Embed Size (px)
Citation preview
Imaging in the Trauma Patient
David A. Spain, MDDepartment of Surgery
Stanford University

Pan Scan Instead of Clinical Exam?

Granted, some patients don’t need CT scan…

Platinum Package – Stanford Special
CT ScanHeadNeckChestAbdomenPelvisWith T/L spine reformats
Takes about 30 minutes to do

LightSpeedThe Power to Scan. Finer. Faster. Further.

The “New” ABCs
AdmitBeginCT scanExamine pt only if CT doesn’t tell you what’s wrong – the “CT-directed physical exam”

Everybody loves CT scan…Often times, resuscitation seems like a race to CT scanSometimes pt’s taken to CT after barely completing primary survey, let alone the secondary portion
Deathbeginsin X-ray

True CaseYoung year old man
Restrained passengerSide impact on his sideIntubated in field (mental status)? Right chest crepitance
Being wheeled to CT scan when trauma resident stopped and insisted on reviewing CXR


Dilemma
What’s the cost of a CT scan – real $$Versus
Cost of missed or delayed injuriesFaster thru put (double-edge)Peace of mind
Can you accurately predict who needs or doesn’t need a CT scan?

Injuries distracting from IAI after blunt trauma
Prospective study, GCS 15 and CT of abdomen or DPLPresence of pain and/or tenderness
sensitivity 82%specificity 45%positive predictive value 21%negative predictive value 93%
Abdominal pain and/or tenderness higher incidence of IAI, the lack of these findings did not preclude IAI
Am J Emerg Med 1998;16:145-9

CT for blunt abdominal trauma in the ED: a prospective study.
196 patients were evaluatedAbdominal tenderness present in 12022 patients had IAI (11%)Abnormal abdomen PE and hematuria
sensitivity of 64%specificity of 94%positive predictive value of 56%negative predictive value of 95%
Am J Emerg Med 1998;16:338-42
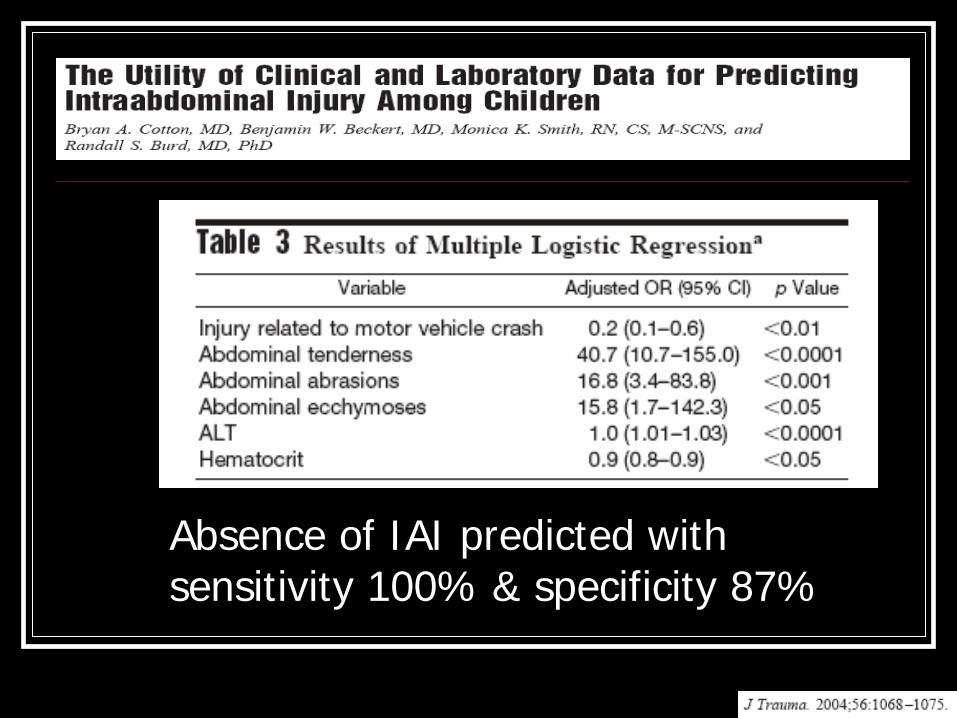
Absence of IAI predicted with sensitivity 100% & specificity 87%

