Embed Size (px)
DESCRIPTION
Citation preview

NOT SO TALL A STORYShe was the only one who saw what happened to two-year-old Andy that day. So, even though Billy Jo wasjust six years old at the time, it made sense to put her on as the first witness for the defense. She walked tothe stand, carrying a pillow to boost her up to the microphone so the jurors could hear her small voice inthe cavernous, New Deal courtroom. Here is what she said:
I was visiting my older sister [Sally]…and I asked if [my cousin] Andy and I could go out to play forawhile, and we played [in the back yard]…of Sally’s house…Then Andy found a hole in the fence andthen he went over in the neighbor’s yard and I followed him …He got on the neighbor’s steps and Igot on…and I tried grabbing him…and I grabbed him around the waist but he pulled away and hefell down the [concrete] steps. His legs sort of hit mine and we went doing somersaults down and Iended up on top of him and he was holding his hand over his head sort of like this and then I ran inthe house and got [my sister]…He was…still laying there, starting to cry.
As Billy Jo finished her story, she proudly displayed the battle scar on her knee that she got falling downthe steps with Andy that day. Andy did not survive to tell the story. He died four days later, suffering thecomplications of the intracranial injuries he sustained in the fall.
When Andy stopped breathing and turned blue days after his tumble down the concrete steps, he was in
T H E W A R R I O R • W i n t e r 2 0 0 4 27
A Matter of Gravity
E L A I N E W H I T F I E L D S H A R P , T L C ‘ 9 8
A Matter of Gravity1” is Part II of a three-part series. In Part I, “The Elephant on theMoon,2” we saw that in the world of science, if one sets out to prove a hypothesis,one risks proving a fallacy and creating pseudo science rather than reliable science.The syndrome called “shaken baby syndrome” or “SBS” is based on faulty assump-tions that, in the past half century, many set out to prove, but few set out to test.While shaking may cause injury to a child’s brain stem, cranio-cervical junction andupper cervical cord, it has now been falsified as a mechanism of causing intracra-nial bleeding above the convexities of the brain and to other areas of the brain.
In Part II, we look at another area of pediatric head injury—short falls—and we askthe question: Can they kill? Or, are the stories of short falls nothing more than talltales woven by the guilty to obscure their evil acts of abuse? And, what of storiesof children who fall and seem fine, only to fail and die later? Can some childrenexperience a lucid interval with few or no symptoms after a traumatic brain injury(TBI) caused by a short fall or an alleged act of lethal shaking?
These are forensic issues of “mechanism of injury”—how much gravity on thehead is too much?—and “timing of injury”—can there be a delay between TBI anddeath? These are questions that defendants charged with child abuse by bluntimpact and/or shaking must be able to answer. If they do not, twelve angry people,bent on avenging the death of an innocent, surely will.

28 T H E W A R R I O R • W i n t e r 2 0 0 4
the sole care of his mother’s boyfriend,Steve. It didn’t take long for the doctors atthe local hospital to accuse Steve ofkilling Andy by violently shaking andslamming his head down with forceequivalent to a two-story drop, head firstonto concrete. The nature of the injurieshad to be intentional and could not havebeen accidental, they reasoned. And,claimed the doctors, Andy’s injuries hadbeen “inflicted” just minutes before Steveran into the emergency room (ER) withthe limp and lifeless toddler in his arms.They as much as said, “Steve did it.”
The two main pillars of the State’s foren-sic case—mechanism of injury and tim-ing of injury—had been formed by thetreating physicians even before the policewere called. These were the twin pillarsupon which the State would build its caseagainst Steve for felony murder. If con-victed, he would spend 25 years to life inprison.
Only Billy Jo knew the real story.
FAULTY FOUNDATIONSThe same pillars of the State’s forensiccase against Steve are typically employedin most cases of alleged shaken-baby-impact syndrome. But they have no solid,scientific foundation.
The fact is that short falls do kill.Frequently, the injuries caused by shortfalls involving impact to the head are the
same as those described in so-called“shaken-baby-syndrome” (SBS) cases:Subdural hematomas,3 subarachnoidhemorrhages,4 retinal hemorrhages,5
brain edema6 and diffuse axonal injury.7
The diagnosis of pure shaking (withoutimpact) is often made because there areno bumps or bruises on the head.However, bangs to the head on some sur-faces do not always leave a mark.8
The fact is that claims by the State’s“experts” that they can pinpoint the timeof injury to minutes or hours and, bydoing so, identify the culprit, are scientif-ically unreliable.
As with most suspect “science,” the prob-lem in the area of pediatric head injurycausation and timing of injury is one offocus. Many physicians were taught inmedical school and in practice to believethat children with SDH’s, SAH’s, RH’sand/or cerebral injury (such as DAI) havebeen either violently shaken and/orslammed down with massive force.Accounts of accidental short falls relatedby frantic parents and caretakers in ER’sare ruled out in the differential diagnosisas “inconsistent” with the “evidence,”that is, as mere tall stories to cover uptheir crimes. Pediatrician DavidChadwick, M.D. wrote in 1991 in TheJournal of Trauma:
In children whose injuries are inflict-ed, parents typically invent accidenthistories which they hope will be
accepted by health care providers.Since most falls of over 10 feet usu-ally require that the fall occur out-doors (from a window, balcony, orother such location), caretakers maynot wish to risk the possibility that ahistory could be proven false by aneighbor or passerby. It is also verypossible that many lay persons believethat short falls may be fatal for chil-dren and are surprised to encounterskepticism. The best explanation of thefindings for the…children who die[] isthat the history was falsified.(Emphasis added.)
The mere existence of the injury is com-monly used to infer the element of inten-tionally-inflicted injury through the useof massive force. One court outlined thedanger of this type of faulty reasoningwith the following syllogism:
1. Some children who suffer subduralhematomas are children who havebeen subjected to trauma or forcesuch as that sustained by a fall froma multistory building or being unre-strained in a high-speed automobileaccident.
