Embed Size (px)
Citation preview

Imaging of Differentiated Thyroid Cancer:
Pre-surgical Planning, Evaluation of Locally Aggressive Disease and Intra-operative Ultrasound
1Salmaan Ahmed MD, 3Michael Ghazarian MD, 3Nakul Gupta MD, 1James Debnam MD, 1Thinh Vu MD, 2Gary Clayman MD
UT MD Anderson Cancer Center1Department of Radiology2Department of Head and Neck Surgery
University of Texas Medical School Houston3Department of Radiology
eEdE–153Control #: 1785

Disclosure: None

Background/Purpose The incidence of thyroid cancer in the U.S. is increasing at
a rate of more than any other cancer
This is in part due to increased workup of incidental thyroid nodules discovered on routine physical exam or imaging (ultrasound, CT or MRI)
Estimated incidence (2015) = 62,450 cases 47,230 in women and 15,220 in men 10th most among solid organ malignancies (2013)
The purpose of this exhibit is to discuss the imaging workup of differentiated thyroid cancer, with a focus of locally aggressive tumors.
American Cancer Society. Thyroid Cancer Overview. 2015. Available at: http://www.cancer.org/acs/groups/cid/documents/webcontent/acspc-030369-pdf.pdf

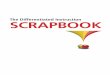
Prevalence (%)
Patel K. Genetic mutations, molecular markers and future directions in research. Oral Oncology. 2013;49(7):711-721. doi:10.1016/j.oraloncology.2013.03.437.
Medullary (3-5)
Anaplastic (1-2)
Follicular (10-15)
PapillaryThyroid
Carcinoma(80-85)
Poorly differentiated carcinoma (<2)

Papillary thyroid cancer Often with indolent clinical course, low mortality and high
likelihood of cure Variants: follicular, tall cell, insular carcinoma Local lymph node metastasis to the central neck (level VI)
and lateral neck (level II-V) is the typical spread of disease Regional metastatic disease is very common, with rates as
high as 80% Impact of nodal disease on outcome depends on age (older
= worse), number of nodes, location, size, and presence of extra capsular extension
Micrometastases and intraoperatively discovered low volume metastases – no impact on outcome
10-15% of cases are aggressive with early metastasis, disease recurrence and increased morbidity/mortalitySaindane A. Pitfalls in the Staging of Cancer of Thyroid. Neuroimaging Clinics of North America. 2013;23(1):123-145. doi:10.1016/j.nic.2012.08.010.Patel K. Genetic mutations, molecular markers and future directions in research. Oral Oncology. 2013;49(7):711-721. doi:10.1016/j.oraloncology.2013.03.437

Follicular thyroid cancer 10-15% of all thyroid cancer cases Often difficult to distinguish from benign follicular
neoplasms on FNA Lymph node spread is uncommon (8-13% of cases) Typical spread hematogenously with distant metastases
(typically lung and bones) in 10-15% of cases Variant: Hurthle cell carcinoma
○ Higher rate of lymph node metastasis than classic FTC○ Rarely presents with distant metastasis○ However, highest incidence of late distance metastasis
Saindane A. Pitfalls in the Staging of Cancer of Thyroid. Neuroimaging Clinics of North America. 2013;23(1):123-145. doi:10.1016/j.nic.2012.08.010.

Medullary thyroid cancer
Up to 5% of all thyroid cancer cases Arises from the neuroendocrine parafollicular (C cells)
responsible for the production of calcitonin ~20% of cases occur in those with multiple endocrine
neoplasia (MEN) syndrome type 2A and 2B or familial MTC
Typical spread of disease is to lymph nodes and hematogenously
Sherman S. Lessons learned and questions unanswered from use of multitargeted kinase inhibitors in medullary thyroid cancer. Oral Oncology. 2013;49(7):707-710. doi:10.1016/j.oraloncology.2013.03.442.