Use of abdominal CT in blunt trauma: do we scan too much?
Only 37% (40 of 109) of scans were suggestive of IAIAccuracy in predicting positive scans in equivocal cases is poorTwo clinical prediction rules were found in the literatureAccurate retrospectively, but haven’t been used prospectively


Admit or obs is not necessary after a negative Abd CT: results of a prospective, multi-institutional trial
22 months at four Level I trauma centersAll patients with blunt abdominal trauma suspected by either PE or mechanism were evaluated by protocolPE in the EDAbdominal CT scanHospitalization for observationStandardized PE repeated 4 - 8 hrs later
J Trauma 1998;44:273-80

Admit or obs is not necessary after a negative Abd CT
2299 fulfilled the entire study protocol21% were positive19% patients with a positive CT scan had no tendernessNegative predictive power of abd CT scan based on prelim reading and need for a laparotomy was 99.63%

Can we omit head CT??Loss of consciousness: when to perform computed tomography?
Kids w/ LOC or amnesia and GCS 13-15 should have a head CT to avoid missing an intracranial injury
Minor head trauma: Is computed tomography always necessary?
Routine head CT in pts with LOC/amnesia but no Sx/signs of depressed skull fracture has minimal value and not warranted
NEXUS

Value of repeat cranial CT in patients with minimal head injury
MHI and a positive cranial CAT scan151 had a persistently normal or improved neurological examinationnone required after the repeat cranial CAT scan? Value repeat CAT scan in this setting
J Trauma 2004;56:475-80

Do we really need CT in primary evaluation of blunt chest trauma in patients with "normal" CXR?
93 consecutive patients 76% MVC > 10 mph24% after fall > 5 ft
25 had normal CXR and 13 (52%) CT scan showed multiple injuries
2 (8%)aortic lacerations3 pleural effusions1 pericardial effusion
J Trauma 2001;51:1173-6

Reevaluation of diagnostic procedures for transmediastinal gunshot wounds
22 stable patients CT scans were positive in 7Directed further diagnostic evaluation – 2 operations 68% had negative CT scans and were observed without further evaluationNo missed injuriesHospital charges generated with CT-based protocol were significantly less
J Trauma 2002;53:635-8

Reformatted visceral protocol HCT vs. conventional radiographs of T and L spine in blunt trauma patients
prospective evaluation of consecutive patients with thoracic and lumbar spine fracturesScreening sensitivity
Reformatted HCT: 97% (T) and 95% (L)Conventional Xray:62% (T) and 86% (L)
J Trauma 2003;55:665-9

It’s always good to exam the patients…
Restrained rear seat passenger with seatbelt, c/o some abd pain

Reliability of clinical exam in detecting pelvic fx in blunt trauma
12 studies with 5454 patients 49 false neg cases fx
majority had either altered consciousness or minor pelvic fracture only
Only 3 clinically relevant pelvic fractures were missed among 441 pts with fracture within a total population > 5000In stable and alert trauma pts, thorough exam will detect pelvic fractures with nearly 100% sensitivity

Selective management of penetrating neck trauma based on level of injury
312 pts over 18 years75% stab, 25% GSWZone I=13%, Zone II=67%, Zone III=20%
34% early exploration (16% non-therapeutic)66% observed (0.5% delayed exploration)
Am J Am J SurgSurg 1997;174:6781997;174:678--8282

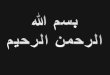
Selective Management
PenetratingPenetratingNeck Neck InjuryInjury
UnstableUnstableHard signsHard signs
OROR
SymptomsSymptomsor Signsor Signs
AsymptomaticAsymptomatic
Zone IZone I
Zone IIZone II
Zone IIIZone III
Zone II/IIIZone II/III
Zone IZone I
studystudy
OROR
angioangio
studystudy
observeobserve

