Embed Size (px)
Citation preview

7/11/2012
1
IHI Expedition: Preventing Obstetrical Adverse Events
Deb Bell-Polson, MSN, RNC-OB
Peter Cherouny, MD
Sue Gullo, RN, BSN, MS
These presenters have nothing to disclose
Expedition Coordinator
2
Kayla DeVincentis, Project Coordinator, has
worked at IHI since 2009, starting as an intern in
the Event Planning department. Since then, Kayla
has contributed to the STAAR Initiative, the IHI
Summer Immersion Program, and the IHI
Expeditions. Kayla obtained her Bachelor’s in
Health Science from Northeastern University and
brings her interest in health and wellness to IHI’s
Health and Fitness team.

7/11/2012
2
3
WebEx Quick Reference
3
WebEx Quick Reference
• Welcome to today’s session!
• Please use Chat to “All
Participants” for questions
• For technology issues only,
please Chat to “Host”
• WebEx Technical Support:
866-569-3239
• Dial-in Info: Communicate /
Join Teleconference (in menu)
Raise your hand
Select Chat recipient
Enter Text
4
When Chatting…
Please send your message to
All Participants

7/11/2012
3
Our Expedition Director
5
Sue Leavitt Gullo, RN, BSN, MS, Managing Director,
Institute for Healthcare Improvement (IHI), brings 30
years of health care experience to her current roles,
which include work in IHI's national and international
patient safety work, and IHI's faculty for leadership and
patient safety. She is the Director of the Perinatal
Improvement Community and The Safer Patient Project
in Denmark. Prior to joining IHI, Ms. Gullo was the
Director of Women's Services at Elliot Hospital in New
Hampshire. Her prior nursing roles included experience
in the frontline clinical areas of maternal-child health,
oncology, and medical-surgical nursing. Ms. Gullo has
also been active as national faculty in obstetrical care
for the last 15 years. Her involvement with IHI dates
back to 1995 as a participant in the IHI Breakthrough
Series on Improving Maternal and Neonatal Outcomes
and continued as IHI faculty until she joined the IHI staff
in 2005.
Ground Rules
6
• We learn from one another – “All teach,
all learn”
• Why reinvent the wheel? - Steal
shamelessly
• This is a transparent learning
environment
• All ideas/feedback are welcome and
encouraged!

7/11/2012
4
Schedule of Calls
Session 1 – Introduction to Obstetrical Adverse Events
Wednesday, May 30, 1:00 PM – 2:30 PM ET
Session 2 – Structure and Process for System Redesign
Date: Wednesday, June 13, 1:30 PM – 2:30 PM ET
Session 3 – Executing Oxytocin Bundles
Date: Wednesday, June 27, 1:30 PM – 2:30 PM ET
Session 4 – Designing Reliable Processes
Date: Wednesday, July 11, 1:30 PM – 2:30 PM
Session 5 – Using the Perinatal Trigger Tool to Identify System Harm
Date: Wednesday, July 25, 1:30 PM – 2:30 PM
Session 6 – Results Report-out and Advanced Bundles
Date: Wednesday, August 8, 1:30 PM – 2:30 PM7
Faculty
8
Deb Bell-Polson, MSN, RNC-OB, is a Masters
prepared Perinatal Nurse with 22 years of experience.
Most recently has worked as a Clinical Nurse Manager
leading a multidisciplinary team that has had great
success in the IHI Perinatal Community. We had proven
results in changing culture for quality and safety and
achieving 95% compliance on the Elective Induction and
Augmentation bundles as well as the Vacuum Bundle.
Also serves on a regional Quality and Safety Network
guidelines team that is working to set regional standards
for care in the Northern New England region. Is most
recently a part of a state wide Committee to review
cases of Sudden unexplained infant Deaths and work to
prevent them in the future. When not working I keep
busy with my family of three sons and a wonderful
husband.

7/11/2012
5
Faculty
9
Peter Cherouny, MD, Professor of Obstetrics and
Gynecology, University of Vermont College of Medicine,
has strong clinical interests in obstetric health care
quality improvement and is currently serving as Chair of
the Institute for Healthcare Improvement's Perinatal
Improvement Community. He was also the lead author
of the IHI white paper, "Idealized Design of Perinatal
Care." He has been Chair of Quality Assurance and
Improvement and Credentialing for the Women's Health
Care Service of Fletcher Allen Heathcare for the last 15
years. His recent research and work in obstetric quality
improvement is as Chair of the March of Dimes
collaborative, "Improving Prenatal Care in Vermont,"
and as co-investigator of the MedTeams project.
Session Four
Designing Reliable Processes
10

7/11/2012
6
Mindful Practice
• It is not enough to do your bestyou must know what to do
and then do your best
�W. Edwards Deming
Designing Reliable Processes
• Do you have reliable processes?
• Do those processes achieve what you
want?
12

7/11/2012
7
If your process does not achieve what you expect, is it?
A Failure of……..
1. Will?
2. Ideas?
3. Execution?
13
http://www.ihi.org/knowledge/Pages/Tools/ExecutiveReviewofProjectsIHI.aspx
Failure of Will
• Resources necessary to the project’s success are not made available
• A few loud nay Sayers are blocking implementation and spread of good ideas
• Absence of any obvious connection between this project and key strategic goals
• Lack of executive and board attention to this project
• Line managers appear to be on the sidelines, not responsible for project success
14

7/11/2012
8
Failure of Ideas
• The project team has not gone outside the organization, or outside health care, to find the best ideas
• Few cycles of improvement have been attempted
• “Big Ideas” appear to be absent—changes being tested are safe, incremental, not radical redesigns
• The team can’t tell you who has the best results in the world on this topic
15
Failure of Execution
• Project setup, and project management
appear to be weak
• Preparation for spread is not part of the
project from the inception
• The project team can not articulate a
coherent change leadership framework
being used by the project
• The project gets good results on pilots, but
never seems to scale up16

