Embed Size (px)
Citation preview

ILA: DIABETES
Ass Prof Dr. Gihan Sharara
• Questions (Based on basic biochemistry)
• What is hyperglycemia?
• Why was there hyperglycemia in this patient?
• Explain why there is increased urination (polyuria) with this
high blood glucose?
• Why Hoda had increased appetite (polyphagia) despite high
glucose levels?
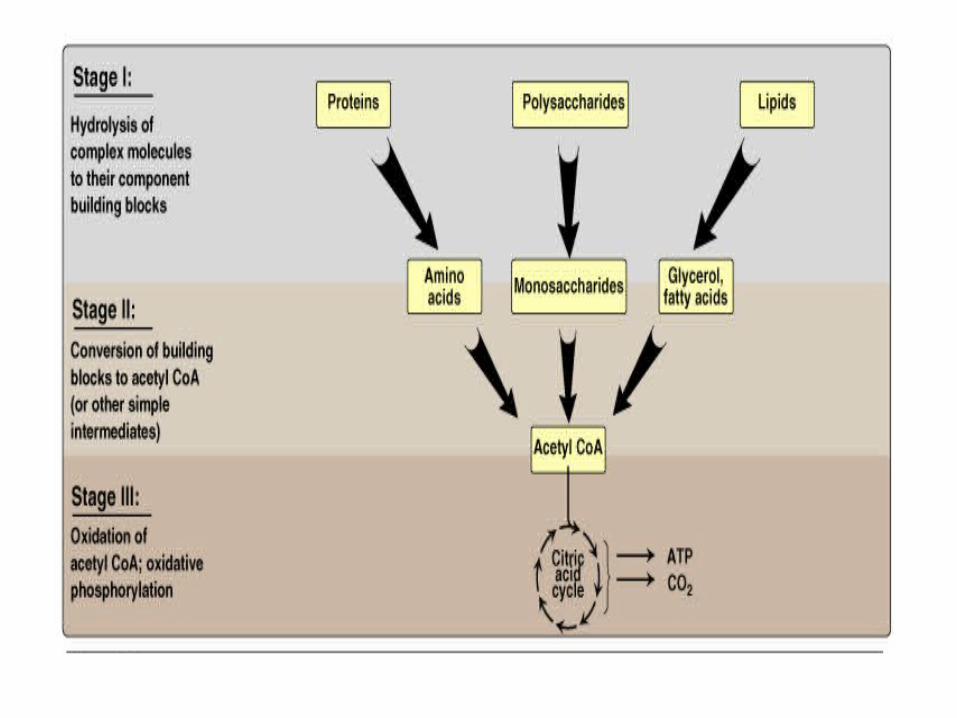
• Discuss normal glucose metabolism
• Suggest the possible alterations in glucose storage and break
down that might occur in this clinical problem.
What is hyperglycemia?
• Hyperglycemia is the elevation of blood
glucose levels above the normal range.
• Normal fasting blood glucose:
• 70 – 100mg/dl
Why was there hyperglycemia in this patient?
• INSULIN DEFICIENCY:
1. decreases uptake of glucose by cells.