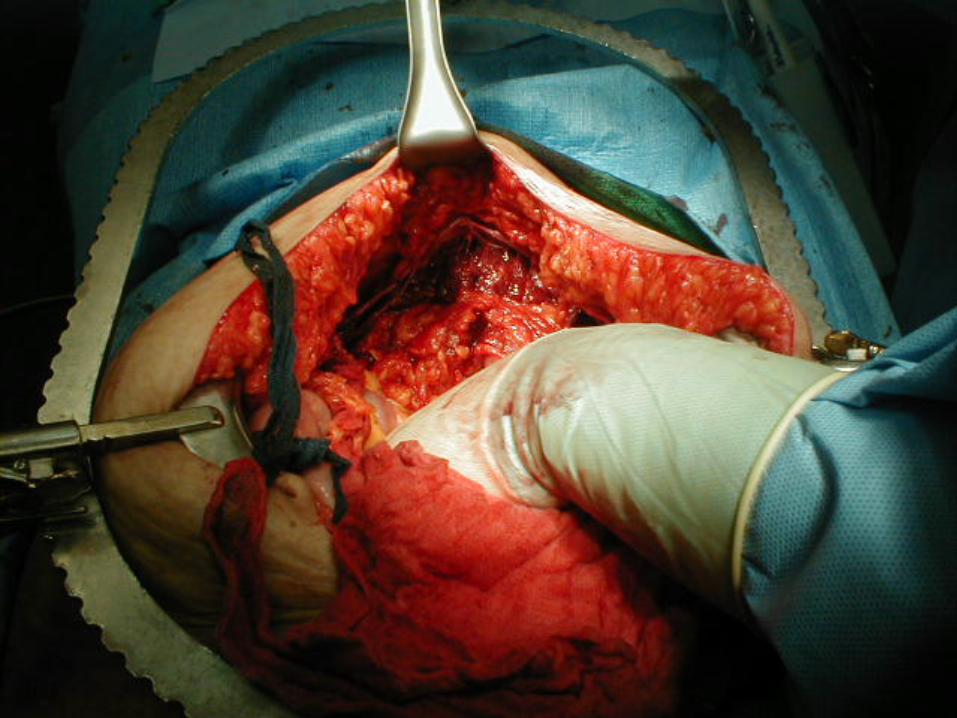
You can’t get it back in…
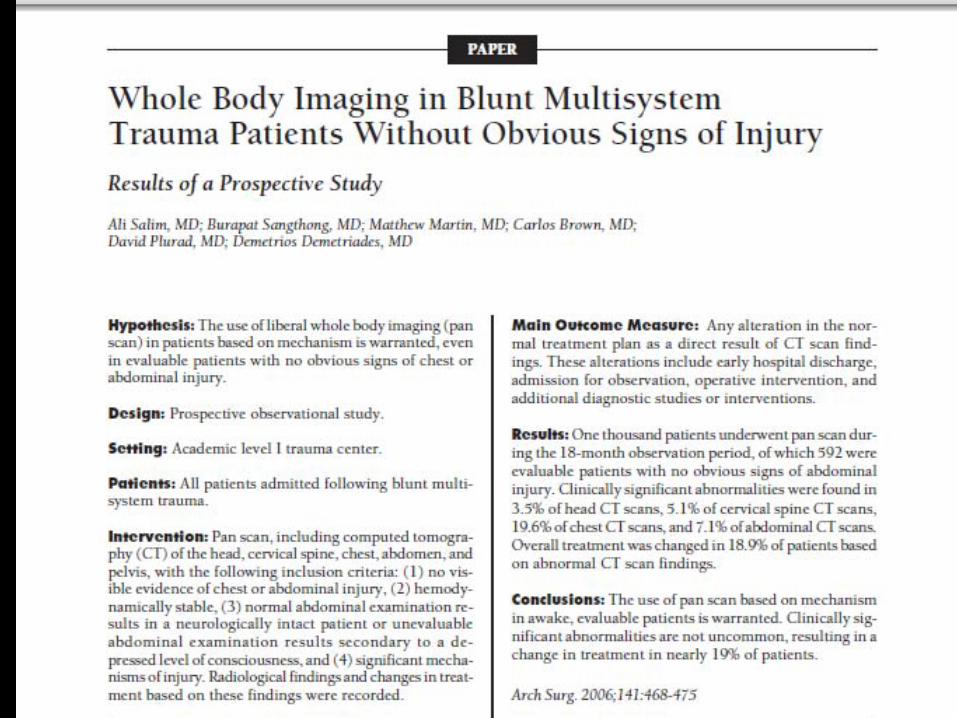