Anaplastic thyroid cancer
Accounts for approximately 1.7% of thyroid cancer cases Can arise de novo or in the setting of multinodular goiter
(up to 80%) or within longstanding differentiated thyroid cancer (DTC)
Marked degree of invasiveness and necrosis All tumors are considered T4 Stage IVA (intrathyroidal tumor), IVB (gross extrathyroidal
extension), IVC (distant mets) Rapidly progressive clinical course with overall poor
prognosis
O’Neill J, Shaha A. Anaplastic thyroid cancer. Oral Oncology. 2013;49(7):702-706. doi:10.1016/j.oraloncology.2013.03.440.

Staging
Generally, the most predictive factors in outcome include age, presence of distant metastases, and extent of the tumor
Given the favorable prognosis of DTC, many of the staging schemes stratify based on risk of recurrence rather than overall survival
However, due to the utility in predicting disease mortality and requirement for cancer registries, the American Thyroid Association continues to recommend AJCC/UICC staging for all patients with DTC

ANATOMIC STAGE/ PROGNOSTIC GROUPS FOR DIFFERENTIATED THYROID CANCER
UNDER 45 YEARSStage I Any T Any N M0
Stage II Any T Any N M1
45 YEARS AND OLDER
Stage I T1 N0 M0
Stage II T2 N0 M0
Stage III T3 N0 M0
T1, T2, T3 N1a M0
Stage IVA T4a N0, N1a M0
T1, T2, T3, T4 N1b M0
Stage IVB T4b Any N M0
Stage IVC Any T Any N M1
From Greene FL, Trotti A, Fritz AG, et al, editors. AJCC Cancer staging handbook. 7th edition. Chicago: American Joint Committee on Cancer; 2010. Chapter 8: Thyroid.

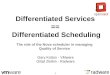
THYROID CANCER SURVIVAL
Papillary carcinoma
Follicular carcinoma
Poorly differentiated
carcinoma
Anaplastic (undifferentiated)
carcinoma
Medullary carcinoma
10 Year Survival (%)
95-98 90-95 ~50 <10 60-80
Stage 5 year Relative Survival Rate (%)
Papillary carcinoma Follicular carcinoma
I ~100 ~100
II ~100 ~100
III 93 71
IV 51 50
American Cancer Society. Thyroid Cancer Overview. 2015. Available at: http://www.cancer.org/acs/groups/cid/documents/webcontent/acspc-030369-pdf.pdf.Patel K. Genetic mutations, molecular markers and future directions in research. Oral Oncology. 2013;49(7):711-721. doi:10.1016/j.oraloncology.2013.03.437.

Discussion: Imaging Workup in Papillary Carcinoma
Real time, 2-D high resolution ultrasound (HRUS) is the preferred modality for evaluation of: Primary tumor Extrathyroidal extension Contralateral/multifocal disease Lymph node metastasis, particularly to the lateral compartment
US guides fine needle aspiration of suspicious nodes (UG-FNA) in the central and lateral compartments
Disadvantages of US Low sensitivity/specificity for central compartment nodes Lateral retropharyngeal and mediastinal nodes not evaluated

Imaging Workup in Papillary Carcinoma: Lymph Node Metastasis
Metastasis to regional nodes is extremely common, typically ipsilateral
Orderly progression from level VI to level III, IV or VII (superior mediastinum)
US features of metastatic lymph nodes: Hypoechoic or heterogeneous echotexture with loss of fatty hilum Internal calcification Rounded configuration Irregular vascular pattern Cystic appearance (cystic change is highly suggestive of PTC)
US has variable sensitivity (37-84%), but high sensitivity (89-98%) for nodal metastasis Jun H, Kim S, Kim B, Lee Y, Chang H, Park C. Overcoming the Limitations of Fine Needle Aspiration Biopsy: Detection of Lateral Neck Node Metastasis in Papillary Thyroid Carcinoma. Yonsei Medical Journal. 2015;56(1):182. doi:10.3349/ymj.2015.56.1.182.