2. insulin dependent enzymes are less active
• Net effect:
A. inhibition of glycolysis
B. Inhibition of glycogenesis (glycogen synthesis)
C. stimulation of gluconeogenesis
D. Stimulation of glycogenolysis (glycogen degradation)
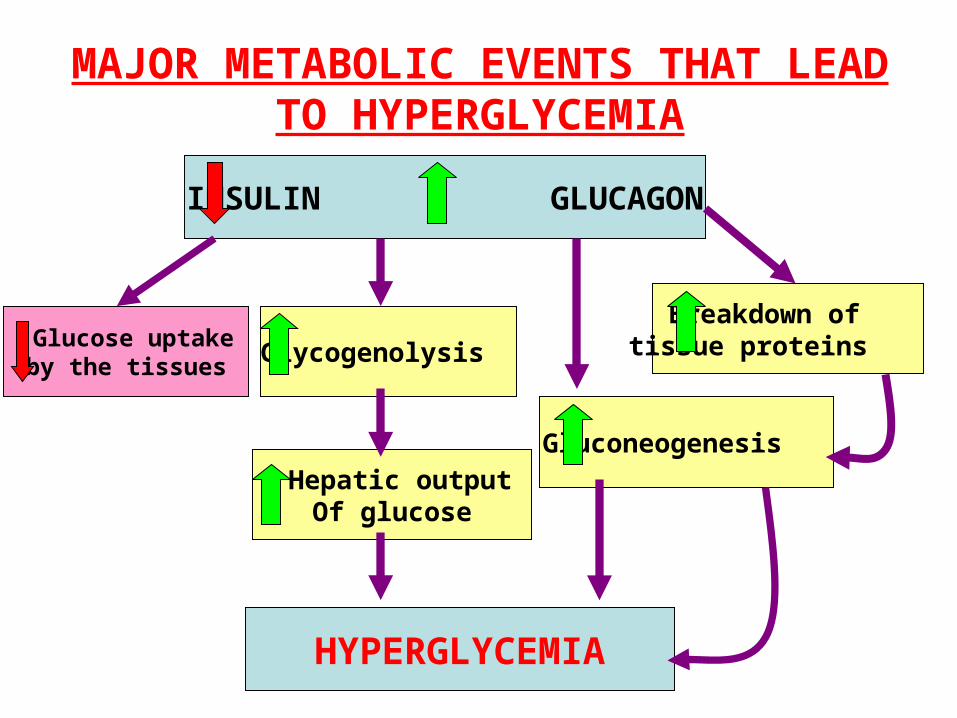
MAJOR METABOLIC EVENTS THAT LEAD TO HYPERGLYCEMIA
INSULIN GLUCAGON
Glucose uptake by the tissues Glycogenolysis
Hepatic output Of glucose
HYPERGLYCEMIA
Gluconeogenesis
Breakdown of tissue proteins
• Explain why there is increased urination
(polyuria) with this high blood glucose?
• When the blood glucose levels exceed the
renal sugar threshold glucose is excreted
in urine (glucosuria)
• Due to the osmotic effect of glucose, more
water accompanies glucose excretion
Polyuria (increase in volume of urine excretion)
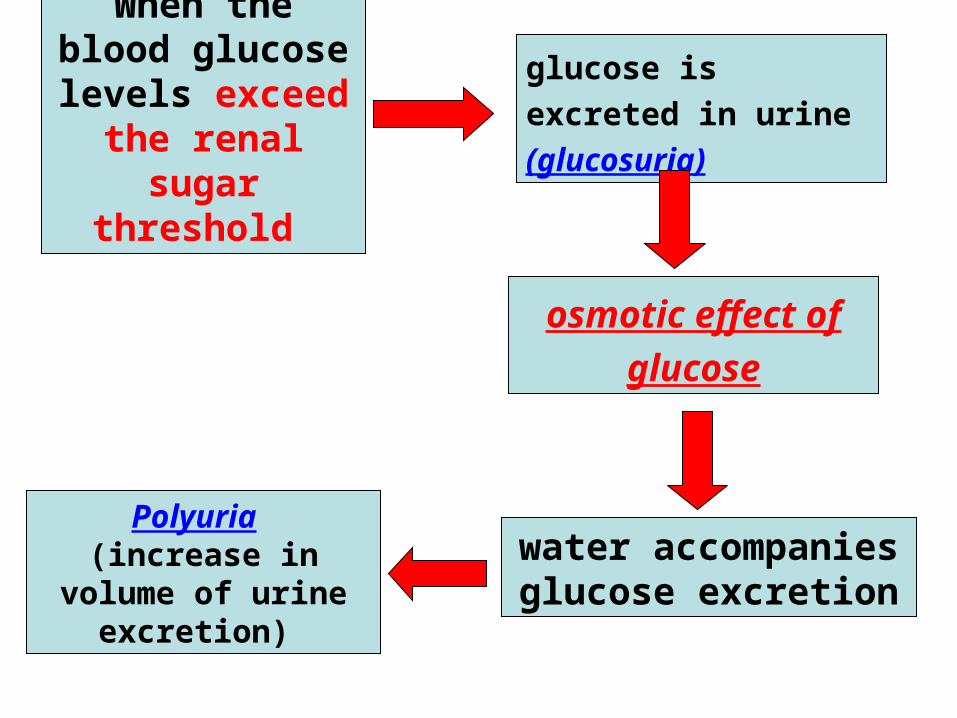
When the blood glucose levels
exceed the renal sugar threshold
glucose is excreted in
urine (glucosuria)
osmotic effect of
glucose
water accompanies glucose excretion
Polyuria (increase in volume of urine excretion)
• To compensate for the water loss
• Thirst centre is stimulated
• More water is is taken (polydepsia:
always thirsty, drinks a lot)
• Why Hoda had increased appetite (polyphagia) despite high glucose levels?
