Embed Size (px)
Citation preview

IC
Da*†
Cberttbrtw
R1SsAc1d1©d
The Journal of Pain, Vol 8, No 10 (October), 2007: pp 767-773Available online at www.sciencedirect.com
mages of Spinal Nerves and Adjacent Structures With Opticaloherence Tomography: Preliminary Animal Studies
avid T. Raphael,* Changhuei Yang,† Nancy Tresser,† Jigang Wu,† Yaoping Zhang,*nd Linda Rever*Keck School of Medicine, University of Southern California, Los Angeles, California.Department of Electrical Engineering, California Institute of Technology; Imalux Corporation, Cleveland, Ohio.
Abstract: Multiple complications have been reported with spinal intervertebral transforaminalinjection procedures, despite the use of fluoroscopic needle-positioning measures. We explored animaging technology (optical coherence tomography, or OCT) for its possible use in spine interven-tional procedures as a means of providing needle tip vision at the neuroforamen. Optical coherencetomography is the B-mode optical analog of ultrasound. With the use of 2 different (time- andfrequency-domain) OCT systems, we obtained high-resolution (�10 �m) images of ex vivo and in situparaspinal structures (spinal nerves, radicular artery, dura, cauda equina) in different animals. An OCTforward-looking, needle-shaped endoscope in development is presented, with a discussion of itspossible method of use, safety, efficacy, technical problems, and future prospects. Further studies areneeded to determine whether such OCT technology has a potential niche in the performance of spinepain procedures.Perspective: This article presents preliminary high-resolution images obtained with an optical im-aging approach (optical coherence tomography) of neurovascular and other structures within thespinal neuroforamen. Advances in this technology may provide effective needle tip vision for paininterventionalists and may help to reduce complications from spine needle injection procedures.
© 2007 by the American Pain SocietyKey words: Complications, intervertebral foramen, optical coherence tomography, imaging, radicular
artery, medullary artery, spinal nerve root, dura.vstlsnbc
binljdfmbHi
ervical radicular pain, for which disc herniation andforaminal stenosis are the major causes, is believedto originate from nerve inflammation. This is the
asis for injecting steroids in conjunction with local an-sthetics. The use of an intervertebral transforaminaloute, as opposed to an interlaminar approach, allowshe direct delivery of steroids and local anesthetics ontohe target nerve. However, major complications haveeen reported with needle injection into the spinal neu-oforamen despite the use of fluoroscopic needle-posi-ioning measures.10,11 An imaging technology is neededhereby needle tip vision is achieved of critical neuro-
eceived September 3, 2006; Revised February 21, 2007; Accepted April4, 2007.upported by departmental funds from the USC Department of Anesthe-iology.ddress reprint requests to Dr. David T. Raphael, Keck School of Medi-ine, University of Southern California, Department of Anesthesiology,200 N. State St., Room 14-901, Los Angeles, CA 90033. E-mail:[email protected]/$32.002007 by the American Pain Society
poi:10.1016/j.jpain.2007.04.006
ascular and other structures at the injection site. Withuch a capability, complications would be minimized, andhe risk of failure of intended therapeutic effects would beessened. We review below the complications and currentafety limitations of current intervertebral transforami-al injection techniques, and how these concerns mighte addressed with a developing optical imaging method,alled optical coherence tomography (OCT).Serious neurologic complications and deaths20 have
een reported with cervical injection procedures, includ-ng severe anterior spinal artery syndrome with fatal spi-al cord infarction,4 bilateral cortical blindness owing to
eft vertebral artery puncture due to air/contrast dye in-ection,18 quadriplegia,1 complex regional pain syn-rome secondary to nerve root needle trauma,22 andatal perforation of the left vertebral artery.21 Manyore cases are known to have occurred, but have not
een reported in the literature for medico-legal reasons.ence, the complication prevalence rate is unknown, but
t is believed to be significantly higher than procedures
erformed in the lumbosacral area.767

ctotaTl
ttwc
ltsTfpfemtdat
mtwmvbccsa
atslwqCNu
M
CSS
icGlpsswcs
I
csnarepf
A
tvorttpais
R
D
E
Fm
768 Images of Spinal Nerves and Adjacent Structures With OCT
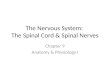
The likely cause of many such neurologic injuries isompromised perfusion in a radicular or medullary ar-ery2 (Fig 1). Particulate material in depot preparationsf corticosteroids, or injected air, can serve as embolihat can be injected directly into an artery, or that can belternatively pressurized through a vessel puncture site.he introduced emboli occlude the radicular or medul-ary artery and infarct the spinal cord.
