Embed Size (px)
Citation preview

Images in Cardiovascular Medicine
Transjugular Tricuspid Valve-in-Valve ReplacementHellmuth Weich, MBChB, MRCP(UK), MMed(Int), Cert Cardiology(CMSA);
Jacques Janson, MBChB, FCS(Cardio), MMed(Thor); Jacques van Wyk, MBChB, FCS(Cardio);Philip Herbst, MBChB, MRCP(UK), FCP(CMSA), Cert Cardiology (CMSA);
Pieter le Roux, MBChB, DA(SA), MMed(Anes), FCA; Anton Doubell, MBChB, MMed(Int), PhD
The patient is a 38-year-old woman with rheumatic heartdisease requiring surgery 21 years ago. She received a St.
Jude mechanical prosthesis in the mitral position and aCarpentier-Edwards Perimount bioprosthesis (size 31) in thetricuspid position.
Over the past 2 years, she has become progressively moreshort of breath with regular admissions for congestive heartfailure despite medical treatment. Transthoracic echocardiog-raphy showed a severely dilated right atrium and a calcifiedtricuspid prosthesis with a mean gradient across the valvevarying between 9 and 12 mm Hg (Figures 1 and 2). Themitral valve prosthesis functioned well.
A decision was made to replace the tricuspid valve, but inconsultation with the heart team, it was agreed that, given thatthe mitral valve prosthesis was functioning well, the risk of asecond sternotomy to replace only the tricuspid valve wasdifficult to justify if an alternative option was available.Given the limited lifespan of a bioprosthesis in a youngperson, she would then require her third (and likely final)sternotomy at a young age. A joint decision was therefore
made to offer the patient a minimally invasive tricuspid valvereplacement by a transcatheter procedure. The risks of atranscatheter procedure were discussed with her, and sheprovided written informed consent.
The option of a transatrial approach was considered, butthis would still have required a thoracotomy, and with theintroduction of the new 19F Edwards-SAPIEN XT valve(Edwards Lifesciences, Irvine, CA), transjugular access waspreferred. Because the old prosthesis was a size 31, there wasconcern that the 26-mm Edwards valve would not fit se-curely. Transesophageal echocardiography showed extensivecalcification of the prosthesis, which was viewed as adequateto anchor the Edwards prosthesis. We furthermore decided tooverexpand the prosthesis to 27 mm, because the anticipatedcentral regurgitation of the valve resulting from the overex-pansion was likely to be mild and well tolerated.
The patient was admitted for intravenous heparinization,and her oral warfarin was stopped. The procedure wasperformed in the catheterization laboratory with the patientunder light general anesthesia to enable constant transesoph-
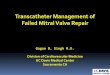
Figure 1. The continuous wave spectral Dopp-ler of the degenerate tricuspid prosthesisbefore the procedure showing a profile ofsevere tricuspid stenosis with averaged(because of atrial fibrillation) peak and meangradients of 12 and 9, respectively. Vmax indi-cates maximum flow velocity; Vmean, meanflow velocity; Pmax, maximal pressure gradient:Pmean, mean pressure gradient; Env Ti, dura-tion of measured envelope; VTI, velocity timeintegral; HR, heart rate.
From the Division of Cardiology, Department of Medicine (H.W., P.H., A.D.), Cardiothoracic Surgery Unit (J.J.), and Department of Anesthesiology(P.l.R.), Tygerberg Academic Hospital and Stellenbosch University; and Department of Cardiothoracic Surgery, Panorama Medi Clinic, Cape Town,South Africa (J.v.W.).
The online-only Data Supplement is available with this article at http://circ.ahajournals.org/cgi/content/full/124/5/e157/DC1.Correspondence to Hellmuth Weich, MBChB, Cardiology Unit, 8th Floor, Tygerberg Academic Hospital, Private Bag x1, Tygerberg 7505, South
Africa. E-mail [email protected](Circulation. 2011;124:e157-e160.)© 2011 American Heart Association, Inc.
Circulation is available at http://circ.ahajournals.org DOI: 10.1161/CIRCULATIONAHA.111.027342
e157
by guest on June 21, 2018http://circ.ahajournals.org/
Dow
nloaded from