2. This child sustained a subduralhematoma;
3. Therefore, this child was subjected totrauma or force equal to or exceedingthat caused by a fall from a multisto-ry building or being unrestrained in ahigh-speed automobile accident.9
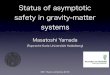
Infant Skull Showing "A-shaped" Lamdoidal Suture.A child who falls and hits his or her head on the occiput, i.e., the back of the head, where the plates of the skull
have not fused at the "A-shaped" lamdoidal sutures, is at much greater risk for injury. The skull is weak here and sothe brain is more vulnerable to injury. Think of it like this: The ice on a lake is weakest at the points where thecracks converge. Blows to the back of an infant's head may be lethal because the material properties are different.
A MATTER OF GRAVITY

T H E W A R R I O R • W i n t e r 2 0 0 4 29
The error of the syllogism is that justbecause some children suffer TBI byfalling from buildings or from car acci-dents does not prove that all childrenwho suffer TBI have fallen from a build-ing or have been in a car accident or havebeen subjected to equivalent forces.
THE BIRTH OF THE BEASTWe join this sorry tale of accusing parentsof falsifying stories about short falls caus-ing injury to their children in 1977, theyear when Ray E. Helfer, M.D., a physi-cian from Michigan State University(MSU) looked through old medicalrecords and reported incidents wherechildren fell out of beds and from coun-ters. Earlier, physicians who claimed SBSwas the real mechanism of SDH’s, SAH’s,DAI and RH’s, had warnedthat tales of short falls wereto be rejected. As childabuse accusations gatheredmomentum and as moreparents professed their inno-cence, Helfer and his col-leagues were determined toprove that injuries fromshort falls do not causesevere head injuries. Hewrote in Pediatrics:
Occasionally, a child whois reported to have fallenout of bed presents with askull fracture, cerebraledema, retinal hemor-rhage, subdural hematoma,and/or epidural hemor-rhage. These severe injuriesare discrepant with the history; it isoften the discrepancy that indicateschild abuse.” (Emphasis added.)
At the outset, Helfer had fallen into thetrap of confirmation bias, one of the hall-marks of unreliable “science.” Heassumed that skull fractures, cerebraledema, RH’s, SDH’s, and/or epiduralhemorrhages “indicate[] child abuse.”
With faulty hypothesis in hand, Helferstudied the reports of 246 children agedsix-months to five years old who had fall-en out of a bed, a crib or from an exam-ining table in the hospital, and from bedsand couches at home. All were falls of 36inches or less. Of the 85 incidents report-ed in hospitals, one child fractured hisskull when he fell from an examining
table. Of the 161 children who fell fromshort heights in the home, two fracturedtheir skulls. According to Helfer, none ofthe three children with skull fractures sus-tained serious head injury.
Among many design and interpretationflaws in Helfer’s study, the claim that “noserious head injury” resulted was madefor children injured from 1969 to 1975,a time when testing for the sequelae oftraumatic brain injury (TBI), such asneuropsychological tests, was less devel-oped and much less available than it istoday. In other words, there is nothing inthe study to convince the reader that aTBI associated with the skull fracturewas, in fact, reliably ruled out.
There is also no mention of follow up
MRI scans or EEG’s to rule out TBI and,instead, only a vague reference to “physi-cians records.” One of the hallmarks ofpeer review literature in medicine and sci-ence is that the reader (i.e., the peer) hasreliable data to enable her to form anindependent judgment about the validityof the author’s conclusions. Even withoutmore data, Helfer’s conclusions are notreliable for, as any lawyer representingtraumatically-brain-injured clientsknows, lack of gross neurological deficitdoes not mean that the person has notsustained a TBI. It is only when a childgrows that the sequelae of a TBI maybecome obvious.
Another flaw in the Helfer study was thatit was based on inductive reasoning.
From that fact that he had not been ableto find many severe injuries in his study,he concluded that such examples are“rare” and/or a parental cover up, writing,“From this study we must conclude thatsevere head injury and CNS damage orinjury of any type are extremely rarewhen children, aged five years or less, fallout of bed.”
Even if one accepts Helfer’s flawed analy-sis, “rare” does not rule out the possibili-ty that serious and fatal head injuries maybe caused by a short fall. There are sever-al examples in the clinical literature wherechildren who fell from short heights suf-fered fatal head injury. (More on thislater.)
The main forensic flaw in Helfer’s studywas that it made no attemptto account for the biome-chanics of the falls.Biomechanics is the scienceof how injury to human tis-sue occurs. Then, as today,no medical school curricularequired medical students tostudy the field of biome-chanics, that is, the science ofinjury causation. Despite thisvoid in training, pediatri-cians and forensic patholo-gists frequently testify as“experts” about the degree of
force necessary to causeinjury.
Most pediatricians and foren-sic pathologists are, in fact,unable to scientifically define
the degree of force needed to cause a spe-cific injury. According to the principle ofNewtonian physics, force is the productof mass (size and weight of the object)and acceleration (the change in speed ofthe object). Force is expressed as “F=ma.”
Irving Root, M.D., was a forensic pathol-ogist who critically questioned theassumptions of doctors like Helfer thatshort falls could not generate sufficientforce to cause serious head injures to chil-dren. He tried to introduce some com-mon sense to the debate by applyingF=ma to free-falls.
Root calculated the terminal (impact)velocities starting from heights rangingfrom two feet up to 30 feet, and wrote:
A MATTER OF GRAVITY
Pediatric vs. Adult Developmental Differences in the SkullTo understand the causes of pediatric head injury, we must understand
not only issues of force (F=Ma), but also the material properties of theskull and brain.