In the Discussion section, we review the safety limita-ions of current intervertebral transforaminal injectionechniques, and how these concerns might be addressedith a developing optical imaging method, called optical
oherence tomography (OCT).OCT is the optical analog of B-mode ultrasound. It is a
aser-based imaging modality that uses visible laser lighto nondestructively image subsurface tissue structures,uch as nerves, fat, muscle, blood vessels, and cartilage.he technique15 is based on comparing light reflectedrom objects to a reference signal to determine depthenetration (interferometry). With a Michelson inter-erometer, OCT measures the amount of the interfer-nce obtained from different points within the tissue byoving the mirror in the reference arm, which changes
he distance light travels in that arm. Two- and three-imensional images are produced by scanning the beamcross the sample and recording the reflection as a func-ion of transverse position.Optical coherence tomography allows imaging throughost tissues, including nerves and arteries, to a depth of up
o 2 mm with good resolution (�10 �m).3,6,9 Although thisould appear to be a very limited viewing depth, itight be sufficient to allow identification of key neuro-
ascular structures located immediately at the needle tipefore injection. For pain interventionalists, a 1- or 2-mmhange in location can make a significant differenceomplication-wise. It follows that if OCT could image keytructures near the needle tip, neural injury could be
igure 1. Arterial supply of the spinal cord, with radicular andedullary arteries. Reprinted with permission.7
voided by slightly withdrawing the needle. f
We present data obtained from preliminary ex vivond in situ animal studies (dog, pig, rabbit, cow), withhe purpose of identifying OCT image features of criticaltructures (nerve, vessel, dura) in front of a forward-ooking OCT imaging system. The images were obtainedith 2 different forward-imaging OCT systems: (1) a fre-uency-domain OCT imaging system developed at thealifornia Institute of Technology and (2) a time-domainiris Imaging System (Imalux, Cleveland, OH) with these of a portable handheld 2.7-mm diameter probe.
aterials and Methods
alifornia Institute of Technology Sweptource Frequency-Domain ImagingystemThe frequency-domain OCT (FDOCT) engine employed
n this experiment is based on a swept laser source (Mi-ron Optics si425-1300SL; Micron Optics Inc., Atlanta,A). The OCT light source, which had a central wave-
ength of 1310 nm with a bandwidth of 70 nm, was cou-led to a fiber-based Michelson interferometer. Axial linecanning rate was 500 Hz. This system was used for ex vivotudies, with the dissected specimens placed in the imagingell of the system. The forward-looking OCT beam, in mi-
rometer translational steps, scanned the fixed-positionpecimens in transverse and longitudinal views.
MALUX NIRIS Time-Domain SystemThe Niris Imaging system from Imalux Corporation is a
ompact desktop, time-domain, forward-imaging OCTystem that uses low-coherent broadband light in theear infrared range. Its scanning depth is 2.2 mm in air,nd its lateral scanning range is 1 mm. Image acquisitionate is at 1.5 seconds/frame. It uses a 2.7-mm outer diam-ter reusable, handheld imaging probe, which waslaced atop structures of interest to generate the imagesor in situ studies.
nimal StudiesAll animal studies were performed with approval of
he Animal Care Institutional Review Boards of the Uni-ersity of Southern California and the California Institutef Technology. All dissections were performed by a neu-osurgeon, with careful exposure of paraspinal struc-ures of interest. Epidural and spinal needles were usedo create dural punctures, respectively, in a euthanizedig and rabbit. Dissected spinal nerve roots and radicularrteries in the intervertebral foramen region were stud-ed in the same animals. The bovine cauda equine wastudied, as were canine brachial plexus nerves.
