Embed Size (px)
Citation preview

J. clin. Path. (1954), 7, 318.
THREE CASES ILLUSTRATING THE PRESENCE OFARGENTAFFIN (KULTSCHITZKY) CELLS IN
THE HUMAN GALL-BLADDERBY
A. C. CHRISTIEFrom the Department of Pathology, Royal Cancer Hospital, London
(RECEIVED FOR PUBLICATION MARCH 29, 1954)
Occasionally typical argentaffin (Kultschitzky)cell or so-called "carcinoid " tumours have beendescribed in the human gall-bladder (Joel, 1929;Porter and Whelan, 1939; Bosse, 1943), althoughI have found no mention in textbooks of histologyor pathology of the presence of such cells in themucosa. There is, however, one case report (Kerrand Lendrum, 1936) of a papilloma of this organcovered with intestinal epithelium containing bothPaneth and argentaffin cells. I propose to describethree cases in which the latter type was present.
Materia and MethodsThe material was obtained from operation cases
in which extra sections were cut from routineformalin-fixed paraffin blocks and stained by analkaline silver method, either that of Masson andHamperl as described by Jacobson (1939) orGomori's (1948) hexamine-silver nitrate technique.In Case 3 the argentaffin cells were numerous andseveral histochemical stains were applied.
Being surgical material, most of the gall-bladdersexamined showed evidence of chronic inflamma-tion. Nicholson (1923) has already given amasterly description of the pathological changesin chronic inflammation and, in particular, hasdrawn attention to areas of mucous gland forma-tion, a phenomenon which he has referred to asindirect metaplasia. He found such areas in 24out of 36 inflamed organs removed at operationand remarked that the percentage would probablyhave been increased had more sections beenexamined. He mentioned that Aschoff (1905),Schridde (1909), and Bodnar (1922) had previously,drawn attention to the presence of mucous glands,upon the surface of the fundus of the inflamedgall-bladder. Schridde (1909) also demonstratedthe origin of these glands from the epithelium ofLuschka's tubes in a case of cholecystoduodenalfistula.
Nicholson demonstrated how these tubularmucous glands change their type in a high pro-portion of cases and assume all the structuralcharacters of gastric glands identical with thoseof the pylorus or those of Brunner. His Fig. 6confirms this finding and presents a very similarpicture to that seen in numerous areas in eachof the three cases described below. Seventeen ofNicholson's series of 24 gall-bladders which con-tained mucous glands possessed those of the gastrictype as well in varying numbers and in all stagesof differentiation. He analysed the changes thateventually end in the formation of such gastricglands in the gall-bladder and considered that theywere of two kinds, namely, regressive, leading tothe production of tubular mucous glands and otherchanges characteristic of the intestines, and pro-gressive, culminating in the production of typicalglands of the gastric type. (He considered Brun-ner's glands to be of the gastric type.)As Nicholson has given such a full description
of the changes in the gall-bladder epithelium inchronic inflammatory lesions, it only remains forme to demonstrate that argentaffin cells also occurboth in the high columnar epithelium covering thesurface of the mucous membrane and in theglandular acini. Morphologically the cells arealmost always conical with a broad base in contactwith the basement membrane and tapering towardsa narrow elongated apex, which usually falls shortof the lumen of the gland or the free mucosalsurface as the case may be. The nucleus isusually situated near the middle of the cell andis vesicular with chromatin aggregations oftenmore or less evenly distributed beneath the nuclearmembrane (Fig. 3): such a nuclear pattern hasbeen beautifully depicted by Ciaccio (1906). Theintracellular granules lie between the nucleus andthe basement membrane, that is, they are infra-nuclear. The histological appearances of these
copyright. on D
ecember 1, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.7.4.318 on 1 Novem
ber 1954. Dow
nloaded from

ARGENTAFFIN CELLS IN HUMAN GALL-BLADDER
cells are, in fact, identical with those of the in-testinal argentaffin cells which have been fullydescribed by other workers (Cordier, 1926; Mas-son, 1928; Gillman, 1942).