30 T H E W A R R I O R • W i n t e r 2 0 0 4
“To put this in common perspective,the average adult will walk at a sus-tained speed of 2.5–4 mph and willbe able to run a short sprint at topspeed of [about] 9–12 mph. (Worldclass sprinters achieve a 100 yd dashin 10 [seconds] and attain a speed of22 mph.)…. To put this further inperspective, assume yourself to be anaverage adult and imagine running,at your top speed, headlonginto a brick wall. It does nottake a great deal of imagina-tion to grasp the magnitudeof the impact.”
Root’s chart shows that in afree fall of only three feet, onewould hit the ground at 9.4mph. (Please see Root’s Chart, atright.)
ALL SHORT FALLSARE NOT EQUAL
The drop height of the falldoes not, alone, determine thepotential for injury. Some peo-ple do fall great distances andsurvive while others fall shortdistances and die. This iswhere it becomes critical toidentify and understand thebiomechanics of the fall.
Unfortunately, while biome-chanics has been used in solv-ing many medical problems, ithas been largely ignored indocumenting the forces andcauses of pediatric head trau-ma. Biomechanics is the sci-ence by which the pumpingstrength and motion of theheart is measured to betterdesign prosthetic heart valves. Itis the science of measuringstress and strain on cartilage tobetter design prosthetic carti-lage, tendon and bone. Heart-assistdevices, heart-lung and dialysis machines,and prosthetic limbs all owe their func-tion to the science of biomechanics.University of California bioengineer Y.C.Fung wrote, “biology can no more beunderstood without biomechanics thanan airplane can without aerodynamics.”10
Living systems have mechanical proper-ties. They have tolerance criteria and fail-
ure rates to stress and strain, torque andtorsion just like any other material on theface of the earth. Poet Thomas Lynch,who is also a funeral director in Michiganwho has seen his fair share of dead chil-dren, reminds us, “God lives by The Lawsof Nature and obeys its statutes, howeverbrutal. Kids die of gravity andphysics…”11
So let us learn to ask the questions thatare critical to the science of pediatric headinjury causation. Once again, Root lendsa hand in the Department of CommonSense.• Was the fall a free fall?• What was the actual distance of the
fall? (Note that this is only one of thequestions to ask.)
• Which specific part/parts of the
anatomy was/were impacted?• Where and how was the force deliv-
ered and distributed? Over what areaand time is the energy impacted?
• Was all the force taken up at once?• Did the body roll and dissipate the
force?• Did the child slide down with fric-
tion, for example, on the edge or sideof a bed or a chair? (This wouldslow the free fall and lessen theenergy of impact.)• Was the child sittingup or standing when the fallbegan, adding distance fromthe head to the floor?• Was there some initialimpelled added energy, i.e.,some rocking motion or anattempt to catch the balanceand, possibly, throw oneselffurther off?
The location of the impact tothe head is, depending on theage of the child and contactsurface, even more importantthan the impact velocity,whether by accident or intent.A child, whose sutures betweenskull plates have not fused, is atmuch greater risk for braininjury from a short fall or otherimpact. If the skull changesshape on impact, the braindeforms, tearing bridging veinsand other vessels and irrepara-bly ripping neurons and axonsapart. The risk of serious injuryis further increased for a baby ifthe trauma is at the back of thehead (i.e., the “occiput”) wherethe three plates of the skull con-verge in the A-shaped lamdoidalsuture. Think of it this way: theice on a lake is weakest at apoint where the cracks are con-
verging (Please see graphic on page 28,showing the “A-shaped” lamdoidal suture atthe back of the infant skull).
The contact surface also makes a differ-ence to the potential for head injury froma short fall. Concrete is a lot less forgivingthan a gym mat.
In the case of Billy Jo and Andy fallingdown the steps, Billy Jo had taken thetwo-year-old down with her when she
Consider what would happen to you if you ran head first into abrick wall. Short distance falls do kill, depending on the material
properties of the skull and brain, the contact surface and themechanics of the fall.
A MATTER OF GRAVITY
*Based on the basic formula, V2=2GS, where in free fallcapacities, V=velocity, G=32ft/s2, and S=distance
ROOT’S CHART

T H E W A R R I O R • W i n t e r 2 0 0 4 31
lost her balance, fell and, landing on topof him, increased the force (by increasingthe weight) with which the toddler’s headhit the ground. One of the pediatricianscalled by the State to testify that Andy’shead injury was not an accident, wasasked on cross examination:
Q: Doctor, you didn’t investigate indetail the biomechanics of the fall,did you?
A: I didn’t find it necessary.
What is not appreciated or understood bythe pediatrician “expert” is equated with“not necessary.”Understanding pediatrichead injury causation isconfounded by conflictingreports in the clinicalmedical literature. Theconflicting cases can onlybe reconciled by under-standing the necessity ofthe biomechanical analysisof falls. Few physicians do.Even fewer try.
Almost completely lackingis any evidence-basedmedicine applying biome-chanics to the area of pedi-atric head injury. This is soeven though now, unlikein the days of Helfer’sstudy, we possess the tech-nology to conduct suchstudies. That technology,called “finite elementanalysis,” involves the useof a computer into whichdata about the materialproperties of the infantskull and underlying braincan be loaded. The models can then bemanipulated with known degrees of forceto determine the potential for injury.Arguments are often made that finite ele-ment analysis has no biofidelity to thehuman body. In fact, it is accurate; somuch so that it is used by automobilemanufacturers to test the design of vehi-cles and their contents to manufacturesafer vehicles and, thus, avoid large prod-ucts-liability judgments.
THE LONG AND SHORT OF ITMAXIMUM VS. MINIMUM FALLSMost studies of pediatric head injury
caused by short distance and long dis-tance falls contain almost no analysis offall mechanics or of the material proper-ties of the pediatric skull and brain. Whatan object is made of determines how itresponds to stresses and strains caused byimpact. Without this scientific informa-tion, all of the fall studies are fallible.What can be said that is helpful is, thatbecause there are clinical examples in themedical literature where children fellshort distances and died from serioushead injuries or from untreated complica-tions of relatively minor head injuries, no
physician can reliably rule out a short fallas the cause.