esults
ural Defects
x Vivo Pig StudyIn a 25-kg euthanized pig, surgical dissection was per-
ormed through the midline lumbar region down to the

lme1arpda
I
bssttlti
mw
N
E
rFrctcshes
I
ar
Fc
FHhd
Fir
F
769ORIGINAL REPORT/Raphael et al
evel of dura, along the pathway of an epidural needleidline approach. A dural specimen was excised, and the
x vivo specimen was fixed in position, punctured with a7-gauge Tuohy epidural needle, and placed in the im-ging well of an FDOCT system. The baseline intact duraeveals an essentially uniform tissue. Subsequent touncture with the epidural needle, the effect on theura is evident as a significant conical defect (Fig 2). Im-ging was performed with the CalTech system.
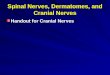
n Situ Rabbit StudyDissection was performed on a euthanized 10-kg rab-it down to the lumbar dura, along the pathway of apinal needle midline-approach. We performed succes-ive dural punctures with a 26-gauge needle. Each punc-ure produced an evident discontinuity in the high scat-ering dural layer when visualized using OCT (Fig 3). Theateral size of the dural defect (370 �m) was comparableo the needle tip (400 �m). No similar defects were seenn the intact (unpunctured) dura. The dura in the rabbit
igure 2. Optical coherence tomography image of dural defectaused by puncture with 17-gauge Tuohy needle.
igure 3. Dural puncture in rabbit spinal cord with 26-g needle.igh scattering horizontal structure with sharp contrast (arrow-eads) is the dura, which measures 43 �m in thickness. A dural
efect measuring 370 �m is identified (arrows). weasured 43 �m in thickness. OCT imaging was doneith the time-domain Niris System.
erve Roots/Radicular Artery
x Vivo Pig StudyDissection was done to expose the lumbar spinal nerve
oots in the neuroforamina of the euthanized pig. With theDOCT system, we obtained ex vivo images of a porcineadicular artery (Fig 4), which longitudinally followed theourse of the spinal nerve root, and which was located onhe posterior surface of the nerve. It has a muscularis layer,ompatible with that of an artery. Of special note is themall size of the subsurface vessel (�500 �m). On the rightand side, in Fig 5, the corresponding hematoxylin andosin stain reveals the same epineurial vessel, its half-moonhaped lumen partially filled with blood.
n Situ Rabbit StudyDissection was done to expose the spinal nerve roots ineuthanized rabbit. No radicular vessel on a spinal nerve
oot was grossly seen during the rabbit dissection; how-
igure 4. Frequency-domain optical coherence tomographymage of a porcine epineurial vessel atop a porcine spinal nerveoot.
igure 5. The same epineurial vessel as in Fig 4 after staining
ith hematoxylin and eosin.
es2
S
E
wspnTmws
ct
I
bm
P
tnit
wtltfttg
Fve
FF6H
Fsb
F
770 Images of Spinal Nerves and Adjacent Structures With OCT
ver, additional OCT images revealed the presence ofubsurface radicular vessels measuring approximately60 to 300 �m in diameter.
pinal Nerve Roots
x Vivo Cow StudyThe distal spinal cord and intact cauda equine of a cowas examined ex vivo. Fig 6 shows a transverse cross-
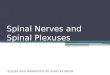
ectional OCT image of the bovine cauda equina. Multi-le nerve roots are evident as round to oval homoge-eous structures, with an average diameter of 300 �m.he corresponding histologic image (Fig 7) shows 4 he-atoxylin and eosin–stained round to oval nerve rootsith intact epineurium. The hematoxylin and eosin–
tained section confirms the homogeneous nature of the
igure 6. Optical coherence tomography image of ex vivo bo-ine cauda equina. Nerve roots appear as distinctive and homog-nous round to oval structures averaging 300 �m in diameter.
igure 7. Histological image of ex vivo bovine cauda equina.our nerve roots are seen corresponding to the OCT image of Fig. Dozens of individual nerve fibers are seen in each nerve root.
ematoxylin and eosin stain. tontents of the spinal nerve roots, each of which con-ains dozens of individual nerve fibers.