Imaging Workup in Papillary Carcinoma: Cross-Sectional Imaging
The ATA does not recommend routine use of CT, MRI, or PET pre-operatively
However, these alternative imaging modalities may be useful in certain clinical settings to assess for involvement of extrathyroidal tissue: Large, rapidly growing tumors Locally invasive tumors Mediastinal extension
CT is useful for the evaluation of mediastinal and lateral retropharyngeal lymph nodes

Imaging Workup in Papillary Carcinoma: CT Iodinated Contrast Agents
The iodine load from contrast enhanced CT may alter the radioactive iodine uptake within the thyroid for up to 6 weeks.
Some institutions inappropriately withhold contrast.
Sohn and Choi, et al. demonstrated no significant difference in UIE at 1 month versus 6 months after preoperative CT scan with ICA
Padovani and Kasamatsu, et al. demonstrated 1 month is sufficient for UIE to return to baseline following ICA administration in post-thyroidectomy patients
Some institutions delay RAI for 2 months post-thyroidectomy and checking UIE, with others delaying ~3 months

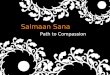
Case 1: Typical sonographic appearance of PTC
27 y.o. female with 1.6 cm right lobe papillary thyroid carcinoma. Gray scale sonographic images with color doppler demonstrate a hypoechoic solid nodule in the right lobe with microcalcification and vascular flow.

Case 1 (cont’d)
US images inferior to the right lobe of the thyroid (star) demonstrates prominent, hypoechoic, rounded nodes in the central compartment. There is loss of normal hilum and increased flow. Right central compartment dissection was performed confirming metastasis in 3 lymph nodes, with the largest measuring 7 mm.

Case 2: Diffuse infiltrative PTC
13 y.o. female with neck mass that has been present since two years of age and gradually increasing in size. CECT demonstrates diffuse heterogenous attenuation of both thyroid lobes with slight mass effect. There is a tiny calcification on the left.
Sonographic images demonstrate diffusely infiltrative hypoechoic heterogenous echotexture with foci of hyper echogenicity. Surgical pathology showed diffuse sclerosing variant of papillary thyroid carcinoma involving both lobes with extrathyroidal extension in a background of chronic lymphocytic thyroiditis.There were nodal metastasis to the bilateral central and lateral compartments.
Right thyroid lobe

Case 2 (cont’d)
Imaging of the neck in the same patient demonstrates bilateral level II adenopathy and some of the nodes have calcification, characteristic of PTC metastasis. On ultrasound, there is abnormal hypoechoic echotexture, loss of the hilum, disorganized flow, and calcification is redemonstrated.
Patient underwent total thyroidectomy with bilateral central and lateral compartment neck dissections, confirming the nodal metastasis.

Case 3: Imaging of recurrent PTC
CECT demonstrate pathologic nodes in the right lower neck with total thyroidectomy changes.
Metastasis at the right tracheoesophageal groove (yellow arrow) which require central compartment dissection. The pathologic node located lateral to this and posterior to the right internal jugular vein (red arrow) will require right lateral neck dissection.
Preoperative cytologic confirmation of metastasis in both, the central and lateral compartments, should be obtained by the radiologist, so the appropriate surgery can be planned.
In case of bilateral recurrence, FNA confirmation of metastasis in bilateral central and lateral compartments should be performed.

Imaging Workup in Papillary Carcinoma: Fine needle aspiration
UG-FNA is used to biopsy the thyroid nodule and suspicious nodes in the lateral compartment
Suspected central compartment metastasis should be biopsied in the absence of lateral compartment metastasis to guide extent of surgical resection.
Most significant complication – neck hematoma, however exceedingly rare
Routine lab screening for coagulation not required The patient should be questioned regarding recent
anticoagulation therapy, which should be withheld for 4-7 day prior to procedure

Imaging Workup in Papillary Carcinoma: FNA
Thyroglobulin (Tg) measurement in washout from lymph node FNA (Tg-FNA) can be used when cystic lymph node FNA biopsy is nondiagnostic
Tg is only produced by follicular cells and thus allows diagnosis of persistence, recurrence, or metastasis of DTC. Overall sensitivity 95.0% and overall specificity 94.5%
False-positives have been described in the literature, predominantly relating to aspiration of level VI nodes Traversal of residual thyroid tissue post-thyroidectomy or normal thyroid tissue
False-negatives have been reported in cases of undifferentiated/poorly differentiated DTC
Grani G, Fumarola A. Thyroglobulin in Lymph Node Fine-Needle Aspiration Washout: A Systematic Review and Meta-analysis of Diagnostic Accuracy. The Journal of Clinical Endocrinology & Metabolism. 2014;99(6):1970-1982. doi:10.1210/jc.2014-1098