Even so, the problem for the defense isoften that long falls or maximum impactsknown to cause fatal head injury areinvariably used to infer the level of force“inflicted” on a child. The level of force isthen used to prove the element of intentto injure and to rebut a defense ofaccident.
MAXIMUM HEIGHTSIn 1991, David Chadwick, M.D., a pedi-atrician practicing at Children’s Hospital,San Diego, Calif., studied falls of all chil-
dren brought to The Children’s TraumaCenter between August 1984 to March1988. It was a retrospective study, that is,one that looks back in time and selects itsparticipants. Retrospective studies,despite best human efforts, are subject toselection bias. Chadwick decided at theoutset that children whose caregiversclaimed they sustained serious headinjury from short falls, were not tellingthe truth. This is called “confirmationbias.” While some of the 317 children inChadwick’s study may have been victimsof abuse because they had multiple
injuries, some simplyhad head injuries. Ofthese, Chadwick wrotein The Journal ofTrauma:
“Inflicted injury isoften diagnosedwhen the cliniciancan state with a highlevel of certainty thatthe single injury seenin a child could notpossibly have beenproduced by theevent described bythe caretaker.”
* * * * * *
“For the most partthis discrimination isbased upon thephysician’s clinicalexperience of chil-dren’s injurability[sic] and the limitedempirical studies12 inthe literature.”
This pediatrician, with no training inbiomechanics of pediatric head injurycausation, then proclaimed that the care-givers of seven of the children in his studywho died from falls had “falsified” the“histor[ies].”
In making this judgment, Chadwickrelied on two studies. In one study, chil-dren who fell 30 feet and more sustainedfatal head injuries. In another study, thelowest fall was from 15 feet. This was thelowest fall that caused life-threateninginjury and death, Chadwick claimed. Heis not alone. It is from this type of study,in which it is claimed that only falls from
Modeling Head InjuryBiomechanicians who are experts in human injury causation usually attend thefirst two years of medical school to study subjects such as human anatomy and
physiology. They are able to combine this knowledge with geometry, mathematicsand physics to create models of the human head on computers.
A MATTER OF GRAVITY

32 T H E W A R R I O R • W i n t e r 2 0 0 4
great heights can cause catastrophic andfatal head injury, that many physiciansconclude that massive impact velocities—equivalent to a drop of two, three or fourstories head first onto concrete—arerequired to cause such injuries.
It doesn’t take a brain surgeon or a physi-cist to figure out that falls from greatheights cause serious head injury. Thesedocumented falls and the injuries sus-tained by the children provide us with areference point of known maximumheights. It is common sense that fallsfrom maximum heights cause seriousinjury. But it takes a biomechanician tofigure out what is the minimum impactvelocity required to cause serious headinjury to children.
To date, no one has answered the ques-tion of what is the minimum impactvelocity it takes to cause skull fractureand/or brain injury in a child who is onemonth old, two months old, threemonths old, and so on. The research hasnot been done. One biomechanicianreceived a grant in 1996 from the U.S.Department of Health and HumanServices to study the issueusing finite element analysis,but lost the funding beforethe project was completed.His idea was to determine thematerial properties of theinfant skull and the infantbrain and, applying differentimpact velocities, determinethe minimum impact veloci-ties that would cause injury.
Despite the fact that we stilldo not have vital informationabout the minimum forcesneeded to cause serious andfatal head injury in babiesand toddlers, “experts” forthe State are allowed to testi-fy about the injuries in casesof children who fall fromgreat heights, as though fallsfrom great heights arerequired to cause suchinjuries. This happened inPeople v Martinez, 51 P.3d1046 (2001). Martinez wascharged with murder of hisgirlfriend’s four-month-olddaughter, whom the physi-cians diagnosed as a victim of
shaken-baby-impact syndrome. The babyhad SDH’s, RH’s, SAH’s, a skull fractureand scalp bruises. After several interviews,including one in which Martinez wasencouraged to confess by detectives whohad been told by the doctors that theinjury happened that day, the defendantclaimed he had grown frustrated andshaken the baby, accidentally banging herhead on the crib. The degree of intent,i.e., whether Martinez acted “knowingly,”“recklessly” or was “criminally negligent,”was an issue the State tried to resolve byquantifying the level of force.
The State’s “expert” pediatrician on headinjury causation, testified:
In talking about how much forcethat it requires to cause this kind ofinjury, we can’t take babies and shakethem and do that for the obviousreason, so what we have had to do istake—there have been multiplestudies of series of witnessed falls orwitnessed accidents where babieshave had similar kinds of injuries.Okay? And in those studies, babieswho had similar kinds of injuries,
the subdural hematoma, have beenthings like a fall from a multiplestory building. Being in a high speedmotor vehicle accident either as apedestrian hit by a high speed motorvehicle or, for example, an unre-strained passenger in a high speedmotor vehicle accident, so those arethe kinds of witnessed injuries thatcan lead to a similar sort of injury.
Martinez was convicted of first degree,knowing murder of a child by a person ina position of trust. Reversing andremanding, the Colorado Court ofAppeals agreed with Martinez that it wasunfairly prejudicial for the State to inferthe minimum amount of force needed tocause the baby’s injuries from maximum-force accident scenarios. The court wrote:
It is one thing clearly to state that acertain quantum of force is necessary toproduce a subdural hematoma; it isquite another to use examples of obvi-ously extreme forces and violence thathave been demonstrated to havecaused subdural hematomas and thensuggest that they constitute the mini-
mum force necessary tocause such an injury inany particular case. Inour view, reasonable infer-ences as to the underlyingissue cannot be drawnfrom that testimony.(Emphasis added.)