n Situ Rabbit StudyThe time-domain system was able to visualize the lum-ar spinal nerve roots, which were evident as bright ho-ogeneous structures (Fig 8).
eripheral NerveIn Fig 9, 1 has the hematoxylin and eosin–stained sec-
ion of a transversely cut ex vivo canine brachial plexuserve. A multitude of myelinated nerve fibers occupy the
nterior of the nerve. Each nerve fiber consists of a cen-ral axon surrounded by a myelin sheath.Fig 10 shows the corresponding OCT transverse image,ith its similarly arrayed multitude of dark ovoid struc-
ures (nerve fibers), each fiber surrounded by a thin,ightly colored rim. This study was done with a polariza-ion sensitive OCT (PS-OCT) system.19 In studies of nerveascicles from the brachial plexus, the nerve fibers withinhe fascicle course not only parallel to the direction ofhe fascicle but also laterally within the fascicle, as sug-ested by the upper portion of the figure. In the longi-
igure 8. Optical coherence tomography image of a rabbitpinal nerve root. Root is shown as it split into 2 distinctranches outlined by dashed lines. Bar is 1 mm.
igure 9. Hematoxylin and eosin–stained transverse cross sec-
ion of a canine brachial plexus nerve. Magnification �45 to 50.
tac
D
s
(
(
(
(
(
O
dTitmnnfv
dfisn
ittc4t
Fc
F
771ORIGINAL REPORT/Raphael et al
udinal view, as shown in Fig 11, the nerve fibers are seens dark tortuous tubular structures that parallel theourse of the nerve.25
iscussionThe limitations of safety measures used to minimize
uch complications are:
1) Inability of Fluoroscopy to Image the Spinal Nerveand Radicular Artery. Fluoroscopy cannot image thespinal nerve roots, nor can it image the radicular/medullary artery except when there is accidental ar-terial injection of contrast dye.20
2) Unreliable Blood Aspiration Test. In both cervical andlumbosacral ESIs, a positive flash or aspiration ofblood is only predictive of intravascular injection inless than half of the documented intravascular re-sponses (�45% false-negative rate). Therefore, aspi-ration before injection is not a consistently reliablemeans of preventing needle intravascular place-ment.10,11,14
3) Individual Deviations From Presumed WorkingAnatomy. Practice guidelines for safe cervical transfo-raminal procedures urge operators to place the needleposteriorly in the intervertebral foramen dorsal to thespinal nerve in order to avoid any arteries, on the as-sumption that these vessels lie anterior to the spinalnerve5,24 (Fig 1). The presumed working anatomy isthat, above the equator, the needle may encounterepiradicular veins, whereas below it, it may encounterthe spinal nerve and its arteries. However, 1 study8 hasdemonstrated that radicular arteries can be seen pos-terior to the spinal nerves, 1 lying high and the otherlying low in relation to the spinal root. The extent ofsuch individual variation is unknown. Hence operatorscannot rely on the presumed working anatomy as anabsolute guarantee of procedural safety.
4) Discontinuous Imaging of Target Site. A test injec-tion of contrast medium is considered mandatory.But an operator may easily miss the fleeting imageof a thin radicular artery branch upon injection.
igure 10. Optical coherence tomography image of transverseross section of a canine brachial plexus peripheral nerve.