Case 4: Cystic nodal metastasis from PTC
64 y.o. female with past history of PTC, diagnosed over 25 years ago. CECT demonstrates cystic right level IIA and IIb nodes (white arrows). Cystic node is also seen in the right inferior neck involving the central and lateral compartment (yellow arrow).

Case 5: Cystic nodal metastasis 46 y.o. female with a 1 cm hypoechoic right lobe nodue with microcalcification biopsied as PTC.
Imaging of the right lower neck demonstrates a predominantly cystic, septated lymph node in lateral compartment. US guided FNA of this lymph node revealed a non-diagnostic, acellular sample.
Repeat aspiration was performed for thyroglubulin assay, with Tg=141,840, confirming metastatic PTC to the lateral compartment.
Aspirate from cystic nodal metastasis in a different patient with PTC demonstrates yellowish clear, non-bloody fluid.

Lateral Retropharyngeal Nodal Metastasis in PTC
Some recent literature suggests a higher incidence of RPN metastasis than previously reported
RPN metastases are only evaluated by CT Mean maximum node size – 23 mm (Togashi et al.) All patients had metastases in the upper jugular chain
nodes
Preoperative transoral FNA is useful to confirm cytology for presurgical planning.
Togashi T, Sugitani I, Toda K, Kawabata K, Takahashi S. Surgical Management of Retropharyngeal Nodes Metastases from Papillary Thyroid Carcinoma. World Journal of Surgery. 2014;38(11):2831-2837. doi:10.1007/s00268-014-2707-8.

Case 5: Lateral retropharyngeal metastasis
71 y.o. male with metastatic PTC. Right lateral retropharyngeal metastasis is obscured by dental artifact. Angled images are useful in accurately diagnosing lateral retropharyngeal metastasis and also in evaluating the parotid regions.

Locally Invasive PTC
6-13% of patients with DTC have extrathyroidal extension (ETE)
Increased incidence of local recurrence, regional and distant metastases, and decreased survival
Most commonly involved structures: Strap muscles (53%)
○ Isolated involvement does not correlate with decreased survival
Recurrent laryngeal nerve (RLN) (47%) Trachea (43%) Esophagus (21%) Larynx (12%)
Saindane A. Pitfalls in the Staging of Cancer of Thyroid. Neuroimaging Clinics of North America. 2013;23(1):123-145. doi:10.1016/j.nic.2012.08.010.

Locally Invasive PTC: Recurrent laryngeal nerve paralysis
RLN paralysis can be demonstrated on CT or MR Ipsilateral laryngeal ventricular enlargement, Internal rotation of
the arytenoid Lack of medial conversion of the vocal cord
RLN paralysis is related to tumor invasion, but also mass effect/pressure on the nerve without invasion
Resection of the RLN recommended with tumor invasion Must confirm that the contralateral RLN is not involved
If RLN is functional pre-operatively, most recommend surgical preservation – no difference in outcome with RLN sacrifice vs. preservation with RAI ablation

Case 6: Tracheal invasion
Significantly decreased survival Independent prognostic factor for
survival in thyroid cancer (whereas RLN or pharynoesophageal invasion is not)
No difference in survival between radial resection and shave procedures in which all gross disease is resected
Saindane A. Pitfalls in the Staging of Cancer of Thyroid. Neuroimaging Clinics of North America. 2013;23(1):123-145. doi:10.1016/j.nic.2012.08.010.
56 y.o. male with aggressive PTC. CECT shows left lobe and isthmus mass directly invading the trachea on the left with endoluminal enhancing soft tissue (red arrow). He underwent thyroidectomy with tracheal resection, manubriectomy, first rib resection, clavicular head resection, free anterolateral thigh flap reconstruction of sternotomy defect, and placement of pedicled vastus lateralis flap.