The Colorado SupremeCourt ultimately reversedthe panel’s decision onother grounds, andremanded.13
MINIMUM HEIGHTSJapanese neurosurgeonNobuhiko Aoki presented astudy in 1984 in theJournal of Neurosurgery inwhich 26 children betweenfour to eleven months olddeveloped subduralhematomas and retinalhemorrhages from shortfalls onto various types ofcontact surfaces. (One childwas slapped.) Two of thechildren who fell short dis-tances died.
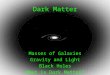
Impact Modeling of the Infant Head Using a method called "finite element analysis," biomechanicians can pre-
dict the deformation in mock pediatric brain tissue that is caused by amaximum "load" of 5000 Newtons, that is, about 1,100 pounds. This is
equivalent to the force generated in a drop of about 13 feet in a onemonth old infant. Looking at the series from top left to right, then bottomleft to right, early in the impact sequence, that is, at time "0.5 millisec-
onds" (ms, one one-thousandth of a second), one can see that there isalmost no local deformation of the brain tissue. From 1.0 ms to 5.0 ms,the wave of energy from the impact moves through the brain tissue caus-
ing deformation in a larger area with each passing millisecond. Thisresults in tissue "stretch" at sites distant from the site of impact. Graphic:"Pediatric Head Injuries: The Influence of Brain and Skull Mechanical
Properties," Thibault, K., PhD, 1997.(For assistance in elaborating on this graphic, thanks is due to Robert
Cargill II, PhD, managing engineer in injury biomechanics at ExponentFailure Analysis, Philadelphia.)
A MATTER OF GRAVITY

T H E W A R R I O R • W i n t e r 2 0 0 4 33
In 1989, J.R. Hall, M.D., reviewed filesof the Cook County [Illinois] MedicalExaminer’s office during 1983-86 forcases related to childhood falls. Eighteenof 44 children who died had only“minor” falls which happened eitherwhile they were running or from fallsfrom furniture (less than three feet).These 18 all died from head injuries,alone, without any other fall injuries.One child in this group was dead onarrival (DOA) at the ER. She was aneight-month-old girl who fell off a couchonto a hard wood floor. Her autopsyrevealed a large, acute subduralhematoma. Investigations of the 18 casesruled out abuse as the cause of theinjuries. Indeed, two of the minor fallsoccurred while the children were undermedical investigation. Hall wrote:“‘Minor falls’ can be lethal, especially in atoddler, and must be evaluated.”
In 1996, neurosurgeon Anne-ChristineDuhaime, M.D. wrote about the cases offour children who sustained unilateralSDHs after three of the children were wit-nessed to have fallen short heights in thehome, and one where the child had fallenfrom a window. What we are told in thearticle is that the SDHs resolved. But,there was no mention of follow up evalu-ation as to whether the children in thestudy suffered permanent brain damage.
In 2001, John Plunkett, M.D., reviewed18 short-distance, accidental falls by chil-dren. The falls were from two to ten feet.Twelve of these were witnessed by peoplewho were not the caretakers so, arguably,their accounts were independent.Thirteen of the children had subduralhematomas. Four of the six children forwhom ophthalmology exams were docu-mented in the medical record had bilater-al retinal hemorrhages. All of the childrendied. (Subdural hematomas and bilateralretinal hemorrhages are said by manyphysicians to be caused by shaking.)
In one tragic case related by Plunkett, agrandmother was videotaping her 23-month-old granddaughter clambering ona jungle gym. When the toddler got tothe top, she was standing 28 inches abovethe ground. Suddenly, she lost her bal-ance and plummeted onto the concretegarage floor, covered by a one-inch plushcarpet remnant. Hands outstretched, thetoddler struck the carpet, then hit the
front, right side of her head, finally land-ing on her shoulder. Afterwards, she gotup and walked and talked, but startedvomiting and went into a stupor fiveminutes later. This toddler had scalpdamage, SDH’s and bilateral retinal hem-orrhages. She died a few days later of thesecondary effects of the primary impact.It is chilling to realize that this tragedymight have been compounded. Withoutthe videotape, grandma would probablynow be behind bars.
That short falls do kill is beyond dispute.The literature proves it. Such cases exist,even though we don’t fully understandwhy. However, to look at clinical caseseries studies to answer the question ofwhat forces are involved in causing injurywithout a scientific frame of reference, islike staring at a few pieces of the jigsawpuzzle and never having enough to com-plete the entire picture.
One way to complete the picture is forfederal and state governments and privatefoundations to fund evidence-based-medicine research in the science of pedi-atric head injury causation. The toleranceand failure rates of human tissue can bemeasured, especially as the practice ofanatomical giving is growing. Data fromtests on this tissue, as well as data alreadycollected, can be programmed into acomputer and, using geometry, physicsand mathematics, tested at variousanatomical sites with a range of impactvelocities. But, so long as millions of dol-lars each year are pumped only into pro-grams to recognize and prevent the dubi-ous shaken baby syndrome, the criticalquestions will go unanswered and falseaccusations will abound. Not even grand-ma is safe unless, of course, she has avideotape.
TIMING OF INJURIESTELL-TALE SIGNS AND
SYMPTOMS OF OLDER INJURIESState “experts” frequently testify aboutthe timing of the injury in order to assistthe government in pinning the “crime”on the accused. But brain injury and itssequelae are complex. All is not what itseems.
A parent or caregiver inexperienced andunknowledgeable about the sequelae of aTBI may think a child is fine after a fall .
Some of the sequelae of TBI include lossof consciousness, history of behaviorchange, seizures, vomiting (especiallyprojectile), depressed mental status, irri-tability, bulging fontanel, focal neurolog-ic findings, such as, pupils dilated andeyes not following, or loss of vital signs.
