x109/L at 18months postsplenectomy. At this time,serum that had been frozen early in hisadmission was thawed and testedagainst his own fresh neutrophils.Strong binding of IgG from his previ-ously frozen serum to his fresh neutro-phils was demonstrated by flow cy-tometry. At 18 monthspostsplenectomy, there was no bindingof IgG or IgM from the patient’s freshserum to his own neutrophils.
DISCUSSIONMore than 100 extraintestinal com-
plications involving almost every or-gan system of the body have been de-
scribed in IBD patients (1,2). Thesemanifestations occur frequently, oftencomplicate management and are a sig-nificant source of morbidity and mor-tality (3).
Hematological abnormalities areseen in many IBD patients. These in-clude iron deficiency anemia (6), folateand vitamin B12 deficiency (7),Coombs’ positive autoimmune hemo-lytic anemia (8,9), thrombocytosis andimpaired platelet function (10,11), andthrombocytopenia (12-16). Thrombo-cytopenia in IBD may occur secondaryto folate and/or vitamin B12 deficiency(12), megakaryocyte aplasia (13),immune thrombocytopenic purpura (14,15) or drugs such as sulfasalazine (16).
As far as the combination of neutro-penia and thrombocytopenia in IBD isconcerned, a literature search usingMEDLINE from 1966 to present revealedonly one case report of a possibleimmune-mediated neutropenia andthrombocytopenia. Gupta et al (17) re-ported a man who developed sclerosingcholangitis, immune thrombocy-topenic purpura (ITP) and neutropeniaduring the course of ulcerative colitis.This patient was on sulfasalazine whenthrombocytopenia developed, butwithdrawing it had no effect on plateletcount. A bone marrow examinationshowed excessive numbers of megakar-yocytes and IgG PA antibodies were
present. He had two episodes of neutro-
penia; the first responding to an in-
creased dose of prednisone and the sec-
ond reverting spontaneously.
Although antibodies against neutro-
phils were not measured in this case, it
was concluded that there was transient
immune neutropenia in association
with ITP similar to one described previ-ously (18).
Even though the pathogenesis of ex-traintestinal manifestations in IBD re-mains speculative (3), the most plausi-ble explanation for thesecomplications is related to immuno-logical phenomena (4,5). Therefore, itis surprising that immune-mediated he-matological complications such as neu-tropenia and thrombocytopenia do notoccur more often in patients with IBD.In contrast, isolated or concurrentimmune-mediated destruction of plate-
Figure 1) White blood cell (WBC) and platelet (Plts) count response to a high dose steroid, intrave-nous gamma-globulin and splenectomy (Splen). Ulcerative colitis was clinically active from day1 to day 15. IVIgG Intravenous immunoglobulin G. —�— Hemoglobin (Hb); —+— Neutrophils(Neut); —*— Plts; —�— WBC
96 CAN J GASTROENTEROL VOL 9 NO 2 MARCH/APRIL 1995
KIM et al

lets and neutrophils has been reportedin several clinical settings where ab-normalities in immune system arethought to play a major pathogeneticrole such as collagen vascular diseases,drug reactions, malignancies and auto-immune disorders (19-27).
Our patient developed neutropeniaand thrombocytopenia likely secondaryto an immune-mediated process. Thepresence of PA IgG, and the demonstra-
tion of binding of the patient’s IgG to
autologous neutrophils, provide strong
evidence for an autoimmune etiology
for these cytopenias.
The bone marrow was consistentwith peripheral consumption of bothmature neutrophils and platelets, withno evidence of a marrow disorder. Al-though a marrow karyotype was notperformed, the diagnosis of myelodys-plasia is extremely unlikely, given thesubsequent normalization of the plate-let count and later marked improve-ment of the neutrophil count. Otherpossible causes for consumptive neu-tropenia and thrombocytopenia suchas infections or disseminated intravas-cular coagulation were excluded. Thepatient had neutropenic fever withoutobvious sources of infections and it isunlikely that he had an overwhelminginfection causing neutropenia andthrombocytopenia. Other causes forautoimmune neutropenia and throm-bocytopenia, such as HIV infection, col-lagen vascular diseases, malignancyand drugs, were excluded. In particular,
the HIV testing (ELISA and WesternBlot) performed nine months after hisacute illness and cytopenias essentiallyruled out HIV infection.