• Although the blood glucose level is high but glucose is not taken up by the cells due to insulin deficiency therefore the cells are starved
• The patient will take more food (polyphagia) to compensate for the loss of glucose and also loss of protein
Although the blood glucose
level is high
BUT glucose is NOT taken up by the cells
due to insulin deficiency
the cells are starved
The patient will take more food (polyphagia) to compensate for the decrease of glucose
and ATP intracellulary
BUT

• Discuss normal glucose metabolism
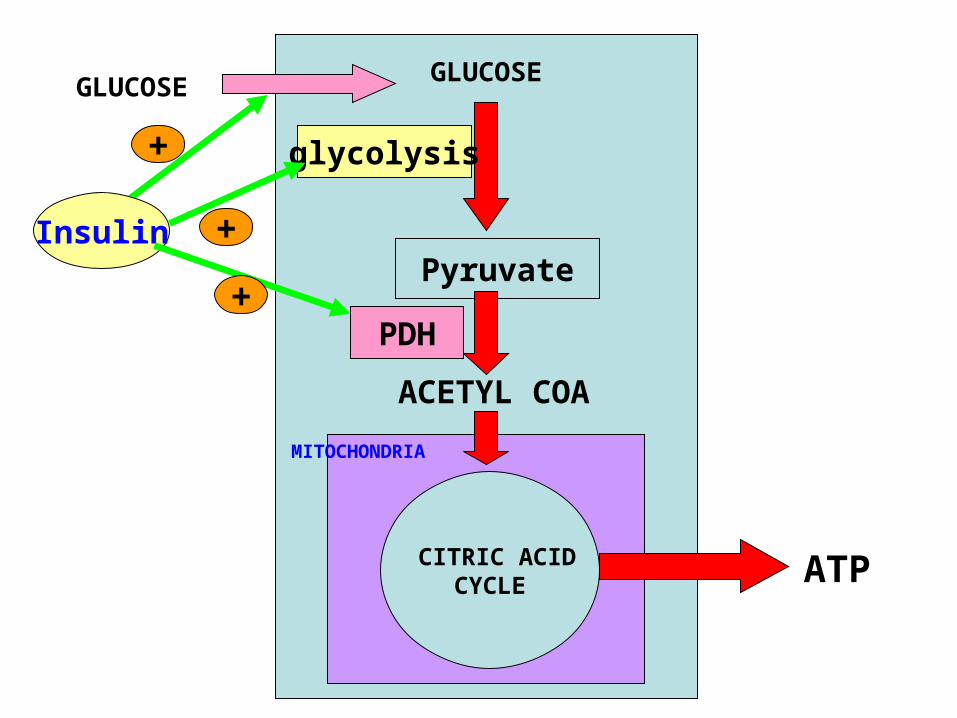
GLUCOSE
Insulin
+
GLUCOSE
glycolysis
+
ACETYL COA
Pyruvate+
PDH
CITRIC ACID CYCLE
MITOCHONDRIA
ATP
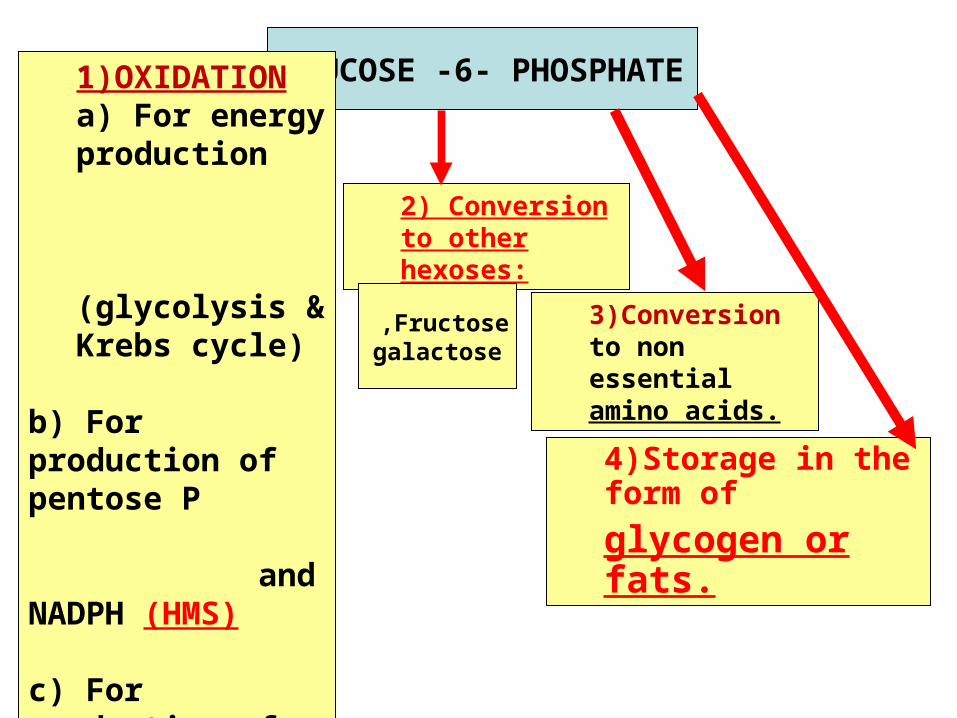