Symptoms of a TBI may be caused by anexpanding SDH pressing on the brain. ASDH may expand slowly, depending onhow many of the bridging veins are tornin the fall, or may stop bleeding and startto resolve, until some event, such as anew and even inconsequential traumacauses it to bleed again. The issue ofrebleeds is controversial, but it is onlythrough the rebleeding of a chronic SDHthat a person exhibits symptoms of aSDH. Rebleeds have been described inthe neurosurgical literature for more thana century. They can occur from new trau-ma or, seemingly, spontaneously. Theyoccur when children, who have acuteSDH’s, continue to rebleed while they arein the hospital under the care of dedicat-ed doctors and nurses. While we don’tknow all the answers to the questionsabout why rebleeds happen, we knowthey do.
These symptoms of the cascading, sec-ondary effects of initial head trauma,such as edema or subdural re-bleeding,are well recognized symptoms of a TBI inthe ER, so much so that ER doctors giveparents a head injury check sheet. Thesesheets, developed in part by various braininjury associations, warn that if thesesymptoms develop after the child hasbeen sent home, parents should immedi-ately bring the child back to the ER.
Despite this standard of care in clinicalpractice, once in the witness box as an“expert” for the State, many physicianstestify that there are no delayed symp-toms or lucid intervals after TBI, or atleast, “not in this case.” Why? Because theprosecution needs to squeeze clinical real-ity out of the picture in order to create alegal fiction. It needs to fix the time of theinjury and, in so doing, identify the peri-od of exclusive access providing theopportunity of the accused to inflict theinjury. Therefore, the State’s expertsargue, the onset of symptoms after theabuse was “immediate” or “followedclosely.”
A MATTER OF GRAVITY

34 T H E W A R R I O R • W i n t e r 2 0 0 4
It’s important, therefore, to fully docu-ment, through interviewing all those whohad contact with the child following anaccidental fall, what the child’s behaviorwas after the fall.
But, sometimes, children are asympto-matic after a head injury, as shown in astudy published in 1999 in Pediatrics byBoston-based doctors David S. Greenes,M.D., and Sara A. Schutzman, M.D. Inthat study, of 608 children brought toone local ER for head injury, 30 childrenwere found to have intracranial injuries.Of those, 16 were active and alert, show-ing no symptoms of what was happeninginside their heads. Only CT scans and/orX-rays diagnosed the injuries.
In 1999, a proponent of shaking as amechanism of injury published an articlein the Journal of Forensic Sciences in whichshe reported that some of the 76 infantsshe studied—whom she believed werevictims of shaking, blunt trauma, orboth—had a lucid and symptom-freeinterval after being lethally shaken or oth-erwise head injured.
Mary G. F. Gilliland, M.D. examinedfive so-called pure shaking cases, i.e., inwhich no impact was proved, and foundthat four of them resulted in severe symp-toms in less than 24 hours, but one child(20%) did not have severe symptoms for24-48 hours. Gilliland also reported thatin 39 blunt trauma cases resulting indeath, six did not develop severe symp-toms for 24-48 hours, three for 48-72hours, and three did not develop severesymptoms for more than 72 hours. Evenin fatal cases labeled as “combined” shak-ing and blunt trauma, eight of 32 chil-dren did not develop severe symptoms for24-48 hours, and one did not developsevere symptoms for more than 72 hours.The article concludes:
Enough variability in the intervalbetween injury and the time ofsevere symptoms or presentation formedical care in fatally injured chil-dren exists to warrant circumspec-tion in describing such an intervalfor investigators or triers of fact. Ourdata indicate that the interval is brief(less than 24 hours) in almost 3/4 ofcases of head injury, especially inshaking injuries. However, in morethan 1/4 of the cases, the interval
from injury to the onset of severesymptoms is longer.
Gilliland’s work confirms that braininjury is complex and that we are still inan unfathomable, black hole when itcomes to understanding its intricacies.
Ayub K. Ommaya, M.D. wrote about asyndrome he called, “Talk, Detoriate andDie” (TADD). Ommaya studied adultvictims of TBI and noted that some ofthem were talking and walking right afterthe event, but later deteriorated and died.
Experts for the State sometimes claimthat the TADD syndrome does not occurin children. At least one study falsifiesthat claim. R.P. Humphreys, M.D.,described four cases in which childrenwho had been in car accidents or whohad fallen each had a lucid interval.Deterioration ranged from 30 to 50hours.
While the reason for and extent of thedelay may lie in the nature of the primaryinjury, in genetic and age-related factors,delayed symptoms are not unusualbecause the secondary effects of an initialblow to the head are not unusual.
A blow to the head may cause a SDH thatdoes not clot. It may cause damage toneurons and axons that, in turn, leakfluid from their damaged cell walls caus-ing edema. There are many secondarysequelae of a bump on the head andoften, if unchecked and untreated, theyare lethal.
Edema is believed to be a particularlydangerous foe of head injured children.In 1984, Netherlands physician J.W.Snoek, M.D., described the cases of 42children who, following seemingly trivialtrauma, developed neurological signsafter a lucid or symptom-free period. Hebelieved that because the brain of a child(defined as 0 - 18 years) is different froman adult’s brain, it is exquisitely suscepti-ble to slowly developing and, sometimes,lethal edema. He termed it “malignantcerebral edema,” an awful process withwhich neurosurgeons are all too familiarand of which they are all fearful.
“WHAT” VERSUS“WHO” DUNNIT
When the State points the accusing fingerof child abuse, jurors are not merely
interested in hearing what did not hap-pen. They want to hear what did happen.How did the baby or toddler die? Thedefense needs to appreciate that there is afunctional presumption of guilt at work,and needs to prepare to carry the burdenof proof as to how the child died. This isno time to be silent. For the accused,investigating alternative theories of causa-tion can mean the difference between lifeand death. This is precisely what it meantin the case of Tamara Sawyer (the lastname is her real name).