Furthermore, we do not believe thatthere is an etiological link betweenAsacol and his hematological abnor-malities for the following reasons: hehad been using Asacol over five yearswithout any hematological complica-tions; his platelet and neutrophilcounts did not recover following cessa-tion of Asacol; his neutrophil andplatelet counts were decreasing evenbefore Asacol was reinstituted after hisdischarge from the hospital; and his neu-trophil and platelet counts have gradu-ally normalized over the 18-monthfollow-up while on Asacol.
In addition, his transient responseto high dose steroids, intravenousgamma-globulin and splenectomy pro-vide further evidence for an immune-mediated process as the primary culprit.Therefore, the most likely precipitatingfactor in this case was the patient’s un-derlying ulcerative colitis which wasactive and had extended proximally asdocumented by endoscopic investiga-tions when he first developed neutro-penia and thrombocytopenia.
The initial response to splenectomyin our patient was encouraging. How-ever, the fact that the neutrophil countsubsequently returned to baseline sug-gests that the gamma-globulin, and notsplenectomy, was responsible for thetransient response in the neutrophil
count. Intravenous gamma-globulinhas been reported to be effective inautoimmune neutropenia (19,28)whereas response rates to splenectomyin immune neutropenia have been re-ported to be about 50%. On the otherhand, splenectomy was most likely re-sponsible for the sustained platelet re-sponse in this patient because theplatelet response to intravenous IgG isusually transient (19).
It is interesting to note that the pa-tient’s neutrophil count has graduallyrisen to normal without further treat-ment, and that he no longer demon-strates serum antineutrophil antibod-ies. The disappearance ofantineutrophil antibodies in associa-tion with remission of autoimmuneneutropenia has been described (20).Whether this is related to removal of amajor site of antibody production withsplenectomy in our patient, remissionof his underlying IBD or some othercause, is unknown.
In summary, we report a case ofimmune-mediated neutropenia andthrombocytopenia in a patient with ul-cerative colitis during a relapse withoutevidence of other causative factors. Heremains slightly neutropenic withoutany clinical consequence. We suggestthat immune-mediated neutropeniaand thrombocytopenia is an unusualhematological complication associatedwith ulcerative colitis.
REFERENCES1. Rankin GB. Extraintestinal and
systemic manifestations ofinflammatory bowel disease. Med ClinNorth Am 1990;74:39-50.
2. Greenstein AJ, Janowitz HD, SacharDB. The extraintestinal complicationsof Crohn’s disease and ulcerativecolitis. A study of 700 patients.Medicine 1976;55:401-12.
3. Kirsner JB. Inflammatory bowel disease:Considerations of etiology andpathogenesis. Am J Gastroenterol1978;65:253-71.
4. Present DH. Extraintestinalmanifestations. Mt Sinai J Med1983;50:126-32.
5. Rankin GB, Watts HD, Melnyk CS,Kelley ML Jr. National cooperativeCrohn’s disease study: Extraintestinalmanifestations and perianal
complications. Gastroenterology1979;77:914-20.
6. Dyer NH, Child JA, Mollin DL,Dawson AM. Anemia in Crohn’sdisease. Q J Med 1972;41:419-36.
7. Elsborg L, Larsen L. Folate deficiencyin chronic inflammatory bowel disease.Scand J Gastroenterol1979;14:1019-24.
8. Allan RN. Extraintestinalmanifestations of inflammatory boweldisease. Clin Gastroenterol1983;12:617-32.
9. Talbot RW, Heppell J, Dozois RR,Beart RW Jr. Vascular complications ofinflammatory bowel disease. MayoClinic Proc 1986;61:140-5.