“Pan Scan”CT of the head, cervical spine, chest, abdomen, and pelvis, with the following inclusion criteria: (1) no visible evidence of chest or abdominal injury(2) hemodynamically stable(3) normal abdominal examination results in a neurologically
intact patient or unevaluable abdominal examination results secondary to a depressed LOC, and
(4) significant mechanisms of injury

Main Outcome MeasureAny alteration in the normal treatment plan as a direct result of CT scan findings. Included:
Early hospital dischargeAdmission for observationOperative interventionAdditional diagnostic studies or interventions

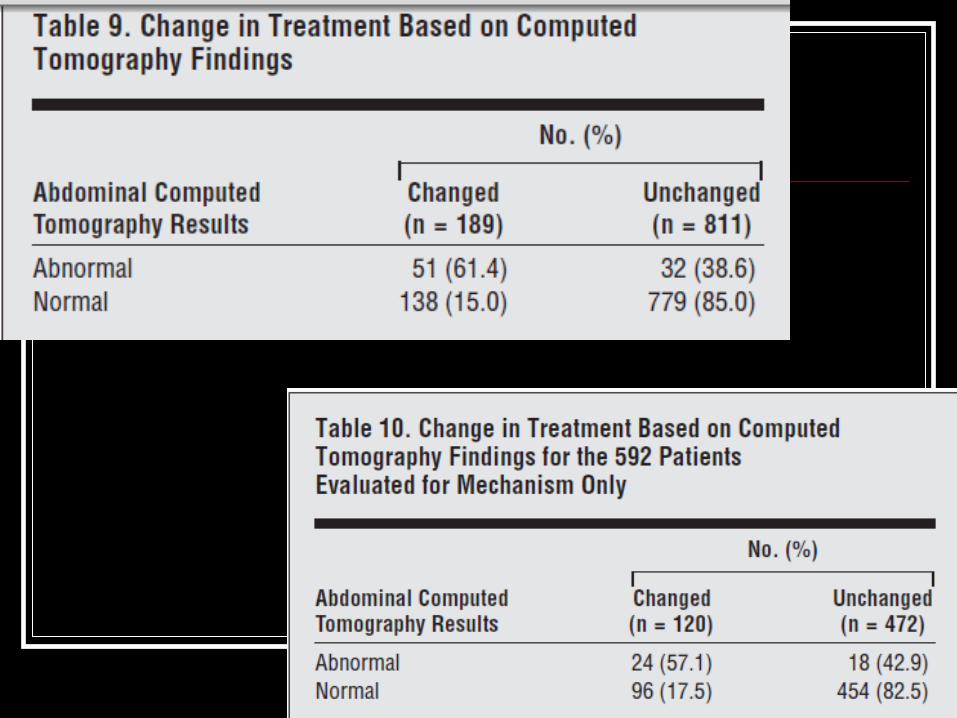
Results:1000 patients underwent pan scan during the 18-months 592 were evaluable patients with no obvious signs of abdominal injuryClinically significant abnormalities were found in
3.5% of head CTs5.1% of cervical spine CTs19.6% of chest CTs7.1% of abdominal CTs
Overall treatment was changed in 19% of patients basedon abnormal CT scan findings
Pan ScanWe believe that a liberal policy of CT scanning is warranted in patients with blunt multisystemtrauma, even among select patients without obvious signsof injury. Although the overall incidence of significantinjuries identified by the pan scan was low among evaluablepatients, it did prompt immediate intervention inseveral potentially life-threatening injuries. Of equal orgreater importance is the value of a normal pan scan inreliably excluding significant injuries and allowing forearlier discharge or disposition of patients.

Not an either/or questionCT scan technology will continue to improve
FasterMore accurateSupplanting other invasive modalities
CT is complimentary to good initial assessment and serial examinations