Tamara’s story begins one muggy morn-ing in northern Florida. Baby Thomas’parents have arrived at Tamara’s house todrop him off, as usual, at 6 a.m. Theyentrust their six-month-old son toTamara, a sister in the evangelical congre-gation to which they all belong. “SisterTamara” cares for Thomas for just a fewdollars a week. She believes this is a wayof loving her neighbors by helping themto work and to survive. They are newimmigrants from Nigeria.
On this morning, there is nothingunusual about the routine: Tamara takesthe sleepy baby from his mother’s armsand lays down with him and her owntoddler to nap on a futon mattress on thefloor.
Her peaceful slumber is broken by thesound of baby Thomas gasping forbreath. She reaches for him, picks him upand peers at his face. His eyes, like adoll’s, are rolling back in his head. White.No pupils. Arms and legs stiffeningstraight out. Palms up. He turns blue. Hedoes not seem to hear Tamara’s voice.
Tamara tries to revive him and, gentlyshaking him, she whispers “Wake upThomas, Thomas, Thomas…wakeup…” He is gasping for breath and isturning bluer. Tamara, now frantic, calls911.
The ER doctor at the local children’s hos-pital diagnoses Thomas with subduralhematomas, i.e., bleeding beneath thedural covering of the brain, retinal hem-orrhages, i.e., bleeding in and betweenthe retinal layers behind the eyes. Helearned in medical school that when achild has subdural hematomas and retinalhemorrhages, this means that the childwas violently shaken or slammed.Recently, the American Academy of
A MATTER OF GRAVITY

T H E W A R R I O R • W i n t e r 2 0 0 4 35
Pediatrics issued a position statementthat, if the caretaker does not have a plau-sible explanation for these injuries, itmeans the child is a victim of “shakenbaby syndrome.” This doctor, like somany others, is unaware that the scientif-ic foundation for the syndrome has beeninvalidated by two experiments using amodel baby. He does not know that thisinvalidation has been corroborated bystudies from other disciplines such asneuropathology and forensic pathology.He may not know about the clinical caseswhere children fell short distances anddied. He may not know that no oneknows the minimum impact velocity ittakes to injure an infant of Thomas’ ageand sex. And, he may not know…. well,you can now fill in the blank.
The ER doctor diagnoses the time of theinjury. He says it was “inflicted” just min-utes before Tamara called 911, whenThomas was in her sole, physical custody.In his role as a mandated reporter of sus-pected child abuse – and as one who maybe criminally prosecuted for failing toreport—the ER doctor notifies the policeand the local department of social sevices.The police arrive to question Tamara, butthe ER doctor has already informed themthat she is a child killer.
Tamara soon faces prosecution and thedeath penalty. There is evidence of bluntimpact, and the other injuries, such asretinal hemorrhages, had to be caused byviolent shaking, the State claims.
But, at autopsy, the top of Thomas’ skullwas as thin as a plastic milk jug. Thiscould be seen in the photographs thatshowed a translucent calvarium sitting onthe autopsy table after it had beenremoved so the medical examiner couldremove the brain. The lights of the autop-sy room shone right through it. In hisrush to judgment, this curious detailseems to have escaped the medical exam-iner’s eyes.
One had to ask: Why was Thomas’ skullwas so thin? It took a Chicago-basedforensic neuropathologist, Jan E.Leestma, M.D. to answer the question.Thomas suffered from birth injury to cis-terns—known as the “ventricles”—deepwithin his brain. Thomas had been fiveweeks premature. It is well known byobstetricians and biomechanicians that
premature children are at much greaterrisk for birth injury than are full termbabies. The ventricles are involved in themanufacture, circulation and reabsorp-tion of cerebral spinal fluid (CSF), awater-like fluid that bathes the brain innutrients.
The forensic neuropathologist found thatsmall filters in the ventricles were cloggedwith calcium, which is part of the scar tis-sue after injury. The result was thatThomas’ brain had become hydrocephal-ic, meaning that it had become enlargedbecause it contained too much of thewatery CSF. The response of bone tostrain and pressure is to remodel. This issimilar to Wolff ’s law, i.e., that the bodylays down bone tissue where it is neededand does not put it down where it is not.In Thomas’ case, a juvenile osteologistopined that his body removed the mem-branous bone from his skull and did notlay down any new bone tissue. It was not“needed” and it was in the way of hisexpanding brain. His skull became thin-ner and thinner to allow his brain moreand more room to expand. Thomas’ skullwas so thin that, by the time he stoppedbreathing in Tamara’s arms he was, literal-ly, playing life without a helmet, his thinskull obscured by a mop of springy hair.In 1999, Oregon neurosurgeon JosephH. Piatt, Jr., wrote that in cases of hydro-cephalus, babies “are exceptionally sus-ceptible to subdural hemorrhage afterwhat would be otherwise inconsequentialtrauma.” Hydrocephalus and SDH’scause intracranial pressure (ICP) to rise.Increased ICP is one cause of retinalhemorrhaging.
Even though there was a forensicallysolid, alternative theory of causation, therisks of trying the case were too great notto take the plea offered by the State afterit learned, in part through a Frye motion,of the defense. Tamara was an AfricanAmerican. She was overweight. She waspoor. She was female. There was a deadbaby and the State was pointing its fingerat her. The plea was three years, withcredit for time served. (This, in contrastto the risk of death.) She took it. Tamarahad given birth to her fourth child in pre-trial custody. She had four children wait-ing for her on the outside. Tamara isalive, and today she is free thanks, in part,to a forensic neuropathologist who
detected the microscopic evidence ofolder injury in Thomas’ brain. Thedefense gave Tamara currency with whichto negotiate in what had previously beena game in which she had no power.