Case ReportsCase 1.-The wall of the gall-bladder, that of a
man aged 71, is up to 0.3 cm. thick and its mucosain some places is thrown into irregular papillary pro-cesses and in others shows both Luschka's tubes pene-trating into the muscularis and foci of glandular acini,the latter arising both from the surface epitheliumand from the tubes.
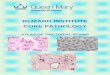
Scattered very irregularly amongst the highcolumnar cells covering the papillary processes arecells with alkaline silver-reducing infranucleargranules which morphologically resemble intestinalargentaffin cells (Fig. 1). Occasionally such cells arepresent in the glandular acini, a feature also depictedin Fig. 1. Goblet cells are rarely seen on the surfaceepithelium, and, when present, bear no relation to theargentaffin cells: both apparently are scattered indis-criminately and very irregularly amongst the highcolumnar cells. Paneth cells are not present. Theunderlying wall is thickened and its musculature ispartly replaced by fibro-cellular connective tissue. Thesubmucosa is only sparsely peppered with chronicinflammatory cells; in fact, the original chronic infec-tive process shows no histological evidence of activity.
Case 2.-The gall-bladder, that of a woman 'aged60, measures 9.5 cm. in length and up to 2.8 cm. indiameter, with a wall averaging 0.2 cm. in thickness.Its mucosa has a wrinkled surface.
Microscopically there is a considerable overgrowthof fibrous tissue involving all three coats. Approxi-mately 5.0 cm. of mucosal surface is included in thesections, although, in parts, the covering epithelium isdenuded. Luschka's tubes penetrate deeply into themucosa, especially in one area where there are
... .... '.......:.S.J@ ~~~'
| ~~~~~~~~~~~~~~~~~. =.x.-....
* Y'........ ....N Y .. S
FiG. l.-Case I, showing argentaffin cells, both on a papillarvprojection of the mucosa (right side) and a solitary cell in a
glandular acinus (lower left corner). Masson-Hamperl's am-
moniacal siver stain. x 200.
K:.~~ ~I'S.
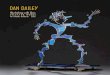
FIG. 2.ase 2, showing argentaffin cells, both solitary and ingroups, in glandular acini. One group (in centre) has beensectioned obliquely. Masson-Hamperl's ammoniacal silverstain. x 200.
numerous coiled glands, many being of Nicholson's" gastric " type. Here and there in this nidus of aciniare cells morphologically resembling the argentaffincells of the intestine and containing infranuclearammoniacal silver-reducing granules (Fig. 2). In onearea, in adjoining acini (almost certainly part of thesame coiled gland system), there are two clumps ofsuch cells, the larger containing eight cells in apposi-tion. In addition, there is an occasional isolatedargentaffin cell in the same gland system (Fig. 2).When present in mucous glands these cells are, as inBrunner's glands, usually found lying at the peripheryof the acinus against the basement membrane andseparated from the lumen by mucous cells. In thepapilliferous mucosa overlying this group of glandsthere are goblet cells and an occasional argentaffincell amidst the high columnar epithelial cells. Else-where in the mucosa there are numerous small fociof glandular acini which, however, contain no argent-affin cells. Paneth cells are absent throughout themucosa.
Case 3.-The specimen is that from a woman aged49. The macroscopic description of this specimen isnot available. Microscopically the wall is slightlythickened due to a moderate overgrowth of fibroustissue involving the submucosa, muscularis, and sub-serosa. The covering mucosa is papilliferous in placesand partly denuded of its overlying epithelium. Themost prominent feature throughout most of themucosa is a large number of tubular glarrds which
319
copyright. on D
ecember 1, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.7.4.318 on 1 Novem
ber 1954. Dow
nloaded from

A. C. CHRISTIE
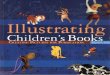
FIG. 3.-Case 3, showing a clump of argentaffin cells in a glandularacinus. In the cell on the extreme right of the clump, the typicalchromatin pattern in the nucleus can be discerned. Gomori'shexamine-silver nitrate stain. x 900.