ageal monitoring. A cardiopulmonary bypass system wasprepared, and rapid conversion to open surgery could beachieved if required. A venogram of the right jugular veinwas performed to confirm adequate size, and this wasfollowed by surgical cutdown and purse string preclosure ofthe vein. Heparin was given intravenously to attain anactivated clotting time of �250 seconds. A straight-tip0.035-inch guidewire was passed over an Amplatz left 3catheter (the Judkins right catheter did not provide enoughbackup to cross the tricuspid valve) into the right pulmonaryartery. This was exchanged for a 260-cm-long Amplatzextrastiff 0.035-inch (Cook Medical Inc, Bloomington, IN)guidewire. Rapid ventricular pacing to stabilize the prosthesisduring expansion was not anticipated, but to assess stability
during inflation, we first performed a predilatation of thevalve with a 16�40-mm Tyshak balloon (NuMED Inc,Hopkinton, NY) (Movie I in the online-only Data Supple-ment). This balloon remained very stable during inflation, butwe encountered significant difficulty in crossing the valvebecause the tricuspid valve was almost horizontal (Figure 3),and downward pushing force resulted in prolapse of thedevice down toward the inferior vena cava. At this point, afinal decision was made to use a transfemoral EdwardsSAPIEN XT device rather than the transapical one, with itsmuch shorter delivery system, because the transfemoralNovoflex delivery system has a tip that can be deflected to aidin aiming the device in the direction of the tricuspid valve.The device was passed over the valve with significantdifficulty. A partial inflation was performed to stabilize thevalve, and final positioning could then be achieved (Figures 4and 5 and Movie II in the online-only Data Supplement). Atthis point, full inflation of the balloon to 27 mm wasperformed with good expansion and good anchoring of thedevice (Figure 6 and Movie III in the online-only DataSupplement). Echocardiography revealed no complicationsand good valve function with no paravalvular regurgitation(Figures 7 and 8 and Movies IV and V in the online-only DataSupplement). The Novoflex delivery system and sheath wereremoved with surgical closure of the jugular vein.
The patient was extubated on the table and mobilized onday 1. She lost 10 kg in weight in the next 4 days and reportedimmediate improvement in dyspnea symptoms. Postproce-dural transthoracic echocardiography showed that the devicewas well anchored, with no paravalvular leaks. The meangradient across the valve was 3 mm Hg. Oral anticoagulationwas reestablished before discharge.
At 2 months after the procedure, the patient is still in NewYork Heart Association class 1 functional class despitecessation of diuretic treatment.
DiscussionWith the advent of transcatheter aortic valve implantation, anew treatment option has become available for patients with
Figure 3. The Amplaz Extrastiff guidewire is across the degener-ate tricuspid prosthesis into the right pulmonary artery. TheNovaFlex delivery system prolapses inferiorly when pushed fromabove. Note also mitral mechanical prosthesis in background.
Figure 2. Pressure half-time (PHT) measuredover the tricuspid valve confirms severe tricus-pid stenosis with a value of 461 ms.
e158 Circulation August 2, 2011
by guest on June 21, 2018http://circ.ahajournals.org/
Dow
nloaded from