GLUCOSE -6- PHOSPHATE
1)OXIDATIONa) For energy production (glycolysis & Krebs cycle)
b) For production of pentose P and NADPH (HMS)
c) For production of uronic acid.
2) Conversion to other hexoses:
3)Conversion to non essential amino acids.
4)Storage in the form of
glycogen or fats.
Fructose ,galactose
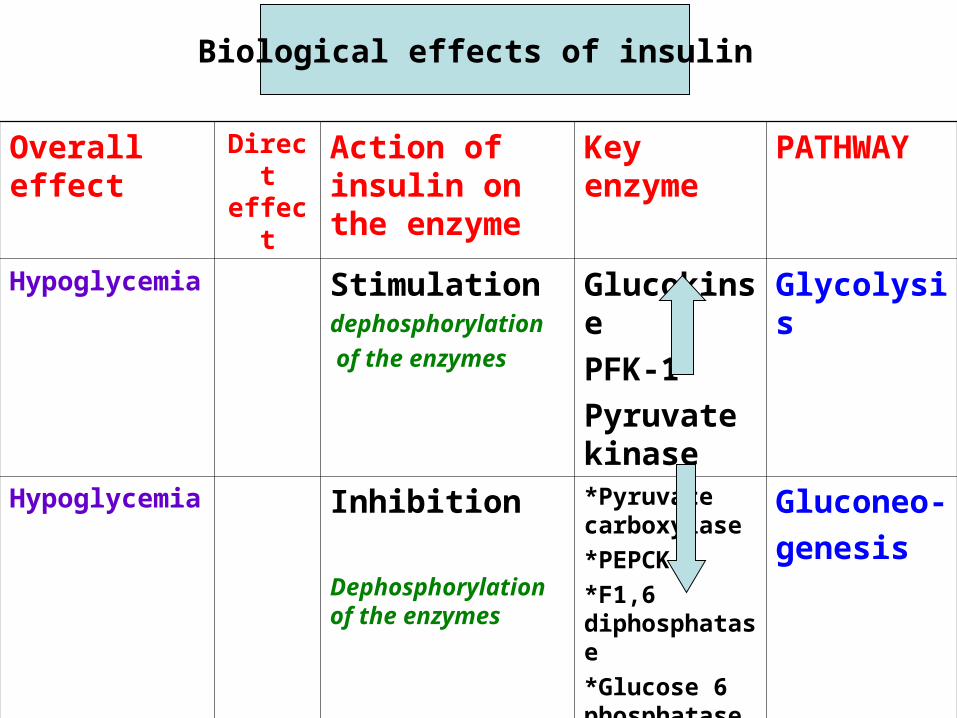
Biological effects of insulin
PATHWAYKey enzyme
Action of insulin on the enzyme
Direct effect
Overall effect
GlycolysisGlucokinse
PFK-1
Pyruvate kinase
Stimulation dephosphorylation
of the enzymes
Hypoglycemia
Gluconeo-
genesis
*Pyruvate carboxylase
*PEPCK
*F1,6 diphosphatase
*Glucose 6 phosphatase
Inhibition
Dephosphorylation of the enzymes
Hypoglycemia
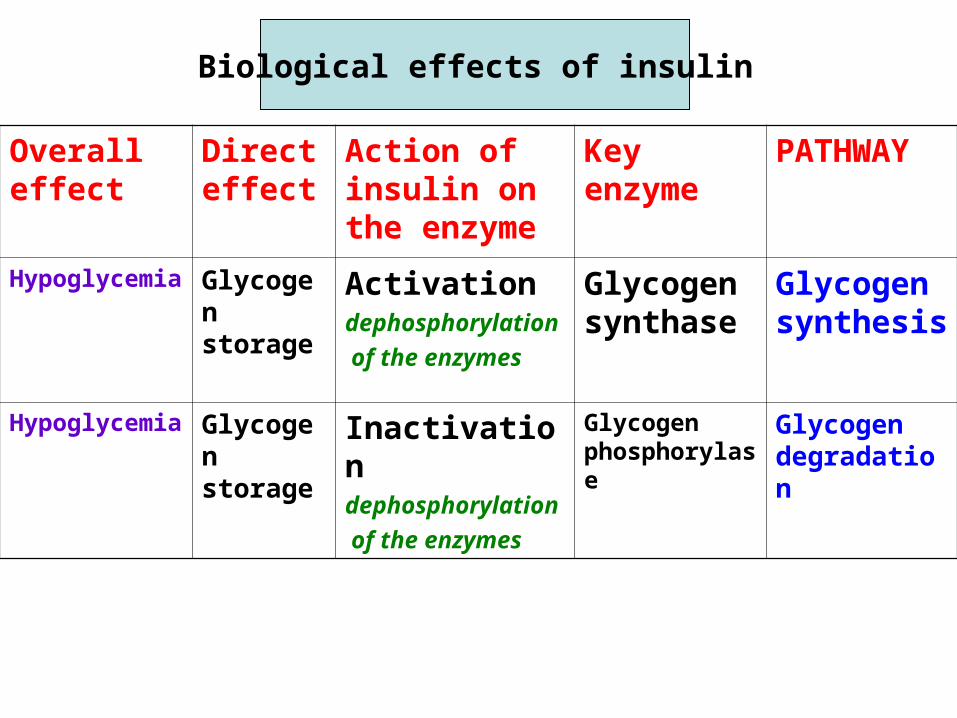
PATHWAYKey enzyme
Action of insulin on the enzyme
Direct effect
Overall effect
Glycogen synthesis
Glycogen synthase
Activationdephosphorylation
of the enzymes
Glycogen storage
Hypoglycemia
Glycogen degradation
Glycogen phosphorylase
Inactivationdephosphorylation
of the enzymes
Glycogen storage
Hypoglycemia
Biological effects of insulin
• In Diabetes Mellitus all these effects are reversed because
• INSULIN
• • GLUCAGON
A. inhibition of glycolysis
B. Inhibition of glycogenesis (glycogen synthesis)
C. stimulation of gluconeogenesis
D. Stimulation of glycogenolysis (glycogen degradation)
• Suggest the possible alterations in
glucose storage and break down that
might occur in this clinical problem.
