Embed Size (px)
Citation preview
IGRAs: Should they replace the TST in the identification of latent tuberculosis?
Allen Kraut, MD, FRCPCMedical Director, Occupational Health WRHA WRHA TB Forum April 12, 2012
Objectives
• Describe how interferon-gamma release assays (IGRAs) work.• List three advantages and disadvantages
of IGRA in comparison to tuberculin skin testing (TST).• Identify populations where IGRA testing
may be of benefit in the management of latent tuberculosis infection.
Conflict of Interest
•Received Quantiferon TB Gold in Tube Tubes from Cellestis as part of a research study.
TST has been used for 100 years
Standard way to diagnose Latent TB.
Many issues with interpretation
Some issues with TST
• Difficulty reading test.• 6mm inter reader variability• Not specific for Mycobacterium Tuberculosis• False +ve with BCG or Atypical Mycobacterium
• Requires two visits days apart for reading• Subject to boosting• Definition of positive test depends on
circumstances
New Technologies – Blood tests• Interferon Gamma Release Assays (IGRAs)•White blood cells in people infected with
TB release Gamma interferon• Detect specific Mycobacterium TB
proteins• Less likely to give false positive results
• Can not differentiate latent and active disease
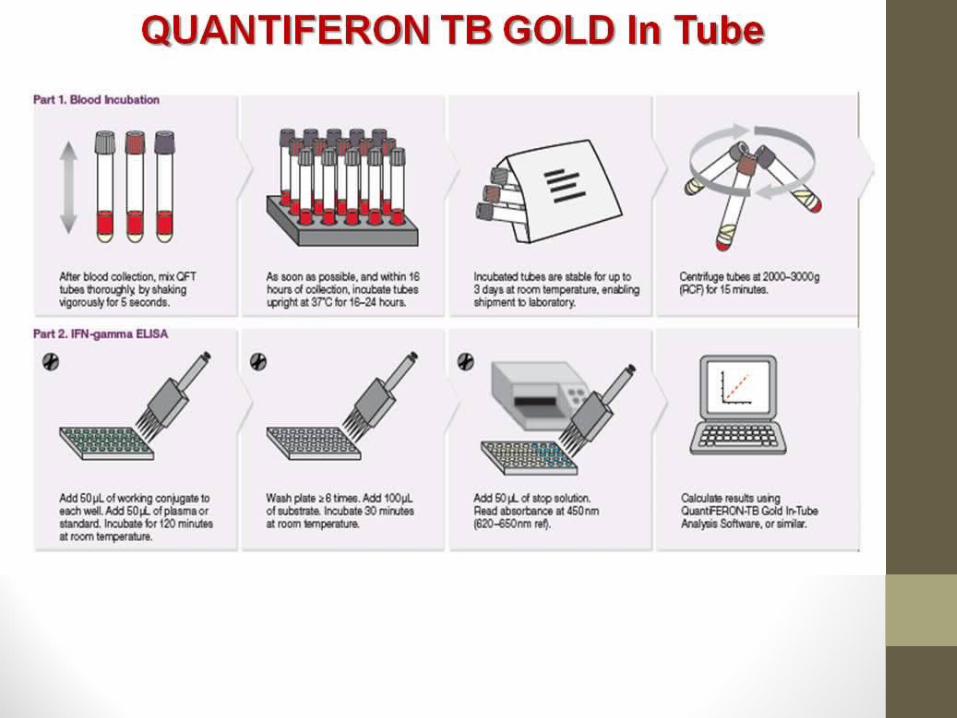
Interferon Gamma Release Assays (IGRAs)• Quantiferon-TB Gold In-Tube Assay• ESAT-6, CFP – 10, TB7.7•Measure IFN- Gamma ELISA• T-spot.TB Assay• ESAT-6, CFP – 10• Count spots which are related to the
number of cells releasing Gamma Interferon.