have arisen, both from the surface epithelium andfrom deeply penetrating Luschka's tubes, the latterhaving penetrated almost completely through the mus-cularis in some places. The glands are of both thetypes described by Nicholson (1923), but the majoritybelong to his " gastric " variety and do, in fact, closelyresemble Brunner's glands. The mucus in both typesof glands gives a strongly positive reaction with theperiodic-acid-Schiff stain for demonstrating the1,2-glycol linkage (as would occur in mucopoly-saccharides). Argentaffin cells are very unevenlydistributed both amongst the glandular mucous cellsand the tall columnar surface epithelium. Quite oftenthey appear in clumps (Fig. 3), and in one relativelysmall group of glands, approximately 1 mm. in dia-meter and just beneath the surface epithelium, 32 suchcells are present, one clump alone containing 13 inapposition. In other areas numerous glandular aciniare seen without a single argentaffin cell. No Panethcells are present. The lamina propria is pepperedwith chronic inflammatory cells, mainly lymphocytesand plasma cells, and there is also capillary conges-tion of a moderate degree.The cells under discussion react positively with the
following stains, as in the case of the intestinalargentaffin cells (1) Gomori's (1948) hexamine-silvernitrate method; (2) Cordier and Lison's (1930) diazodye method: the technique as described by Jacobson
(1939) was used and the particular dye was " echtrot-salz" supplied by G. T. Gurr, London; (3) Schmorl'sferric ferricyanide reduction test (Lillie and Burtner,1953): the granules stain a blue-green colour.As only formalin-fixed, paraffin-embedded blocks
are available, I have been unable to carry out Baker'sacid haematein and pyridine extraction test for phos-pholipines. It has recently been shown (Christie,1954) that the granules give a positive reaction in thatthey stain black in the first part of the test but notin the second-namely, the pyridine extraction-acidhaematein test.The chromaffin reaction could not be observed as it
cannot be applied to tissues previously treated withformalin (Pearse, 1953).
DiscussionIt is of paramount importance to decide first
whether the cells under discussion are, in fact,argentaffin (Kultschitzky) cells such as occur inthe intestine. That this is so can hardly be indoubt both from morphological appearances andstaining reactions. Masson (1928) has given anadmirable account of these cells in the humanintestine and his description applies equally wellto the cells described in the above three cases.The granules within these cells also show histo-chemical similarities with the intestinal argentaffincells, for they give a positive reaction with Cordierand Lison's diazo dye technique, and also possessstrongly reducing properties as shown by theirability to reduce both alkaline silver and ferricferricyanide solutions. Whilst there are other sub-stances occurring in the tissues which have equallystrong reducing tendencies, they are not concen-trated as fine granules in such a characteristicinfranuclear position within the cell as in boththese cells and in the typical argentaffin cell ofthe human intestinal mucosa.
It is very likely that such cells are frequentlypresent in areas of intestinal metaplasia in in-flamed gall-bladders but have not been noted, asthe usual stains employed in routine histologicalwork do not show them up very clearly, although,if the eosin be properly differentiated in the stan-dard haematoxylin and eosin stain, they can befairly easily discerned if sought after, for thecharacteristic granules are quite strongly eosino-philic (Masson, 1928). If the fixative employedcontains alcohol then the granules are no longerseen by any staining technique even if formalinis also present in the fixative (Masson, 1928).However, formalin or formalin-containing mix-tures are not the only fixatives of these cells asthe granules are also preserved by potassiumdichromate which gives them a yellow tint (even
320
.. .; ...4
.....N
copyright. on D
ecember 1, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.7.4.318 on 1 Novem
ber 1954. Dow
nloaded from

ARGENTAFFIN CELLS IN HUMAN GALL-BLADDER
in the complete absence of formalin) and byosmium tetroxide which both preserves andblackens them due to its reduction to lo,veroxides.