A. Inhibition of glycogenesis (glycogen
synthesis)
B. Stimulation of glycogenolysis
(glycogen degradation)
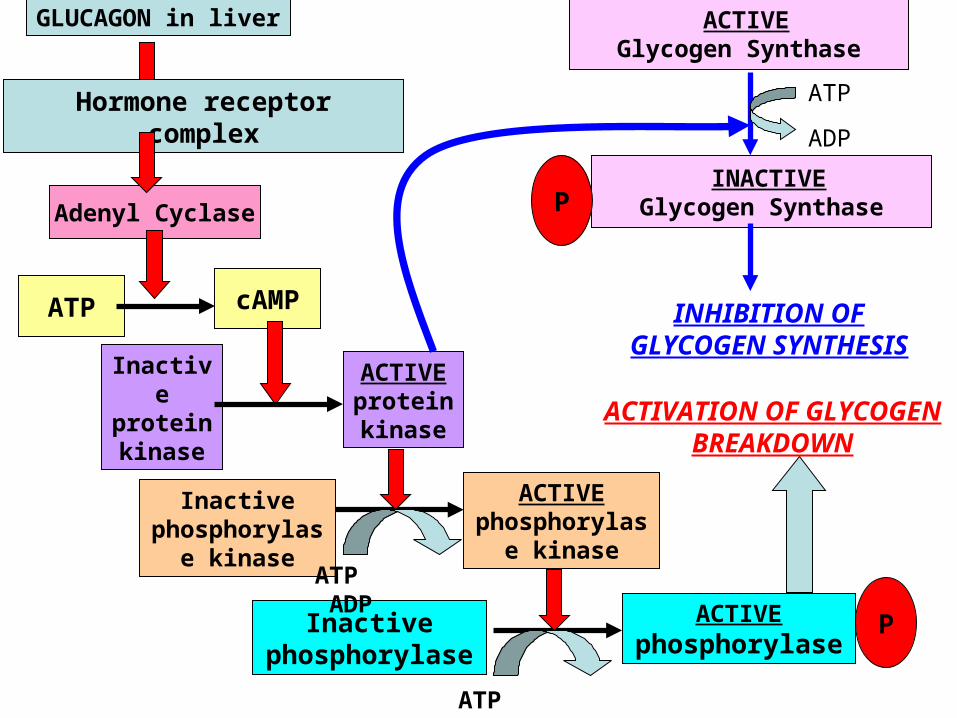
GLUCAGON in liver
Hormone receptor complex
Adenyl Cyclase
ATP cAMP
Inactive protein kinase
ACTIVE protein kinase
Inactive phosphorylase
kinase
ACTIVE phosphorylase
kinase
Inactive phosphorylase
ACTIVE phosphorylase
P
ATP ADP
ATP ADP
ACTIVATION OF GLYCOGEN BREAKDOWN
ACTIVE Glycogen Synthase
INACTIVE Glycogen Synthase
ATP
ADP
INHIBITION OF GLYCOGEN SYNTHESIS