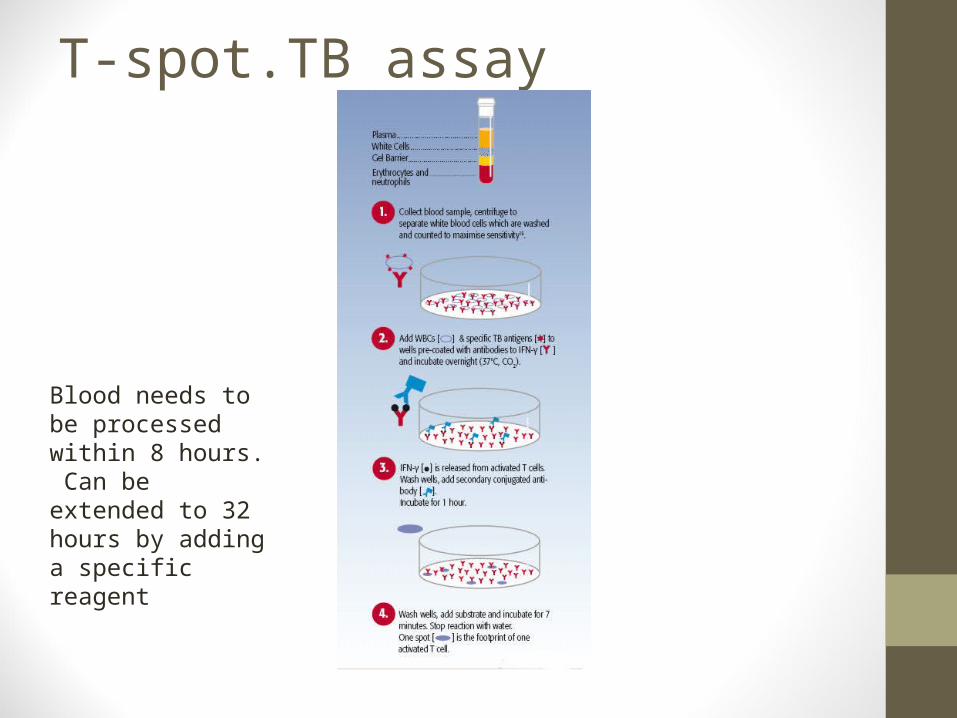
T-spot.TB assay
Blood needs to be processed within 8 hours. Can be extended to 32 hours by adding a specific reagent
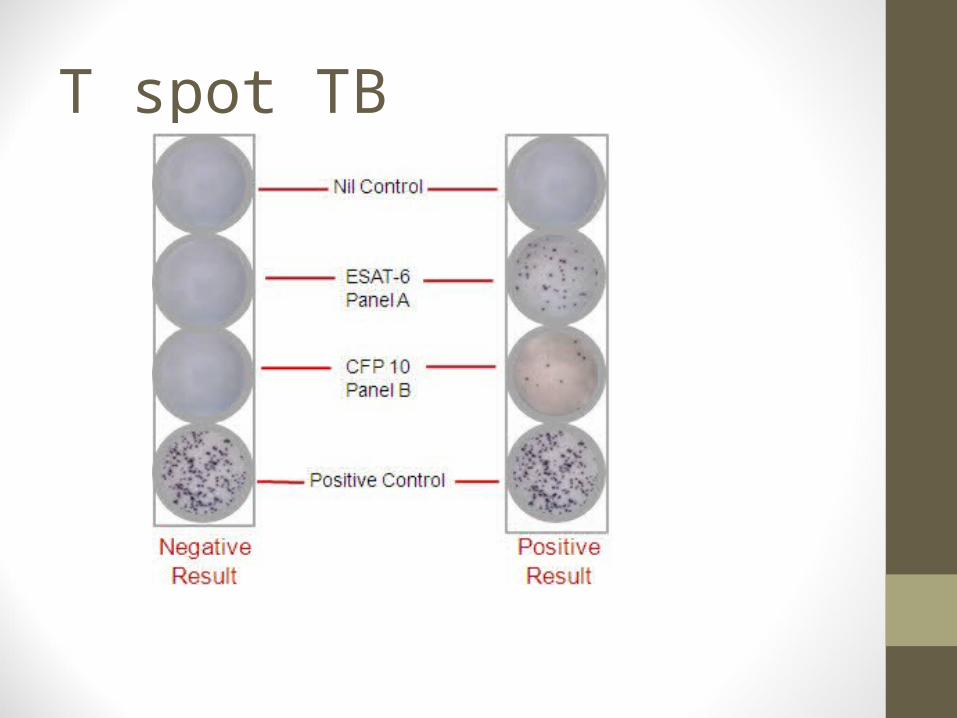
T spot TB
IGRAs• Advantages • More specific for Mycobacterium TB.