inoperable aortic valve stenosis. The calcified degeneratednative aortic valve has a rough inner surface that acts as aneffective anchor for the prosthesis. The irregular inner surfaceand metal frame of a degenerated bioprosthesis have similarcharacteristics, and form an ideal docking station for atranscatheter valve. This has led to a number of valve-in-valve implants, mostly in the aortic position.1 The first case oftranscatheter valve-in-valve tricuspid valve replacement wasdescribed by Hon et al.2 Their approach was, however, via athoracotomy and direct puncture of the right atrium. This hasdefinite advantages with regard to delivery of the device, butremains more invasive. The first transcatheter tricuspid valve-
in-valve procedure was performed by Leen van Garsse, butdiffered from the case described here in a number of ways:The patient described by van Garse was not a surgicalcandidate, she was placed on extracorporeal circulation forthe duration of the procedure, the valve was deployed underrapid ventricular pacing, and the older 24F Edwards SAPIENdevice was used.3
Using the new Edwards SAPIEN XT device requiredmounting it on the balloon shaft in an orientation opposite toits design. When the balloon is pulled back into the deviceafter exiting the distal end of the delivery sheath, it has thepotential to cause folding or damage to the valve cusps. Wedid not encounter this, and believe that this theoretical risk iswell justified by the smaller caliber of the delivery sheath.
Other potential pitfalls we considered included stability ofthe device within the tricuspid prosthesis; the degeneratebioprosthesis tends to have less bulky calcification than asenile aortic stenosis valve, but the wire frame of the valveadds to the potential of the valve to grip the transcathetervalve, and the low pressure system of the right heart willplace less strain on the new prosthesis. Undersizing of ourtranscatheter valve was a concern, and in the future, one couldconsider larger valves when they become available. Size ofthe access vessel was a consideration, but because of theseverely congested venous system, this concern was un-founded. Crossing of the degenerated tricuspid prosthesis wasdifficult because of its angle and downward prolapsing of thedevice when pressure was applied. A femoral approach mayprove easier, because the route may be straighter with bettertransmission of pushing forces.
This patient presented with a rare combination of prob-lems, and it is unlikely that this procedure would becomewidely used. If indicated, however, it is feasible provided thata large enough device is available and the approach isevaluated carefully. Rapid ventricular pacing and extracorpo-real circulatory support are not mandatory.
Figure 4. Device shown after we crossed the degenerate tricus-pid prosthesis.
Figure 5. To prevent the prosthesis from being pulled all theway back into the right atrium, a partial balloon inflation is done,and the device is then pulled back into position.
Figure 6. Final image showing good positioning of the EdwardsSAPIEN device within the other prosthesis.
Weich et al Transjugular Tricuspid Valve-in-Valve Replacement e159
by guest on June 21, 2018http://circ.ahajournals.org/
Dow
nloaded from

DisclosuresDr Weich is a proctor for implantation of transcatheter aortic valvesfor Edwards Lifesciences.
References1. Webb JG, Wood DA, Ye J, Gurvitch R, Masson JB, Rodes-Cabau J,
Osten M, Horlick E, Wendler O, Dumont E, Carere R, Wijesinghe N,Nietlispach F, Johnson M, Thompson C, Moss R, Leipsic J, Munt B,
Lichtenstein SV, Cheung A. Transcatheter valve-in-valve implantationfor failed bioprosthetic heart valves. Circulation. 2010;121:1848–1857.
2. Hon JKF, Cheung A, Ye J, Carere RG, Munt B, Josan K, Lichtenstein SV,Webb J. Transatrial transcatheter tricuspid valve-in-valve implantation ofballoon expandable bioprosthesis. Ann Thorac Surg. 2010;90:1696–1697.
3. Van Garsse LAFM, ter Bekke RMA, van Ommen VGVA. Percutaneoustranscatheter valve-in-valve implantation in stenosed tricuspid valve bio-prosthesis. Circulation. 2011;123:e219–e221.
Figure 7. Postprocedure continuous waveDoppler shows that the profile has now normal-ized with a reduction of the peak and meangradients to 7 and 3, respectively.
Figure 8. Postprocedure tricuspid inflow Dopp-ler confirms a good result with a pressure half-time (PHT) of 128 ms. MV PHT indicates tricuspidvalve pressure half-time.
e160 Circulation August 2, 2011
by guest on June 21, 2018http://circ.ahajournals.org/
Dow
nloaded from

DoubellHellmuth Weich, Jacques Janson, Jacques van Wyk, Philip Herbst, Pieter le Roux and Anton
Transjugular Tricuspid Valve-in-Valve Replacement
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 2011 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/CIRCULATIONAHA.111.027342
2011;124:e157-e160Circulation.
http://circ.ahajournals.org/content/124/5/e157World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org/content/suppl/2011/07/27/124.5.e157.DC1Data Supplement (unedited) at:
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information aboutOffice. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialCirculationin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on June 21, 2018http://circ.ahajournals.org/
Dow
nloaded from