10. Lake AM, Stauffer JQ, Stuart MJ.Hemostatic alterations in inflammatorybowel disease: Response to therapy.Am J Dig Dis 1978;23:897-902.
11. Talstad I, Rootwell K, Gjore E.Thrombocytosis in ulcerative colitisand Crohn’s disease. Scand JGastroenterol 1973;8:135-8.
12. Keene WR. Uncommon abnormalitiesof blood associated with chroniculcerative colitis. Med Clin North Am1966;50:535-41.
13. Fox RM, Firkin FC. Sequential purered cell and megakaryocytic aplasiaassociated with chronic liver diseaseand ulcerative colitis. Am J Hematol1978;4:79-85.
14. Edwards FC, Truelove SC. The courseand prognosis of ulcerative colitis 3.Complications. Gut 1964;5:1-22.
15. Kocoshis SA, Gartner JC Jr. GaffneyPC, Gryboski JD. Thrombocytopeniain ulcerative colitis. J Pediatr1979;95:83-4.
16. Gremse DA, Bancroft J, Moyer MS.
CAN J GASTROENTEROL VOL 9 NO 2 MARCH/APRIL 1995 99
Immune-mediated neutropenia and thrombocytopenia in IBD

Sulfasalazine hypersensitivity withhepatotoxicity, thrombocytopeniaand erythroid hyperplasia.J Pediatr Gastroenterol Nutr1989;9:261-3.
17. Gupta S, Saverymuttu SH, MarshJCW, Hodgson HJ, Chadwick VS.Immune thrombocytopenic purpura,neutropenia and sclerosing cholangitisassociated with ulcerative colitisin an adult. Clin Lab Haematol1986;8:67-9.
18. Linker CA, Newcom SR, Nilsson CM,Wolfe JL, Shuman MA. Combinedidiopathic neutropenia andthrombocytopenia. Ann Intern Med1980;93:704-7.
19. Novak RM, Ou DW. Variable responseto intravenous gamma- globulintreatment in a patient withautoimmune neutropenia, thrombo-cytopenia and pemphigoid. SouthMed J 1988;81:653-5.
20. Bux J, Robertz-Vaupel GM,Glasmacher A, Dengler HJ,Mueller-Eckhardt C. Autoimmuneneutropenia due to NAI specificantibodies in primary biliary cirrhosis.Br J Hematol 1991;77:121-2.
21. Weitberg AB, Harmon DC.Autoimmune neutropenia, hemolyticanemia and reticulocytopenia inHodgkin’s disease. Ann Intern Med1984;100:702-3.
22. Kruskall MS, Weitzman SA, StosselTP, Harris N, Robinson SH.Lymphoma with autoimmuneneutropenia and hepatic sinusoidalinfiltration: A syndrome. Ann InternMed 1982;97:202-5.
23. Bluming AZ, Plotkin D. Severetransient pancytopenia associated withprocainamide ingestion. JAMA1976;236:2520-1.
24. Castro O, Nash I. Quinidineleukopenia and thrombocytopenia with
a drug-dependent leukoagglutinin. NEngl J Med 1977;296:572.
25. Barnes CG, Turnbull AL,Vernon-Roberts B. Felty’s syndrome: Aclinical and pathological survey of 21patients and their response totreatment. Ann Rheum Dis1971;30:359-74.
26. Fagiolo E. Platelet and leucocyteantibodies in autoimmune hemolyticanemia. Acta Hematol1976;56:97-106.
27. Budwan DR, Steinberg AD.Hematologic aspects of systemic lupuserythematosus: Current concepts. AnnIntern Med 1977;86:220-9.
28. Pollack S. High dose intravenousgamma-globulin for autoimmuneneutropenia. N Engl J Med1983;307:253.
KIM et al

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com