Case 7: Tracheal and esophageal invasion
Esophgeal involvement is variable 5-21% of cases of invasive
disease
MR is the preferred imaging modality for evaluation, and involvement on CT can be suggested when fat planes are entirely effaced.
Saindane A. Pitfalls in the Staging of Cancer of Thyroid. Neuroimaging Clinics of North America. 2013;23(1):123-145. doi:10.1016/j.nic.2012.08.010.
94 y.o. woman with invasive papillary thyroid cancer, presenting with right TVC paralysis and clinical suggestion of esophageal and tracheal invasion. CECT shows a large right thyroid mass displacing midline structures towards the left. There is extenive tumor infiltrating the right tracheoesophageal groove and fat planes with the trachea, esophagus, and prevertebral soft tissues are effaced. Surgical resection included esophageal muscularis excision for diffuse involvement and tracheal resection with primary anatamosis. The right recurrent laryngeal nerve was sacrificed.

Case 7: Esophageal invasion (cont’d)
94 y.o. woman with invasive papillary thyroid cancer, presenting with right TVC paralysis and clinical suggestion of esophageal and tracheal invasion. CECT shows a large right thyroid mass displacing midline structures towards the left. There is extenive tumor infiltrating the right tracheoesophageal groove and fat planes with the trachea, esophagus, and prevertebral soft tissues are effaced. Surgical resection included esophageal muscularis excision for diffuse involvement and tracheal resection with primary anatamosis. The right recurrent laryngeal nerve was sacrificed.

Case 8: Prevertebral and Carotid Invasion
Involvement of prevertebral muscles and encasement of the carotid or brachiocephalic arteries upstages to T4b
63 y.o. male with advanced papillary thyroid carcinoma. CECT demonstrates circumferential encasement of the right common carotid artery (red arrow). Enhancing tumor extends posteriorly to involve the prevertebral soft tissues on the right. Imaging higher up demonstrated invasion of the supraglottic larynx and hypopharynx.Patient was treated with vemurafenib and subsequently with dabrafenib, and then taken to the OR for extensive complicated right neck dissection, flap rescontruction and radiation therapy.

Case 9: Jugular vein invasion
46 y.o. woman with papillary thyroid carcinoma metastatic to the right neck and mediastinum. Right level II adenopathy surrounds the internal carotid artery and the internal jugular vein is partially effaced. Sagittal image suggests there is compression of the vein without frank invasion.

Case 9: Jugular vein invasion(cont’d)
US evaluation of the right upper neck demonstrates tumor thrombus (white arrow) within the internal jugular vein, rather than extrinsic compression.
CT Imaging of the mediastinum demonstrates extensive tumor thrombus filling the bracheocephalic vein (red arrow).

Summary The incidence of thyroid cancer in the U.S. is increasing at a rate of more than
any other cancer, in part due to increased workup of incidental thyroid nodules.
Majority of patients with PTC will have an indolent clinical course. 10-15% of cases are aggressive with early metastasis, disease recurrence and increased morbidity/mortality.
2-D high resolution ultrasound with color doppler and ultrasound guided FNA are the preferred modalities for evaluating patients with PTC
Thyroglobulin (Tg) measurement in washout from lymph node FNA (Tg-FNA) can be used when cystic lymph node FNA biopsy is nondiagnostic.
High resolution contrast enhanced CT is useful in evaluating locally invasive tumors, mediastinal extension/adenopathy, and lateral retropharyngeal adenopathy.