Moreover, an inadvertent intra-arterial injection b
might still occur after an ever so slight movementof the operator’s hand, or even with a minimaldisplacement of the syringe needle or of the vol-ume tubing subsequent to the digital angiogram.This is a significant limitation of discontinuous im-aging.14
5) Nonfusion of Midline Cervical and High ThoracicLigamentum Flavum. For interlaminar midline ap-proaches with spinal needle procedures, the loss-of-resistance technique relies on a perceptible pen-etration of the ligamentum flavum. In a study of 52human cadavers, mid-line gaps in the ligamentaflava are frequent at cervical (�50%) and high tho-racic levels (2% to 20%) but are rare at the T3 leveland below. Hence, one cannot rely on penetrationof the ligamentum flavum as a perceptible barrierto interlaminar cervical placement of an epiduralneedle.17
CT Image ResultsWith FDOCT imaging in a pig, the dural defect pro-uced by the 17-g Tuohy needle has the shape of a cone.he defect is widest at the surface, and extends to anntradural depth of 1.2 mm. The subsurface extension ofhe defect is not evident in conventional en face electronicrographs that show the defect frontally. It should be
oted that the spinal dura mater is a tube of dense con-ective tissue that is generally not very vascular, exceptor tiny twigs from the spinal arteries. Hence, intraduralessels in these images are not seen, as expected.With an in situ 26-gauge dural puncture in a rabbit, theefect appears as a discontinuity in the dura. The defectlls up with underlying cerebrospinal fluid. In compari-on to the pig epidural defect, the spinal needle defect isot as evident in the depth direction.The radicular artery is a critical feature that a pain
nterventionalist must recognize in order to avoid in-ravascular injection while advancing the needle in theransforaminal region. A porcine epineurial vessel islearly imageable on top of a spinal nerve root in Figsand 5. The evident musucularis layer distinguishes
his structure as an artery, which is surrounded by fatty
igure 11. Optical coherence tomography longitudinal view of
rachial plexus peripheral nerve.
taivoa
ifcmhicefilaobtsn
P
Ogamcniuom
crao
anocptmttwirpminb
pap
tgfidnrnmrosaeensjp
d(vOtmti
itawtidCwdavvts
ficpno
tpmqu
772 Images of Spinal Nerves and Adjacent Structures With OCT
issue, and which very likely is the posterior branch ofradicular artery. The crescent moon shape is compat-
ble with the appearance of extrinsic nutrient arterialessels that reach the epineurium, ramify within theuter layer, and supply the intraneural plexus throughscending and descending branches.As shown in earlier studies,3 OCT can be used to
dentify nerve fascicles, a characteristic and definingeature of peripheral nerves. An individual nerve fas-icle, depending on its location and function, can beonofascicular, bifascicular, or polyfascicular. With aigher resolution OCT system, it may be possible to
mage nerve fibers within the fascicles. Fig 10 shows aanine brachial plexus nerve with a honeycomb of my-linated nerve fibers in transverse cross-section, con-rmed by hematoxylin and eosin staining (Fig 9). In
ongitudinal cross-section (Fig 11), a pattern of sinuousnd tortuous parallel tubular tracts is evident. Tortu-sity of the ex vivo fascicles within the nerve occursecause the elastic and normally stretched nerves re-ract upon excision.19 With high-frequency ultra-ound, the same tortuous pattern is seen in longitudi-al images of ex vivo nerve specimens.25
roposed Imaging ApproachFor pain specialists, the basic question is whetherCT imaging can prevent neural injury. Prior investi-ations indicate significant neural injury results whenneedle penetrates through the fascicle, and evenore so when local anesthetic is injected into the fas-
icle.12 In contrast, little or no injury occurs when theeedle path, even with local anesthetic injection or
nfusion, is extrafascicular, that is, into the epineuri-m.13,23 Certainly, if a nerve fascicle is seen at the tipf a forward-imaging OCT needle endoscope, it wouldake sense to withdraw the needle slightly.What about injection into a vessel? For an artery, OCT
an image the wall layers of the vessel, and allow itseady identification as such. Distinguishing an epineurialrtery from a vein would require observing the thicknessf the muscularis layer.Hence, given the limited depth window of OCT, for
n image of the tissue in the immediate vicinity of theeedle tip, is the combined absence in the OCT imagef a vessel and the absence of nerve fascicles a suffi-iently protective measure against neural harm? Thereliminary evidence presented herein allows us tohink so. First, the conventional radiological guidanceethodology could be employed to optimally position
he needle tip. Second, OCT could be used to explorehe proposed injection site, if need be, to determinehether a vessel or nerve was in the immediate vicin-
ty. If a nerve or vessel was noted, the needle could beepositioned such that no neurovascular structure wasresent in the OCT image, indicating at least a 2-mmargin of safety, for which the risk of an intraneural or
ntravascular injection should be nil. On a cautionaryote, we note that other imaging techniques have
een proposed in which the absence of a single end fioint was deemed as safe, yet subsequent clinical us-ge revealed that it was found to be insufficient torovide complete safety or protection.Optical coherence tomography has significant limi-
ations. It is unlikely that it can be used as a majoruidance method to direct the needle from skin tonal foraminal injection site. For example, if the nee-le tip is 1 to 2 cm away from the target site, thearrow OCT imaging depth window of 2 mm may noteveal any identifiable reference structures in the spi-al foraminal area. Careful half-millimeter-sizedovements of the needle would be needed to bring
eference structures into view. The most suitable rolef OCT would then seem to be to combine it withtandard radiological positioning, and then to use it asn exclusionary high-resolution device for the finalnd positioning. At the very end, OCT could be used toxclude the possibility of any injection into a criticaleurovascular structure. Such an approach might beuperior to conventional blood aspiration and dye in-ection tests that have not proven to be sufficientlyrotective.Present studies indicate that the effective imagingepth of OCT can be extended. Adaptive ranging16
AR) is a dynamic feedback technique currently in de-elopment whereby image data are used to adjust theCT system coherence gate offset, improve dB sensi-
ivity, and extend the imaging range to as much as 7m. If this extended imaging range is consistently at-
ainable with AR-equipped OCT systems, OCT as anmaging modality would become much easier to use.