7/11/2012
9
“What, exactly, are you trying
to accomplish in this project?”
17
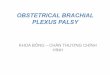
What are we trying toAccomplish?
How will we know that achange is an improvement?
What change can we make that will result in improvement?
The Model for Improvement
Act Plan
Study DoSource:
Langley, et al. The Improvement Guide, 1996.
The three questions provide the strategy
The PDSA cycle provides the tactical approach to work

7/11/2012
10
The Sequence for Improvement
Spreading a change to other
locations
Developing a change
Implementing a change
Testing a change
Act Plan
Study Do
Theory and
Prediction
Test under
a variety of
conditions
Make part
of routine
operations
20

7/11/2012
11
21
1.Prevent failure (a breakdown in operations or functions).
2. Identify and Mitigate failure: Identify failure when it occurs and intercede before harm is caused, or mitigate the harm caused by failures that are not detected and intercepted.
3. Redesign the process based on the critical failures identified.
IHI uses a three-tiered strategy for designing reliable care
systems, with processes and procedures in place intended to:
Improvement Concepts Associated with Performance Resulting in 80-90% Process Reliability
(Primarily can be described as intent, vigilance, and hard work)
• Common equipment, standard order sheets, multiple choice protocols, and written policies/procedures
• Personal check lists
• Feedback of information on compliance
• Suggestions of working harder next time
• Awareness and training

7/11/2012
12
Prevent-Identify/Mitigate-Redesign 23
Any process stability?
Improvement Concepts Resulting in 95% Process Reliability
(Uses human factors and reliability science to design failure prevention, failure
identification, and mitigation)
• Decision aids and reminders built into the system
• Desired action the default (based on scientific evidence)
• Redundant processes utilized
• Scheduling used in design development
• Habits and patterns know and taken advantage of in the design
• Standardization of process

7/11/2012
13
Process/Structure/Outcome
1919-2000
Avedis Donabedian, M.D., M.P.H.
Structure and Process
• Create the sense of urgency─Deep Dive for data
• Define what to measure─Structure and process measures

7/11/2012
14
Vacuum Bundle
� Alternative labor strategies considered
� Prepared patient
�Informed consent discussed and documented
� High probability of success
�EFW, fetal position and station known
� Maximum application time and number of pop-offs predetermined
� Exit strategy available
�Cesarean and resuscitation team available

7/11/2012
15
Questions?
29
Raise your hand
Use the Chat
What are we trying toaccomplish?
How will we know that achange is an improvement?
What change can we make that
will result in improvement?
Model for Improvement
Act Plan
Study Do
Aim of Improvement
Measurement of
Improvement
Developing a Change
Testing a Change
Adapted from Langley, G. J., Nolan, K. M., Nolan, T. W., Norman, C. L., & Provost, L. P. The Improvement Guide: A Practical Approach to Enhancing Organizational Performance. San Francisco, CA: Jossey-Bass, 1996.
30

7/11/2012
16
Plan• Compose aim
•Pose questions/predictions
•Create action plan to carry
out cycle (who, what, when,
where)
•Plan for data collection
DoStudy
Act
• Carry out the test and
collect data
•Document what occurred
•Begin analysis of data
• Complete data analysis
•Compare to predictions
•Summarize learning
• Decide changes to make
•Arrange next cycle
31
Principles & Guidelines for Testing
• A test of change should answer a specific question
• A test of change requires a theory and prediction
• Test on a small scale
• Collect data over time
• Build knowledge sequentially with multiple PDSA cycles for each change idea
• Include a wide range of conditions in the sequence of tests
32

7/11/2012
17
Repeated Use of the PDSA Cycle
Hunches
Theories
Ideas
Changes That
Result in
Improvement
A P
S D
A P
S D
Very Small
Scale Test
Follow-up
Tests
Wide-Scale Tests
of Change
Implementation of
Change
Sequential building of knowledge under a wide range of conditions Spread
33
Aim: Implement Rapid Response Team on non-ICU unit
Improved Communication
A P
S D
A P
S D
Cycle 1: ICU nurse responds to rapid response team calls on one unit,
one shift for one day
Cycle 2: Repeat cycle 1 for three days
Cycle 3: Have Respiratory Therapist attend
rapid response calls with ICU Nurse
Cycle 4: Expand coverage of RRT on unit
to one unit for one shift for five days
Cycle 5: Have Nurse Practitioner
respond to calls in addition to RT and
RN
Cycle 6: Expand rounds to
one unit for one shift seven
days a week
34

7/11/2012
18
Questions?
Raise your hand
Use the Chat
35
Storyboard Project
• Homework assignments for each call will
build on each other to create a
“storyboard” to present your progress
36

7/11/2012
19
Storyboard Explanation
• Intent: use this as an active tool over the year to
describe your work plan and improvements- successes
and barriers- and share your learning. Although you may
not have all of the measures currently in place, we have
included all of them in this template.
• “Building” storyboard” as you create the infrastructure
to achieve your aim, you will continuously expand this
template to share your journey.
• See notes on each slide for description of content.
37
Homework for Next Session
• Update your storyboard
─Complete as much as possible
38

7/11/2012
20
Expedition Communications
• If you would like additional people to
receive session notifications please send
their email addresses to
• We have set up a listserv for the
Expedition to enable you to share your
progress. To use the listserv, address an
email to [email protected].
39
Next Session
Session 5 – Using the Perinatal Trigger Tool to Identify System Harm
Date: Wednesday, July 25, 1:30 PM – 2:30 PM
40