P
ATP cAMP
Inactive protein kinase
ACTIVE protein kinase
Inactive phosphorylase
kinase
ACTIVE phosphorylase
kinase
Inactive phosphorylase
ACTIVE phosphorylase
P
ATP ADP
ATP ADP
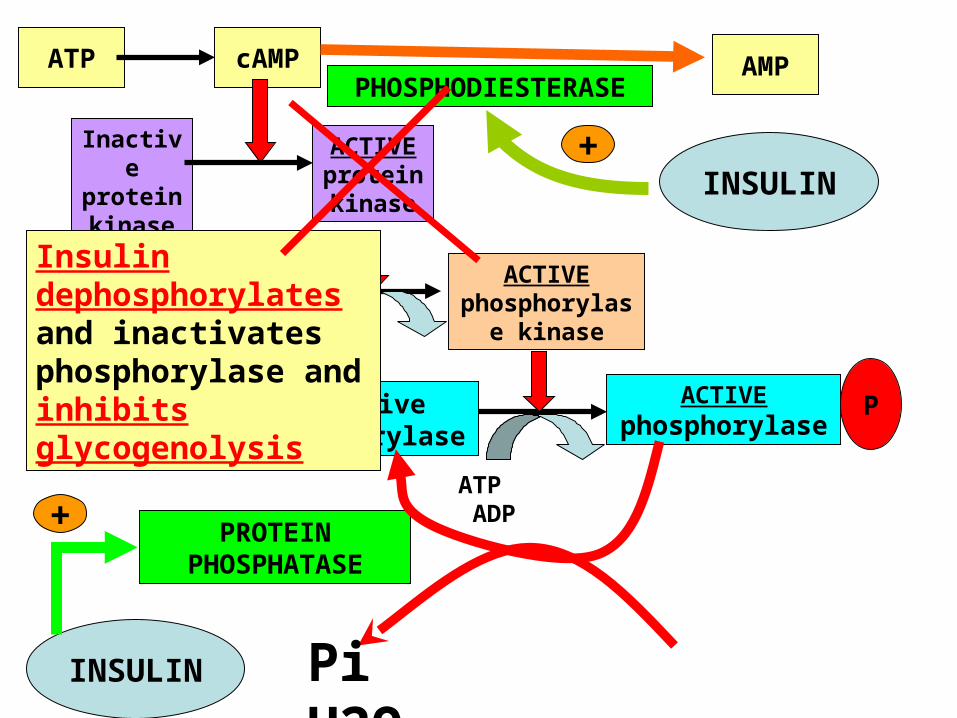
PHOSPHODIESTERASEAMP
INSULIN+
INSULIN
PROTEIN PHOSPHATASE
Pi H2O
+
Insulin dephosphorylates and inactivates phosphorylase and inhibits glycogenolysis
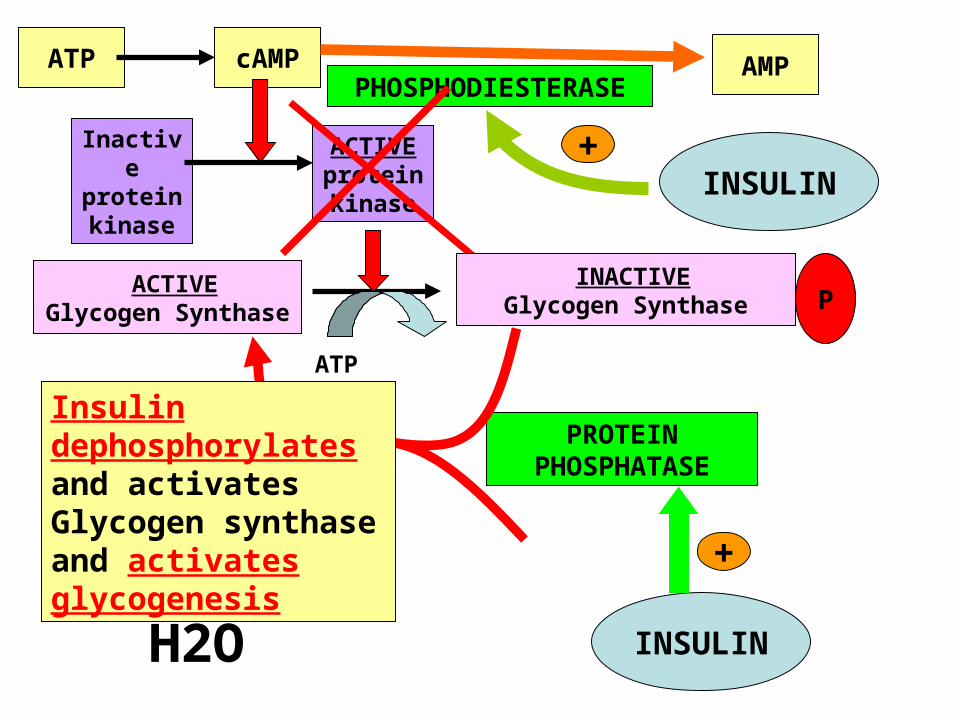
ATP cAMP
Inactive protein kinase
ACTIVE protein kinase
P
ATP ADP
PHOSPHODIESTERASEAMP
INSULIN+