Extensive histochemical studies could not beundertaken as only formalin-fixed tissue wasavailable.A point of considerable interest is the very
uneven distribution of these cells. Sometimes, asin Cases 2 and 3 (Figs. 2 and 3, respectively), smallclumps of them are seen. In the latter case suchclumps contain more cells in apposition with oneanother than is usually seen in intestinal cryptsof Lieberkuhn. (I have previously once seen suchan aggregation in a small cystic space lined byintestinal epithelium in a teratoma of the ovary.)They do not appear to be related in any specificway to the other cell types seen in metaplasticareas, such as goblet or mucous cells, but ratherseem to occur for no apparent reason. In areasof intestinal metaplasia in the stomach, Panethcells are also often seen, but they have not beenobserved in the above three cases, although, asmentioned above, Kerr and Lendrum (1936) didsee them in their case of a papilloma covered withintestinal epithelium. Although there is someevidence of an active low-grade chronic infectiveprocess in the underlying mucosa in the secondand third cases, the actual inflammatory lesion,as judged by histological evidence, is no moresevere in the mucosa where the argentaffin cellsare aggregated than where they are absent.
I have thus no explanation to offer concerningthe function of these cells in the sites where theyare present, or, for that matter, in the gall-bladderas a whole, except to say that it appears they arelikely to occur in intestinal epithelium whereverit may arise. However, their presence in suchepithelium is certainly not invariable and this isalso the case in areas of intestinal epithelium interatomata. The presence of these cells in clumpsdoes suggest one or other (or perhaps both) of twopossibilities; namely, either that when conditionsare such in a particular area for one cell-type toappear, then the stimulus affects the differentiationof more than one stem cell with the consequent
production of a group of similar cells; or, alter-natively, that when one cell differentiates in aparticular direction such as to form an argentaffincell, then this cell remains true to type for a timeat least, and divides to form similar daughter cellswhich, in turn, may divide to produce a group ofspecialized cells as in Fig. 3 of Case 3. Thepresence of such clumps also suggests a likelysite for possible tumour formation.The occurrence of argentaffin cells in this organ,
as in teratomata, indicates that direct absorptionof precursor substances from the intestine is notesssential for the formation of the chemical sub-stance (or substances) composing the granules.
SummaryThree cases are described in which chronically
inflamed gall-bladders removed at operation con-tain areas of intestinal metaplasia with thepresence of typical argentaffin (Kultschitzky) cellsboth amongst the high-columnar surface epithelialcells and within the mucous glands. The identityof these cells is established both on morphologicaland histochemical grounds. An explanation is thusafforded for the rare carcinoid tumours of thisorgan.
I am indebted to Mr. F. E. Speed for the photo-micrographs and to Mr. C. G. Chadwin for the histo-logical sections.
REFERENCESAschoff, L. (1905). Verh. dtsch. path. Ges., 9, 41.Bodnar, L. (1922). Vlirchows Arch. path. Anat., 238, 359.Bosse, M. D. (1943). Arch. Path., Chicago, 35, 898.Christie, A. C. (1954). Nature, Lond., 173, 589.Ciaccio, C. (1906). C. R. Soc. Biol., Paris, 60, 76.Cordier, R. (1926). Arch. Biol., Paris, 36, 427.
and Lison, L. (1930). Bull. Histol. Tech. micr., 7, 140.Gillman, J. (1942). S. Afr. J. med. Sci., 7, 144.Gomori, G. (1948). Arch. Path., Chicago, 45, 48.Jacobson, W. (1939). J. Path. Bact.. 49, 1.Joel, W. (1929). Zbl. allg. Path. path. Anat., 46, 1.Kerr, A. B., and Lendrum, A. C. (1936). Brit. J. Surg., 23, 615.Lillie. R. D., and Burtner, H. J. (1953). J. Hittocheni. Cytochem., 1,
87.Masson, P. (1928). Amer. J. Path., 4, 181Nicholson, G. W. (1923). J. Path. Bact., 26, 399.Pearse. A. G. E. (1953). Histochemistry. Theoretical and Applied,
p. 346. Churchill, London.Porter, J. E., and Whelan, C. S. (1939). Amer. J. Cancer, 36, 343.Schridde. H. (1909). Die ortsfremden Epithelgewebe des Menschen.
Fischer, Jena.
321
copyright. on D
ecember 1, 2021 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.7.4.318 on 1 Novem
ber 1954. Dow
nloaded from