Jun H, Kim S, Kim B, Lee Y, Chang H, Park C. Overcoming the Limitations of Fine Needle Aspiration Biopsy: Detection of Lateral Neck Node Metastasis in Papillary Thyroid Carcinoma. Yonsei Medical Journal. 2015;56(1):182. doi:10.3349/ymj.2015.56.1.182.
Kim M, Kim E, Park S et al. US-guided Fine-Needle Aspiration of Thyroid Nodules: Indications, Techniques, Results1. RadioGraphics. 2008;28(7):1869-1886. doi:10.1148/rg.287085033.
Grani G, Fumarola A. Thyroglobulin in Lymph Node Fine-Needle Aspiration Washout: A Systematic Review and Meta-analysis of Diagnostic Accuracy. The Journal of Clinical Endocrinology & Metabolism. 2014;99(6):1970-1982. doi:10.1210/jc.2014-1098.
Sohn S, Choi J, Kim N et al. The Impact of Iodinated Contrast Agent Administered During Preoperative Computed Tomography Scan on Body Iodine Pool in Patients with Differentiated Thyroid Cancer Preparing for Radioactive Iodine Treatment. Thyroid. 2014;24(5):872-877. doi:10.1089/thy.2013.0238.
Nimmons G, Funk G, Graham M, Pagedar N. Urinary Iodine Excretion After Contrast Computed Tomography Scan. JAMA Otolaryngol Head Neck Surg. 2013;139(5):479. doi:10.1001/jamaoto.2013.2552.
Padovani R, Kasamatsu T, Nakabashi C et al. One Month Is Sufficient for Urinary Iodine to Return to Its Baseline Value After the Use of Water-Soluble Iodinated Contrast Agents in Post-Thyroidectomy Patients Requiring Radioiodine Therapy. Thyroid. 2012;22(9):926-930. doi:10.1089/thy.2012.0099.
Shellenberger T, Fornage B, Ginsberg L, Clayman G. Transoral resection of thyroid cancer metastasis to lateral retropharyngeal nodes. Head & Neck. 2007;29(3):258-266. doi:10.1002/hed.20513.
Togashi T, Sugitani I, Toda K, Kawabata K, Takahashi S. Surgical Management of Retropharyngeal Nodes Metastases from Papillary Thyroid Carcinoma. World Journal of Surgery. 2014;38(11):2831-2837. doi:10.1007/s00268-014-2707-8.
References

Saindane A. Pitfalls in the Staging of Cancer of Thyroid. Neuroimaging Clinics of North America. 2013;23(1):123-145. doi:10.1016/j.nic.2012.08.010.
McIver B. Evaluation of the thyroid nodule. Oral Oncology. 2013;49(7):645-653. doi:10.1016/j.oraloncology.2013.03.435.
Nixon I, Shaha A. Management of regional nodes in Thyroid Cancer. Oral Oncology. 2013;49(7):671-675. doi:10.1016/j.oraloncology.2013.03.441.
Tuttle R, Ganly I. Risk stratification in medullary thyroid cancer: Moving beyond static anatomic staging. Oral Oncology. 2013;49(7):695-701. doi:10.1016/j.oraloncology.2013.03.443.
Nixon I, Ganly I, Shah J. Thyroid cancer: Surgery for the primary tumor. Oral Oncology. 2013;49(7):654-658. doi:10.1016/j.oraloncology.2013.03.439.
O’Neill J, Shaha A. Anaplastic thyroid cancer. Oral Oncology. 2013;49(7):702-706. doi:10.1016/j.oraloncology.2013.03.440.
Patel K. Genetic mutations, molecular markers and future directions in research. Oral Oncology. 2013;49(7):711-721. doi:10.1016/j.oraloncology.2013.03.437.
Darr E, Randolph G. Management of laryngeal nerves and parathyroid glands at thyroidectomy. Oral Oncology. 2013;49(7):665-670. doi:10.1016/j.oraloncology.2013.03.438.
Sherman S. Lessons learned and questions unanswered from use of multitargeted kinase inhibitors in medullary thyroid cancer. Oral Oncology. 2013;49(7):707-710. doi:10.1016/j.oraloncology.2013.03.442.
American Cancer Society. Thyroid Cancer Overview. 2015. Available at: http://www.cancer.org/acs/groups/cid/documents/webcontent/acspc-030369-pdf.pdf. Accessed April 3, 2015.
Greene FL, Trotti A, Fritz AG, et al, editors. AJCC Cancer staging handbook. 7 th edition. Chicago: American Joint Committee on Cancer; 2010. Chapter 8: Thyroid.
References