INSULIN
PROTEIN PHOSPHATASE
Pi H2O +
ACTIVE Glycogen Synthase
INACTIVE Glycogen Synthase
Insulin dephosphorylates and activates Glycogen synthase and activates glycogenesis
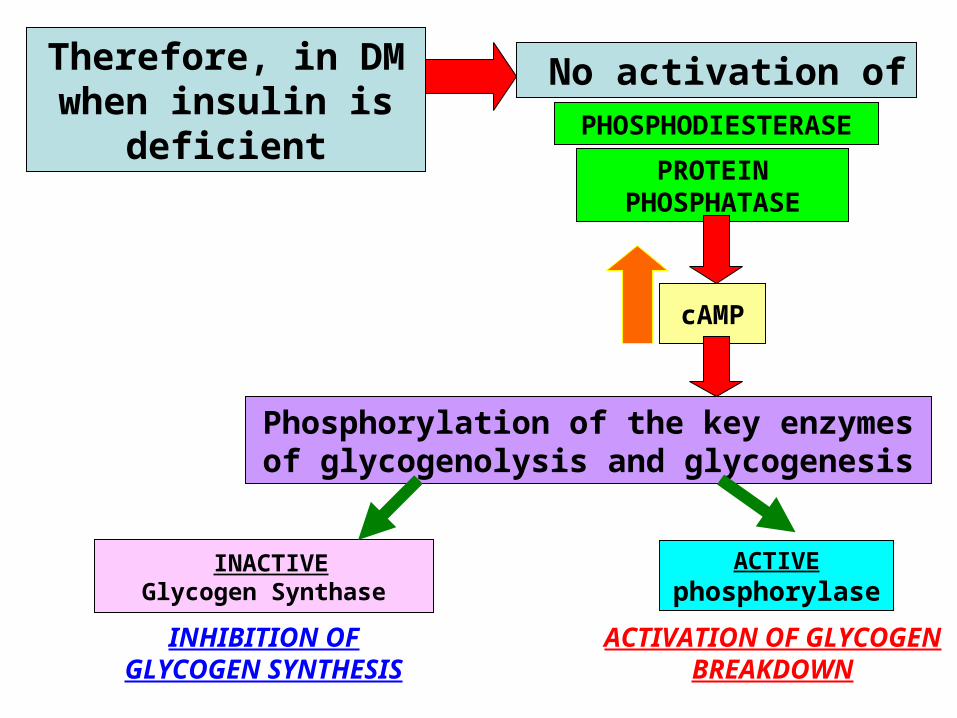
Therefore, in DM when insulin is
deficientPROTEIN
PHOSPHATASE
PHOSPHODIESTERASE
No activation of
cAMP
Phosphorylation of the key enzymes of glycogenolysis and glycogenesis
INACTIVE Glycogen Synthase
INHIBITION OF GLYCOGEN SYNTHESIS
ACTIVE phosphorylase
ACTIVATION OF GLYCOGEN BREAKDOWN