The case of Tamara Sawyer and the casewhere Andy and Billy Jo tumbled downthe steps have much in common. In eachcase, forensic neuropathology was criti-cal. In Tamara’s case, the issue was injuryto the cisterns. In other cases, one mayfind healing cells at the site of a subduralhematoma or in retinal hemorrhages.These are forensic gifts because theyrefute the State’s oft-chanted mantra thatthe injury was inflicted minutes or hoursbefore the child was brought to the ER.Billy Jo’s testimony about the fall and thedefense position that this fall—four daysearlier—caused Andy’s fatal head injuries,including SDH’s, was corroborated bythe forensic neuropathology: At the siteof the SDH’s, there were healing cells thatwere four to five days old.
PRINCE LLEWELYN’S LAMENTThings are not always as they seem. Inthe rush to judgment, false accusations flyfast and furious. Such accusations basedon faulty assumptions can, as in theWelsh folklore tale of Prince Llewelyn(Loo-ell-in) and his dog Gelert, causeheartbreak, incarceration and even death.As the story goes, Prince Llewelynreturned after a hunt to his castle inBeddgelert, Caenarvonshire, to find hisdog Gelert’s jaws dripping with blood.His son had been left in Gelert’s care butthe baby was not to be found. In his dis-tress, Llewelyn slew the faithful hound. Itwas only later that Llewelyn found hisson, close to the body of a wolf, whichthe hound had killed.14
And, so it goes when a child is injuredand dies: We look to place blame.Someone must pay. But blame withoutreliable science to support it is unjust.Accusing a parent or babysitter of killinga child by slamming the child’s head withmassive force and of doing it within aspecific time frame, may be to slay thefaithful hound.
POST SCRIPTNo vocabulary of thanks and praiseincludes words sufficient for what I, andthe accused, owe to death penalty special-
A MATTER OF GRAVITY

36 T H E W A R R I O R • W i n t e r 2 0 0 4
ist Ed Stafman of Tallahassee, Florida,and criminal defense lawyer WarnerEisenbise of Wichita, Kansas to whom Iwas co-counsel in the specific casesincluded in this article. Thanks is due toneuropathologist Jan Leestma, M.D., forhelpful discussions and to neurosurgeonRonald H. Uscinski, M.D., who invitedme into the OR to see both chronic andacute SDH’s to help me understand howrebleeds occur.
NEXT ISSUEShaking a baby cannot cause many of theinjuries that the State’s experts claim. Shortfalls can be fatal, and the signs and symp-toms of TBI after a short fall can mimicthose of so-called SBS. The mechanism ofinjury proffered by the State is frequentlyunreliable.
There are documented cases of lucid inter-vals or delayed symptoms after TBI. Thetiming of the injury proffered by the State isfrequently unreliable.
Sometimes, an expert has improperlyapplied good science to a case.
Faced with the State’s “expert” testimonyand depending on strategic considerations,the defense may want to consider filing amotion in limine to exclude unreliable sci-ence. Three cases give some guidance: (1)Daubert v Merrill Dow, 509 US 579
(1993), (2) General Elec. v Joiner, 522U.S. 136 (1997) and (3) Kumho Tire Co.v Carmichael, 119 S. Ct 1167 (1999).(All of these cases are now embodied in FRE702.) Some states have adopted Daubertand its progeny. Others are still using Frye vUnited States, 54 App. D.C. 46 (1923), ora combination of Frye and Daubert.
Part III will include examples of how tochallenge mechanism of injury, timing ofinjury, misapplication of science to a case,and expert qualifications.
ENDNOTES
1 This is part of a book by ElaineWhitfield Sharp. Copyright byElaine Whitfield Sharp, October2003. Permission to publish givento The Warrior.
2 Part I may be obtained by orderinga back issue of The Warrior, or maybe accessed in PDF by logging onto www.sharplaw.biz.
3 Subdural Hematoma (SDH):Bleeding beneath the dural cov-ering of the brain. In this article,SDH refers to bleeding beneath thedura over the convexities of thebrain. It does not refer to bleedingbeneath the dura around the brainstem or upper cervical cord. Suchinjury may indicate that a child wasinjured by shaking.
4 Subarachnoid hemorrhage (SAH):Bleeding beneath the arachnoidmeningeal layer covering the brain.In this article, the use of the termSAH refers to bleeding over theconvexities of the brain, only, andnot to bleeding beneath the arach-noid layer around the brain stemand upper cervical cord. (Please seeprevious endnote.)
5 Retinal hemorrhage (RH):Bleeding behind and between oneor more of the retinal layers aroundthe eye.
6 Brain edema: Swelling of the braindue to leakage of water from deador injured brain cells.
7 Diffuse axonal injury(DAI): Injuryto the axons and neurons of thebrain on a global or diffuse scale, asopposed to localized injury. In thisarticle, the use of the term DAIrefers to microscopic brain cellinjury in all parts of the brain,except the brain stem, the cranio-cervical junction (where the brainstem joins the upper cervical cord)and the upper cervical cord. DAI inthese latter areas may indicate thatsomeone shook the baby.
8 The topic of the potential injury tothe infant brain on blunt impactwas discussed in Part I, “TheElephant on the Moon.” (Please seeendnote 2.)
9 People v Martinez, 51 P3d 1046(2001) (R’hrg den. 2002) (cert.granted, 2002); People v Martinez,74 P.3d 316 (2003) (R’hrg den.2003).
10 Fung, Y.C., Biomechanics:Mechanical Properties of LivingTissues, Ch. 1, p 1 (Springer, 2d ed,1993).
11 Lynch, T, The Undertaking: LifeStudies from the Dismal Trade, pp45-46 (Penguin, 1997).
12 There are no “empirical studies inthe literature” that are scientificallyreliable.
13 Martinez, supra.
14 Dictionary of Phrase and Fable(Wordsworth 1996).
The Lament of Prince Llewelyn (Loo-ell-lyn)Things are not always what they seem. Prince Llewelyn slayed hishound Gelert when he rushed to the judgment that the dog hadkilled his son, the baby prince. Later, Llewelyn discovered the
truth, but it was too late.
A MATTER OF GRAVITY