The major remaining limitation is thinness of themaging probe. Current research is proceeding towardhe creation of even thinner OCT needle probes. Ide-lly, it would seem that practitioners need a 25-g for-ard-looking OCT needle for cervical foraminal injec-
ions. However, the smallest forward-looking OCTmaging needle currently in existence is a frequency-omain 21-gauge imaging needle developed atalTech.26 This is close in size to a 22-gauge spinal needle,hich is used often in lumbosacral spinal injection proce-ures. However, it may be otherwise argued that the use of25-gauge needle may make it easier to enter the small
essels near the neuroforamen, although there is no con-incing evidence collected in a prospective randomly wayo justify preference of a slightly larger needle versus amall needle.Any such OCT needle probe, with its internal opticalber incorporated into the needle, would also require aonduit for the administration of injectate. In its pro-osed design, the OCT needle endoscope would alloweedle tip visualization of the actual site of injection andf the local spread of the injectate.These preliminary animal experiments suggest a po-
ential niche for an OCT-based imaging needle in theerformance of spinal foraminal injections. However,any more investigations involving humans are re-
uired before OCT can be recommended for routinese. An extensive OCT neuroforaminal image database
rst needs to be created, in order to better appreciate
tcwta
A
M
R
1i2
2fa2
3Bcm
4at
5(3
6tt
7CC
8a
9rt
1ie
1is
1n4
1icd
773ORIGINAL REPORT/Raphael et al
he effects of individual variation and disease pro-esses. If the OCT imaging range can be extended, asith adaptive ranging, the training curve in the use of
his technology should be no greater than that associ-
ted with ultrasound. pase study. Neurosurgery 6:263-72, 1980
1r2
1CO1
1Tr
1Ktm
1rf
1Ot
2i
2mno3
2do
2F1
2sM
2bsA
2Pp
cknowledgments
We wish to extend our thanks for graphics assistance tos. Diane McIntee, Special Projects Coordinator, USC De-
artment of Anesthesiology.