• Atypical mycobacteria • M. kansasii, M. szulgai, and M.marinum.
• Single patient encounter• Objective criteria for positive response
• Disadvantages • Requires blood draw• Requires sophisticated equipment• Elements of processing time sensitive• Results may not be readily available• ? Immunosuppressed - T spot.TB may be better• Higher direct costs, but may have lower costs if include all
required follow up and treatment
IGRAs in HCP
• Significant discordance is found between TST and IGRA positivity rates in healthcare workers (HCWs), • TST+/IGRA- - BCG vaccinations.• IGRAs seem to correlate with markers of
exposure in HCWs• Serial testing results limited
• CCDR Vol36 June 2010
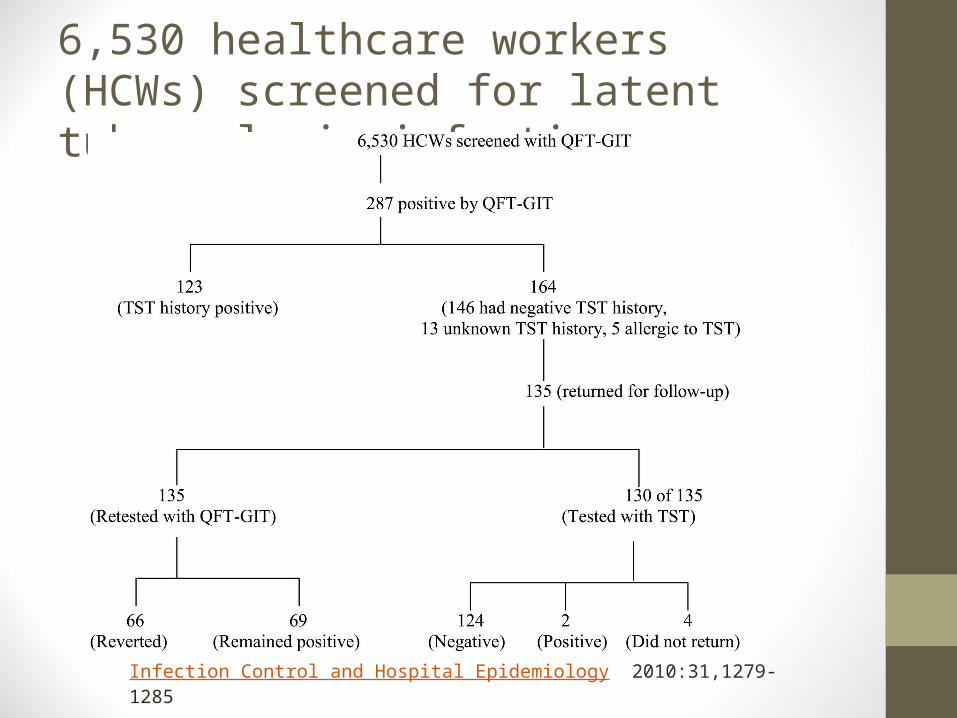
6,530 healthcare workers (HCWs) screened for latent tuberculosis infection
Infection Control and Hospital Epidemiology 2010:31,1279-1285
• 25 fold increase in conversion rate using QFT vs TST• Direct costs • QFT TB Gold in Tube $436,096 • TST $78,360. • Indirect costs • confirmatory TSTs, additional chest
radiographs, extra nurse assessments, and examinations.
• Total costs $521,890
Are IGRA results constant?
• Reversion rates are higher when baseline IFN-γ levels are just above the cut-off point and when baseline results are discordant (i.e. TST-/IGRA+).• Reversion rates low when baseline IFN-γ
levels are high and when baseline results are concordantly positive (TST+/IGRA+).
IGRA performance in contacts and outbreak investigations
• IGRAs correlate well with surrogate markers of exposurein contact and outbreak settings, but not necessarily betterthan TST in all populations.
• Correlation between IGRA results and surrogate markers ofexposure is better than TST in low incidence settings whereBCG has been commonly used; this is not evident in highincidence countries.
• Discordance between TST and IGRAs are almost alwaysfound. Concordance levels seem to vary when IGRAand TST cut-off points are changed.