eferences
. Anonymous: Miss-’n-mix and mimics. Tetraplegia follow-ng erroneous epidural injection. Acta Anaesthesiol Belg 52:05-206, 2001
. Baker R, Dreyfuss P, Mercer S, Bogduk N: Cervical trans-oraminal injection of corticosteroids into a radicular artery:possible mechanism for spinal cord injury. Pain 103:211-
15, 2003
. Boppart SA, Bouma BE, Pitris C, Tearney GJ, Southern JF,rezinski ME, Fujimoto JG: Intraoperative assessment of mi-rosurgery with three-dimensional optical coherence to-ography. Radiology 208:81-86, 1998
. Brouwers P, Kottink E, Simon MAM, Prevo RL: A cervicalnterior spinal artery syndrome after diagnostic blockade ofhe right C6-nerve root. Pain 91:397-399, 2001
. Chakravorty BG: Arterial supply of cervical spinal cordwith special reference to radicular arteries). Anat Rec 1770:11-330, 1971
. Choma M, Sarunic M, Yang C, Izatt J: Sensitivity advan-age of swept source and Fourier domain optical coherenceomography. Optics Express 11:2183-2189, 2003
. Cousins MJ, Bridenbaugh PO (eds): Neural Blockade inlinical Anesthesia and Management of Pain. J.B. Lippincottompany, Philadelphia, PA, 1980, p 155
. Crock HV: An Atlas of Vascular Anatomy of the Skeletonnd Spinal Cord. Martin Duntz, London, UK, 1996, pp 31-32
. Ding Z, Zhao Y, Ren H, Nelson J, Chen Z: Real-time phase-esolved optical coherence tomography and optical Doppleromography. Optics Express 10:236-245, 2002
0. Furman MB, O’Brien EM, Zgleszewski TM: Incidence ofntravascular penetration in transforaminal lumbosacralpidural steroid injections. Spine 25:2628-2632, 2000
1. Furman MB, Giovaniello MT, O’Brien EM: Incidence ofntravascular penetration in transforaminal cervical epiduralteroid injections. Spine 28:21-25, 2003
2. Gentili F, Hudson AR, Kline DG, Hunter D: Peripheralerve injection injury: Experimental study. Neurosurgery:244-253, 1979
3. Gentili F, Hudson AR, Hunter D, Kline D: Nerve injectionnjury with local anesthetic agents: A light and electron mi-roscopic, fluorescent microscopic, and horseradish-peroxi-
4. Houten JK, Errico TJ: Paraplegia after lumbosacral nerveoot block: Report of three cases. Spine Journal 2:70-75,002
5. Huang D, Swanson EA, Lin CP, Schuman JS, Stinson WG,hang W, Flotte T, Gregory K, Puliafito CA, Fujimoto JG:ptical coherence tomography. Science 254:1178-1181,991
6. Iftimia NV, Bouma BE, De Boer JF, Park BH, Cense B,earney GJ: Adaptive ranging for optical coherence tomog-aphy. Optics Express 12:4025-4034, 2002
7. Link P, Kolbitsch C, Putz G, Colvin J, Colvin HP, Lorenz I,eller C, Kirchmair L, Rieder J, Moriggl B: Cervical and high
horacic ligamentum flavum frequently fails to fuse in theidline. Anesthesiology 99:1387-1390, 2003
8. McMillan MR, Crumpton C: Cortical blindness and neu-ologic injury complicating cervical transforaminal injectionor cervical radiculopathy. Anesthesiology 99:509-511, 2003
9. Raphael DT, Zhang J, Zhang Y, Chen Z, Miller C, Zhou L:CT/PS-OCT imaging of brachial plexus neurovascular struc-
ures. Proc SPIE Biomedical Optics 5312:388-395, 2004
0. Rathmell JP, Aprill C, Bogduk N: Cervical transforaminalnjection of steroids. Anesthesiology 100:1595-1600, 2004
1. Rozin L, Rozin R, Koehler SA, Shakir A, Ladham S, Bar-ada M, Dominick J, Wecht CH: Death during transforami-al epidural steroid nerve root block (C7) due to perforationf the left vertebral artery. Am J Forensic Med Pathol 24:51-355, 2003
2. Siegfried S: Development of complex regional pain syn-rome after a cervical epidural steroid injection. Anesthesi-logy 86:1394-1396, 1997
3. Terzis JK, Smith KL: The Peripheral Nerve: Structure,unction, and Reconstruction. Raven Press, New York, NY,990, pp 38-46
4. Turnbull IM, Breig A, Hassler O: Blood supply of cervicalpinal cord in man: A microangiographic study. Acta Patholicrobiol Scand 24:951-965, 1966
5. Wang TY, Chui PT, Metreweli C: Anatomy of the normalrachial plexus revealed by sonography and the role ofonographic guidance in anesthesia of the brachial plexus.m J Radiol 171:1631-1636, 1998
6. Wu JW, Conry M, Gu C, Wang F, Yaqoob Z, Yang C:aired-angle rotation scanning optical coherence tomogra-
hy forward-imaging probe. Optics Lett 31:1265, 2006