CTS recommendations
• IGRAs should not be used in the diagnosis of active TB in adults may be a supplemental aide in dx in children.• Contacts – • IGRAs can be used to confirm +ve TSTS• IGRAS or TSTs can be used to identify
+ves for TX for LTBI
CTS recommendations
• Immunocompromised• TST first test• If TST –ve IGRA can be used and if +ve
consider treatment• Degree of benefit unknown in TST –ve
IGRA +ve.• T Spot .TB may be better in an
immunosuppressed population
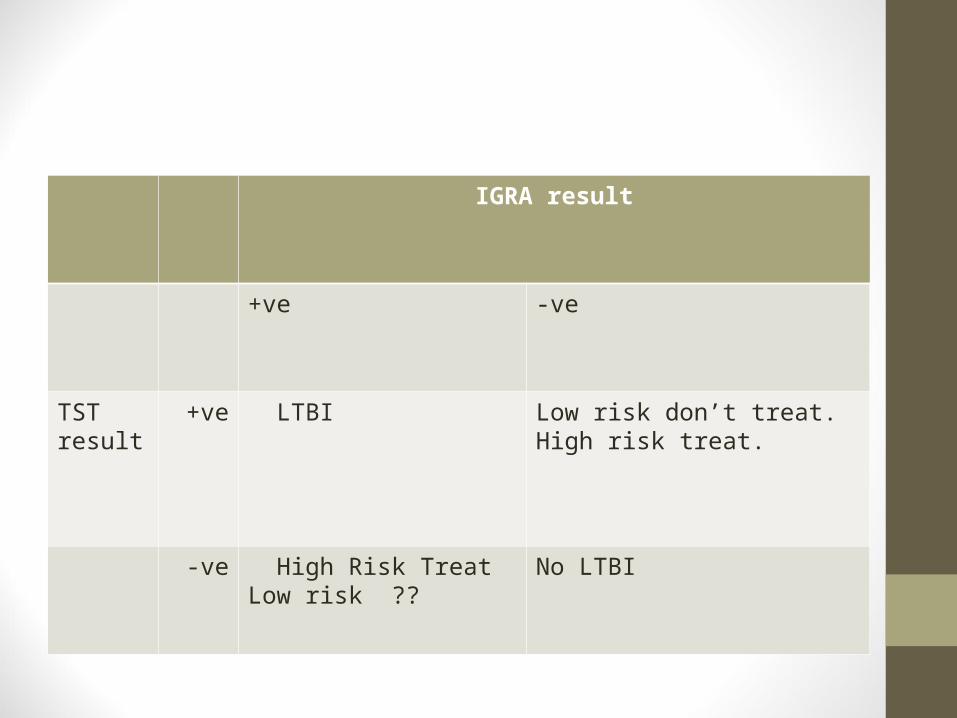
IGRA result
+ve -ve
TST result
+ve LTBI Low risk don’t treat. High risk treat.
-ve High Risk TreatLow risk ??
No LTBI
International GuidelinesClin Microbiol Infect 2011; 17: 806–814 • 33 guidelines and position papers from 25 countries and two
supranational organizations. • The results show considerable diversity in the
recommendations on IGRAs• (i) two-step approach of tuberculin skin test (TST) first, followed
by IGRA either when • the TST is negative (to increase sensitivity, mainly in
immunocompromised individuals), • or when the TST is positive (to increase specificity, mainly in BCG
vaccinated individuals); • (ii) Either TST or IGRA, but not both; • (iii) IGRA and TST together (to increase sensitivity); • (iv) IGRA only, replacing the TST.
• Overall, the use of IGRAs is increasingly recommended,
International GuidelinesClin Microbiol Infect 2011; 17: 806–814 • Most of the current guidelines do not use objective,
transparent methods to grade evidence and recommendations, and
• Do not disclose conflicts of interests. • Future IGRA guidelines must aim to be transparent, evidence-
based, periodically updated, and free of financial conflicts and industry involvement.
Conclusions
• IGRAs will help identify who needs treatment for LTBI• Exact role need to be determined• Very helpful in low risk TST +ve BCG
population• ? immunosuppressed population • Useful for population that is hard to follow
• Definition of positive reaction may have to vary depending on situation of testing